
Profiling of Tumour-Infiltrating Lymphocytes and Tumour-Associated Macrophages in Ovarian Epithelial Cancer—Relation to Tumour Characteristics and Impact on Prognosis
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Cellular Markers According to Histological Subtype, Stage and Grade of Disease
2.2. Comparison between TILs Expression in Borderline Ovarian Tumours versus Cancer
2.3. TIL Patterns in Patients Who Received Neoadjuvant Chemotherapy
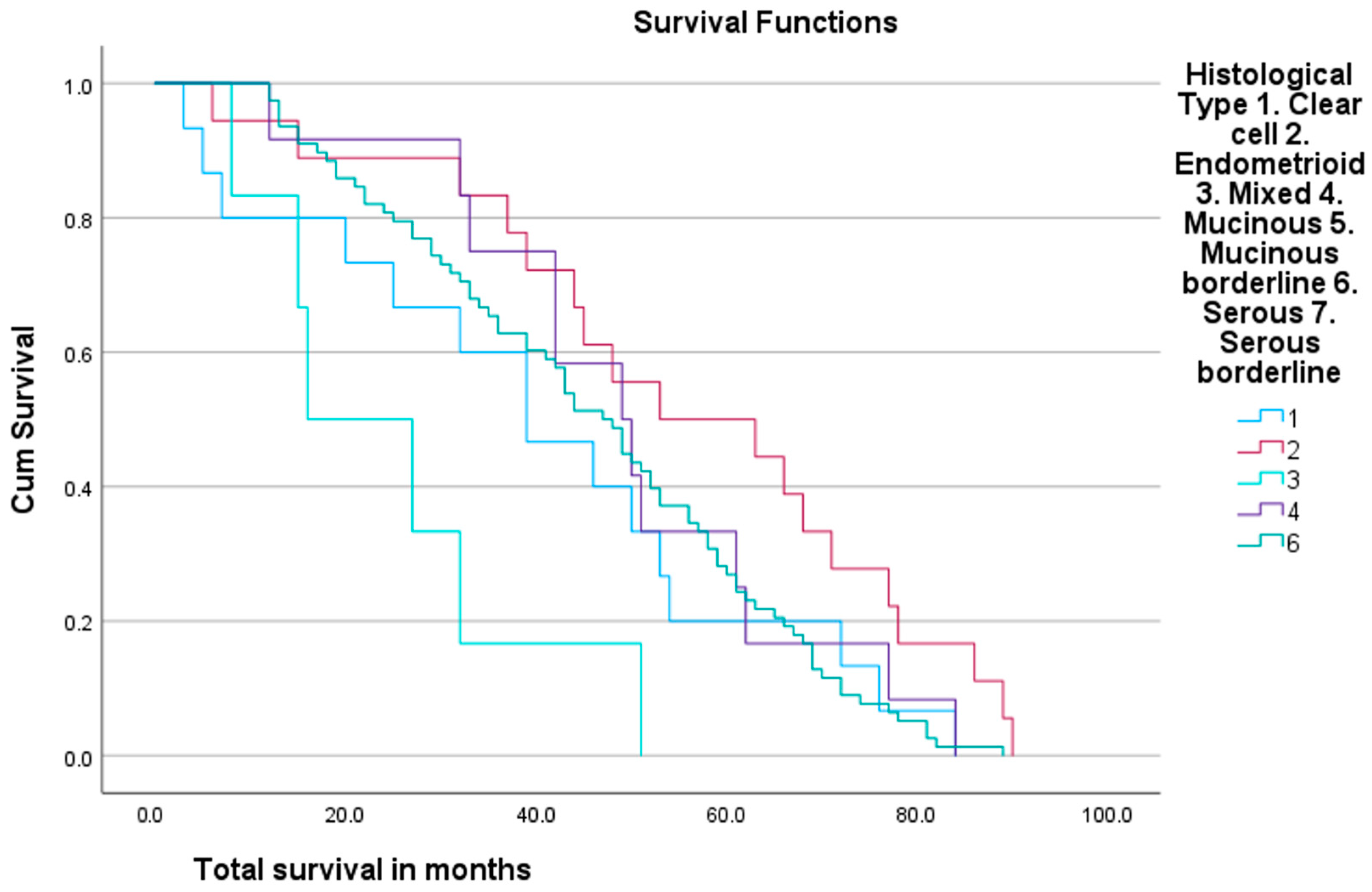
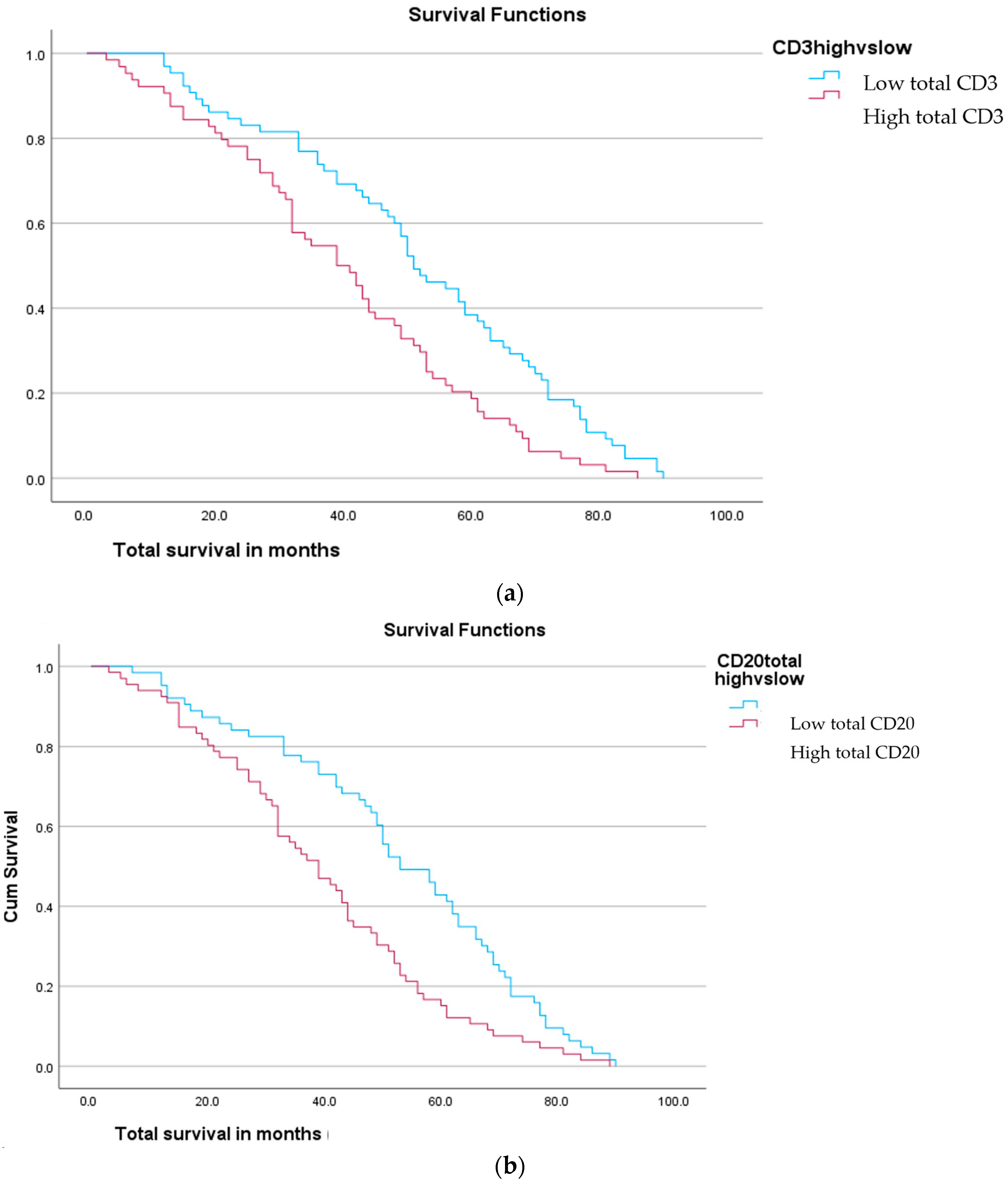
2.4. Survival
3. Discussion
4. Materials and Methods
Data Collection and Laboratory Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Office for National Statistics. Cancer Survival in England for Patients Diagnosed between 2014 and 2018, and Followed up Until 2019—GOV.UK. Available online: https://www.gov.uk/government/statistics/cancer-survival-in-england-for-patients-diagnosed-between-2014-and-2018-and-followed-up-until-2019 (accessed on 29 July 2022).
- Zhang, L.; Conejo-Garcia, J.R.; Katsaros, D.; Gimotty, P.A.; Massobrio, M.; Regnani, G.; Makrigiannakis, A.; Gray, H.; Schlienger, K.; Liebman, M.N.; et al. Intratumoral T Cells, Recurrence, and Survival in Epithelial Ovarian Cancer. N. Engl. J. Med. 2003, 348, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non-Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv. Anat. Pathol. 2017, 24, 311. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The Evaluation of Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259. [Google Scholar] [CrossRef]
- Bowtell, D.D.; Böhm, S.; Ahmed, A.A.; Aspuria, P.J.; Bast, R.C.; Beral, V.; Berek, J.S.; Birrer, M.J.; Blagden, S.; Bookman, M.A.; et al. Rethinking Ovarian Cancer II: Reducing Mortality from High-Grade Serous Ovarian Cancer. Nat. Rev. Cancer 2015, 15, 668. [Google Scholar] [CrossRef]
- Santoiemma, P.P.; Powell, D.J. Tumor Infiltrating Lymphocytes in Ovarian Cancer. Cancer Biol. Ther. 2015, 16, 807–820. [Google Scholar] [CrossRef]
- Macpherson, A.M.; Barry, S.C.; Ricciardelli, C.; Oehler, M.K. Epithelial Ovarian Cancer and the Immune System: Biology, Interactions, Challenges and Potential Advances for Immunotherapy. J. Clin. Med. 2020, 9, 2967. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, J.; Chen, R.; Bai, Y.; Lu, X. The Prognostic Value of Tumor-Infiltrating T Lymphocytes in Ovarian Cancer. Oncotarget 2017, 8, 15621–15631. [Google Scholar] [CrossRef]
- Cai, D.; Jin, L. Immune Cell Population in Ovarian Tumor Microenvironment. J. Cancer 2017, 8, 2915–2923. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Lee, H.; Jove, V.; Deng, J.; Zhang, W.; Liu, X.; Forman, S.; Dellinger, T.H.; Wakabayashi, M.; Yu, H.; et al. Prognostic significance of B-cells and pSTAT3 in patients with ovarian cancer. PLoS ONE 2013, 8, e54029. [Google Scholar] [CrossRef]
- Milne, K.; Köbel, M.; Kalloger, S.E.; Barnes, R.O.; Gao, D.; Gilks, C.B.; Watson, P.H.; Nelson, B.H. Systematic Analysis of Immune Infiltrates in High-Grade Serous Ovarian Cancer Reveals CD20, FoxP3 and TIA-1 as Positive Prognostic Factors. PLoS ONE 2009, 4, e6412. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, Y.; Yang, J.; Zhao, X.; Wei, X. Tumor Microenvironment in Ovarian Cancer: Function and Therapeutic Strategy. Front. Cell Dev. Biol. 2020, 8, 758. [Google Scholar] [CrossRef]
- Yuan, X.; Zhang, J.; Li, D.; Mao, Y.; Mo, F.; Du, W.; Ma, X. Prognostic significance of tumor-associated macrophages in ovarian cancer: A meta-analysis. Gynecol. Oncol. 2017, 147, 181–187. [Google Scholar] [CrossRef]
- Lan, C.; Huang, X.; Lin, S.; Huang, H.; Cai, Q.; Wan, T.; Lu, J.; Liu, J. Expression of M2-Polarized Macrophages Is Associated with Poor Prognosis for Advanced Epithelial Ovarian Cancer. Technol. Cancer Res. Treat. 2013, 12, 259–267. [Google Scholar] [CrossRef]
- Larionova, I.; Tuguzbaeva, G.; Ponomaryova, A.; Stakheyeva, M.; Cherdyntseva, N.; Pavlov, V.; Choinzonov, E.; Kzhyshkowska, J. Tumor-Associated Macrophages in Human Breast, Colorectal, Lung, Ovarian and Prostate Cancers. Front. Oncol. 2020, 10, 566511. [Google Scholar] [CrossRef]
- O’Neill, D.; Rice, K.; Bhatnagar, A.; Kearns, D.; Berditchevski, F.; El-Ghobashy, A.; Shaaban, A.M. Immunohistochemical Profiling of the Tumour Microenvironment in Borderline and Malignant Ovarian Tumours in Young Women. Oncol. Lett. 2023, 25, 177. [Google Scholar] [CrossRef]
- Toss, M.; Miligy, I.; Al-kawaz, A.; Alsleem, M.; Khout, H.; Rida, P.; Aneja, R.; Green, A.; Ellis, I.; Rakha, E. Prognostic Significance of Tumour Infiltrating Lymphocytes in Ductal Carcinoma in Situ of the Breast. Mod. Pathol. 2018, 31, 1226–1236. [Google Scholar] [CrossRef]
- Xu, F.F.; Zheng, S.F.; Xu, C.; Cai, G.; Wang, S.B.; Qi, W.X.; Wang, C.F.; Chen, J.Y.; Lu, C. Prognostic and Predictive Significance of Tumor Infiltrating Lymphocytes for Ductal Carcinoma in Situ. Oncoimmunology 2021, 10, 1875637. [Google Scholar] [CrossRef]
- Sato, E.; Olson, S.H.; Ahn, J.; Bundy, B.; Nishikawa, H.; Qian, F.; Jungbluth, A.A.; Frosina, D.; Gnjatic, S.; Ambrosone, C.; et al. Intraepithelial CD8+ Tumor-Infiltrating Lymphocytes and a High CD8+/Regulatory T Cell Ratio Are Associated with Favorable Prognosis in Ovarian Cancer. Proc. Natl. Acad. Sci. USA 2005, 102, 18538. [Google Scholar] [CrossRef]
- Stumpf, M.; Hasenburg, A.; Riener, M.O.; Jütting, U.; Wang, C.; Shen, Y.; Orlowska-Volk, M.; Fisch, P.; Wang, Z.; Gitsch, G.; et al. Intraepithelial CD8-Positive T Lymphocytes Predict Survival for Patients with Serous Stage III Ovarian Carcinomas: Relevance of Clonal Selection of T Lymphocytes. Br. J. Cancer 2009, 101, 1513. [Google Scholar] [CrossRef] [PubMed]
- Leary, A.; Genestie, C.; Blanc-Durand, F.; Gouy, S.; Dunant, A.; Maulard, A.; Drusch, F.; Cheaib, B.; Michels, J.; Bentivegna, E.; et al. Neoadjuvant Chemotherapy Alters the Balance of Effector to Suppressor Immune Cells in Advanced Ovarian Cancer. Cancer Immunol. Immunother. 2021, 70, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Sánchez, A.; Cybulska, P.; Mager, K.L.V.; Koplev, S.; Cast, O.; Couturier, D.L.; Memon, D.; Selenica, P.; Nikolovski, I.; Mazaheri, Y.; et al. Unraveling Tumor-Immune Heterogeneity in Advanced Ovarian Cancer Uncovers Immunogenic Effect of Chemotherapy. Nat. Genet. 2020, 52, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Salas-Benito, D.; Vercher, E.; Conde, E.; Glez-Vaz, J.; Tamayo, I.; Hervas-Stubbs, S. Inflammation and Immunity in Ovarian Cancer. EJC Suppl. 2020, 15, 56. [Google Scholar] [CrossRef] [PubMed]
- Barnett, J.C.; Bean, S.M.; Whitaker, R.S.; Kondoh, E.; Baba, T.; Fujii, S.; Marks, J.R.; Dressman, H.K.; Murphy, S.K.; Berchuck, A. Ovarian Cancer Tumor Infiltrating T-Regulatory (Treg) Cells Are Associated with a Metastatic Phenotype. Gynecol. Oncol. 2010, 116, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Clarke, B.; Tinker, A.V.; Lee, C.H.; Subramanian, S.; van de Rijn, M.; Turbin, D.; Kalloger, S.; Han, G.; Ceballos, K.; Cadungog, M.G.; et al. Intraepithelial T Cells and Prognosis in Ovarian Carcinoma: Novel Associations with Stage, Tumor Type, and BRCA1 Loss. Mod. Pathol. 2009, 22, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Bösmüller, H.-C.; Wagner, P.; Peper, J.K.; Schuster, H.; Pham, D.L.; Greif, K.; Beschorner, C.; Rammensee, H.-G.; Stevanović, S.; Fend, F.; et al. Combined Immunoscore of CD103 and CD3 Identifies Long-Term Survivors in High-Grade Serous Ovarian Cancer. Int. J. Gynecol. Cancer. 2016, 26, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Tomšová, M.; Melichar, B.; Sedláková, I.; Šteiner, I. Prognostic Significance of CD3+ Tumor-Infiltrating Lymphocytes in Ovarian Carcinoma. Gynecol. Oncol. 2008, 108, 415–420. [Google Scholar] [CrossRef] [PubMed]
- James, F.R.; Jiminez-Linan, M.; Alsop, J.; Mack, M.; Song, H.; Brenton, J.D.; Pharoah, P.D.P.; Ali, H.R. Association between Tumour Infiltrating Lymphocytes, Histotype and Clinical Outcome in Epithelial Ovarian Cancer. BMC Cancer 2017, 17, 657. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.S.; Sahota, R.A.; Milne, K.; Kost, S.E.; Nesslinger, N.J.; Watson, P.H.; Nelson, B.H. CD20+ Tumor-Infiltrating Lymphocytes Have an Atypical CD27- Memory Phenotype and Together with CD8+ T Cells Promote Favorable Prognosis in Ovarian Cancer. Clin. Cancer Res. 2012, 18, 3281–3292. [Google Scholar] [CrossRef] [PubMed]
- Mesnage, S.J.L.; Auguste, A.; Genestie, C.; Dunant, A.; Pain, E.; Drusch, F.; Gouy, S.; Morice, P.; Bentivegna, E.; Lhomme, C.; et al. Neoadjuvant Chemotherapy (NACT) Increases Immune Infiltration and Programmed Death-Ligand 1 (PD-L1) Expression in Epithelial Ovarian Cancer (EOC). Ann. Oncol. 2017, 28, 651–657. [Google Scholar] [CrossRef]
- Zitvogel, L.; Kepp, O.; Kroemer, G. Immune Parameters Affecting the Efficacy of Chemotherapeutic Regimens. Nat. Rev. Clin. Oncol. 2011, 8, 151–160. [Google Scholar] [CrossRef]
- Böhm, S.; Montfort, A.; Pearce, O.M.T.; Topping, J.; Chakravarty, P.; Everitt, G.L.A.; Clear, A.; McDermott, J.R.; Ennis, D.; Dowe, T.; et al. Neoadjuvant Chemotherapy Modulates the Immune Microenvironment in Metastases of Tubo-Ovarian High-Grade Serous Carcinoma. Clin. Cancer Res. 2016, 22, 3025–3036. [Google Scholar] [CrossRef]
- Pölcher, M.; Braun, M.; Friedrichs, N.; Rudlowski, C.; Bercht, E.; Fimmers, R.; Sauerwald, A.; Keyver-Paik, M.D.; Kübler, K.; Büttner, R.; et al. Foxp3+ Cell Infiltration and Granzyme B+/Foxp3+ Cell Ratio Are Associated with Outcome in Neoadjuvant Chemotherapy-Treated Ovarian Carcinoma. Cancer Immunol. Immunother. 2010, 59, 909–919. [Google Scholar] [CrossRef]
- Lo, C.S.; Sanii, S.; Kroeger, D.R.; Milne, K.; Talhouk, A.; Chiu, D.S.; Rahimi, K.; Shaw, P.A.; Clarke, B.A.; Nelson, B.H. Neoadjuvant Chemotherapy of Ovarian Cancer Results in Three Patterns of Tumor-Infiltrating Lymphocyte Response with Distinct Implications for Immunotherapy. Clin. Cancer Res. 2017, 23, 925–934. [Google Scholar] [CrossRef]
- Dai, D.; Liu, L.; Huang, H.; Chen, S.; Chen, B.; Cao, J.; Luo, X.; Wang, F.; Luo, R.; Liu, J. Nomograms to Predict the Density of Tumor-Infiltrating Lymphocytes in Patients With High-Grade Serous Ovarian Cancer. Front Oncol. 2021, 11, 590414. [Google Scholar] [CrossRef]
- Wouters, M.C.A.; Komdeur, F.L.; Workel, H.H.; Klip, H.G.; Plat, A.; Kooi, N.M.; Wisman, G.B.A.; Mourits, M.J.E.; Arts, H.J.G.; Oonk, M.H.M.; et al. Treatment Regimen, Surgical Outcome, and T-Cell Differentiation Influence Prognostic Benefit of Tumor-Infiltrating Lymphocytes in High-Grade Serous Ovarian Cancer. Clin. Cancer Res. 2016, 22, 714–724. [Google Scholar] [CrossRef]
- Cancer Research UK. Proportion of Cancer Cases by Stage at Diagnosis. Available online: https://crukcancerintelligence.shinyapps.io/EarlyDiagnosis/ (accessed on 14 April 2024).
- Ovarian Cancer Survival Statistics|Cancer Research UK. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/ovarian-cancer/survival#heading-Zero (accessed on 14 April 2024).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histological Subtype | Clear Cell | Endometrioid | Mixed | Mucinous | Mucinous Borderline | Serous | Serous Borderline |
| 15 | 18 | 6 | 12 | 6 | 79 | 2 | |
| Stage | Stage 1 | Stage 2 | Stage 3 | Stage 4 | |||
| 53 | 10 | 60 | 11 | ||||
| Grade | Grade 1 | Grade 2 | Grade 3 | Borderline | |||
| 19 | 10 | 100 | 8 | ||||
| Age | <30 yrs | 31–40 | 41–50 | 51–60 | 61–70 | 71–80 | >81 |
| 4 | 9 | 13 | 40 | 37 | 29 | 6 | |
| Ethnicity | White British | Indian | White Eastern European | Black Caribbean | Other Asian | Pakistani | White Southern European |
| 122 | 7 | 4 | 1 | 1 | 1 | 1 |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Epithelial ovarian primary tumours | Representative tumour histology not available (n = 45) |
| Grade 1–3 + borderline ovarian tumours | Histological subtype not epithelial (n = 14) |
| Stage 1–4 | Primary malignancy not ovarian (n = 29) |
| Any or no treatment | Recurrence of previous malignancy (n = 5) |
| All ages | Inadequate documentation available (n = 2) |
| Magnification | Indicator | Staining |
|---|---|---|
| ×4 | Overall percentage cell infiltrate | Haemotoxin + Eosin |
| ×40 (mean score from five separate high-power fields) | Total cell number | Immunohistochemistry for CD3, CD20, CD68 PG-M1, CD163 antibodies |
| Stromal cell count | ||
| Intra-tumoral cell count | ||
| Touching lymphocyte count | ||
| Stromal aggregate presence | ||
| Tumoral aggregate presence | ||
| Total cell count in largest stromal hotspot (where present) | ||
| Total cell count in largest tumoral hotspot (where present) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stout, A.; Facey, N.; Bhatnagar, A.; Rice, K.; Berditchevski, F.; Kearns, D.; Metcalf, A.; Elghobashy, A.; Shaaban, A.M. Profiling of Tumour-Infiltrating Lymphocytes and Tumour-Associated Macrophages in Ovarian Epithelial Cancer—Relation to Tumour Characteristics and Impact on Prognosis. Int. J. Mol. Sci. 2024, 25, 4524. https://doi.org/10.3390/ijms25084524
Stout A, Facey N, Bhatnagar A, Rice K, Berditchevski F, Kearns D, Metcalf A, Elghobashy A, Shaaban AM. Profiling of Tumour-Infiltrating Lymphocytes and Tumour-Associated Macrophages in Ovarian Epithelial Cancer—Relation to Tumour Characteristics and Impact on Prognosis. International Journal of Molecular Sciences. 2024; 25(8):4524. https://doi.org/10.3390/ijms25084524
Chicago/Turabian StyleStout, Annabel, Natalya Facey, Anjali Bhatnagar, Kirstie Rice, Fedor Berditchevski, Daniel Kearns, Amy Metcalf, Alaa Elghobashy, and Abeer M. Shaaban. 2024. "Profiling of Tumour-Infiltrating Lymphocytes and Tumour-Associated Macrophages in Ovarian Epithelial Cancer—Relation to Tumour Characteristics and Impact on Prognosis" International Journal of Molecular Sciences 25, no. 8: 4524. https://doi.org/10.3390/ijms25084524