Investigation of Exhaled Breath Samples from Patients with Alzheimer’s Disease Using Gas Chromatography-Mass Spectrometry and an Exhaled Breath Sensor System


Abstract
:1. Introduction
2. Materials and Methods
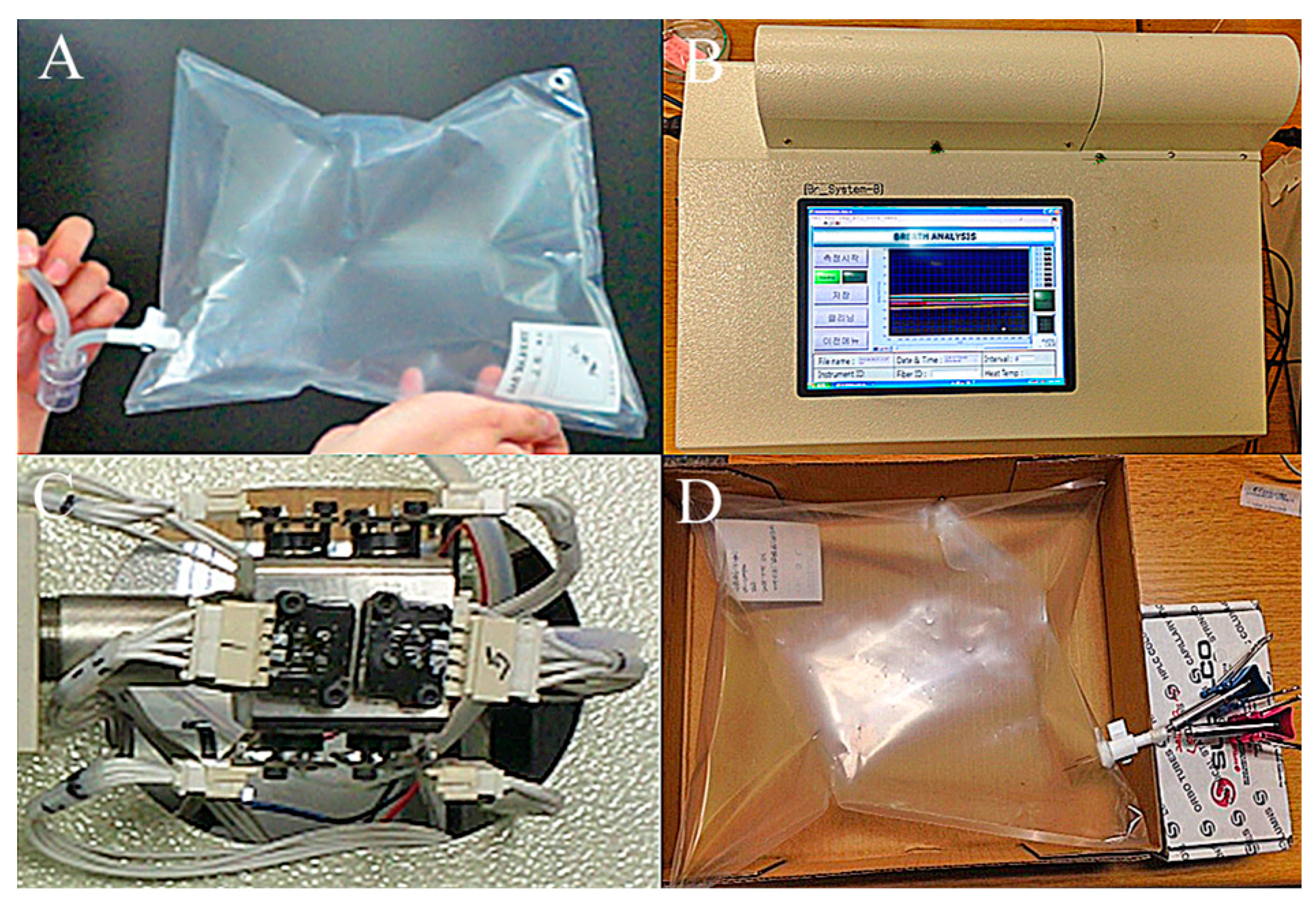
2.1. Collection of Exhaled Breath Samples from Participants
2.2. Design of Solid Phase Microextraction (SPME)
2.3. Characterization of Chemical Compounds Present in Exhaled Breath Using GC-MS
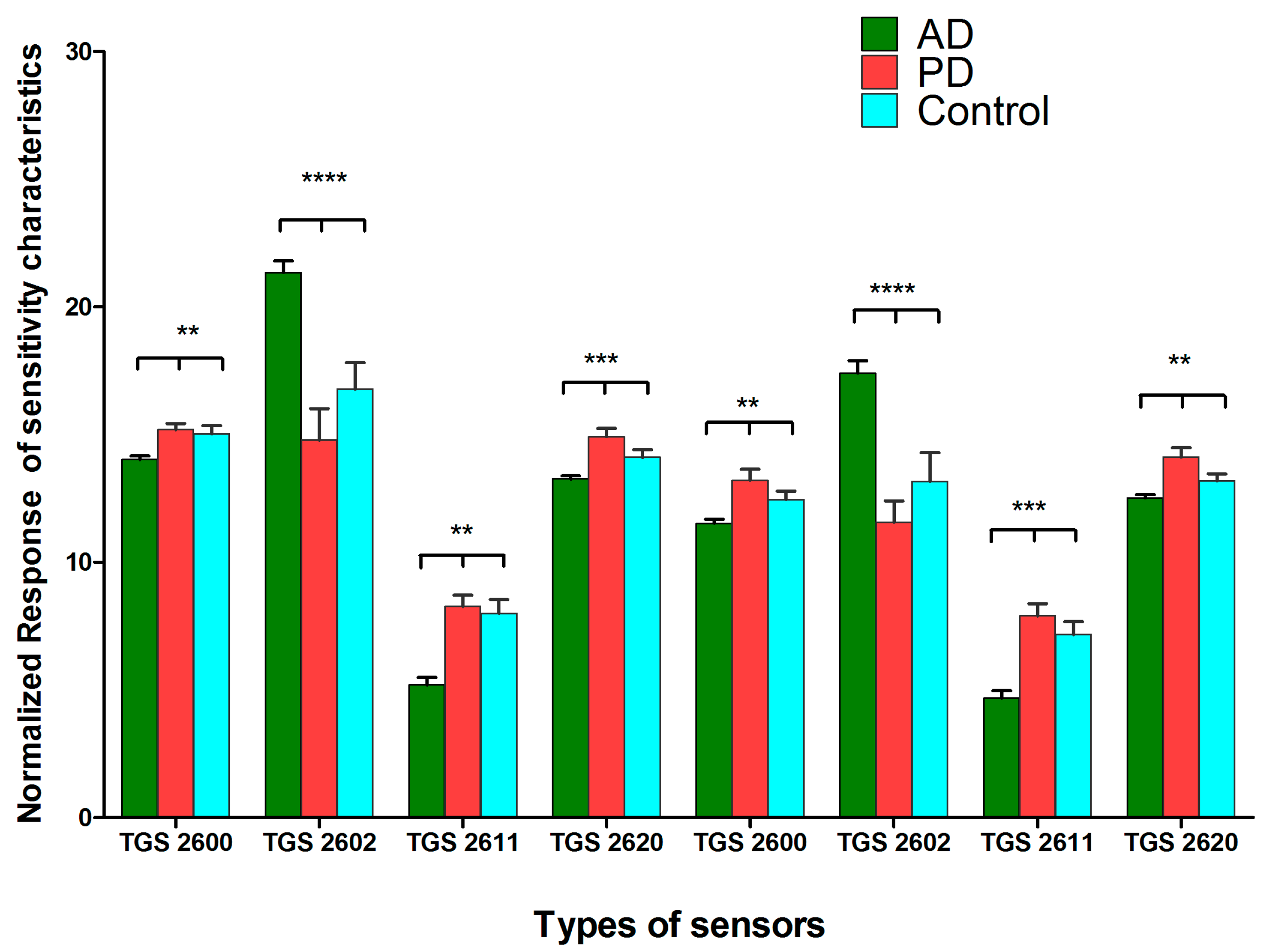
2.4. Clustering Analysis of Exhaled Breath Samples Using an Exhaled Breath Sensor System
2.5. Statistical Tests
3. Results and Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ferraris, V.A. What do dogs, ancient Romans, Linus Pauling, and mass spectrometry have in common? Early lung cancer and exhaled breath. J. Thorac. Cardiovas. Sur. 2016, 151, 313–314. [Google Scholar] [CrossRef] [PubMed]
- Shneh, S.; Ranjan, N.; Trinad, C. Clinical Application of Volative Organic Compound Analysis for Detecting Infectious Diseases. Clin. Microbiol. Rev. 2013, 26, 462–475. [Google Scholar]
- Pereira, J.; Porto-Figueira, P.; Cavaco, C.; Taunk, K.; Rapole, S.; Dhakne, R.; Nagarajaram, H.; Câmara, J.S. Breath Analysis as a Potential and Non-Invasive Frontier in Disease Diagnosis: An Overview. Metabolites 2015, 5, 3–55. [Google Scholar] [CrossRef] [PubMed]
- Amann, A.; Spanel, P.; Smith, D. Breath analysis: The approach towards clinical applications. Mini Rev. Med. Chem. 2007, 7, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Jahan, S.A.; Kabir, E. A review of breath analysis for diagnosis of human health. TrAC Trends Anal. Chem. 2012, 33, 1–8. [Google Scholar] [CrossRef]
- Dowlaty, N.; Yoon, A.; Galassetti, P. Monitoring states of altered carbohydrate metabolism via breath analysis: Are times ripe for transition from potential to reality? Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Buszewski, B.; Kęsy, M.; Ligor, T.; Amann, A. Human exhaled air analytics: Biomarkers of diseases. Biomed. Chromatogr. 2007, 21, 553–566. [Google Scholar] [CrossRef] [PubMed]
- Miekisch, W.; Schubert, J.K.; Noeldge-Schomburg, G.F. Diagnostic potential of breath analysis—Focus on volatile organic compounds. Clin. Chim. Acta 2004, 347, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.-B.; Byun, H.-G.; So, M.-S.; Huh, J.-S. Analysis of diabetic patient’s breath with conducting polymer sensor array. Sens. Actuators B Chem. 2005, 108, 305–308. [Google Scholar] [CrossRef]
- Peng, G.; Hakim, M.; Broza, Y.Y.; Billan, S.; Abdah-Bortnyak, R.; Kuten, A.; Tisch, U.; Haick, H. Detection of lung, breast, colorectal, and prostate cancers from exhaled breath using a single array of nanosensors. Br. J. Cancer 2010, 103, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Peng, Y.; Duan, Y. Diagnosis of breast cancer based on breath analysis: An emerging method. Crit. Rev. Oncol. Hematol. 2013, 87, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Byun, H.-G.; Persaud, K.C.; Pisanelli, A.M. Wound-state monitoring for burn patients using E-Nose/SPME system. ETRI J. 2010, 32, 440–446. [Google Scholar] [CrossRef]
- Fens, N.; Roldaan, A.; Van der Schee, M.; Boksem, R.; Zwinderman, A.; Bel, E.; Sterk, P. External validation of exhaled breath profiling using an electronic nose in the discrimination of asthma with fixed airways obstruction and chronic obstructive pulmonary disease. Clin. Exp. Allergy 2011, 41, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Arasaradnam, R.P.; Ouaret, N.; Thomas, M.G.; Quraishi, N.; Heatherington, E.; Nwokolo, C.U.; Bardhan, K.D.; Covington, J.A. A novel tool for noninvasive diagnosis and tracking of patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Tisch, U.; Schlesinger, I.; Ionescu, R.; Nassar, M.; Axelrod, N.; Robertman, D.; Tessler, Y.; Azar, F.; Marmur, A.; Aharon-Peretz, J. Detection of Alzheimer’s and Parkinson’s disease from exhaled breath using nanomaterial-based sensors. Nanomedicine 2013, 8, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Byun, H.G.; Persaud, K.C.; Khaffaf, S.M.; Hobbs, P.J.; Misselbrook, T.H. Application of unsupervised clustering methods to the assessment of malodour in agriculture using an array of conducting polymer odour sensors. Comput. Electron. Agric. 1997, 17, 233–247. [Google Scholar] [CrossRef]
- Chowdhary, P.; Raveendran, N.; Mehta, K. Rational design and synthesis of some substituted aminoethanones and acetamides as novel acetyl cholinesterase inhibitors. Adv. Res. Pharm. Biol. 2013, 3, 400–402. [Google Scholar]
- Patri, M.; Padmini, A.; Babu, P.P. Polycyclic aromatic hydrocarbons in air and their neurotoxic potency in association with oxidative stress: A brief perspective. Ann. Neurosci. 2010, 16, 22–30. [Google Scholar] [CrossRef]
- Jee, J.-H.; Kang, J.-C. Effect of phenanthrene on haematological parameters in olive flounder, Paralichthys olivaceus (Temminch et Schlegel). Aquac. Res. 2004, 35, 1310–1317. [Google Scholar] [CrossRef]
- Mallet, P.E.; Beninger, R.J.; Flesher, S.N.; Jhamandas, K.; Boegman, R.J. Nucleus basalis lesions: implication of basoamygdaloid cholinergic pathways in memory. Brain Res. Bull. 1995, 36, 51–56. [Google Scholar] [CrossRef]
- Choi, S.J.; Kim, M.J.; Heo, H.J.; Kim, J.K.; Jun, W.J.; Kim, H.K.; Kim, E.-K.; Kim, M.O.; Cho, H.Y.; Hwang, H.-J. Ameliorative effect of 1,2-benzenedicarboxylic acid dinonyl ester against amyloid beta peptide-induced neurotoxicity. Amyloid 2009, 16, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Duysen, E.G.; Lockridge, O. Induction of plasma acetylcholinesterase activity in mice challenged with organophosphorus poisons. Toxicol. Appl. Pharmacol. 2011, 255, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Law, K.-S.; Acey, R.A.; Smith, C.R.; Benton, D.A.; Soroushian, S.; Eckenrod, B.; Stedman, R.; Kantardjieff, K.A.; Nakayama, K. Dialkyl phenyl phosphates as novel selective inhibitors of butyrylcholinesterase. Biochem. Biophys. Res. Commun. 2007, 355, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Peroni, D.G.; Bodini, A.; Corradi, M.; Coghi, A.; Boner, A.L.; Piacentini, G.L. Markers of oxidative stress are increased in exhaled breath condensates of children with atopic dermatitis. Br. J. Dermatol. 2012, 166, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Inonu, H.; Doruk, S.; Sahin, S.; Erkorkmaz, U.; Celik, D.; Celikel, S.; Seyfikli, Z. Oxidative stress levels in exhaled breath condensate associated with COPD and smoking. Respir. Care 2012, 57, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Sayre, L.M.; Perry, G.; Smith, M.A. Oxidative stress and neurotoxicity. Chem. Res. Toxicol. 2007, 21, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.-J.; Zhang, X.; Chen, W.-W. Role of oxidative stress in Alzheimer’s disease. Biomed. Rep. 2016, 4, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Greenough, M.A.; Camakaris, J.; Bush, A.I. Metal dyshomeostasis and oxidative stress in Alzheimer’s disease. Neurochem. Int. 2013, 62, 540–555. [Google Scholar] [CrossRef] [PubMed]
- Farina, M.; Avila, D.S.; da Rocha, J.B.T.; Aschner, M. Metals, oxidative stress and neurodegeneration: a focus on iron, manganese and mercury. Neurochem. Int. 2013, 62, 575–594. [Google Scholar] [CrossRef] [PubMed]
- Berlyne, G.; Dudek, E.; Adler, A.; Rubin, J.; Seidman, M. Silicon metabolism: the basic facts in renal failure. Kidney Int. Suppl. 1985, 17, S175–S177. [Google Scholar] [CrossRef] [PubMed]
- Adler, A.; Berlyne, G. Silicon metabolism. Nephron 1986, 44, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Haick, H.; Broza, Y.Y.; Mochalski, P.; Ruzsanyi, V.; Amann, A. Assessment, origin, and implementation of breath volatile cancer markers. Chem. Soc. Rev. 2014, 43, 1423–1449. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.B.; Byun, H.G.; Zhang, S.; Lim, J.O.; Huh, J.S. Exhaled breath analysis of lung cancer patients using a metal oxide sensor. J. Sens. Sci. Technol. 2011, 20, 300–304. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | AD N (20) | PD N (20) | Control N (20) | p-Value |
|---|---|---|---|---|
| Age, (Y) | 74.9 ± 7.53 | 72.3 ± 7.55 | 67.6 ± 7.03 | - |
| Male sex-no (%) | 30 | 50 | 25 | - |
| Smoker (%) | 10 | 5 | 10 | - |
| Ex-smoker (%) | 5 | 20 | 10 | - |
| MMSE | 17.95 ± 4.86 | 22.85 ± 4.65 | 28.55 ± 1.05 | ≤0.05 |
| CDR-SOB | 6.1 ± 2.6 | 2.24 ± 2.67 | 0.25 ± 0.30 | ≤0.05 |
| H-Y | nd | 2.31 ± 0.56 | nd | - |
| Compound | AD | PD | Control | p-Value |
|---|---|---|---|---|
| Acetamide | 25.76 ± 3.66 | 20.58 ± 1.41 | 24.86 ± 3.78 | ≤0.05 |
| Phenol | 60.45 ± 3.87 | 59.88 ± 2.28 | 60.00 ± 6.54 | ns |
| Alkanes | 0.17 ± 0.13 | 0.21 ± 0.14 | 0.20 ± 0.13 | ns |
| Pentadecane | ||||
| Heptadecane | ||||
| Tetradecane | ||||
| Siloxanes | 4.58 ± 3.05 | 8.38 ± 2.31 | 4.89 ± 2.33 | ≤0.05 |
| Cyclopentasiloxane | ||||
| Cyclotrisiloxane | ||||
| 1,2-benzenedicarboxylic acid diethyl ester | 0.46 ± 0.46 | 0.09 ± 0.04 | 0.32 ± 0.38 | ns |
| Ethyl 3-cyano-2,3-bis (2,5-dimethyl-3-thienyl)-acrylate | 0.04 ± 0.01 | 0 | nd | ≤0.05 |
| Triphenyl phosphate | 0.03 ± 0.03 | nd | 0.07 ± 0.07 | ≤0.05 |
| 1-phenanthrenol | 0.04 ± 0.01 | 0.019 ± 0.01 | nd | ≤0.05 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, H.-C.; Yu, J.-B.; Lee, H.-W.; Huh, J.-S.; Lim, J.-O. Investigation of Exhaled Breath Samples from Patients with Alzheimer’s Disease Using Gas Chromatography-Mass Spectrometry and an Exhaled Breath Sensor System. Sensors 2017, 17, 1783. https://doi.org/10.3390/s17081783
Lau H-C, Yu J-B, Lee H-W, Huh J-S, Lim J-O. Investigation of Exhaled Breath Samples from Patients with Alzheimer’s Disease Using Gas Chromatography-Mass Spectrometry and an Exhaled Breath Sensor System. Sensors. 2017; 17(8):1783. https://doi.org/10.3390/s17081783
Chicago/Turabian StyleLau, Hui-Chong, Joon-Boo Yu, Ho-Won Lee, Jeung-Soo Huh, and Jeong-Ok Lim. 2017. "Investigation of Exhaled Breath Samples from Patients with Alzheimer’s Disease Using Gas Chromatography-Mass Spectrometry and an Exhaled Breath Sensor System" Sensors 17, no. 8: 1783. https://doi.org/10.3390/s17081783