1. Introduction
Bladder cancer worldwide is the 10th most common form of malignant tumor and has the 14th highest cancer-associated mortality [
1]. Urinary bladder urothelial carcinoma (UB UC) is the most common tumor found in the urinary bladder. UB UC can be divided into papillary urothelial carcinoma, which shows papillary growth, and invasive urothelial carcinoma, which initially shows invasive growth. The two types of tumor are known to have different pathogenesis. Recent studies reported that papillary urothelial carcinoma originates from the intermediate cells of the urothelium and that carcinoma in situ and invasive urothelial carcinoma originate from the basal cells of the urothelium [
2].
Recently, several studies have been published that utilized next-generation sequencing (NGS) analysis to analyze and classify UB UC according to gene expression [
3,
4,
5]. While several different mRNA-based subtype classifications exist, some of them overlap with one another. Universally, UB UC is classified into luminal and basal subtypes, and according to each classification system, it is further classified into Tp53-like type, urothelial-like A type, infiltrated type, genomically unstable type, mesenchymal-like type, and small-cell/neuroendocrine-like type [
3]. Each subtype shows high expression of specific genes. While the basal type shows high expression of stem cell or basal urothelial cell markers such as KRT14, KRT5, KRT6, and CD44, the luminal type shows high expression of urothelial differentiation markers such as KRT20, GATA3, and FOXA1 [
3,
5]. Furthermore, consistent with gene expression in each subtype, on immunohistochemistry (IHC) staining, the basal type shows high expression of cytokeratin (CK)5/6, and the luminal type shows high expression of CK20 [
3,
5]. Through the consensus meeting, bladder cancers showing positive KRT5/6, KRT14 expression and negative GATA3, FOXA1 expression were classified into a specific subtype, known as basal-squamous-like (BASQ) [
6]. In the previous study, we classified muscle-invasive urinary bladder cancer (MIBC) into BASQ or non-BASQ subtypes based on the IHC results [
7].
Molecular subtypes for UB UC have been established recently, and studies attempting to demonstrate their clinical significance are actively in progress [
8]. Molecular subtype classification in UB UC also has the potential to play a major role in treatment decisions and prognosis predictions [
9,
10]. In fact, various studies have reported that prognosis, neoadjuvant chemotherapy response, and driver gene mutation vary among molecular subtypes in UB UC. Neoadjuvant cisplatin-based chemotherapy is the standard of care for high-risk MIBC. Neoadjuvant chemotherapy response varies among with molecular subtype, especially the p53-like subtype, which is known to be chemo-resistant, and basal-type MIBC, which is reported to benefit from neoadjuvant chemotherapy because of its chemo-sensitive nature [
3,
11]. In a phase II clinical trial of IMvigor210, different treatment responses to the immune check point inhibitor atezolizumab and prognosis were reported among molecular subtypes in patients with locally advanced urothelial carcinoma. In phase II clinical trial of CheckMate 275 using nivolumab, another immune check point inhibitor, different treatment responses were reported among molecular subtypes in patients with advanced stage urothelial carcinoma [
12,
13,
14,
15]. Thus, molecular subtype classification of UB UC is crucial for effective prognosis estimation and treatment planning.
In the mRNA-based subtype classification, high expression of KRT5 is classified as the basal type and high expression of KRT20 is classified as the luminal type [
4,
5,
16,
17]. Accordingly, with IHC, the basal type shows high expression of CK5/6 and the luminal type shows high expression of CK20 [
3,
5]. However, little has been published regarding cases in which both CK5/6 and CK20 showed high expression or in which neither protein showed high expression. In this study, two additional groups besides the basal and luminal types have been defined. These two groups are the double-positive type and double-negative type, for which we will investigate the molecular genetic characteristics. We could expect great clinical utility if two IHC assays could predict the molecular genetic characteristics of a tumor.
3. Discussion
In recent years, research on molecular-based UB UC subtype classification has been actively underway. As gene expression profiles were reported to show different disease progressions, responses to chemotherapy and survival rates, the UB UC molecular subtype classification became a necessary step in UB UC diagnosis and treatment planning. In MIBC, the basal type is known to arise from basal and stem cells of normal urothelium, and the luminal type is known to arise from terminally differentiated superficial umbrella cells [
20]. During urothelium differentiation, basal and intermediate cells express KRT5 but do not express KRT20. Furthermore, terminal differentiation process is associated with suspension of KRT5 expression and start of KRT20 expression [
21]. Additionally, as KRT14 is also involved in this process, basal cells are known to show KRT14+KRT5+KRT20−, intermediate cells show KRT14−KRT5+KRT20−, and differentiated cells show KRT14−KRT5−KRT20+ [
22]. In MIBC, the basal subtype shows high expression of KRT5, KRT6, KRT14, CD44 and CDH3, shows chemo-sensitive properties, is intrinsically aggressive, and is associated with poor prognosis. The luminal subtype shows high expression of UPK, KRT20, FOXA1, and GATA3, shows chemo-resistant properties, and seems to be less aggressive [
20]. In addition to mRNA levels, IHC protein level markers include CK5/6 and CK14 for the basal subtype and CK20, GATA3, and Uroplakin2 for the luminal subtype. Furthermore, one study indicated that expression of CK5/6 and CK20 was inversely related in MIBC [
3]. Based on these results, in a practical context, affordable IHC antibodies, CK5/6 and CK20, were selected as surrogate markers for IHC-based subgroup classification.
Previous studies utilized NGS analysis to assess gene expression patterns and reported differences in CK expression patterns between molecular subtypes. In this study, we took a different approach in case selection. Cases of the CK5/6 SP, CK20 SP, DP and DN subgroups were selected based on CK IHC results, and gene expression profiles were evaluated with these cases. Furthermore, based on IHC, CK5/6 and CK20 protein expression areas were accurately evaluated before tissue collection, which led to more precise tumor tissue collection.
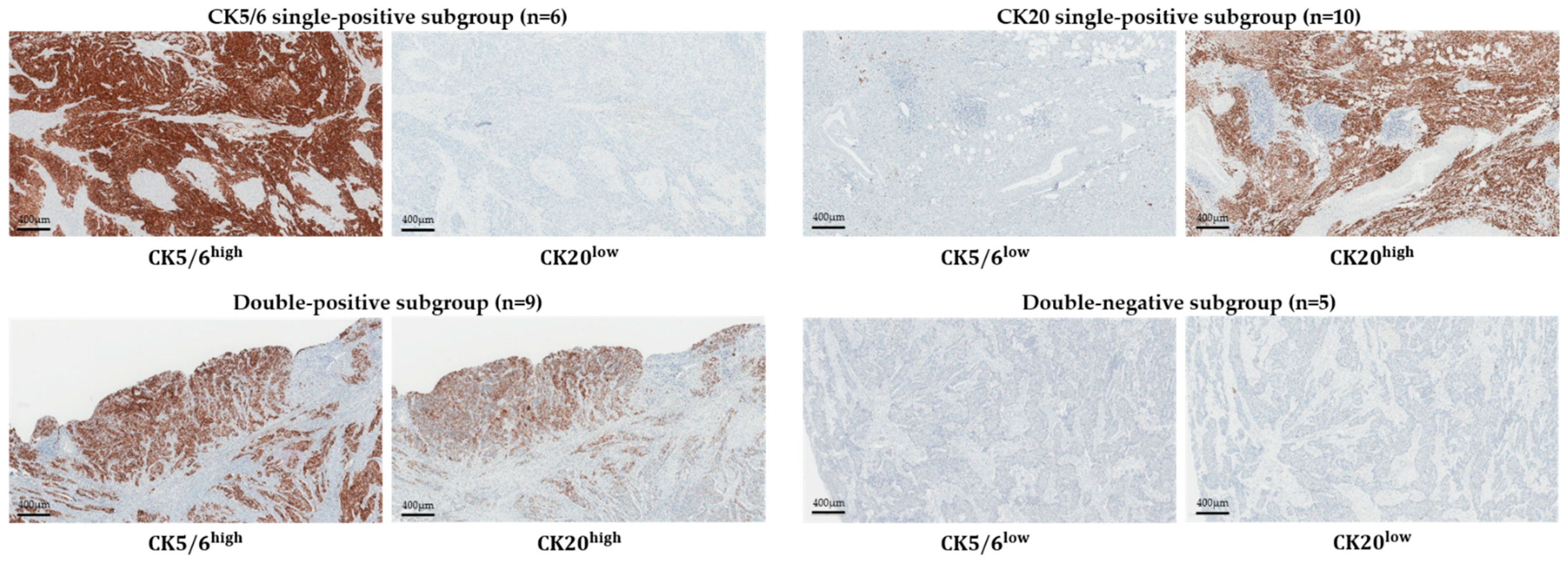
MIBC cases with sufficient fresh-frozen tissues were included, which resulted in 30 samples classified to four subgroups based on CK5/6 and CK20 IHC results. Nine cases in the DP subgroup and five cases in the DN subgroup among 30 cases may indicate a relatively high proportion of DP and DN subgroups in UB UC molecular subtype classification. The DP and DN subgroup cases may be in a stage of transition between molecular subtypes or they may be subtypes completely independent from CK5/6 SP and CK20 SP subgroups. However, research regarding this aspect of subtype classification has not been presented to date. Compared to the CK5/6 SP and CK20 SP subgroups, the DP subgroup showed a relatively high expression of basal- and luminal-type markers, which gave us the impression of a mixed phenotype. This subgroup showed the strongest immune signature genes expression. However, in GO, IPA, and GSEA functional analysis, the DP subgroup did not show a significant difference from the CK5/6 SP subgroup. Based on these results, the DP subgroup was expected to be close to the CK5/6 SP subgroup in tumor characteristic aspects. The DN subgroup, in every comparison with the three other subgroups, showed the highest number on GO and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways with significant differences. The DN subgroup also showed mostly low gene expression on biological signature gene cluster expression analysis. In GO, IPA, and GSEA functional analysis, the DN subgroup showed no significant difference from the CK20 SP subgroup, except for “activation of cells’ associated molecules”, in the IPA result. The DN subgroup is the most similar to the CK20 SP subgroup among the three other subgroups, but we think it is a unique subtype that shows differences in gene expression from the other subgroups.
Expression of p63-associated genes was high in the CK5/6 SP and DP subgroups. TP63, which is a transcription factor associated with basal/stem cells in the urothelium, is known to be activated in the basal-type MIBC and to regulate basal gene expression signature [
3]. In line with previous studies, which reported that p63-associated genes were enriched in the basal-type MIBC, CK5/6 SP and DP subgroups showed high expression of p63-associated genes.
In comparison between subgroups, expression of TP53-like signature genes was the lowest in the DN subgroup and varied among cases. Six cases, which showed diffusely strong positive results on IHC, showed high expression of TP53-associated gene mRNA. Association between TP53 mRNA expression and TP53 IHC protein expression showed a positive correlation.
Expression of immune response-associated genes was high in the DP subgroup, and the CK5/6 SP, DN, and CK20 SP subgroups followed in respective order. Dividing the genes into two groups based on CK5/6 IHC results, immune response GO term associated DEGs were more enriched and associated genes were more upregulated in DP and CK5/6 SP subgroups than in DN and CK20 SP subgroups. Additionally, on IPA analysis, immune activation was more upregulated in DP and CK5/6 SP subgroups than in the other subgroups. In a previous study in our group, it was found that programmed cell death-ligand 1 (PD-L1) expression was enriched in the BASQ subtype positive for CK5/6 and CK14 on IHC [
7]. These results correlate with previous studies, which reported high immune gene signature expression in the basal subtype [
8,
23].
Expression of EMT marker was enriched in the DP and CK5/6 SP subgroups. The EMT is the process of epithelial or endothelial cells acquiring mesenchymal phenotypes, and is associated with tumor progression and metastasis process [
24,
25,
26,
27]. Furthermore, some studies reported that, in various cancers, EMT showed a strong correlation with immune activation, and had high expression of programmed cell death-1 (PD-1), PD-L1, CTLA4, OX40L and PD-L2. In these studies, activation of the immune cell signaling pathway was observed in the EMT setting, which was interpreted as an indication that the EMT may facilitate a change of the tumor microenvironment [
28,
29]. Additionally, Chen et al. suggested that microRNA-200 (miR-200) formed a negative feedback loop with ZEB1, an EMT activator, suppressed the EMT, and suppressed PD-L1 expression. These authors demonstrated that the EMT is linked to the immunosuppression through the miR-200/ZEB1 axis [
30,
31]. The miR-200 family is known to be enriched in the luminal type, which also correlates well with the results of this study, as CK20 SP and DN subgroups showed low EMT and immune response-associated gene expression [
3].
Expression of cell adhesion markers showed low expression of tight junction-related genes TPJ2 and CLDN4 and high expression of desmosome-related genes DSC3 and PKP1, gap junction-related genes GJB3 and GLB4, and epithelial integrin genes ITGA6 and ITGB4 in the CK5/6 SP subgroup. These results imply that the CK5/6 SP subgroup shows increased expression of cell adhesion, especially basolateral cell adhesion-related genes. This result is in keeping with previous studies, which reported high cell adhesion gene expression signature in the mRNA-based basal subtype, including urobasal B and SCC-like subtype [
16].
Expression of the MAPK and TNF signaling pathways was enriched in the DP and CK5/6 SP subgroups. Most of the DEGs associated with these signaling pathway were upregulated in the DP and CK5/6 SP subgroups.
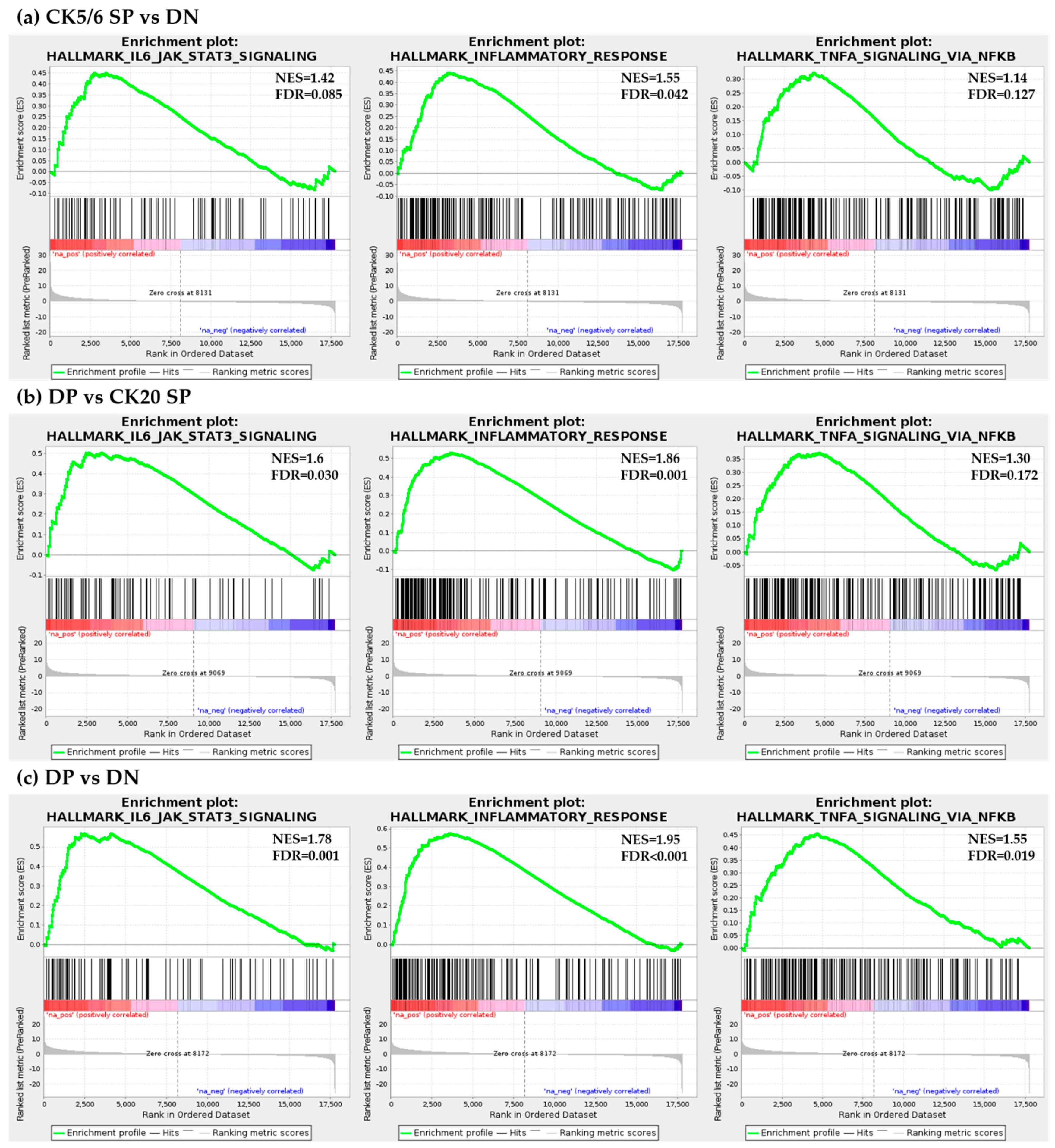
On GSEA analysis, the IL6-JAK-STAT3 signaling pathway and TNF-α signaling via NF-κB signaling pathway were significantly enriched in DP and CK5/6 SP subgroups. In contrast, the DN subgroup was found to be less sensitive to this pathway. The IL6-JAK-STAT3 signaling pathway is upregulated in various types of cancer and its hyperactivation is associated with adverse clinical outcome [
32,
33,
34]. Furthermore, the TNF-α/NF-κB signaling pathway is known to be involved in the tumor invasion and metastasis [
35,
36]. Considering the GSEA results, the CK5/6-positive subgroup (CK5/6 SP and DP subgroups) is a more aggressive subtype than the CK5/6-negative or at least the DN subgroup.
On IPA analysis, compared to the other subgroups, the DN subgroup showed downregulated cell movement, cell migration, and cell activation. Such cellular functions, which are associated with cell motility, are closely related to cancer invasion and cancer metastasis [
37,
38,
39,
40]. Based on IPA analysis we can expect the DN subgroup to have a less aggressive behavior than the three other subgroups.
Different molecular subtypes were reported to have different prognoses and chemotherapy sensitivity in MIBC. In addition, we also found that the IHC-based classification has prognostic value. Compared with the CK5/6-negative subgroup (CK20 SP and DN subgroups), the CK5/6-positive subgroup (CK5/6 SP and DP subgroups), which implies the high EMT, IL6-JAK-STAT3 signaling pathway, TNF-α/NF-κB signaling pathway and immune gene expression signature, show adverse disease progression outcome, and this result is in keeping with the findings of previous studies [
3,
5]. It is assumed that the effective immune escape process that arises by expression of PD-L1 may be related to disease progression. Although the DP subgroup showed no difference in disease progression rate from other CK20 SP and DN subgroups, this consequence is considered because there were very few cases of the DP subgroup in this study population. In contrast to the PFS, there was no significant difference in OS rate between IHC-defined subgroups. The difference in PFS for each subgroup but no difference in OS can be interpreted as meaning that the post-progression period is considerably long. We think this is related to the fact that most of the subjects of this study consist of pathologic stage T2 cases. Since it was composed of cases with a good overall prognosis, there was no significant difference in the OS analysis for each subgroup.
In the personalized precision medicine era, subgrouping of patients based on molecular characteristics has considerable influence on selecting therapeutic regimens and forecasting therapeutic responses and prognoses. In addition, mRNA sequencing analysis is a good method to examine phenotype characteristics of a tumor, however, in this study we utilized an IHC-based classification that is simpler and more affordable. We examined the molecular characteristics of subgroups based on IHC classification. In summary, we found that the CK5/6-positive subgroup showed a high gene expression signature related to aggressive behavior and showed worse clinical outcomes.
4. Materials and Methods
4.1. Tissue Samples and Case Selection
In total, MIBC tissues from 30 patients who underwent a radical cystectomy at Seoul National University Hospital (SNUH) from 2016 to 2018 were included in this study. First, 30 fresh frozen tissue samples from 2016 to 2018 were investigated. The section containing prominent tumor tissue was selected, of which one section was prepared as a formalin-fixed paraffin-embedded (FFPE) tissue block, and the corresponding symmetric section was fresh frozen with liquid nitrogen and preserved in −70 °C until tumor excision. A total of 30 samples were classified to four subgroups based on IHC results for CK5/6 and CK20. In each subgroup three representative cases were selected, and RNA sequencing was carried out with a total of 12 fresh frozen tissue samples. All 12 patients were included in the prospective studies. Written informed consent was obtained from all patients enrolled in this mRNA analysis group.
Additionally, 189 MIBC patients who underwent transurethral resection of the bladder or radical cystectomy at SNUH or Seoul Metropolitan government-Seoul National University Boramae Medical Center were included in the survival analysis group. A total of 189 FFPE block tissue samples from 2004 to 2010 were investigated. A tissue microarray (TMA) block was prepared from FFPE tissue blocks (SuperBioChips Laboratories, Seoul, Republic of Korea). Two cores (2 mm in diameter) containing invasive tumor areas were obtained from each case. This study was approved by the Institutional Review Board (IRB) of SNUH (IRB No C-1701-083-823, 24 January 2017).
4.2. Immunohistochemistry
IHC for CK5/6, CK20, CK14, GATA3, FOXA1, CD44 and TP53 was performed with an automatic immunostainer (BenchMark XT; Ventana Medical Systems, Tucson, AZ, USA), following the manufacturer’s instructions. The primary antibodies against CK5/6 (1:100; D5/16 B4; Dako, Glostrup, Denmark), CK20 (1:50; Ks 20.8; Dako), CK14 (1:300; LL002; Cell Marque, Rocklin, CA), CD44 (1:100; 156-3C11; Thermo Fisher), GATA3 (L50-823; 1:500; Cell Marque), FOXA1 (1:500; PA5-27157; Thermo Fisher, Waltham, MA, USA) and p53 (1:1000; DO7; Dako) were used. Immunohistochemical positive control tissues were tonsil tissue for CK5/6 and CD44, duodenal mucosa epithelium for CK20, squamous cell carcinoma tissue for CK14, urothelial carcinoma tissue for GATA3, gastric mucosa epithelium for TP53, and breast cancer tissue, previously confirmed with positive expression for FOXA1.
The full-section IHC staining was performed on all 12 cases, and in each case, two different invasive tumor areas were investigated. Additionally, the same IHC was carried out for 189 MIBC tissue TMA blocks.
The evaluation results of CK5/6, CK20, CK14, GATA3 and FOXA1 IHC were derived from a previously published study [
7]. Briefly explaining the evaluation criteria again, >20% expression was defined as high expression status. In previous studies, 20% cut-off value was reported to be ideal for classification of molecular subtypes in bladder cancer [
41,
42]. The same cut-off was applied for CK5/6, CK20, CK14 and CD44. For GATA3 and FOXA1, the percentage of nuclear stained cells and staining intensity were considered. Staining intensity was scored from 0 to 3+ (0: no staining, 1+: weak staining, 2+: moderate staining, and 3+: strong staining). IHC staining with both 3+ intensity and more than 20% of tumor cells was defined as high expression. Two pathologists (B.K. and C.L.) evaluated IHC staining at two different time points, without awareness of the previous results at the second evaluations. In the case of discrepant results between evaluations another pathologist (K.C.M) was consulted before making the final decision.
4.3. RNA Sequencing
After IHC results were identified on the FFPE tissue block, mRNA was extracted from the corresponding location of the symmetric fresh-frozen MIBC tissues. A 3-mm-sized plunger was used for punching out the fresh-frozen tissue. RNA library was assembled with TruSeq RNA Access Library Prep Kit, and base sequence analysis was carried out with Illumina HiSeq 2500 platform (Illumina, San Diego, CA, USA). (Macrogen, Inc., Seoul, Korea) Paired demultiplexed fastq files were generated, and initial quality control was performed using FastQC (Phred quality score >30). The adaptor sequences were removed by using Trimmomatic program and trimmed data were mapped to the reference genome (UCSC hg19) using the HISAT2 and Bowtie2. Previously known gene/transcripts were assembled with the StringTie program. Raw data were normalized and, mRNA expression data were presented as reads transcript per million and were transformed into log 2 volume values for the analysis.
4.4. Functional Analysis
In this study, DEGs were identified with DESeq2. Statistical analysis was performed on selected genes whose median count for each gene was greater than 5 in at least one comparison combination. Functional analysis of DEGs was performed using GO and the KEGG pathway (adjusted p-value < 0.05 and |fold change| ≥2). The analyses were performed by biological process, molecular function, and cellular component, which are the GO subcategories. Functional annotation based on the KEGG database was implemented. Additionally, the functional analyses were performed with the use of IPA.
4.5. Statistical Analysis
The association between IHC defined subgroups with immunohistochemistry expression was evaluated by the chi-squared test. The associations between IHC based subgroups and PFS, and OS were evaluated by the Kaplan–Meier method with the log-rank test. Statistical analyses were performed using SPSS software (version 23; IBM, Armonk, NY, USA). Two-sided p-values < 0.05 were considered to be statistically significant.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}