
Effect of a Vegan Diet on Alzheimer’s Disease
by
 ,
,
Alzbeta Katonova
1,
Katerina Sheardova
2,
Jana Amlerova
1,
Francesco Angelucci
1,* and
Jakub Hort
1 1
Memory Clinic, Department of Neurology, 2nd Faculty of Medicine, Charles University and Motol University Hospital, 150 06 Prague, Czech Republic
2
International Clinical Research Centre, St. Anne’s University Hospital, 602 00 Brno, Czech Republic
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2022, 23(23), 14924; https://doi.org/10.3390/ijms232314924
Submission received: 5 November 2022
/
Revised: 19 November 2022
/
Accepted: 23 November 2022
/
Published: 29 November 2022
(This article belongs to the Special Issue Nutrients and Neurodegenerative Diseases)
Abstract
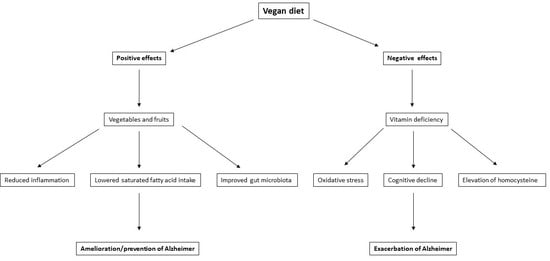
:There is evidence indicating that a vegan diet could be beneficial in the prevention of neurodegenerative disorders, including Alzheimer’s disease (AD). The purpose of this review is to summarize the current knowledge on the positive and negative aspects of a vegan diet regarding the risk of AD. Regarding AD prevention, a vegan diet includes low levels of saturated fats and cholesterol, contributing to a healthy blood lipid profile. Furthermore, it is rich in phytonutrients, such as vitamins, antioxidants, and dietary fiber, that may help prevent cognitive decline. Moreover, a vegan diet contributes to the assumption of quercetin, a natural inhibitor of monoamine oxidase (MAO), which can contribute to maintaining mental health and reducing AD risk. Nonetheless, the data available do not allow an assessment of whether strict veganism is beneficial for AD prevention compared with vegetarianism or other diets. A vegan diet lacks specific vitamins and micronutrients and may result in nutritional deficiencies. Vegans not supplementing micronutrients are more prone to vitamin B12, vitamin D, and DHA deficiencies, which have been linked to AD. Thus, an evaluation of the net effect of a vegan diet on AD prevention and/or progression should be ascertained by taking into account all the positive and negative effects described here.
1. Introduction
In recent years, a vegan diet has grown in popularity worldwide. According to a survey conducted in 2021, vegans represent about 2–3% of the population in European countries [1]. The complex effect of a vegan diet on mortality, health, and environmental outcomes was also reflected by the recommendation for a sustainable diet strategy based on the survey from 150 countries worldwide, where a vegan diet turned out to be the most effective for the followed parameters as compared to vegetarian, pescatarian, and flexitarian diets [2]. The main reasons why people seek diets without meat and animal products can be ideological, religious, or medical [3,4]. Among these reasons, there is some evidence indicating that a vegan diet could be beneficial in preventing neurodegenerative disorders, such as Alzheimer’s disease (AD).
Neurodegenerative disorders are also on the rise worldwide. It was estimated that more than 50 million people worldwide lived with dementia in 2019, which is expected to triple in 30 years, reaching 152 million in 2050 [5]. AD is the leading cause of dementia, and its prevalence is growing rapidly, making it a major public health issue. The onset of AD is predicted by several risk factors, which are both genetic and modifiable (Table 1). Non-modifiable risk factors include advanced age [6,7,8], gender [7,8], a family history of dementia, and genetic susceptibility [6]. AD is also associated with modifiable risk factors, such as depression [9,10,11], hypertension [12,13,14], type 2 diabetes [15,16,17], obesity [18,19,20], physical inactivity [21,22], low education [6,7,23], and unhealthy diet [24,25]. Even though there is currently no cure for AD, people can reduce their risk by addressing the modifiable risk factors. One of the key lifestyle factors that can be modified to prevent AD is diet. The purpose of the present review is to summarize the current knowledge on the positive and the negative aspects of a vegan diet in the prevention and during the course of AD.
2. Vegan Diet and Brain Function
Nutrition plays a crucial role in maintaining proper brain function as we age. Researchers have been increasingly studying the role of dietary and lifestyle factors, such as plant-based diets, in AD [25]. Brain health was found to be improved by diets such as the Mediterranean, Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND), or Dietary Approaches to Stop Hypertension (DASH). Adhering to the Mediterranean, DASH, or MIND diet can decrease cognitive decline and AD risk [26,27,28]. What these diets have in common is that they limit sugar and saturated fat intake and recommend eating a high percentage of fruits, vegetables, whole grains, and nuts and consuming minimal amounts of red or processed meat. Several medical organizations have recommended a plant-based diet to optimize cognitive health and potentially prevent dementia [29,30,31]. To maintain cognitive health and prevent cognitive aging, consuming a plant-based diet can be a low-risk and beneficial lifestyle change.
However, plant-based and vegan diets are not synonymous. A vegan diet tends to be plant-based, but plant-based diets are not vegan by definition. In a plant-based diet, plants are the primary component, but animal products are also included in small amounts. A whole-food, plant-based diet is centered on whole, unrefined plant foods and minimizes highly refined foods, such as bleached flour, refined sugar, oil, and processed packaged foods [32]. A vegan diet entirely abstains from animal products and is a stricter version of vegetarianism. In addition to cutting out meat, vegans eliminate everything made or derived from an animal, including dairy, eggs, and honey. Additionally, vegans refrain from using animal products in other areas of their lives, including beauty products, footwear, and clothing [4].
The effects of a plant-based diet on brain health and cognition are well documented. A vegan diet seems effective for various outcomes, ranging from weight loss to cardiometabolic health [33] to reduced cancer incidence [34]. Still, its effects on the brain are not well ascertained. Does strict veganism confer any more protective benefits for the brain than vegetarianism or healthy eating? The results of vegetarian diets regarding health outcomes are not necessarily applicable to a vegan diet because a vegan diet is stricter and contains only plant-based foods. A rapid increase in veganism has necessitated a better scientific understanding of the effects of a vegan diet on human health, particularly relating to the brain and cognitive functions.
3. Possible Beneficial Effects of a Vegan Diet on the Brain and the Risk of AD
The quality and quantity of nutrients vary according to the diet one follows. Compared to omnivorous diets, a vegan diet is typically richer in fiber; polyunsaturated fatty acids (PUFA); vitamins A, B1, B6, C, and E; folate; magnesium; iron; and copper [35,36,37]. All these nutrients can have an effect on AD pathophysiology. A vegan diet could therefore aid in either the primary or secondary prevention of AD. In this section, we will analyze each of the diet components and specify whether they are useful for the primary or secondary prevention of AD.
3.1. Fruits and Vegetables
Vegetables, fruits, grains, legumes, nuts, and seeds constitute the bulk of a vegan diet. Several meta-analyses have found that the increased consumption of fruits and vegetables can reduce dementia risk and slow down cognitive decline in older adults [38,39,40]. Conversely, a low vegetable intake is associated with poorer cognition in AD dementia [41]. A high intake of fruits and vegetables could therefore act as secondary prevention in AD. Furthermore, the phytochemicals, vitamins, minerals, and fiber found in fruits and vegetables have well-established anti-inflammatory and antioxidant properties, which may protect the brain by reducing the pathological processes associated with aging and dementia [42] (Figure 1).
3.2. Reduction in Inflammation
Inflammation plays an important role in the development of AD. Inflammatory cascades may contribute to AD pathogenesis when the amyloid beta (Aβ) levels are continuously high, mobilizing the innate immune system through microglia activation [43]. Patients with AD often present with high levels of inflammatory markers, and these markers are linked to cognitive decline as well [44,45].
Part of the protective mechanisms of a vegan diet could be attributed to its beneficial effect on the reduction of inflammatory markers (Figure 1), thus acting as secondary prevention in AD. It appears that meat-based dietary patterns are positively correlated with biomarkers of low-grade inflammation, while vegetable- and fruit-based diets are inversely correlated [46]. However, studies providing data on inflammatory biomarkers in vegans are sparse and inconsistent. In a cross-sectional study of 36 vegans and 36 omnivores, Menzel et al. found no significant differences in any of the seven investigated inflammatory biomarkers (high-sensitivity C-reactive protein (hsCRP), adiponectin, ICAM-1, IL-18, IL-1 RA, omentin-1, and resistin). The participants that adhered to the vegan diet for over 4.8 years were more likely to have lower hsCRP levels compared to those adhering to a vegan diet for less than 4.8 years [47], suggesting the length of the diet may be an essential factor in reducing systemic inflammation. Šebeková et al. also found that plasma CRP levels did not differ significantly between vegans and omnivores [48]. In contrast, Franco de Moreaes et al. detected lower values of inflammatory markers, CRP, and the TNF-α/IL-10 ratio in strict vegetarians (defined as consuming animal products less than once a month) compared to vegetarians and omnivores [49]. Suttlife et al. found reductions in the circulating CRP after a three-week lifestyle intervention that included a vegan diet [50]. Because the study included only overweight and obese participants, the decline in the CRP level between the baseline and follow-up could have been a result of various factors. The reduction in the body mass index was probably the most influential because overweight and obesity are associated with high levels of inflammation [51]. Researchers found that participants following a vegan diet prior to the intervention had the most favorable CRP profiles compared to vegetarians and omnivores [50], which may hint at the fact that a vegan diet may help to reduce inflammatory processes. Finally, a recent meta-analysis concluded that vegans have lower levels of CRP than omnivores [52].
Despite these data, the evidence regarding the effect of a vegan diet on inflammatory biomarkers is still limited. The majority of studies examining inflammatory biomarkers in vegans have small sample sizes and are cross-sectional, so causality cannot be determined. So far, only one vegan intervention study has been conducted, and because the participants were overweight, generalizing to other populations was not possible [50]. Further studies are needed to prove that a vegan diet may help prevent or counteract inflammatory states and subsequently aid in lowering the risk of AD.
3.3. Modifiable Risk Factors for AD
Other than genetic factors, hypertension [12,13,14], diabetes [15,16,17], obesity [18,19,20], and midlife elevated blood lipids [53,54,55,56] all increase the AD dementia risk. All these AD risk factors can be modified through a vegan diet; therefore, a vegan diet can also aid in the primary prevention of AD. As a whole, a vegan diet can indirectly improve cognition by maintaining a healthy body weight and by reducing cardiovascular risk factors, such as cholesterol [34], blood glucose [57], and blood pressure [58]. Furthermore, a vegan diet might be a valuable tool for preventing diabetes [59]. Vegan diets have a lower energy content, making the people adopting them more likely to have a healthier body mass index (BMI) and lower obesity rates than those following other diets [34,35]. Low BMIs, maintained on the vegan diet, likely contribute to improved lipid profiles, glycemic results, and insulin sensitivity.
A vegan diet influences nutrient intake in several ways, which may ultimately affect insulin sensitivity. A vegan diet increases the intake of protective nutrients, such as polyphenols [60]. Dietary polyphenols inhibit glucose absorption in the intestine, stimulate insulin secretion, and enhance insulin-dependent glucose uptake [61]. The glucose-lowering effect of a vegan diet may also be attributed to the higher fiber content. Soluble dietary fiber improves glycemic control by delaying gastric emptying and the consequent slower glucose absorption and uptake [59]. Additionally, both soluble and insoluble fiber consumption can result in improved glycemic control by increasing insulin sensitivity [62]. A low-fat vegan dietary intervention leads to lower intramyocellular and hepatocellular lipid storage and thus increased insulin sensitivity [63].
3.4. GI Tract
A growing body of research shows that the gut microbiome plays a crucial role in AD pathogenesis [64,65,66]. The gut microbiome of AD patients is compositionally different, and it has a decreased diversity compared with those of cognitively unimpaired people [67]. Interactions between the intestine and the brain are mediated by the nervous system or by chemical substances crossing the blood–brain barrier [68]. A dysbiotic gut microbiome may contribute to the progression and exacerbation of the disease, possibly by promoting immune activation, systemic inflammation, Aβ aggregation, and insulin resistance in the periphery and the brain [66]. A vegan diet could act as a secondary prevention measure in AD by potentially establishing a healthier gut microbiota.
The ability to target the gut microbiota and restore its composition through food-based therapy may provide new preventive and therapeutic options for AD. Diet is among the key factors affecting the gut microbiota ecosystem [69]. A vegan diet differs from an omnivorous diet in terms of its macronutrient composition. The protein, total fat, and saturated fat intake is lower, while the carbohydrate and fiber intake is higher on a vegan diet [35,70]. The macronutrient balance alters the composition of the gut microbiota and, in turn, affects the production of metabolites that may have a positive or negative effect on health. A vegan diet seems to promote a more diverse gut microbiome and a more even distribution of microbial species [71]. The diversity and stability of the vegan gut microbiota are primarily attributed to a higher intake of complex carbohydrates, fiber, and polyphenols [35,72]. However, researchers have reported mixed results about how exactly a vegan diet affects the microbiome and its diversity. A short-term, four-week vegan diet intervention in omnivorous participants that were randomized to a vegan or an omnivorous diet led to no remarkable changes in their gut microbiota [73]. No significant difference between the alpha diversity of the subjects on the vegan or omnivore diet was observed; there were, however, changes in the abundance of the genera Coprococcus, Roseburia, and Blautia after the trial, but most of them were only detectable in a few of the samples [73]. Coprococcus, which was enriched in a vegan diet and depleted in an omnivore diet [73], was previously reported to be depleted both in the gut microbiota of 3xTg-AD mice [74] and in the fecal microbiota of AD patients and positively correlated with Mini Mental State Exam (MMSE) scores [75]. Prochazkova et al. also found only modest differences in the microbiome composition associated with a long-term vegan vs. omnivore diet [76].
A recent systematic review of cross-sectional studies concluded that most studies report an increased abundance of Bacteroidetes on the phylum level and a higher abundance of Prevotella on the genus level in vegans compared to omnivores [77]. Prevotella is one of the fiber-utilizing bacterial species that ferments fiber into short-chain fatty acids (SCFAs). SCFAs are among the most abundant metabolites of the gut microbiota, and they play a crucial role in mediating gut–brain interactions. Their presence has been implicated in the occurrence and development of AD, and they play an important role in the disease process by regulating the synaptic plasticity, reducing the Aβ and tau pathology, and neuroinflammation [78]. In fecal samples, SCFAs decrease progressively from amnestic mild cognitive decline (MCI) to AD [79]. A vegan diet should in theory result in higher concentrations of SCFAs due to the increased intake of fiber, but the results of the studies are not unanimous. While Prochazkova et al. found a higher concentration of SCFAs in vegan fecal and serum metabolome [76], Trefflich et al., Wu et al., and Reiss et al. observed no significant differences in the fecal SCFA concentrations between vegans and omnivores [80,81,82]. While De Filippis et al. found that a vegan diet produced greater quantities of SCFAs, they also found a positive correlation between the SCFAs levels and adherence to a Mediterranean diet also in omnivores, irrespective of the diet type [83].
The vegan gut microbiota may also provide health benefits by reducing inflammation because it has been found to contain fewer pathobionts associated with low-grade inflammation [77]. Cattaneo et al. found that Aβ-positive AD patients have more pro-inflammatory bacteria in the gut than healthy controls and Aβ-negative patients. The inflammatory state, cognitive impairment, and Aβ presence in the brain were all positively related to the presence of pro-inflammatory microorganisms in the gut [84].
There is still some uncertainty about whether or not it leads to a more protective, healthier gut microbiota [77]. It seems that a vegan diet could be beneficial for the gut microbiota, although individual responses vary [73]. Despite the similarity between the gut microbiota of vegans and omnivores, their metabolomic profiles are quite different [76,81]. Veganism reduces the abundance of potentially harmful metabolites and increases the abundance of beneficial metabolites [76]. There is a need for further research to clarify the complicated mechanisms and interactions between the vegan diet, gut microbiota, and the subsequent effect of the diet on the pathophysiology and development of AD. Diet diversity is a critical driver of microbiota stability, and as such, it might be more essential to consume a variety of plant-based foods rather than to exclude animal products [85].
3.5. TMAO Reduction
Trimethylamine N-Oxide (TMAO) is the product of a microbial metabolite that increases with red meat consumption and has been linked to neurological diseases [71,72,85]. It was shown that the accumulation of tau and Aβ in the brain may be enhanced by TMAO. TMAO is capable of controlling the folding and aggregation state of the Aβ and accelerating its random coil-to-β-sheet conformational change, which is essential for the formation of Aβ fibers, thus accelerating the amyloidogenic plaque formation [86]. Accordingly, in AD and MCI patients, elevated cerebrospinal fluid TMAO levels correlate positively with the biomarkers of AD pathology and neurodegeneration [87], suggesting that TMAO may contribute to AD pathology. A possible mechanism by which TMAO could contribute to the development of AD is through the exacerbation of neurodegenerative and neuroinflammatory processes. Additionally, TMAO has the potential to contribute to AD by stimulating insulin resistance and other metabolic disturbances associated with AD pathophysiology [88]. An increase in plasma TMAO has been shown to promote brain aging and cognitive impairment and to worsen AD by reducing the neurite density and increasing the synaptic damage in mice [89,90]. Conversely, reducing the TMAO levels in plasma has been shown to ameliorate cognitive decline in a mouse model of AD [91].
Vegan diets decrease the TMAO levels in plasma and urine, thus acting as a secondary prevention in AD, while diets high in animal protein have a negative effect [92]. In an interventional study investigating the impact of a vegan diet, the TMAO levels decreased after only eight weeks of consuming a vegan diet [93]. It has also been shown that following the consumption of L-carnitine, trimethylamine that is abundant in red meat, TMAO is produced in greater quantities by the intestinal microbiota of omnivores compared to vegetarians and vegans [94]. However, the plasma concentrations of TMAO between lacto-ovo-vegetarians and vegans do not seem to differ [95], suggesting that a vegetarian diet might be also powerful enough to lower TMAO levels.
3.6. Mental Health
Mental health could be an important factor to prevent AD insurgence. In the case of problems associated with mental health, it is possible that the risk of getting AD will increase. Factors such as chronic stress and depression can in fact increase the risk of developing AD [9,10,11]. In this regard, there is some light evidence that a vegan diet positively affects mental health and well-being, thus acting as primary prevention in AD.
Systemic reviews on the association between a vegan diet and depression reveal conflicting evidence, possibly due to the heterogeneity of the studies included. Thus, the pitfall of the existing studies is that the causal effect between depression and a vegan diet cannot be depicted [96].
Another meta-analysis found an association between a vegan diet and lower scores of anxiety [97]. The only intervention study with a raw vegan diet reported improvement in the overall QOL by 11.5% (p = 0.001), a decrease in anxiety by 18.6% (p = 0.009), and perceived stress by 16.4% (p < 0.001) after 12 weeks [98].
Possible mechanisms for the effects of a vegan diet in reducing depression and/or anxiety could be related to the action of quercetin, which is found only in plant foods [99]. Quercetin acts as an inhibitor of monoamine oxidase (MAO), an enzyme that breaks down the neurotransmitters regulating mood, such as serotonin, dopamine, and norepinephrine [100]. Thus, by acting as a sort of natural antidepressant, quercetin can increase the amount of serotonin, dopamine, and norepinephrine in the brain [101], an effect that can mitigate anxiety and depression. In addition to its antidepressant properties, it was shown that quercetin exerts a neuroprotective effect in AD animal models. Mice treated with quercetin show a significant improvement in cognitive performance [102]. As a neuroprotective agent, quercetin inhibits Aβ aggregation and tauopathy [103], reduces oxidative stress and inflammation [104], and stimulates neurogenesis and neuronal plasticity by increasing the BNDF/TrkB signaling [105].
Conversely, arachidonic acid, which is found mostly in animal food, increases inflammation in the body [106], which is subsequently associated with feelings of anxiety, stress, and depression. Therefore, a diet that avoids arachidonic acid and increases quercetin could have a beneficial effect on one’s mood. Nonetheless, longitudinal interventional studies for confirming this causal effect are lacking.
4. Possible Detrimental Effects of a Vegan Diet on the Brain and the Risk of AD
A vegan diet is restrictive and has fewer food options, increasing the risk of various nutrient deficiencies (Table 2). Regarding the micronutrient supply, two recent systematic reviews have found significant differences between the nutrient intake of meat-eaters and vegans. Veganism was associated with a low intake of vitamins B2, B3, B12, and D; iodine; calcium; selenium; and zinc [35,36].
4.1. Vitamin B12 Deficiency
Vitamin B12 (cobalamin) is an essential vitamin that plays a vital role in the health of the brain and nervous system. The central nervous system requires vitamin B12 for the proper development and initial myelination as well as for the maintenance of the myelin sheath [110]. Upon absorption, vitamin B12 acts as a cofactor for methionine synthase, an enzyme responsible for the synthesis of methionine from homocysteine. Consequently, a vitamin B12 deficiency may result in a decreased synthesis of methionine and S-adenosylmethionine, adversely affecting methylation reactions, which play an essential role in the metabolism of myelin sheath components [111]. Vitamin B12 also acts as a coenzyme for methylmalonyl-CoA mutase to convert methylmalonyl-CoA into succinyl-CoA. A failure to perform this reaction results in the conversion of methylmalonyl-CoA into methylmalonic acid, which destabilizes the myelin sheath [111]. Thus, a low B12 status can, among other neurological symptoms, lead to progressive axonal demyelination and an increased rate of cerebral atrophy in the elderly [110,112,113]. An elevated homocysteine concentration is considered a sensitive metabolic marker for a vitamin B12 deficiency [114] and is closely linked to an increased risk of AD [115]. Clinical trials have found that lowering homocysteine levels with B vitamins treatment slows down the rate of brain atrophy and cognitive decline in people with MCI with high homocysteine levels at baseline [116,117,118]. In a vegan diet, a deficiency in vitamin B12 is likely because animal food is the primary source of this nutrient (Figure 2). Although some plant-based foods contain amounts of B12, such as soy-yogurt, mushrooms, and seaweed, these tend to be less efficient than animal foods as they contain significant quantities of vitamin B12 analogues that are biologically inactive in humans [119,120].
Therefore, it is not surprising that the intake of vitamin B12 is significantly lower in vegan diets than that of other dietary types [35,36]. An unsupplemented vegan diet will inevitably result in a B12 deficiency. In a five-year prospective study, transitioning from an omnivore to a vegan diet was linked to vitamin B-12 deficiency [107]. Nonetheless, only the participants that did not take any supplements became deficient. In contrast, the group that consumed food fortified with B12 did not exhibit any signs of deficiency [107], confirming that foods fortified with B12 and B12 supplements are the only reliable vegan sources of B12.
Even a short four-week vegan diet intervention decreased the bioactive form of vitamin B12 holotranscobalamin in plasma [121]. A low intake of dietary B12 does not necessarily result in a deficiency. According to cross-sectional studies comparing the micronutrient status of vegans and omnivorous diets, vegans consume negligible amounts of dietary vitamin B12. Still, their vitamin B12 status is mainly normal, and a deficiency in this particular vitamin is rare [37,108]. Vegans who regularly supplement with cobalamin have similar serum cobalamin levels to nonvegans [122]. Most vegans nowadays are aware of the risk of a vitamin B12 deficiency associated with the diet, and vitamin B12 is one of the most commonly taken supplements [37]. In general, vegans do not have to be worried about a deficiency leading to a high homocysteine level if they supplement regularly.
4.2. Vitamin D Deficiency
A vitamin D deficiency is not a unique feature of the vegan diet [123], but because plant foods that naturally provide vitamin D are few, a vegan diet is generally associated with a lower intake of vitamin D when compared to other diet types [35]. In the Nutritional Evaluation Study, Dawczynski and coworkers found that while the dietary intake of vitamin D was below the recommendations in all diet groups (omnivore, flexitarian, vegetarian, and vegan), it was by far the lowest in vegans [70]. Schupbach et al. observed the same trend in Switzerland vegans, vegetarians, and omnivores [108]. Among Danish vegans, the intake of vitamin D, including supplements, did not reach the 2012 Nordic Nutrition Recommendation of 10 μg/day [109]. The lower levels of vitamin D intake among vegans are not surprising considering that animal foods are the major dietary sources of vitamin D. Nonetheless, vitamin D can also be synthesized in the skin post-sunlight exposure, consumed in fortified foods (plant milk, tofu, and orange juice), and it can be taken as a dietary supplement. Two forms of vitamin D supplements are available: vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). As ergocalciferol is produced in plants and fungi, it is always suitable for vegans, while cholecalciferol can be derived from either sheep wool (a nonvegan source) or lichen (a vegan-friendly source).
Vitamin D has a well-established neuroprotective effect in the central nervous system (CNS) [124]; therefore, its deficiency may potentially play a role in the development of AD. The neuroprotective role of vitamin D in the CNS could be due to several factors, including the upregulation of neurotrophic factor production, Aβ clearance, oxidative stress mechanisms, neuronal calcium homeostasis, and immune modulation [124]. Accordingly, low vitamin D concentrations in blood have been linked to cognitive impairment and dementia in observational studies [125,126,127]. Thus, a vitamin D deficiency associated with a vegan diet could be seen as a potential increasing factor for AD development [128] (Figure 2). This assumption is supported by several data in AD patients. When absorbed, vitamin D is transported to the liver where it is converted into 25-(OH)D, which can be measured in the blood. AD patients have lower serum 25(OH)D levels than healthy controls [129] and individuals with MCI [130]. In addition, MCI patients who develop AD suffer from significantly lower 25(OH)D levels compared to MCI patients who do not progress to AD [130]. The meta-analyses of prospective cohort studies on vitamin D concentration and dementia generally support the fact that there is an association between vitamin D deficiency and a higher risk of AD [126,127,128]. A recent umbrella review of observational studies and randomized controlled trials confirmed the finding that lower concentrations of vitamin D were indeed associated with a higher risk for AD [125]. Furthermore, this association seems to be stronger in the case of a severe vitamin D deficiency (<25 ng/mL) as compared to a moderate vitamin D insufficiency (25–49.9 ng/mL), suggesting the possibility of a dose–response association between serum 25(OH)D and the risk of AD or dementia [126,128,131].
4.3. Omega-3 Polyunsaturated Fatty Acids Deficiency
α-linolenic (ALA), eicosapentaenoic (EPA), and docosahexaenoic acids (DHA), classified as omega-3 fatty polyunsaturated acids (n-3 PUFAs), constitute the primary source of fat in a vegan diet [35,60,132,133]. The essential fatty acid ALA is the most prevalent plant-based source. EPA and DHA, however, occur primarily in seafood and fish oil, making them likely to be of concern to vegans. EPA and DHA can be converted from ALA and thus are not considered essential. However, many factors influence the relationship between the n-3 diet intake, bioavailability, and conversion [134]. Humans generally convert ALA into DHA and EPA poorly [135]. Most studies indicate that vegans have low or no dietary intakes of DHA or EPA [36,132,134]; however, the clinical significance of this is unknown. Vegetarians do not exhibit clinical signs of a DHA deficiency [136]. Because plant-based sources of EPA and DHA are lacking, vegans must rely mainly on endogenous synthesis for long-chain omega-3 PUFAs or supplement with algae oil capsules.
The positive effects of n-3 PUFAs on AD may be due to various mechanisms—an increasing clearance of Aβ, increasing neurotrophic and neuroprotective factors, and anti-inflammatory mechanisms [137]. N-3 PUFAs are precursors of specialized pro-resolving mediators (SPMs) that act as powerful anti-inflammatory agents [138]. In AD, the ability of peripheral blood mononuclear cells to make SPMs decreases over time [139]. The levels of SPMs are reduced in the cerebrospinal fluid samples of AD patients and positively correlate with MMSE scores [140], indicating that deficient SPM production may contribute to cognitive decline in AD. Six months of n-3 PUFAs supplementation is able to prevent this reduction in SPMs production in AD patients [139]. Transthyretin is a protein that binds Aβ and inhibits its toxicity. In a 12-month long randomized controlled trial, n-3 PUFAs supplementation was found to increase plasma transthyretin in AD patients [141]. Through its ability to shift the proportion of amyloidogenic and non-amyloidogenic amyloid precursor protein processing to non-amyloidogenic processing, DHA effectively reduces the Aβ generation and release [142]. In addition, n-3 PUFAs have also been reported to stimulate the Aβ42 phagocytosis and the production of the brain-derived neurotrophic factor while simultaneously suppressing the expression of pro-inflammatory cytokines in vitro [143].
The effects of DHA on mental and cognitive function are particularly important. It has been reported that patients with AD have lower levels of DHA in the serum [144]. Among patients with AD receiving acetylcholinesterase inhibitors, lower blood n-3 PUFAs levels, particularly DHA, were associated with a higher cognitive decline risk [145]. Some studies have demonstrated a correlation between higher blood levels of DHA and a reduced AD risk [146,147], while others have not [148,149]. The response to DHA interventions can be heterogeneous, depending on both the DHA level and cognitive status at baseline. N-3 PUFAs consumption is associated with a lower risk of dementia and a reduced likelihood of cognitive decline in patients with early-stage AD; however, it does not seem to provide any cognitive benefits in patients with late-stage AD [150,151,152,153]. A three-year investigation of n-3 PUFAs supplementation did not show significant improvements in cognitive decline in older people with memory complaints overall [154], but there were significant benefits in those with a low omega-3 status at baseline [155], suggesting that individuals with a low omega-3 index, such as vegans, may especially benefit from n-3 PUFAs supplementation. However, there is some evidence that a well-planned vegan diet with sufficient sources of ALA, including walnuts, flax seeds, chia seeds, and leafy green vegetables, might be sufficient for good mental health [156]. There is some evidence that vegetarians have a lower risk of dementia [157] and no evidence about the association of a vegan diet with dementia.
The use of DHA and EPA supplements is currently recommended in vegans; however, the entitlement of this recommendation requires more research, especially concerning possible side effects because there is some evidence that higher plasma n-3 PUFAs levels are associated with an increased prostate cancer risk [158].
5. Conclusions and Future Directions
A growing number of people are choosing to reduce or eliminate animal products from their diet. Given that AD pathology is strongly associated with diabetes, obesity, insulin resistance, or cardiovascular diseases, preventative strategies such as nutritional interventions may help reduce the risk of AD. However, large-scale, long-term research is needed to verify this effect, and the vegan diet has not yet been studied for its long-term effects. The possible advantage of a vegan diet lowering the chances of developing AD has been studied primarily through observational studies. Because of this, it is difficult to draw definitive conclusions about whether the benefits are directly attributable to the vegan diet. Moreover, there is the possibility that the beneficial effects of a vegan diet could be counterbalanced by the lack of specific nutrients.
Vegan diets lack specific vitamins and micronutrients and may result in some nutritional deficiencies. Vegans not supplementing micronutrients are more prone to vitamin B12, vitamin D, and DHA deficiencies, which have been linked to AD. Conversely, a vegan diet includes low levels of saturated fats and cholesterol, contributing to a healthy blood lipid profile. Furthermore, it is rich in phytonutrients, such as vitamins, antioxidants, and dietary fiber, that may help prevent cognitive decline.
Do the shortcomings overshadow the positive nutritional aspects of an animal product-free lifestyle? Whether vegan or nonvegan, any dietary practice can be detrimental to health if essential nutrients are not consumed appropriately. Vegan diets are followed for a variety of reasons, and this may affect the quality of the diet, which in turn affects brain health. The availability of highly processed vegan foods has increased, making it possible to eat a vegan diet without eating much whole-plant food. To reap the benefits of veganism, consuming a balanced diet with a wide variety of foods is essential. Ultimately, vegan diets must be closely monitored and supplemented, but they can provide adequate nutrition for all stages of life when planned carefully.
The data available to date do not allow an assessment of whether strict veganism is beneficial for brain health or AD risk compared with vegetarianism or diets with occasional meat consumption. Increasing plant-based foods may positively affect cognitive health and perhaps prevent AD. However, it is difficult to find evidence of the effects of a strictly vegan diet on cognition. Plant-based diets have a more extensive body of research that indicates protective effects on brain health. Further, it is unclear if the beneficial health effects are due to the avoidance of harmful effects associated with excessive calories and meat consumption, the specific dietary nutrients and bioactive compounds found in plants, or a combination of both. Randomized controlled trials and prospective cohort studies comparing veganism to other popular diets are scarce. The evidence provided in this review indicates that the net effect of a vegan diet on AD prevention and/or progression should be ascertained by taking into account all the positive and negative effects described here. It is advised that future studies on a vegan diet in AD should include supplementation with specific micronutrients to optimize any positive effects.
Author Contributions
Conceptualization, F.A., J.H. and A.K.; Writing—Original Draft Preparation, F.A. and A.K.; Writing—Review and Editing, F.A., A.K., K.S., J.A. and J.H.; Funding Acquisition, F.A. and J.H. Authors aimed to provide an unbiased overview of the topic and therefore the team included vegans (A.K.), vegetarians (K.S.), flexitarians (J.A.), and omnivores (F.A. and J.H.). All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by IPE 2. LF UK Grant No. 6980382 and by the National Institute for Neurological Research (Programme EXCELES, ID Project No. LX22NPO5107)—Funded by the European Union—Next Generation EU. The sponsors had no role in the design, execution, interpretation, or writing of the study.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Share of Vegans in European Countries. 2021. Available online: https://www.statista.com/forecasts/1256518/share-of-vegans-in-european-countries/ (accessed on 31 August 2022).
- Springmann, M.; Wiebe, K.; Mason-D’Croz, D.; Sulser, T.B.; Rayner, M.; Scarborough, P. Health and Nutritional Aspects of Sustainable Diet Strategies and Their Association with Environmental Impacts: A Global Modelling Analysis with Country-Level Detail. Lancet Planet. Health 2018, 2, e451–e461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reasons for Being Vegan in Europe. 2019. Available online: https://www.statista.com/statistics/1263270/survey-reasons-for-being-vegan-in-europe/ (accessed on 31 August 2022).
- Miki, A.J.; Livingston, K.A.; Karlsen, M.C.; Folta, S.C.; McKeown, N.M. Using Evidence Mapping to Examine Motivations for Following Plant-Based Diets. Curr. Dev. Nutr. 2020, 4, nzaa013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T.; et al. Estimation of the Global Prevalence of Dementia in 2019 and Forecasted Prevalence in 2050: An Analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, J.; Laurin, D.; Verreault, R.; Hébert, R.; Helliwell, B.; Hill, G.B.; McDowell, I. Risk factors for Alzheimer’s disease: A Prospective Analysis from the Canadian Study of Health and Aging. Am. J. Epidemiol. 2002, 156, 445–453. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Katzman, R.; Salmon, D.; Jin, H.; Cai, G.; Wang, Z.; Qu, G.; Grant, I.; Yu, E.; Levy, P.; et al. The prevalence of dementia and Alzheimer’s disease in Shanghai, China: Impact of age, gender, and education. Ann. Neurol. 1990, 27, 428–437. [Google Scholar] [CrossRef]
- Brookmeyer, R.; Evans, D.A.; Hebert, L.; Langa, K.M.; Heeringa, S.G.; Plassman, B.L.; Kukull, W.A. National estimates of the prevalence of Alzheimer’s disease in the United States. Alzheimer’s Dement. 2011, 7, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Green, R.C.; Cupples, L.A.; Kurz, A.; Auerbach, S.; Go, R.; Sadovnick, D.; Duara, R.; Kukull, W.A.; Chui, H.; Edeki, T.; et al. Depression as a Risk Factor for Alzheimer Disease. Arch. Neurol. 2003, 60, 753–759. [Google Scholar] [CrossRef] [Green Version]
- Ownby, R.L.; Crocco, E.; Acevedo, A.; John, V.; Loewenstein, D. Depression and Risk for Alzheimer Disease. Arch. Gen. Psychiatry 2006, 63, 530. [Google Scholar] [CrossRef] [Green Version]
- Cantón-Habas, V.; Rich-Ruiz, M.; Romero-Saldaña, M.; Carrera-González, M.D.P. Depression as a Risk Factor For Dementia and Alzheimer’s Disease. Biomedicines 2020, 8, 457. [Google Scholar] [CrossRef]
- Lennon, M.J.; Makkar, S.R.; Crawford, J.D.; Sachdev, P.S. Midlife Hypertension and Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2019, 71, 307–316. [Google Scholar] [CrossRef]
- Rajan, K.B.; Barnes, L.L.; Wilson, R.S.; Weuve, J.; McAninch, E.A.; Evans, D.A. Blood Pressure and Risk of Incident Alzheimer’s Disease Dementia by Antihypertensive Medications and APOE Ε4 Allele. Ann. Neurol. 2018, 83, 935–944. [Google Scholar] [CrossRef]
- Kivipelto, M.; Helkala, E.L.; Laakso, M.P.; Hänninen, T.; Hallikainen, M.; Alhainen, K.; Iivonen, S.; Mannermaa, A.; Tuomilehto, J.; Nissinen, A.; et al. Apolipoprotein E Epsilon4 Allele, Elevated Midlife Total Cholesterol Level, and High Midlife Systolic Blood Pressure Are Independent Risk Factors for Late-Life Alzheimer Disease. Ann. Intern. Med. 2002, 137, 149–155. [Google Scholar] [CrossRef]
- Huang, C.C.; Chung, C.M.; Leu, H.B.; Lin, L.Y.; Chiu, C.C.; Hsu, C.Y.; Chiang, C.H.; Huang, P.H.; Chen, T.J.; Lin, S.J.; et al. Diabetes Mellitus and the Risk of Alzheimer’s Disease: A Nationwide Population-Based Study. PLoS ONE 2014, 9, e87095. [Google Scholar] [CrossRef] [PubMed]
- Profenno, L.A.; Porsteinsson, A.P.; Faraone, S.V. Meta-Analysis of Alzheimer’s Disease Risk with Obesity, Diabetes, and Related Disorders. Biol. Psychiatry 2010, 67, 505–512. [Google Scholar] [CrossRef]
- Arvanitakis, Z.; Wilson, R.S.; Bienias, J.L.; Evans, D.A.; Bennett, D.A. Diabetes Mellitus and Risk of Alzheimer Disease and Decline in Cognitive Function. Arch. Neurol. 2004, 61, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Hassing, L.B.; Dahl, A.K.; Thorvaldsson, V.; Berg, S.; Gatz, M.; Pedersen, N.L.; Johansson, B. Overweight in Midlife and Risk of Dementia: A 40-Year Follow-Up Study. Int. J. Obes. 2009, 33, 893–898. [Google Scholar] [CrossRef] [Green Version]
- Razay, G.; Vreugdenhil, A. Obesity in Middle Age and Future Risk of Dementia: Midlife Obesity Increases Risk of Future Dementia. BMJ 2005, 331, 455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivipelto, M.; Ngandu, T.; Fratiglioni, L.; Viitanen, M.; Kåreholt, I.; Winblad, B.; Helkala, E.L.; Tuomilehto, J.; Soininen, H.; Nissinen, A. Obesity and Vascular Risk Factors at Midlife and the Risk of Dementia and Alzheimer Disease. Arch. Neurol. 2005, 62, 1556–1560. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol. Med. 2008, 39, 3–11. [Google Scholar] [CrossRef]
- Beckett, M.W.; Ardern, C.I.; Rotondi, M.A. A meta-analysis of prospective studies on the role of physical activity and the prevention of Alzheimer’s disease in older adults. BMC Geriatr. 2015, 15, 9. [Google Scholar] [CrossRef]
- Stern, Y.; Gurland, B.; Tatemichi, T.K.; Tang, M.X.; Wilder, D.; Mayeux, R. Influence of Education and Occupation on the Incidence of Alzheimer’s Disease. JAMA. 1994, 271, 1004–1010. [Google Scholar] [CrossRef]
- Samadi, M.; Moradi, S.; Moradinazar, M.; Mostafai, R.; Pasdar, Y. Dietary pattern in relation to the risk of Alzheimer’s disease: A systematic review. Neurol. Sci. 2019, 40, 2031–2043. [Google Scholar] [CrossRef]
- Pistollato, F.; Iglesias, R.C.; Ruiz, R.; Aparicio, S.; Crespo, J.; Lopez, L.D.; Manna, P.P.; Giampieri, F.; Battino, M. Nutritional Patterns Associated with the Maintenance of Neurocognitive Functions and the Risk of Dementia and Alzheimer’s Disease: A Focus on Human Studies. Pharmacol. Res. 2018, 131, 32–43. [Google Scholar] [CrossRef]
- Van Den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; Van De Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease—A Review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Barnes, L.L.; Bennett, D.A.; Aggarwal, N.T. MIND Diet Slows Cognitive Decline with Aging. Alzheimer’s Dement. 2015, 11, 1015–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND Diet Associated with Reduced Incidence of Alzheimer’s Disease. Alzheimer’s Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO European Office for the Prevention and Control of Noncommunicable Diseases. Plant-Based Diets and Their Impact on Health, Sustainability and the Environment: A Review of the Evidence; WHO Regional Office for Europe: Copenhagen, Denmark, 2021; pp. 1–11. [Google Scholar]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Richter, M.; Boeing, H.; Grünewald-Funk, D.; Heseker, H.; Kroke, A.; Leschik-Bonnet, E.; Oberritter, H.; Strohm, D.; Watzl, B. Vegan Diet. Position of the German Nutrition Society (DGE). Ernaehrungs Umsch. Int. 2016, 63, 92–102. [Google Scholar] [CrossRef]
- Pye, A.; Bash, K.; Joiner, A.; Beenstock, J. Good for the Planet and Good for Our Health: The Evidence for Whole-Food Plant-Based Diets. BJPsych Int. 2022, 19, 90–92. [Google Scholar] [CrossRef]
- Termannsen, A.D.; Clemmensen, K.K.B.; Thomsen, J.M.; Nørgaard, O.; Díaz, L.J.; Torekov, S.S.; Quist, J.S.; Færch, K. Effects of Vegan Diets on Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Obes. Rev. 2022, 23, e13462. [Google Scholar] [CrossRef]
- Selinger, E.; Neuenschwander, M.; Koller, A.; Gojda, J.; Kühn, T.; Schwingshackl, L.; Barbaresko, J.; Schlesinger, S. Evidence of a Vegan Diet for Health Benefits and Risks—An Umbrella Review of Meta-Analyses of Observational and Clinical Studies. Crit. Rev. Food Sci. Nutr. 2022. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Halloran, A.; Rippin, H.L.; Oikonomidou, A.C.; Dardavesis, T.I.; Williams, J.; Wickramasinghe, K.; Breda, J.; Chourdakis, M. Intake and Adequacy of the Vegan Diet. A Systematic Review of the Evidence. Clin. Nutr. 2021, 40, 3503–3521. [Google Scholar] [CrossRef] [PubMed]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2021, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Trefflich, I.; Menzel, J.; Obeid, R.; Longree, A.; Dierkes, J.; Meyer, K.; Herter-Aeberli, I.; Mai, K.; Stangl, G.I.; et al. Vitamin and Mineral Status in a Vegan Diet. Dtsch. Arztebl. Int. 2020, 117, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, J.; Cao, L.; Shi, M.; Liu, H.; Zhao, Y.; Xia, Y. Fruit and Vegetable Consumption and Cognitive Disorders in Older Adults: A Meta-Analysis of Observational Studies. Front. Nutr. 2022, 9, 871061. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; Walach, H. Fruit, Vegetables and Prevention of Cognitive Decline or Dementia: A Systematic Review of Cohort Studies. J. Nutr. Health Aging 2012, 16, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Huang, J.; Song, D.; Deng, R.; Wei, J.; Zhang, Z. Increased Consumption of Fruit and Vegetables Is Related to a Reduced Risk of Cognitive Impairment and Dementia: Meta-Analysis. Front. Aging Neurosci. 2017, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Fieldhouse, J.L.P.; Doorduijn, A.S.; de Leeuw, F.A.; Verhaar, B.J.H.; Koene, T.; Wesselman, L.M.P.; de van der Schueren, M.; Visser, M.; van de Rest, O.; Scheltens, P.; et al. A Suboptimal Diet Is Associated with Poorer Cognition: The NUDAD Project. Nutrients 2020, 12, 703. [Google Scholar] [CrossRef] [Green Version]
- Collins, A.E.; Saleh, T.M.; Kalisch, B.E. Naturally Occurring Antioxidant Therapy in Alzheimer’s Disease. Antioxidants 2022, 11, 213. [Google Scholar] [CrossRef]
- Heneka, M.T.; Golenbock, D.T.; Latz, E. Innate Immunity in Alzheimer’s Disease. Nat. Immunol. 2015, 16, 229–236. [Google Scholar] [CrossRef]
- Su, C.; Zhao, K.; Xia, H.; Xu, Y. Peripheral Inflammatory Biomarkers in Alzheimer’s Disease and Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Psychogeriatrics 2019, 19, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Passamonti, L.; Tsvetanov, K.A.; Jones, P.S.; Bevan-Jones, W.R.; Arnold, R.; Borchert, R.J.; Mak, E.; Su, L.; O’Brien, J.T.; Rowe, J.B. Neuroinflammation and Functional Connectivity in Alzheimer’s Disease: Interactive Influences on Cognitive Performance. J. Neurosci. 2019, 39, 7218–7226. [Google Scholar] [CrossRef] [Green Version]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary Pattern Analysis and Biomarkers of Low-Grade Inflammation: A Systematic Literature Review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- Menzel, J.; Biemann, R.; Longree, A.; Isermann, B.; Mai, K.; Schulze, M.B.; Abraham, K.; Weikert, C. Associations of a Vegan Diet with Inflammatory Biomarkers. Sci. Rep. 2020, 10, 1933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šebeková, K.; Krajčovičová-Kudláčková, M.; Schinzel, R.; Faist, V.; Klvanová, J.; Heidland, A. Plasma Levels of Advanced Glycation End Products in Healthy, Long-Term Vegetarians and Subjects on a Western Mixed Diet. Eur. J. Nutr. 2001, 40, 275–281. [Google Scholar] [CrossRef]
- Franco-De-Moraes, A.C.; De Almeida-Pititto, B.; Da Rocha Fernandes, G.; Gomes, E.P.; Da Costa Pereira, A.; Ferreira, S.R.G. Worse Inflammatory Profile in Omnivores than in Vegetarians Associates with the Gut Microbiota Composition. Diabetol. Metab. Syndr. 2017, 9, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutliffe, J.T.; Wilson, L.D.; de Heer, H.D.; Foster, R.L.; Carnot, M.J. C-Reactive Protein Response to a Vegan Lifestyle Intervention. Complement. Ther. Med. 2015, 23, 32–37. [Google Scholar] [CrossRef]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. Elevated C-Reactive Protein Levels in Overweight and Obese Adults. JAMA 1999, 282, 2131–2135. [Google Scholar] [CrossRef] [Green Version]
- Menzel, J.; Jabakhanji, A.; Biemann, R.; Mai, K.; Abraham, K.; Weikert, C. Systematic Review and Meta-Analysis of the Associations of Vegan and Vegetarian Diets with Inflammatory Biomarkers. Sci. Rep. 2020, 10, 21736. [Google Scholar] [CrossRef]
- Chen, H.; Du, Y.; Liu, S.; Ge, B.; Ji, Y.; Huang, G. Association between Serum Cholesterol Levels and Alzheimer’s Disease in China: A Case-Control Study. Int. J. Food Sci. Nutr. 2019, 70, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Marcum, Z.A.; Walker, R.; Bobb, J.F.; Sin, M.K.; Gray, S.L.; Bowen, J.D.; McCormick, W.; McCurry, S.M.; Crane, P.K.; Larson, E.B. Serum Cholesterol and Incident Alzheimer’s Disease: Findings from the Adult Changes in Thought Study. J. Am. Geriatr. Soc. 2018, 66, 2344–2352. [Google Scholar] [CrossRef]
- Rantanen, K.K.; Strandberg, A.Y.; Pitkälä, K.; Tilvis, R.; Salomaa, V.; Strandberg, T.E. Cholesterol in Midlife Increases the Risk of Alzheimer’s Disease during an up to 43-Year Follow-Up. Eur. Geriatr. Med. 2014, 5, 390–393. [Google Scholar] [CrossRef]
- Helzner, E.P.; Luchsinger, J.A.; Scarmeas, N.; Cosentino, S.; Brickman, A.M.; Glymour, M.M.; Stern, Y. Contribution of Vascular Risk Factors to the Progression in Alzheimer Disease. Arch. Neurol. 2009, 66, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, Vegan Diets and Multiple Health Outcomes: A Systematic Review with Meta-Analysis of Observational Studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef] [PubMed]
- Appleby, P.N.; Davey, G.K.; Key, T.J. Hypertension and Blood Pressure among Meat Eaters, Fish Eaters, Vegetarians and Vegans in EPIC–Oxford. Public Health Nutr. 2002, 5, 645–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollakova, D.; Andreadi, A.; Pacifici, F.; Della-Morte, D.; Lauro, D.; Tubili, C. The Impact of Vegan Diet in the Prevention and Treatment of Type 2 Diabetes: A Systematic Review. Nutrients 2021, 13, 2123. [Google Scholar] [CrossRef] [PubMed]
- Elorinne, A.L.; Alfthan, G.; Erlund, I.; Kivimäki, H.; Paju, A.; Salminen, I.; Turpeinen, U.; Voutilainen, S.; Laakso, J. Food and Nutrient Intake and Nutritional Status of Finnish Vegans and Non-Vegetarians. PLoS ONE 2016, 11, e0148235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.A.; Keogh, J.B.; Clifton, P.M. Polyphenols and Glycemic Control. Nutrients 2016, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Ylönen, K.; Saloranta, C.; Kronberg-Kippilä, C.; Groop, L.; Aro, A.; Virtanen, S.M. Associations of Dietary Fiber with Glucose Metabolism in Nondiabetic Relatives of Subjects with Type 2 Diabetes: The Botnia Dietary Study. Diabetes Care 2003, 26, 1979–1985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahleova, H.; Petersen, K.F.; Shulman, G.I.; Alwarith, J.; Rembert, E.; Tura, A.; Hill, M.; Holubkov, R.; Barnard, N.D. Effect of a Low-Fat Vegan Diet on Body Weight, Insulin Sensitivity, Postprandial Metabolism, and Intramyocellular and Hepatocellular Lipid Levels in Overweight Adults: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e2025454. [Google Scholar] [CrossRef] [PubMed]
- Bairamian, D.; Sha, S.; Rolhion, N.; Sokol, H.; Dorothée, G.; Lemere, C.A.; Krantic, S. Microbiota in Neuroinflammation and Synaptic Dysfunction: A Focus on Alzheimer’s Disease. Mol. Neurodegener. 2022, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- Lazar, E.; Sherzai, A.; Adeghate, J.; Sherzai, D. Gut Dysbiosis, Insulin Resistance and Alzheimer’s Disease: Review of a Novel Approach to Neurodegeneration. Front. Biosci. (Schol. Ed.) 2021, 13, 17–29. [Google Scholar] [CrossRef]
- Liu, S.; Gao, J.; Zhu, M.; Liu, K.; Zhang, H.L. Gut Microbiota and Dysbiosis in Alzheimer’s Disease: Implications for Pathogenesis and Treatment. Mol. Neurobiol. 2020, 57, 5026–5043. [Google Scholar] [CrossRef]
- Vogt, N.M.; Kerby, R.L.; Dill-McFarland, K.A.; Harding, S.J.; Merluzzi, A.P.; Johnson, S.C.; Carlsson, C.M.; Asthana, S.; Zetterberg, H.; Blennow, K.; et al. Gut Microbiome Alterations in Alzheimer’s Disease. Sci. Rep. 2017, 7, 13537. [Google Scholar] [CrossRef] [Green Version]
- Angelucci, F.; Cechova, K.; Amlerova, J.; Hort, J. Antibiotics, Gut Microbiota, and Alzheimer’s Disease. J. Neuroinflamm. 2019, 16, 108. [Google Scholar] [CrossRef] [Green Version]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet Rapidly and Reproducibly Alters the Human Gut Microbiome. Nature 2013, 505, 559–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawczynski, C.; Weidauer, T.; Richert, C.; Schlattmann, P.; Dawczynski, K.; Kiehntopf, M. Nutrient Intake and Nutrition Status in Vegetarians and Vegans in Comparison to Omnivores—The Nutritional Evaluation (NuEva) Study. Front. Nutr. 2022, 9, 819106. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.W.; Yi, C.H.; Liu, T.T.; Lei, W.Y.; Hung, J.S.; Lin, C.L.; Lin, S.Z.; Chen, C.L. Impact of Vegan Diets on Gut Microbiota: An Update on the Clinical Implications. Tzu-Chi Med. J. 2018, 30, 200–203. [Google Scholar] [CrossRef]
- Tomova, A.; Bukovsky, I.; Rembert, E.; Yonas, W.; Alwarith, J.; Barnard, N.D.; Kahleova, H. The Effects of Vegetarian and Vegan Diets on Gut Microbiota. Front. Nutr. 2019, 6, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohnert, E.; Kreutz, C.; Binder, N.; Hannibal, L.; Gorkiewicz, G.; Müller, A.; Storz, M.A.; Huber, R.; Lederer, A.K. Changes in Gut Microbiota after a Four-Week Intervention with Vegan vs. Meat-Rich Diets in Healthy Participants: A Randomized Controlled Trial. Microorganisms 2021, 9, 727. [Google Scholar] [CrossRef] [PubMed]
- D’Argenio, V.; Veneruso, I.; Gong, C.; Cecarini, V.; Bonfili, L.; Eleuteri, A.M. Gut Microbiome and Mycobiome Alterations in an In Vivo Model of Alzheimer’s Disease. Genes 2022, 13, 1564. [Google Scholar] [CrossRef] [PubMed]
- Ling, Z.; Zhu, M.; Yan, X.; Cheng, Y.; Shao, L.; Liu, X.; Jiang, R.; Wu, S. Structural and Functional Dysbiosis of Fecal Microbiota in Chinese Patients With Alzheimer’s Disease. Front. Cell Dev. Biol. 2021, 8, 634069. [Google Scholar] [CrossRef] [PubMed]
- Prochazkova, M.; Budinska, E.; Kuzma, M.; Pelantova, H.; Hradecky, J.; Heczkova, M.; Daskova, N.; Bratova, M.; Modos, I.; Videnska, P.; et al. Vegan Diet Is Associated With Favorable Effects on the Metabolic Performance of Intestinal Microbiota: A Cross-Sectional Multi-Omics Study. Front. Nutr. 2022, 8, 783302. [Google Scholar] [CrossRef]
- Losno, E.A.; Sieferle, K.; Armando Perez-Cueto, F.J.; Ritz, C.; Losno, C.; Sieferle, E.A.; Perez-Cueto, K.; Ritz, F.J.A. Vegan Diet and the Gut Microbiota Composition in Healthy Adults. Nutrients 2021, 13, 2402. [Google Scholar] [CrossRef] [PubMed]
- Qian, X.H.; Xie, R.Y.; Liu, X.L.; Chen, S.D.; Tang, H.D. Mechanisms of Short-Chain Fatty Acids Derived from Gut Microbiota in Alzheimer’s Disease. Aging Dis. 2022, 13, 1252. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Han, Y.; Zheng, Z.; Peng, G.; Liu, P.; Yue, S.; Zhu, S.; Chen, J.; Lv, H.; Shao, L.; et al. Altered Gut Microbial Metabolites in Amnestic Mild Cognitive Impairment and Alzheimer’s Disease: Signals in Host–Microbe Interplay. Nutrients 2021, 13, 228. [Google Scholar] [CrossRef]
- Trefflich, I.; Dietrich, S.; Braune, A.; Abraham, K.; Weikert, C. Short-and Branched-Chain Fatty Acids as Fecal Markers for Microbiota Activity in Vegans and Omnivores. Nutrients 2021, 13, 1808. [Google Scholar] [CrossRef]
- Wu, G.D.; Compher, C.; Chen, E.Z.; Smith, S.A.; Shah, R.D.; Bittinger, K.; Chehoud, C.; Albenberg, L.G.; Nessel, L.; Gilroy, E.; et al. Comparative Metabolomics in Vegans and Omnivores Reveal Constraints on Diet-Dependent Gut Microbiota Metabolite Production. Gut 2016, 65, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Reiss, A.; Jacobi, M.; Rusch, K.; Andreas, S. Association of Dietary Type with Fecal Microbiota and Short Chain Fatty Acids in Vegans and Omnivores. J. Int. Soc. Microbiota 2016, 1, 1–19. [Google Scholar] [CrossRef]
- De Filippis, F.; Pellegrini, N.; Vannini, L.; Jeffery, I.B.; La Storia, A.; Laghi, L.; Serrazanetti, D.I.; Di Cagno, R.; Ferrocino, I.; Lazzi, C.; et al. High-Level Adherence to a Mediterranean Diet Beneficially Impacts the Gut Microbiota and Associated Metabolome. Gut 2016, 65, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, A.; Cattane, N.; Galluzzi, S.; Provasi, S.; Lopizzo, N.; Festari, C.; Ferrari, C.; Guerra, U.P.; Paghera, B.; Muscio, C.; et al. Association of Brain Amyloidosis with Pro-Inflammatory Gut Bacterial Taxa and Peripheral Inflammation Markers in Cognitively Impaired Elderly. Neurobiol. Aging 2017, 49, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Gentile, C.L.; Weir, T.L. The Gut Microbiota at the Intersection of Diet and Human Health. Science 2018, 362, 776–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, D.S.; Yip, C.M.; Huang, T.H.J.; Chakrabartty, A.; Fraser, P.E. Manipulating the amyloid-β aggregation pathway with chemical chaperones. JBC 1999, 274, 32970–32974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogt, N.M.; Romano, K.A.; Darst, B.F.; Engelman, C.D.; Johnson, S.C.; Carlsson, C.M.; Asthana, S.; Blennow, K.; Zetterberg, H.; Bendlin, B.B.; et al. The Gut Microbiota-Derived Metabolite Trimethylamine N-Oxide Is Elevated in Alzheimer’s Disease. Alzheimer’s Res. Ther. 2018, 10, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrona Cardoza, P.; Spillane, M.B.; Morales Marroquin, E. Alzheimer’s disease and gut microbiota: Does trimethylamine N-oxide (TMAO) play a role? Nutr. Rev. 2022, 8, 271–281. [Google Scholar] [CrossRef]
- Zarbock, K.R.; Han, J.H.; Singh, A.P.; Thomas, S.P.; Bendlin, B.B.; Denu, J.M.; Yu, J.-P.J.; Rey, F.E.; Ulland, T.K. Trimethylamine N-Oxide Reduces Neurite Density and Plaque Intensity in a Murine Model of Alzheimer’s Disease. J. Alzheimer’s Dis. 2022, 90, 585–597. [Google Scholar] [CrossRef]
- Li, D.; Ke, Y.; Zhan, R.; Liu, C.; Zhao, M.; Zeng, A.; Shi, X.; Ji, L.; Cheng, S.; Pan, B.; et al. Trimethylamine-N-oxide promotes brain aging and cognitive impairment in mice. Aging Cell. 2018, 17, e12768. [Google Scholar] [CrossRef]
- Gao, Q.; Wang, Y.; Wang, X.; Fu, S.; Zhang, X.; Wang, R.; Zhang, X. Decreased levels of circulating trimethylamine N-oxide alleviate cognitive and pathological deterioration in transgenic mice: A potential therapeutic approach for Alzheimer’s disease. Aging 2019, 11, 8642–8663. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.; Aulisa, G.; Marcon, D.; Rizzo, G. The Influence of Animal- or Plant-Based Diets on Blood and Urine Trimethylamine-N-Oxide (TMAO) Levels in Humans. Curr. Nutr. Rep. 2022, 11, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Argyridou, S.; Davies, M.J.; Biddle, G.J.H.; Bernieh, D.; Suzuki, T.; Dawkins, N.P.; Rowlands, A.V.; Khunti, K.; Smith, A.C.; Yates, T. Evaluation of an 8-Week Vegan Diet on Plasma Trimethylamine-N-Oxide and Postchallenge Glucose in Adults with Dysglycemia or Obesity. J. Nutr. 2021, 151, 1844–1853. [Google Scholar] [CrossRef] [PubMed]
- Koeth, R.A.; Wang, Z.; Levison, B.S.; Buffa, J.A.; Org, E.; Sheehy, B.T.; Britt, E.B.; Fu, X.; Wu, Y.; Li, L. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 2013, 19, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Obeid, R.; Awwad, H.M.; Keller, M.; Geisel, J. Trimethylamine-N-oxide and its biological variations in vegetarians. Eur. J. Nutr. 2017, 56, 2599–2609. [Google Scholar] [CrossRef]
- Jain, R.; Larsuphrom, P.; Degremont, A.; Latunde-Dada, G.O.; Philippou, E. Association between Vegetarian and Vegan Diets and Depression: A Systematic Review. Nutr. Bull. 2022, 47, 27–49. [Google Scholar] [CrossRef]
- Iguacel, I.; Huybrechts, I.; Moreno, L.A.; Michels, N. Vegetarianism and Veganism Compared with Mental Health and Cognitive Outcomes: A Systematic Review and Meta-Analysis. Nutr. Rev. 2021, 79, 361–381. [Google Scholar] [CrossRef]
- Link, L.B.; Hussaini, N.S.; Jacobson, J.S. Change in Quality of Life and Immune Markers after a Stay at a Raw Vegan Institute: A Pilot Study. Complement. Ther. Med. 2008, 16, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Sultana, B.; Anwar, F. Flavonols (kaempeferol, quercetin, myricetin) contents of selected fruits, vegetables and medicinal plants. Food Chem. 2008, 108, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Grewal, A.K.; Singh, T.G.; Sharma, D.; Sharma, V.; Singh, M.; Rahman, M.H.; Najda, A.; Walasek-Janusz, M.; Kamel, M.; Albadrani, G.M. Mechanistic Insights and Perspectives Involved in Neuroprotective Action of Quercetin. Biomed. Pharmacother. 2021, 140, 111729. [Google Scholar] [CrossRef]
- Dixon Clarke, S.E.; Ramsay, R.R. Dietary Inhibitors of Monoamine Oxidase A. J. Neural Transm. 2011, 118, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.W.; Chen, J.Y.; Ouyang, D.; Lu, J.H. Quercetin in animal models of Alzheimer’s disease: A systematic review of preclinical studies. Int. J. Mol. Sci. 2020, 21, 493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paula, P.C.; Maria, S.G.A.; Luis, C.H.; Patricia, C.G.G. Preventive effect of quercetin in a triple transgenic Alzheimer’s disease mice model. Molecules 2019, 24, 2287. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Parashar, A.; Udayabanu, M. Quercetin prevents chronic unpredictable stress induced behavioral dysfunction in mice by alleviating hippocampal oxidative and inflammatory stress. Physiol. Behav. 2017, 171, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Ke, F.; Li, H.R.; Chen, X.X.; Gao, X.R.; Huang, L.L.; Du, A.Q.; Jiang, C.; Li, H.; Ge, J.F. Quercetin alleviates LPS-induced depression-like behavior in rats via regulating BDNF-related imbalance of copine 6 and TREM1/2 in the hippocampus and PFC. Front. Pharmacol. 2020, 10, 544. [Google Scholar] [CrossRef] [Green Version]
- Taber, L.; Chiu, C.H.; Whelan, J. Assessment of the arachidonic acid content in foods commonly consumed in the American diet. Lipids 1998, 33, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Mądry, E.; Lisowska, A.; Grebowiec, P.; Walkowiak, J. The Impact of Vegan Diet on B-12 Status in Healthy Omnivores: Five-Year Prospective Study. Acta Sci. Pol. Technol. Aliment. 2012, 2, 209–212. [Google Scholar]
- Schüpbach, R.; Wegmüller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient Status and Intake in Omnivores, Vegetarians and Vegans in Switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef]
- Kristensen, N.B.; Madsen, M.L.; Hansen, T.H.; Allin, K.H.; Hoppe, C.; Fagt, S.; Lausten, M.S.; Gøbel, R.J.; Vestergaard, H.; Hansen, T.; et al. Intake of Macro- and Micronutrients in Danish Vegans. Nutr. J. 2015, 14, 115. [Google Scholar] [CrossRef] [Green Version]
- Rathod, R.; Kale, A.; Joshi, S. Novel Insights into the Effect of Vitamin B12 and Omega-3 Fatty Acids on Brain Function. J. Biomed. Sci. 2016, 23, 17. [Google Scholar] [CrossRef] [Green Version]
- Scalabrino, G. The multi-faceted basis of vitamin B12 (cobalamin) neurotrophism in adult central nervous system: Lessons learned from its deficiency. Prog. Neurobiol. 2009, 88, 203–220. [Google Scholar] [CrossRef]
- Vogiatzoglou, A.; Refsum, H.; Johnston, C.; Smith, S.M.; Bradley, K.M.; De Jager, C.; Budge, M.M.; Smith, A.D. Vitamin B12 status and rate of brain volume loss in community-dwelling elderly. Neurology 2008, 71, 826–832. [Google Scholar] [CrossRef]
- Tangney, C.C.; Aggarwal, N.T.; Li, H.; Wilson, R.S.; Decarli, C.; Evans, D.A.; Morris, M.C. Vitamin B12, cognition, and brain MRI measures: A cross-sectional examination. Neurology 2011, 77, 1773. [Google Scholar] [CrossRef] [Green Version]
- Jarquin Campos, A.; Risch, L.; Nydegger, U.; Wiesner, J.; Vazquez Van Dyck, M.; Renz, H.; Stanga, Z.; Risch, M. Diagnostic Accuracy of Holotranscobalamin, Vitamin B12, Methylmalonic Acid, and Homocysteine in Detecting B12 Deficiency in a Large, Mixed Patient Population. Dis. Markers 2020, 2020, 7468506. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhao, J.; Chang, H.; Liu, X.; Zhu, R. Homocysteine and Folic Acid: Risk Factors for Alzheimer’s Disease—An Updated Meta-Analysis. Front. Aging Neurosci. 2021, 13, 665114. [Google Scholar] [CrossRef] [PubMed]
- De Jager, C.A.; Oulhaj, A.; Jacoby, R.; Refsum, H.; Smith, A.D. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: A randomized controlled trial. Int. J. Ger. Psych. 2012, 27, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Smith, S.M.; de Jager, C.A.; Whitbread, P.; Johnston, C.; Agacinski, G.; Oulhaj, A.; Bradley, K.M.; Jacoby, R.; Refsum, H. Homocysteine-Lowering by B Vitamins Slows the Rate of Accelerated Brain Atrophy in Mild Cognitive Impairment: A Randomized Controlled Trial. PLoS ONE 2010, 5, e12244. [Google Scholar] [CrossRef] [Green Version]
- Douaud, G.; Refsum, H.; De Jager, C.A.; Jacoby, R.; Nichols, T.E.; Smith, S.M.; Smith, A.D. Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment. Proc. Natl. Acad. Sci. USA 2013, 110, 9523–9528. [Google Scholar] [CrossRef] [Green Version]
- Marques de Brito, B.; Campos, V. de M.; Neves, F.J.; Ramos, L.R.; Tomita, L.Y. Vitamin B12 Sources in Non-Animal Foods: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2022, 28, 1–15. [Google Scholar] [CrossRef]
- Nakos, M.; Pepelanova, I.; Beutel, S.; Krings, U.; Berger, R.G.; Scheper, T. Isolation and Analysis of Vitamin B12 from Plant Samples. Food Chem. 2017, 216, 301–308. [Google Scholar] [CrossRef]
- Lederer, A.K.; Hannibal, L.; Hettich, M.; Behringer, S.; Spiekerkoetter, U.; Steinborn, C.; Gründemann, C.; Zimmermann-Klemd, A.M.; Müller, A.; Simmet, T.; et al. Vitamin B12 Status Upon Short-Term Intervention with a Vegan Diet—A Randomized Controlled Trial in Healthy Participants. Nutrients 2019, 11, 2815. [Google Scholar] [CrossRef] [Green Version]
- Selinger, E.; Kühn, T.; Procházková, M.; Anděl, M.; Gojda, J. Vitamin B12 Deficiency Is Prevalent Among Czech Vegans Who Do Not Use Vitamin B12 Supplements. Nutrients 2019, 11, 3019. [Google Scholar] [CrossRef] [Green Version]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D Deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [Green Version]
- Kalueff, A.V.; Eremin, K.O.; Tuohimaa, P. Mechanisms of Neuroprotective Action of Vitamin D3. Biochemistry 2004, 69, 738–741. [Google Scholar] [CrossRef]
- Liu, D.; Meng, X.; Tian, Q.; Cao, W.; Fan, X.; Wu, L.; Song, M.; Meng, Q.; Wang, W.; Wang, Y. Vitamin D and Multiple Health Outcomes: An Umbrella Review of Observational Studies, Randomized Controlled Trials, and Mendelian Randomization Studies. Adv. Nutr. 2022, 13, 1044–1062. [Google Scholar] [CrossRef]
- Kalra, A.; Teixeira, A.L.; Diniz, B.S. Association of Vitamin D Levels with Incident All-Cause Dementia in Longitudinal Observational Studies: A Systematic Review and Meta-Analysis. J. Prev. Alzheimer’s Dis. 2020, 7, 14–20. [Google Scholar] [CrossRef]
- Shen, L.; Ji, H.F. Vitamin D Deficiency Is Associated with Increased Risk of Alzheimer’s Disease and Dementia: Evidence from Meta-Analysis. Nutr. J. 2015, 14, 76. [Google Scholar] [CrossRef] [Green Version]
- Chai, B.; Gao, F.; Wu, R.; Dong, T.; Gu, C.; Lin, Q.; Zhang, Y. Vitamin D Deficiency as a Risk Factor for Dementia and Alzheimer’s Disease: An Updated Meta-Analysis. BMC Neurol. 2019, 19, 284. [Google Scholar] [CrossRef]
- Annweiler, C.; Llewellyn, D.J.; Beauchet, O. Low Serum Vitamin D Concentrations in Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2013, 33, 659–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavraki, E.; Ioannidis, P.; Tripsianis, G.; Gioka, T.; Kolousi, M.; Vadikolias, K. Vitamin D in Mild Cognitive Impairment and Alzheimer’s Disease. A Study in Older Greek Adults. Hippokratia 2020, 24, 120–126. [Google Scholar]
- Jayedi, A.; Rashidy-Pour, A.; Shab-Bidar, S. Vitamin D Status and Risk of Dementia and Alzheimer’s Disease: A Meta-Analysis of Dose-Response†. Nutr. Neurosci. 2019, 22, 750–759. [Google Scholar] [CrossRef]
- Menzel, J.; Longree, A.; Abraham, K.; Schulze, M.B.; Weikert, C. Dietary and Plasma Phospholipid Profiles in Vegans and Omnivores—Results from the RBVD Study. Nutrients 2022, 14, 2900. [Google Scholar] [CrossRef] [PubMed]
- Sobiecki, J.G.; Appleby, P.N.; Bradbury, K.E.; Key, T.J. High Compliance with Dietary Recommendations in a Cohort of Meat Eaters, Fish Eaters, Vegetarians, and Vegans: Results from the European Prospective Investigation into Cancer and Nutrition-Oxford Study. Nutr. Res. 2016, 36, 464–477. [Google Scholar] [CrossRef] [Green Version]
- Lane, K.E.; Wilson, M.; Hellon, T.G.; Davies, I.G. Bioavailability and Conversion of Plant Based Sources of Omega-3 Fatty Acids—A Scoping Review to Update Supplementation Options for Vegetarians and Vegans. Crit. Rev. Food Sci. Nutr. 2022, 62, 4982–4997. [Google Scholar] [CrossRef]
- Burns-Whitmore, B.; Froyen, E.; Heskey, C.; Parker, T.; Pablo, G.S. Alpha-Linolenic and Linoleic Fatty Acids in the Vegan Diet: Do They Require Dietary Reference Intake/Adequate Intake Special Consideration? Nutrients 2019, 11, 2365. [Google Scholar] [CrossRef] [PubMed]
- Saunders, A.V.; Davis, B.C.; Garg, M.L. Omega-3 polyunsaturated fatty acids and vegetarian diets. Med. J. Aust. 2013, 19, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H. Effects of N-3 Polyunsaturated Fatty Acids on Dementia. J. Clin. Med. Res. 2017, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacobbe, J.; Benoiton, B.; Zunszain, P.; Pariante, C.M.; Borsini, A. The Anti-Inflammatory Role of Omega-3 Polyunsaturated Fatty Acids Metabolites in Pre-Clinical Models of Psychiatric, Neurodegenerative, and Neurological Disorders. Front. Psychiatry 2020, 11, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Hjorth, E.; Vedin, I.; Eriksdotter, M.; Freund-Levi, Y.; Wahlund, L.O.; Cederholm, T.; Palmblad, J.; Schultzberg, M. Effects of N-3 FA Supplementation on the Release of Proresolving Lipid Mediators by Blood Mononuclear Cells: The OmegAD Study. J. Lipid Res. 2015, 56, 674–681. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhu, M.; Hjorth, E.; Cortés-Toro, V.; Eyjolfsdottir, H.; Graff, C.; Nennesmo, I.; Palmblad, J.; Eriksdotter, M.; Sambamurti, K.; et al. Resolution of Inflammation Is Altered in Alzheimer’s Disease. Alzheimer’s Dement. 2015, 11, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Faxén-Irving, G.; Freund-Levi, Y.; Eriksdotter-Jönhagen, M.; Basun, H.; Hjorth, E.; Palmblad, J.; Vedin, I.; Cederholm, T.; Wahlund, L.O. Effects on Transthyretin in Plasma and Cerebrospinal Fluid by DHA-Rich n − 3 Fatty Acid Supplementation in Patients with Alzheimer’s Disease: The OmegAD Study. J. Alzheimer’s Dis. 2013, 36, 1–6. [Google Scholar] [CrossRef]
- Grimm, M.O.W.; Kuchenbecker, J.; Grosgen, S.; Burg, V.K.; Hundsdorfer, B.; Rothhaar, T.L.; Friess, P.; De Wilde, M.C.; Broersen, L.M.; Penke, B.; et al. Docosahexaenoic Acid Reduces Amyloid Beta Production via Multiple Pleiotropic Mechanisms. J. Biol. Chem. 2011, 286, 14028–14039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjorth, E.; Zhu, M.; Toro, V.C.; Vedin, I.; Palmblad, J.; Cederholm, T.; Freund-Levi, Y.; Faxen-Irving, G.; Wahlund, L.O.; Basun, H.; et al. Omega-3 Fatty Acids Enhance Phagocytosis of Alzheimer’s Disease-Related Amyloid-Β42 by Human Microglia and Decrease Inflammatory Markers. J. Alzheimer’s Dis. 2013, 35, 697–713. [Google Scholar] [CrossRef] [Green Version]
- Tully, A.M.; Roche, H.M.; Doyle, R.; Fallon, C.; Bruce, I.; Lawlor, B.; Coakley, D.; Gibney, M.J. Low Serum Cholesteryl Ester-Docosahexaenoic Acid Levels in Alzheimer’s Disease: A Case–Control Study. Br. J. Nutr. 2003, 89, 483–489. [Google Scholar] [CrossRef]
- Chu, C.S.; Hung, C.F.; Ponnusamy, V.K.; Chen, K.C.; Chen, N.C. Higher Serum DHA and Slower Cognitive Decline in Patients with Alzheimers Disease: Two-Year Follow-Up. Nutrients 2022, 14, 1159. [Google Scholar] [CrossRef]
- Sala-Vila, A.; Satizabal, C.L.; Tintle, N.; Melo van Lent, D.; Vasan, R.S.; Beiser, A.S.; Seshadri, S.; Harris, W.S. Red Blood Cell DHA Is Inversely Associated with Risk of Incident Alzheimer´s Disease and All-Cause Dementia: Framingham Offspring Study. Nutrients 2022, 14, 2408. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, E.J.; Bongard, V.; Beiser, A.S.; Lamon-Fava, S.; Robins, S.J.; Au, R.; Tucker, K.L.; Kyle, D.J.; Wilson, P.W.F.; Wolf, P.A. Plasma Phosphatidylcholine Docosahexaenoic Acid Content and Risk of Dementia and Alzheimer Disease: The Framingham Heart Study. Arch. Neurol. 2006, 63, 1545–1550. [Google Scholar] [CrossRef]
- Kröger, E.; Verreault, R.; Carmichael, P.H.; Lindsay, J.; Julien, P.; Dewailly, É.; Ayotte, P.; Laurin, D. Omega-3 Fatty Acids and Risk of Dementia: The Canadian Study of Health and Aging. Am. J. Clin. Nutr. 2009, 90, 184–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurin, D.; Verreault, R.; Lindsay, J.; Dewailly, É.; Holub, B.J. Omega-3 Fatty Acids and Risk of Cognitive Impairment and Dementia. J. Alzheimer’s Dis. 2003, 5, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.H.R.; Chappell, H.F.; Zulyniak, M.A. Dietary and Supplemental Long-Chain Omega-3 Fatty Acids as Moderators of Cognitive Impairment and Alzheimer’s Disease. Eur. J. Nutr. 2022, 61, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Araya-Quintanilla, F.; Gutiérrez-Espinoza, H.; Sánchez-Montoya, U.; Muñoz-Yañez, M.J.; Baeza-Vergara, A.; Petersen-Yanjarí, M.; Fernández-Lecaros, L. Effectiveness of Omega-3 Fatty Acid Supplementation in Patients with Alzheimer Disease: A Systematic Review and Meta-Analysis. Neurología (Engl. Ed.) 2020, 35, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.C.; Su, K.P.; Cheng, T.C.; Liu, H.C.; Chang, C.J.; Dewey, M.E.; Stewart, R.; Huang, S.Y. The Effects of Omega-3 Fatty Acids Monotherapy in Alzheimer’s Disease and Mild Cognitive Impairment: A Preliminary Randomized Double-Blind Placebo-Controlled Study. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2008, 32, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Freund-Levi, Y.; Eriksdotter-Jönhagen, M.; Cederholm, T.; Basun, H.; Faxén-Irving, G.; Garlind, A.; Vedin, I.; Vessby, B.; Wahlund, L.O.; Palmblad, J. Omega-3 Fatty Acid Treatment in 174 Patients with Mild to Moderate Alzheimer Disease: OmegAD Study: A Randomized Double-Blind Trial. Arch. Neurol. 2006, 63, 1402–1408. [Google Scholar] [CrossRef] [Green Version]
- Andrieu, S.; Guyonnet, S.; Coley, N.; Cantet, C.; Bonnefoy, M.; Bordes, S.; Bories, L.; Cufi, M.N.; Dantoine, T.; Dartigues, J.F.; et al. Effect of Long-Term Omega 3 Polyunsaturated Fatty Acid Supplementation with or without Multidomain Intervention on Cognitive Function in Elderly Adults with Memory Complaints (MAPT): A Randomised, Placebo-Controlled Trial. Lancet Neurol. 2017, 16, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Hooper, C.; de Souto Barreto, P.; Coley, N.; Cantet, C.; Cesari, M.; Andrieu, S.; Vellas, B. Cognitive Changes with Omega-3 Polyunsaturated Fatty Acids in Non-Demented Older Adults with Low Omega-3 Index. J. Nutr. Health Aging 2017, 21, 988–993. [Google Scholar] [CrossRef] [PubMed]
- Beezhold, B.L.; Johnston, C.S.; Daigle, D.R. Vegetarian diets are associated with healthy mood states: A cross-sectional study in Seventh Day Adventist adults. Nutr. J. 2010, 9, 26. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.-N.; Chiu, T.H.; Chang, C.-E.; Lin, M.-N. The Impact of a Plant-based Dietary Pattern on Dementia Risk: A Prospective Cohort Study. Innov. Aging 2019, 3, S734. [Google Scholar] [CrossRef]
- Brasky, T.M.; Darke, A.K.; Song, X.; Tangen, C.M.; Goodman, P.J.; Thompson, I.M.; Meyskens, F.L.; Goodman, G.E.; Minasian, L.M.; Parnes, H.L.; et al. Plasma Phospholipid Fatty Acids and Prostate Cancer Risk in the SELECT Trial. J. Natl. Cancer Inst. 2013, 105, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Proposed factors involved in the positive effects of a vegan diet in Alzheimer’s disease (AD). The intake of fruits and vegetables in a vegan diet is associated with a reduction in inflammatory processes and a normalization of the gut microbiota due to the high antioxidant, fiber, and polyphenol content. The absence of red meat also leads to a reduction in Trimethylamine N-Oxide (TMAO) in plasma and urine. These effects can counteract the development of AD pathology. Furthermore, the reduction in caloric intake reduces the risk of obesity and type 2 diabetes (T2DM), thus contributing to the prevention of AD, together with the reduced intake of saturated fatty acids (SFA).
Figure 1.
Proposed factors involved in the positive effects of a vegan diet in Alzheimer’s disease (AD). The intake of fruits and vegetables in a vegan diet is associated with a reduction in inflammatory processes and a normalization of the gut microbiota due to the high antioxidant, fiber, and polyphenol content. The absence of red meat also leads to a reduction in Trimethylamine N-Oxide (TMAO) in plasma and urine. These effects can counteract the development of AD pathology. Furthermore, the reduction in caloric intake reduces the risk of obesity and type 2 diabetes (T2DM), thus contributing to the prevention of AD, together with the reduced intake of saturated fatty acids (SFA).

Figure 2.
Proposed factors involved in the negative effects of a vegan diet in Alzheimer’s disease (AD). A vegan diet can easily lead to a deficiency in vitamins B12 and D if unsupplemented. Vitamin B12 deficiency accelerates cognitive decline, while a lack of vitamin D increases oxidative stress and Aβ and tau pathology. An insufficient intake of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), on the other hand, reduces brain glucose utilization. These factors can lead to the worsening of AD. Furthermore, these vitamin deficiencies lead to an increased risk of AD, both directly and indirectly (increase in plasma homocysteine levels).
Figure 2.
Proposed factors involved in the negative effects of a vegan diet in Alzheimer’s disease (AD). A vegan diet can easily lead to a deficiency in vitamins B12 and D if unsupplemented. Vitamin B12 deficiency accelerates cognitive decline, while a lack of vitamin D increases oxidative stress and Aβ and tau pathology. An insufficient intake of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), on the other hand, reduces brain glucose utilization. These factors can lead to the worsening of AD. Furthermore, these vitamin deficiencies lead to an increased risk of AD, both directly and indirectly (increase in plasma homocysteine levels).


{kind=link}
{kind=link}
{kind=link}
Table 1.
Modifiable and non-modifiable risk factors for Alzheimer’s disease.
| Non-Modifiable Risk Factors | Non-Modifiable Risk Factors |
|---|---|
| Advanced age [6,7,8] | Depression [9,10,11] |
| Gender [7,8] | Hypertension [12,13,14] |
| Genetic predisposition [26] | Diabetes [15,16,17] |
| Obesity [18,19,20] | |
| Physical inactivity [21,22] | |
| Low education [6,7,23] | |
| Unhealthy diet [24,25] |
Table 2.
Positive and negative effects of a vegan diet on Alzheimer’s disease.
| Positive Effects | Negative Effects |
|---|---|
| Reduction in systemic inflammation [49,50,52,76] | Increased risk of vitamin B12 deficiency [35,36,107] |
| Reduced risk of developing obesity [34] and type II diabetes [59] | Increased risk of vitamin D deficiency [70,108,109] |
| Reduction in TMAO levels in plasma and urine [92,93] | Insufficient intake of DHA and EPA [70] |
| Lower caloric intake and saturated fat intake compared to other types of diets [35,70] | |
| Decreased pro-inflammatory bacteria in the gut [77,84] | |
| Increased production of beneficial bacterially produced metabolites [76,81] |
TMAO: Trimethylamine N-Oxide; DHA: docosahexaenoic acid; EPA: eicosapentaenoic acid.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Katonova, A.; Sheardova, K.; Amlerova, J.; Angelucci, F.; Hort, J. Effect of a Vegan Diet on Alzheimer’s Disease. Int. J. Mol. Sci. 2022, 23, 14924. https://doi.org/10.3390/ijms232314924
AMA Style
Katonova A, Sheardova K, Amlerova J, Angelucci F, Hort J. Effect of a Vegan Diet on Alzheimer’s Disease. International Journal of Molecular Sciences. 2022; 23(23):14924. https://doi.org/10.3390/ijms232314924
Chicago/Turabian StyleKatonova, Alzbeta, Katerina Sheardova, Jana Amlerova, Francesco Angelucci, and Jakub Hort. 2022. "Effect of a Vegan Diet on Alzheimer’s Disease" International Journal of Molecular Sciences 23, no. 23: 14924. https://doi.org/10.3390/ijms232314924
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.