Optimal Clinical Time for Reliable Measurement of Transcutaneous CO2 with Ear Probes: Counterbalancing Overshoot and the Vasodilatation Effect

Abstract
:OBJECTIVES:
EXPERIMENTAL SECTION:
RESULTS:
CONCLUSIONS:
1. Introduction
2. Experimental Section
Patients
Methods
Statistical Analysis
3. Results
4. Discussion and Conclusions
Abbreviations:
| SpO2: | oxygen saturation |
| TcPCO2: | transcutaneous partial pressure of carbon dioxide |
| PaCO2: | arterial pressure of carbon dioxide |
| PaO2: | arterial oxygen pressure |
| ABG: | arterial blood gas analysis |
| SpO2: | transcutaneous arterial oxygen saturation |
| FEV1: | forced spirometry value in the first second |
| FVC: | forced vital capacity |
| PFTs: | pulmonary function testings |
Acknowledgments
References
- Domingo, Ch.; Roig, J.; Coll, R.; Klamburg, J.; Izquierdo, J.; Ruiz-Manzano, J.; Morera, J.; Domingo, E. Evaluation of the use of three different devices for nocturnal oxygen therapy in COPD patients. Respiration 1996, 63, 230–235. [Google Scholar]
- Domingo, Ch.; Klamburg, J.; Roig, J.; Coll, R.; Izquierdo, J.; Morera, J.; Serés, L.; Domingo, E. Acute and long-term haemodynamic response to home oxygen therapy: nasal prongs versus oxygen saving devices. J. Appl. Res 2004, 4, 149–163. [Google Scholar]
- Domingo, Ch.; Canturri, E.; Luján, M.; Moreno, A.; Espuelas, H.; Marín, A. Transcutaneous measurement of partial pressure of carbon dioxide and oxygen saturation: validation of the SenTec monitor. Arch. Bronconeumol 2006, 42, 245–250. [Google Scholar]
- Lujan, M.; Canturri, E.; Moreno, A.; Arranz, M.; Vigil, L.; Domingo, Ch. Capnometry in spontaneously breathing patients: influence of chronic obstructive pulmonary disease and expiration manoeuvres. Med. Sci. Mon 2008, 14, 485–492. [Google Scholar]
- Rohling, R.; Biro, P. Clinical investigation of a new combined pulse oximetry and carbon dioxide tension sensor in adult anesthesia. J. Clin. Monit 1999, 15, 23–27. [Google Scholar]
- Tschupp, A.; Fanconi, S. A combined ear sensor for pulse oximetry and carbon dioxide tension monitoring: accuracy in critically ill children. Anesth. Analg 2003, 96, 82–84. [Google Scholar]
- Janssens, J.P.; Perrin, E.; Bennani, I.; de Muralt, B.; Titelion, V.; Picaud, C. Is Continuous transcutaneous monitoring of PCO2 (TcPCO2) over 8 h reliable in adults? Respir. Med 2001, 95, 331–335. [Google Scholar]
- Sanchis, J.; Casán, P.; Castillo, J.; Gonzalez, N.; Palenciano, L.; Roca, J. Normativa para la practica de la espirometria forzada. Arch. Bronconeumol 1989, 25, 132–142. [Google Scholar]
- Roca, J.; Sanchis, J.; Agusti-Vidal, A.; Segarra, F.; Navajas, A.; Rodriguez-Roisin, R.; Casan, P.; Sans, S. Spirometric reference values from a Mediterranean population. Bull. Eur. Physiopathol. Respir 1986, 22, 217–224. [Google Scholar]
- Agustí, A.G.N.; Burgos, F.; Casán, P.; Perpiñá, M.; Rodríguez-Roisín, R.; Sánchez, L.; Sobradillo, V.; Togores, B. Normativa de la gasometría arterial. Arch. Bronconeumol. 1998, 34, 142–153. [Google Scholar]
- Storre, J.H.; Steurer, B.; Kabitz, H.J.; Dreher, M.; Windisch, W. Transcutaneous PCO2 monitoring during initiation of noninvasive ventilation. Chest 2007, 132, 1810–1816. [Google Scholar]
- Kagawa, S.; Otani, N.; Kamide, M.; Gisiger, P.A.; Eberhard, P.; Severinghaus, J.W. Initial transcutaneous PCO2 overshoot with ear probe at 42 degrees. C. J. Clin. Monit. Comput 2004, 18, 343–345. [Google Scholar]
- Hirabayashi, M.; Otani, N.; Kagawa, S.; Kamide, M. Method of evading the overshoot phenomenon of transcutaneous P (CO2) measurement at the ear lobe. Masui 2006, 55, 1018–1022, (abstract in English).. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistics notes: Measurement error. BMJ 1996, 313, 744–745. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical Methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar]
- Molinero, L. Errores de medida en variables numéricas: Correlación y Concordancia. Available online: http://www.seh-lelha.org/stat1.htm/ (accessed on 18 August 2009).
- Kagawa, S.; Severinghaus, J.W. Errors in monitoring transcutaneous PCO2 in the ear. Crit. Care Med 2005, 3, 2414–2415. [Google Scholar]
- McBride, D.S., Jr.; Johnson, J.O.; Tobias, J.D. Noninvasive carbon dioxide monitoring during neurosurgical procedures in adults: end-tidal versus transcutaneous techniques. South Med. J 2002, 95, 870–874. [Google Scholar]
- Tobias, J.D. Transcutaneous carbon dioxide monitoring in infants and children. Paediatr. Anaesth 2009, 19, 434–444. [Google Scholar]
- Luján, M.; Moreno, A.; Veigas, C.; Montón, C.; Pomares, S.; Domingo, Ch. Non-invasive home mechanical ventilation: effectiveness and efficiency of an outpatient initiation protocol compared with the standard in-hospital model. Respir. Med 2007, 101, 1177–1182. [Google Scholar]
- Hirabayashi, M.; Fujiwara, C.; Ohtani, N.; Kagawa, S.; Kamide, M. Transcutaneous C02 monitors are more accurate than end-tidal C02 monitors. J. Anesth 2009, 23, 198–202. [Google Scholar]
- Domingo, Ch.; Sans-Torres, J.; Solà, J.; Espuelas, H.; Marín, A. Effectiveness and efficiency of a specialized unit in the care of patients with chronic obstructive pulmonary disease and respiratory insufficiency. Arch. Bronconeumol 2006, 42, 104–112. [Google Scholar]
- Domingo, Ch.; Ortún, V. Design and analysis of health products and services. An example at a specialized COPD unit. Open Resp. Med. J 2008, 2, 7–15. [Google Scholar]
- Domingo, Ch. Home oxygen therapy for the 21st century. Curr. Respir. Med. Rev 2006, 2, 237–251. [Google Scholar]


{kind=link}
| Variable | Mean ± SD | Range |
|---|---|---|
| Age (years) | 63.1 ± 11.8 | 37–86 |
| FEV1 (l) | 2.21 ± 0.87 | 0.51–4.33 |
| FEV1% | 72.92 ± 23.9 | 17–124 |
| FVC (l) | 3.13 ± 0.92 | 1.23–5.14 |
| FVC % | 75.4 ± 16.2 | 37–107 |
| FEV1/FVC | 70 ± 15.6 | 24–88 |
| pH | 7.41 ± 0.02 | 7.35–7.48 |
| PaCO2 (mm Hg) | 39.91 ± 4.85 | 29–55 |
| PaO2 (mm Hg) | 82.6 ± 13.23 | 49.2–126 |
| HCO3 (mmol/L) | 25.5 ± 2.14 | 19–32 |
| SaO2 (%) | 95.7 ± 2.30 | 85–99 |
| Hb (g/L) | 14.26 ± 1.79 | 9.2–19 |
| 2’ | 4’ | 6’ | 8’ | 10’ | 12’ | 14’ | 16’ | 18’ | 20’ | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean TcPCO2 (SD) | 30.1 (7.5) | 36.04 (6.7) | 38 (7.5) | 39.2 (6.2) | 39.3 (5.8) | 39 (5.6) | 38.7 (5.5) | 38.6 (5.3) | 38.2 (5.3) | 38.15 (5.1) |
| Mean PaCO2-TcPCO2 (SD) | 9.6 (7.6) | 3.8 (5.8) | 1.8 (6) | 0.7 (4.2) | 0.57 (3.5) | 0.87 (3.3) | 1.14 (3) | 1.28 (2.9 | 1.6 (3) | 1.7 (2.8) |
| 95 % CI | 8.0–11.2 | 2.5–5 | 0.5–3 | −0.2–1.5 | −0.17–1.32 | 0.17–1.56 | 0.5–1.8 | 0.6–1.9 | 0.9–2.2 | 1.1–2.3 |
| Pearson correlation coefficients (r) | 0.292 | 0.549 | 0.594 | 0.741 | 0.791 | 0.810 | 0.834 | 0.834 | 0.822 | 0.838 |
| ICC | 0.267 | 0.519 | 0.54 | 0.718 | 0.777 | 0.801 | 0.827 | 0.830 | 0.819 | 0.836 |
| 2’ | 4’ | 6’ | 8’ | 10’ | 12’ | 14’ | 16’ | 18’ | 20’ | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean SpO2 (SD) | 96.8 (2.1) | 96.4 (2.2) | 96.38 (2.1) | 96.33 (2.18) | 96.24 (2.3) | 96.3 (2.3) | 96.3 (2.1) | 96.2 (2.4) | 96.3 (2.1) | 96.4 (2.1) |
| Mean SaO2-SpO2 (SD) | −1.14 (1.32) | −0.71 (1.5) | −0.7 (1.49) | −0.68 (1.6) | −0.59 (1.69) | −0.61 (1.72) | −0.68 (1.46) | −0.52 (2) | −0.61 (1.45) | −0.78 (1.48) |
| 95 % CI | −0.86; −1.42 | −0.4; −1.02 | −0.38; −1.01 | −0.34; −1.01 | −0.23; −0.94 | −0.24; −0.97 | −0.37; −0.99 | −0.09; −0.94 | −0.3; −0.9 | −0.46; −1.09 |
| Pearson correlation coefficients (r) | 0.822 | 0.782 | 0.772 | 0.738 | 0.721 | 0.710 | 0.780 | 0.634 | 0.788 | 0.776 |
| ICC | 0.818 | 0.780 | 0.768 | 0.735 | 0.721 | 0.709 | 0.775 | 0.633 | 0.785 | 0.772 |
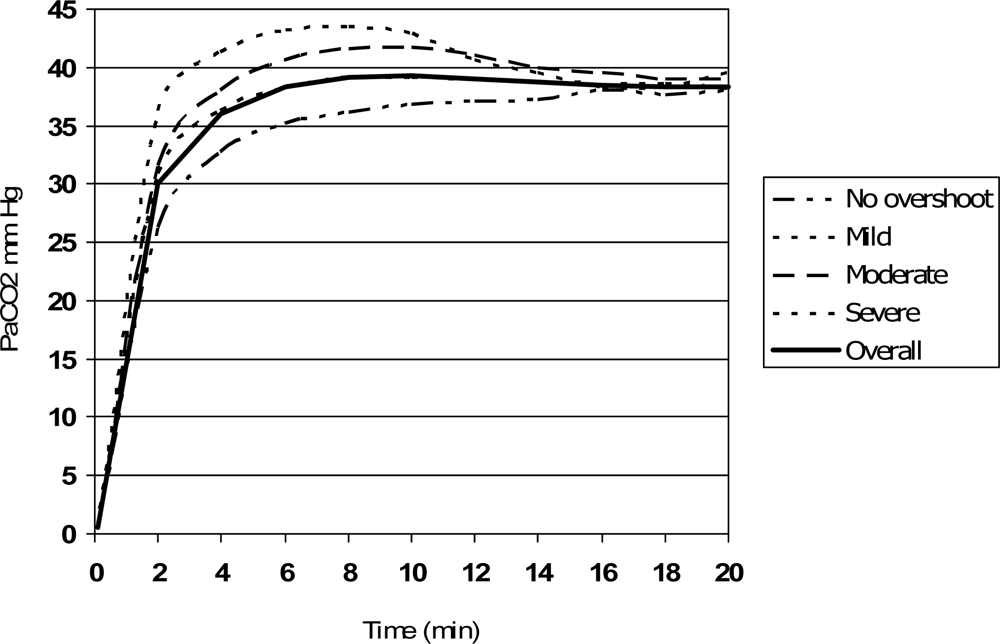
| Overshoot | PaCO2 (mmHg) | 2’ | 4’ | 6’ | 8’ | 10’ | 12’ | 14’ | 16’ | 18’ | 20’ |
|---|---|---|---|---|---|---|---|---|---|---|---|
| None (n = 29) | 40.2 ± 4.9 | 26.3 ± 8.7 | 32.7 ± 8.2 | 35.2 ± 7.1 | 36.2 ± 6.4 | 36.9 ± 5.7 | 37.1 ± 5.5 | 37.3 ± 5.6 | 38 ± 5.6 | 37.6 ± 5.5 | 38 ± 5 |
| Light (n = 33) | 39.5 ± 4.3 | 30.9 ± 6.3 | 36.3 ± 5 | 38.4 ± 4.8 | 39.1 ± 4.9 | 39.2 ± 4.8 | 39 ± 4.7 | 38.7 ± 4.7 | 38.5 ± 4.7 | 38.6 ± 4.7 | 38.2 ± 4.6 |
| Moderate (n = 20) | 39.9 ± 6.1 | 31.5 ± 5.3 | 38.0 ± 5.6b | 40.7 ± 6.3 b | 41.6 ± 6.6 b | 41.7 ± 6.9b | 41 ± 7 | 40.0 ± 6 | 39.5 ± 6.5 | 39 ± 6.4 | 39 ± 6.2 |
| Severe (n = 9) | 40.2 ± 3.6 | 36.3 ± 6.5a | 41.3 ± 4.8b | 43.3 ± 4.6 b | 43.5 ± 5 b | 42.9 ± 4.2 b | 40.7 ± 3.7 | 39.5 ± 3.4 | 38.4 ± 3.5 | 38.4 ± 3.9 | 39.5 ± 4.1 |
©2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/)
Share and Cite
Domingo, C.; Canturri, E.; Moreno, A.; Espuelas, H.; Vigil, L.; Luján, M. Optimal Clinical Time for Reliable Measurement of Transcutaneous CO2 with Ear Probes: Counterbalancing Overshoot and the Vasodilatation Effect. Sensors 2010, 10, 491-500. https://doi.org/10.3390/s100100491
Domingo C, Canturri E, Moreno A, Espuelas H, Vigil L, Luján M. Optimal Clinical Time for Reliable Measurement of Transcutaneous CO2 with Ear Probes: Counterbalancing Overshoot and the Vasodilatation Effect. Sensors. 2010; 10(1):491-500. https://doi.org/10.3390/s100100491
Chicago/Turabian StyleDomingo, Christian, Elisa Canturri, Amalia Moreno, Humildad Espuelas, Laura Vigil, and Manel Luján. 2010. "Optimal Clinical Time for Reliable Measurement of Transcutaneous CO2 with Ear Probes: Counterbalancing Overshoot and the Vasodilatation Effect" Sensors 10, no. 1: 491-500. https://doi.org/10.3390/s100100491
APA StyleDomingo, C., Canturri, E., Moreno, A., Espuelas, H., Vigil, L., & Luján, M. (2010). Optimal Clinical Time for Reliable Measurement of Transcutaneous CO2 with Ear Probes: Counterbalancing Overshoot and the Vasodilatation Effect. Sensors, 10(1), 491-500. https://doi.org/10.3390/s100100491