1. Introduction
The early detection of functional decline, which occurs with age and results, among others, in an increased fall risk, is important to initiate timely preventive measures, slow down the progress of decline and maintain older peoples’ independent living. The Timed Up and Go test (TUG), developed by Podsiadlo and Richardson [
1], is a well-established assessment and one of the most frequently-used tests for mobility. This test assesses the basic mobility skills, which make up important abilities for independent living. Besides balance and strength, mobility is one of the essential components of physical function [
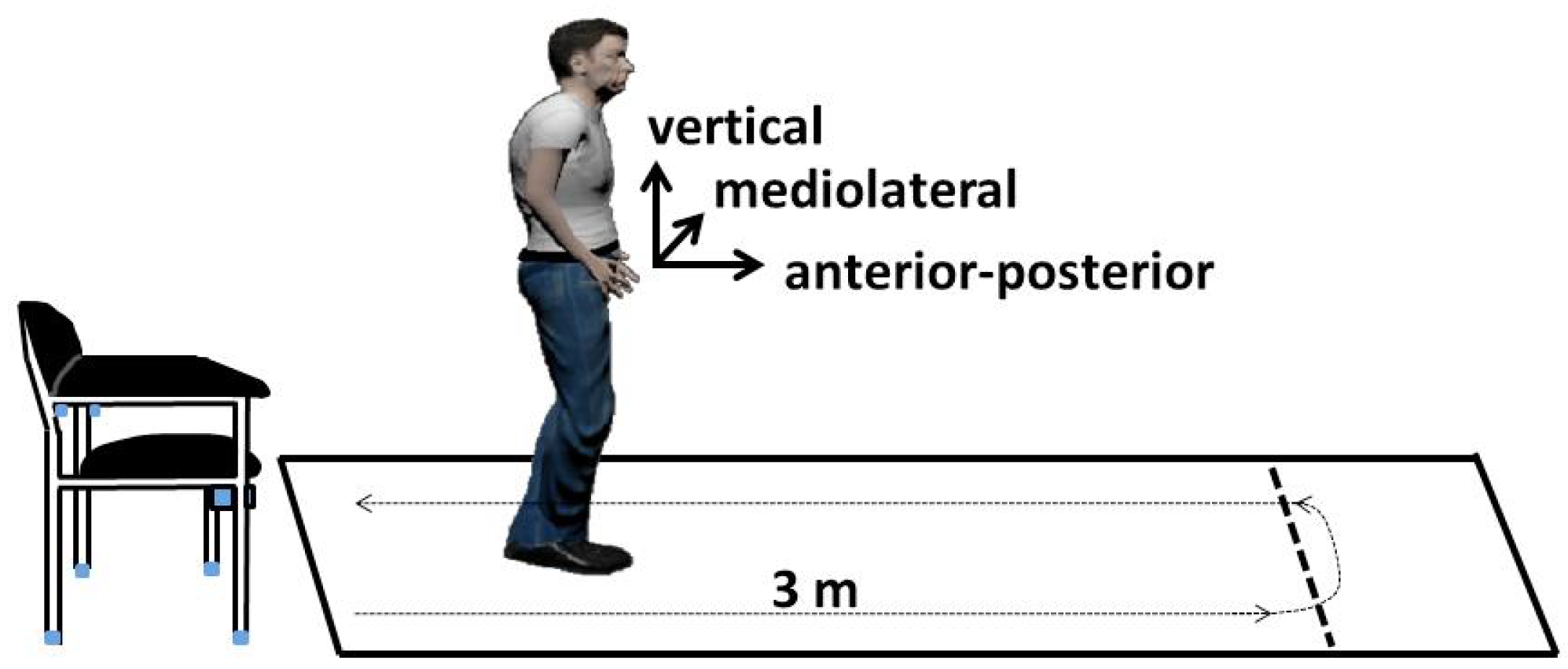
2]. The TUG consists of several components of everyday movements (see
Figure 1). At the beginning of the test, the patient is sitting on a chair leaning against the backrest. Then, she or he gets up from the chair, walks 3 m, turns around, walks back and sits down again. The test starts with the request and stops when the participant is seated again correctly in the chair with his/her back resting at the back of the chair. According to the necessary duration, the patient’s mobility is categorized into four groups: <10 s freely mobile, 11–19 s mostly independent, 20–29 s variable mobility, >30 s impaired mobility. Therefore, a faster time indicates a better functional performance. The TUG test is an established and widely-used test as part of geriatric assessments, and the intra-rater, inter-rater and test-retest reliability of the individual components of the instrumented TUG (iTUG) have been shown to be excellent to good for total duration in patients with Parkinson’s disease [
3]. Therefore, the TUG test is a suitable test to investigate temporal progressions. For example, van Iersel et al. [
4] pointed out that the TUG test is sensitive to clinically-relevant changes in functional mobility in frail elderly patients within a period of two weeks. Over time, the TUG test was enhanced several times: Wall et al. [
5] introduced the Expanded Timed Get-up-and-Go (ETGUG) test, in which the length was increased to 10 m, and times for each of the components tasks were measured separately using a multi-memory stopwatch.
The advantage of the TUG test is its simplicity: the short test duration, the low required equipment and the possibility to perform the test even for patients with functional impairments. However, because of the importance of detecting early changes in functional decline, these assessment should be performed regularly and in a high frequency to initiate early interventions and slow down the functional decline. To relieve clinicians and reduce the stress for the patients, these assessments should take place in the daily life of the patients in the form of unsupervised self-assessments. Inertial Measurement Units (IMU) are well suited for automated analyses and can be easy to use, flexible and inexpensive, thus suitable for self-guided assessments.
Sprint et al. [
6] provided in their survey an overview of the TUG test and technologies utilized for TUG instrumentation. Besides video-based measurements, ambient technologies and wearable or smartphone-based technologies have been already used for studies. The automated/ambient TUG (aTUG) [
7] uses ambient sensors attached to a chair and provides a fully-automated TUG test execution. The aTUG consists of a laser range scanner for gait analysis, force sensors in the chair legs to analyze the components of rising from the chair or sitting down and a laser barrier to measure the test duration, which shows a high correlation with stop-watch measurements [
8].
The suitability of the aTUG system in diverse health care environments was already shown in [
9].
Wearable sensors have become quite popular, and therefore, IMU were used in several studies.
Table 1 shows a selection of studies, which used inertial measurement units or smartphones for TUG analyses.
Already in 2008, Higashi et al. [
10] developed the TUG-T and measured the duration of the six single components of the test (standing up, walking forward, turn one, walking back, turn two and sitting down) with two inertial sensors. An instrumented version of the TUG (iTUG) was proposed to measure the duration of four components (sit-to-stand, steady-state gait, turning, turn-to-sit) and a set of balance and gait parameters [
11], but required seven inertial sensors. Reinfelder et al. [
16] developed a TUG phase segmentation system with two IMU and reached a mean sensitivity of 81.80% over all phases by using a support vector machine. A smartphone application called sTUG was developed by Milosevic et al. [
15], which completely automates the iTUG test, determines the beginning and the end of the test and quantifies its individual phases. With a system of 17 IMU and a rule-based algorithm, accuracies of 100% could be achieved for TUG phases’ recognition [
17].
Many studies in the literature focus on the discrimination between different diseases or phenotypes such as Parkinson’s disease or fallers like for example [
12,
18]. Although there are good results for combined use of multiple IMU, the recognition accuracy of the TUG phases with a single IMU can be improved and should be confirmed for larger study populations. Many studies used rule-based algorithms, while some others used logistic regression models for fall prediction [
19], dynamic time warping [
14] or for example feature selection [
12]. Until now, only a rather small minority use machine learning for the TUG classification like [
16]. However, in order to support a higher motion variety and motion anomalies, machine learning might be more suitable regarding different study populations, which differ for example in age, functional status or diseases, which affect the locomotor system. Additionally, these studies do not focus on settings beyond the laboratory, as well as automated self-assessments, except Milosevic et al. [
15]. However, Milosevic’s system needs the interaction of the user (start and stop record) since it cannot identify phases of the TUG execution automatically in a longer sequence.
Thus, we develop an activity recognition via machine learning and a rule-based algorithm, which detects both standardized TUG-sequences and similar sequences, which may occur in daily life and is more naturalistic than the standard TUG setup. We used one single IMU integrated into a belt to enable an easy use and an unobtrusive sensor placement, especially regarding future self-assessments at home. After the validation of our system under standardized conditions in a laboratory environment, we evaluate the suitability for future self-assessments by a non-standardized situation with similar movement patterns to the TUG test.
In contrast to the previous studies, we conducted a study with a larger sample size to cover common age-related varieties of motion patterns and corresponding anomalies. As the ground truth, we applied both clinical caregivers (stopwatch measurements) and the aTUG system. In comparison to Milosevic’s system, we chose a more unobtrusive and easier sensor placement than the chest. Our system can be used without assistance and interactions. Another major difference lies in the application of a machine learning algorithm instead of a rule-based algorithm. Since a high variance in movement patterns or strategies can occur, especially for transitions, in older adults, machine learning algorithms might be more robust than rule-based algorithms. If large datasets are available, which cover a majority of these variances, it is preferable to use machine learning. Rule-based algorithms need to be very complex to take different study populations into account, which differing in functional status or diseases. With increasing complexity, reading and adjusting a rule-based system becomes often cumbersome.
In summary, we want to develop an accurate system for automated mobility assessments for older people based on inertial TUG measurements, which is able to be used in clinical environments, as well as in future unsupervised self-assessments at home for a high variety of patients.
2. Materials and Methods
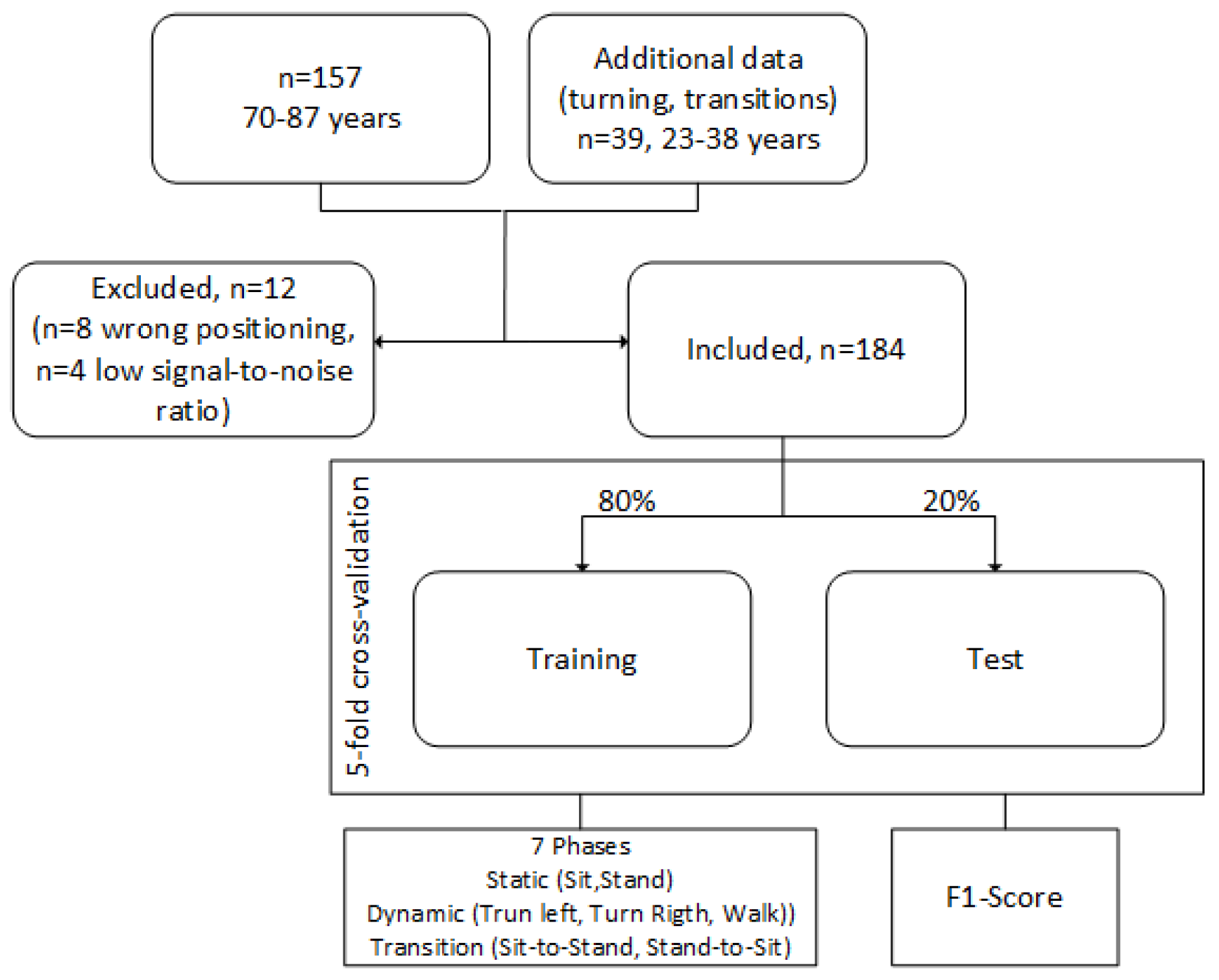
In order to evaluate an approach for automated measurement and analysis of the TUG test based on 3D accelerometer and 3D gyroscope data via machine learning, we included 157 participants in our study (87 female (59%), 60 male (41%)), aged 70 years and above.
Table 2 lists the characteristics of our study population. The data of 10 participants were excluded in this analysis, due to a low signal-to-noise ratio or a wrong positioning of the sensor (cf. also
Figure 2).
Besides the TUG test, the screening study consists of other different geriatric tests such as the Short Physical Performance Battery (SPPB), the Stair Climb Power Test (SCPT), the 6-min walk test, frailty criteria and counter movement lump. These tests were measured in a conventional way by medical professionals and additionally with ambient and wearable technology. More details are described in [
20]. The study has been approved by the appropriate ethics committees (ethical vote: Hannover Medical School, No. 6948; ethical vote: Carl von Ossietzky University, Drs.33/2016) and conducted in accordance with the Declaration of Helsinki.
We used a five-fold cross-validation. Therefore, our dataset was randomly divided into 5 equally-sized subsamples. One subsample (20% of the data) was retained as the validation data for testing the model, and the remaining 4 subsamples (80%) were used as training data. The cross-validation process was then repeated 5 times, with each of the 5 subsamples used once as the validation data.
Figure 2 illustrates the data used for our machine learning model. Due to optimization steps and to enable an increased sensitivity, we added additional data of a younger study population (
n = 39, 23–38 years) for left and right turnings, as well as sit-to-stand and stand-to-sit transitions, which were underrepresented in our dataset. Imbalanced data refer often to classification problems because standard classifiers tend to be overwhelmed by the large classes and ignore the small ones [
21]. Before this optimization step, data of these activities were underrepresented in comparison to walking and sitting.
The geriatric tests in our study were supported by technology. Thereby, the TUG was technically measured via the aTUG system and the sensor belt, which are described in the following.
2.1. aTUG System
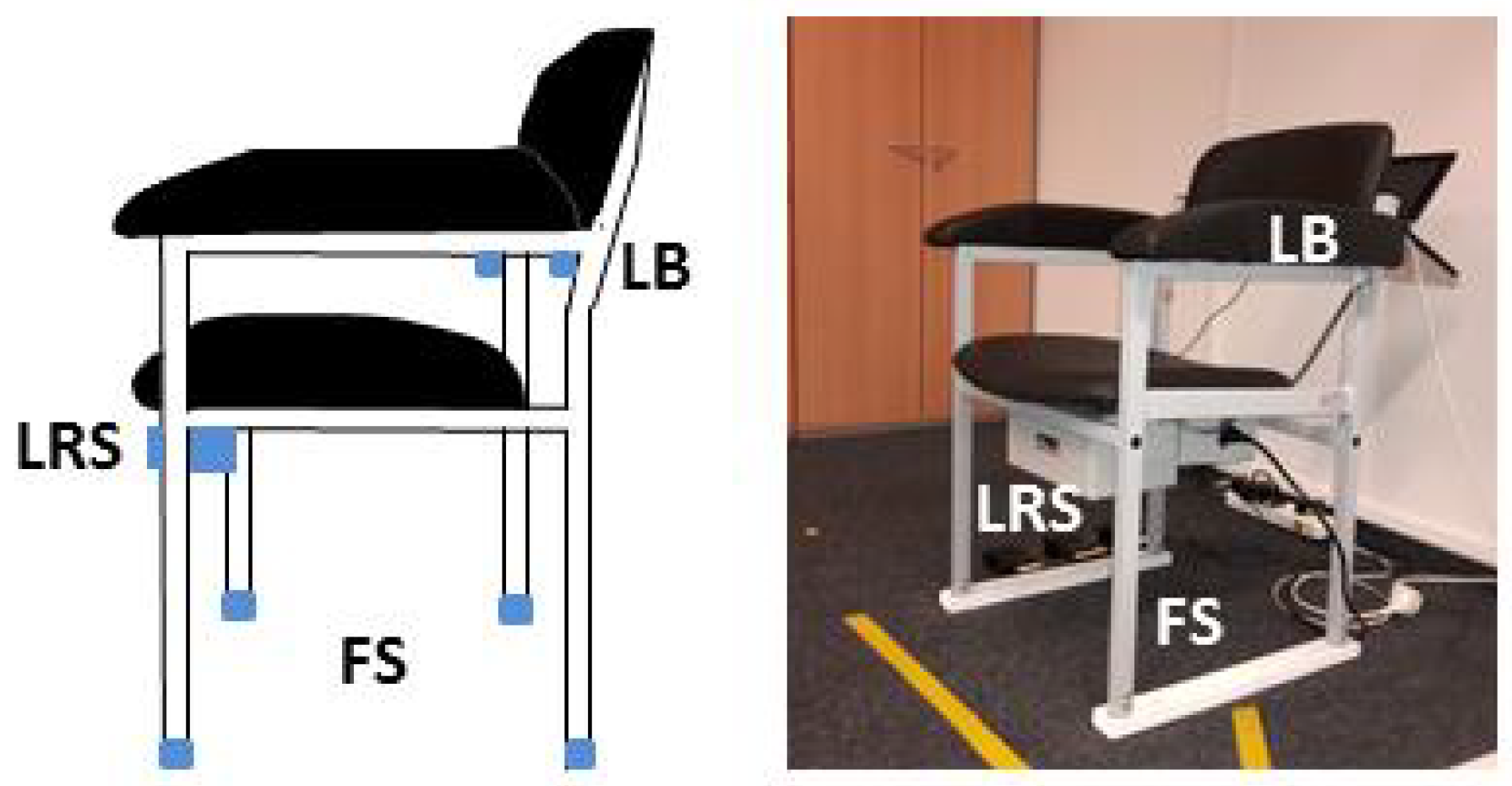
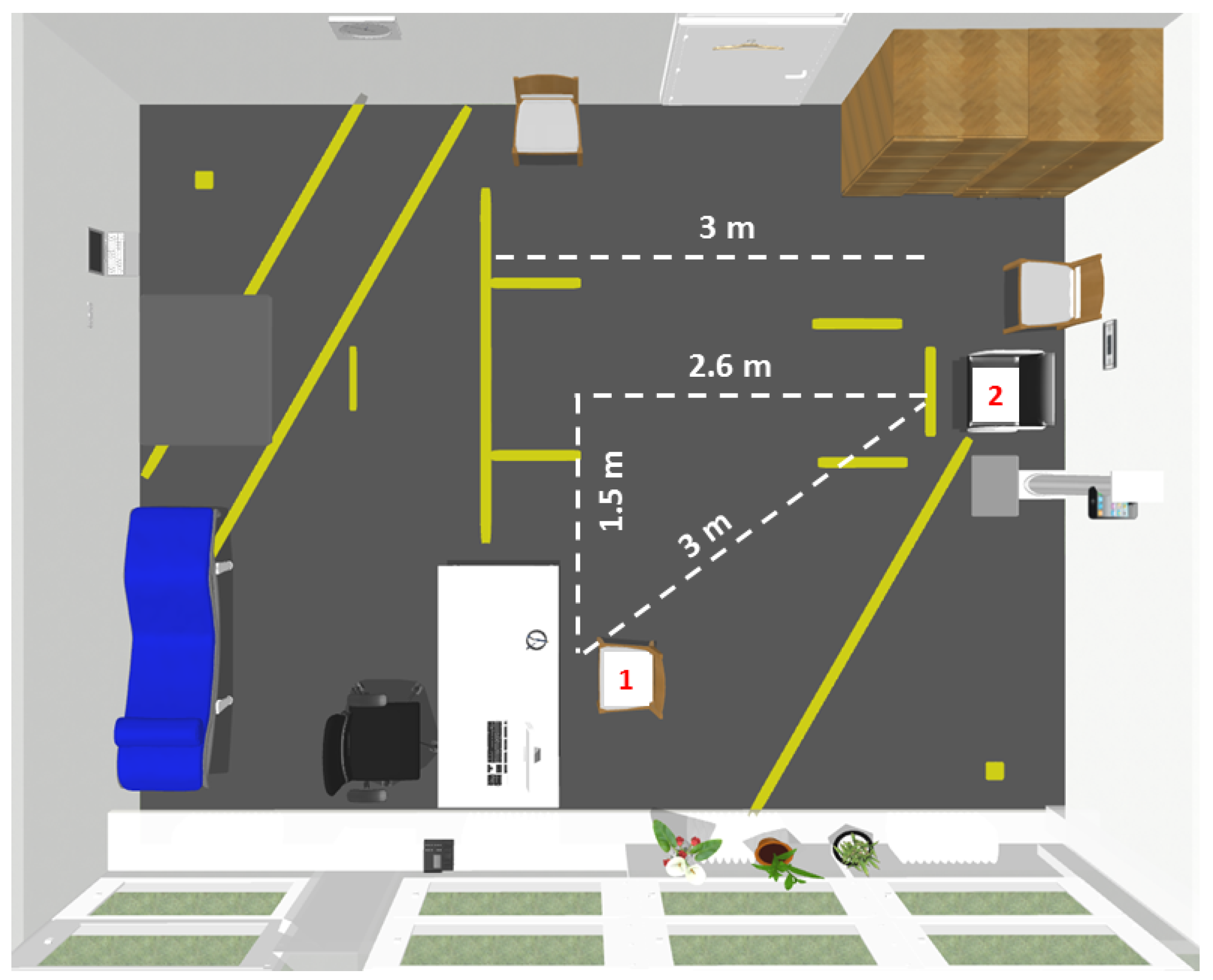
The aTUG system is illustrated in
Figure 3. It includes four force sensors (FS) in each chair leg, a laser range scanner (LRS) and a light barrier (LB). The force sensors (rated force: 1 kN, accuracy class: 1%) measure the force distribution on the chair. Especially the transitions (sit-to-stand, stand-to-sit) can be analyzed by these sensors. The TUG duration analysis by force sensors achieved a root mean square error (RMSE) of 0.90 s after calibration [
8]. The laser range scanner (Hokuyo UTM-30LX, Hokuyo Automatic Co., Ltd., Osaka, Japan) was used for gait analyses during the walking phases and the turning. Additionally, a light barrier (OSRAM LD271, OSRAM Opto Semiconductors GmbH, Regensburg, Germany) was mounted at the backrest of the chair to detect the beginning and end of the TUG test. All sensors are commercially available. The aTUG system is able to detect the duration of the TUG test with a mean error of 0.05 s and a standard deviation of 0.59 s [
22].
Due to its valid and precise measurements, the aTUG system is used as the reference system.
2.2. Sensor-Belt
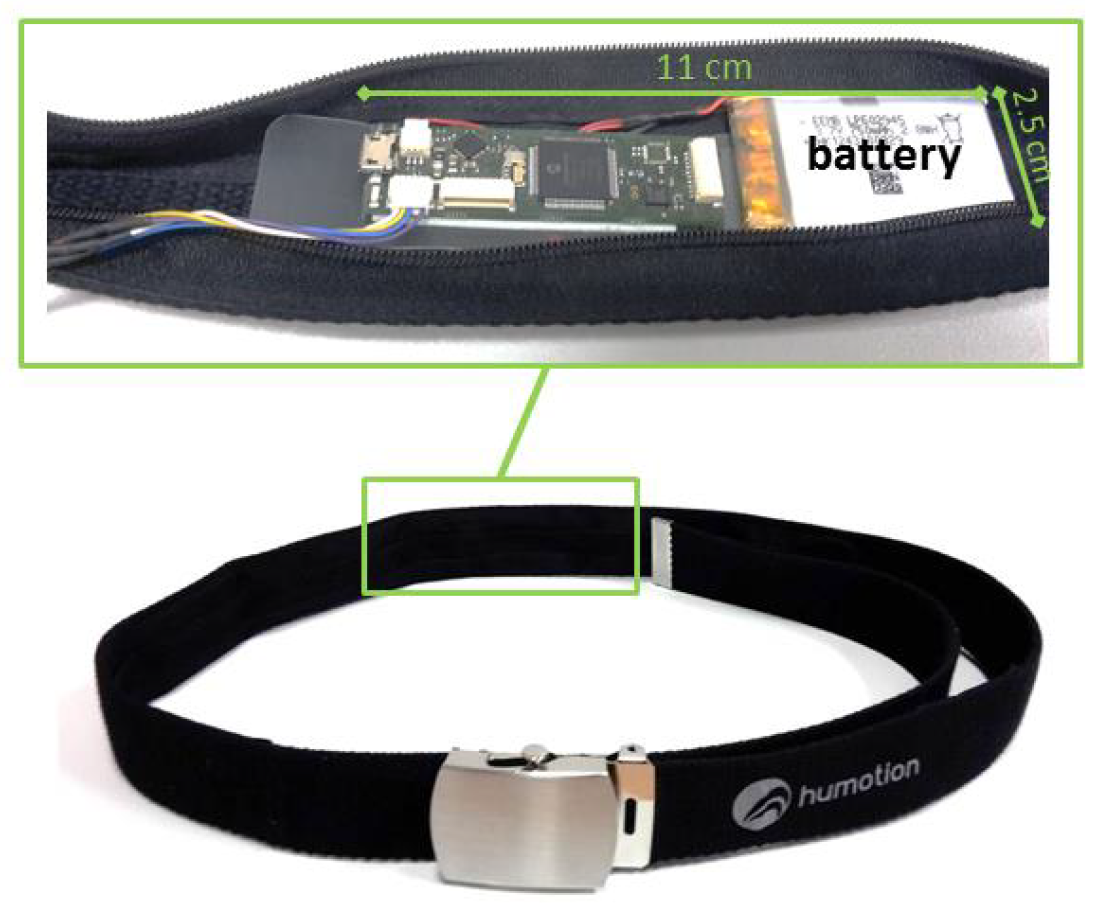
Besides the aTUG system, a wearable system was utilized, which is also commercially available.
Figure 4 shows the sensor system, which is integrated into a belt and worn at the hip. The dimension of the sensor unit is about 11 cm × 2.5 cm (battery included), and the overall weight of the belt is 140 g. This compact and light system enables an easy, unobtrusive and comfortable measurement. The sensor unit consists of a triaxial accelerometer (Bosch BMA180, Bosch Sensortec GmbH, Reutlingen, Germany), gyroscope (STMicroelectronics L3GD20H, STMicroelectronics, Geneva, Switzerland) and magnetometer, as well as a barometer. The sensitivity of the accelerometer is ±16G and the resolution 12 bit, while the sensitivity of the gyroscope lies at
deg ·
. We used a general sampling rate of 100 Hz in our study. The orientation of the sensors is illustrated in
Figure 1. The correct placement of the sensor belt, as well as the position of the sensor unit inside the belt were checked for each participant of our study by our physical therapists or study nurses and was adapted individually to ensure a correct alignment between the L3 and L5 lumbar vertebral body. Especially regarding our machine learning approach, a correct alignment is important for a good classification performance.
In our study, we used only the inertial sensors (accelerometer and gyroscope) to avoid over-fitting, because the magnetometer is highly influenced by environmental noise (metal chair). The barometer can be used to detect changes in height. However, since the accuracy lies about ±10 cm, the air pressure data were excluded due to their low additional information content.
2.3. Machine Learning and Algorithm
2.3.1. Pattern of TUG Test and Labeling
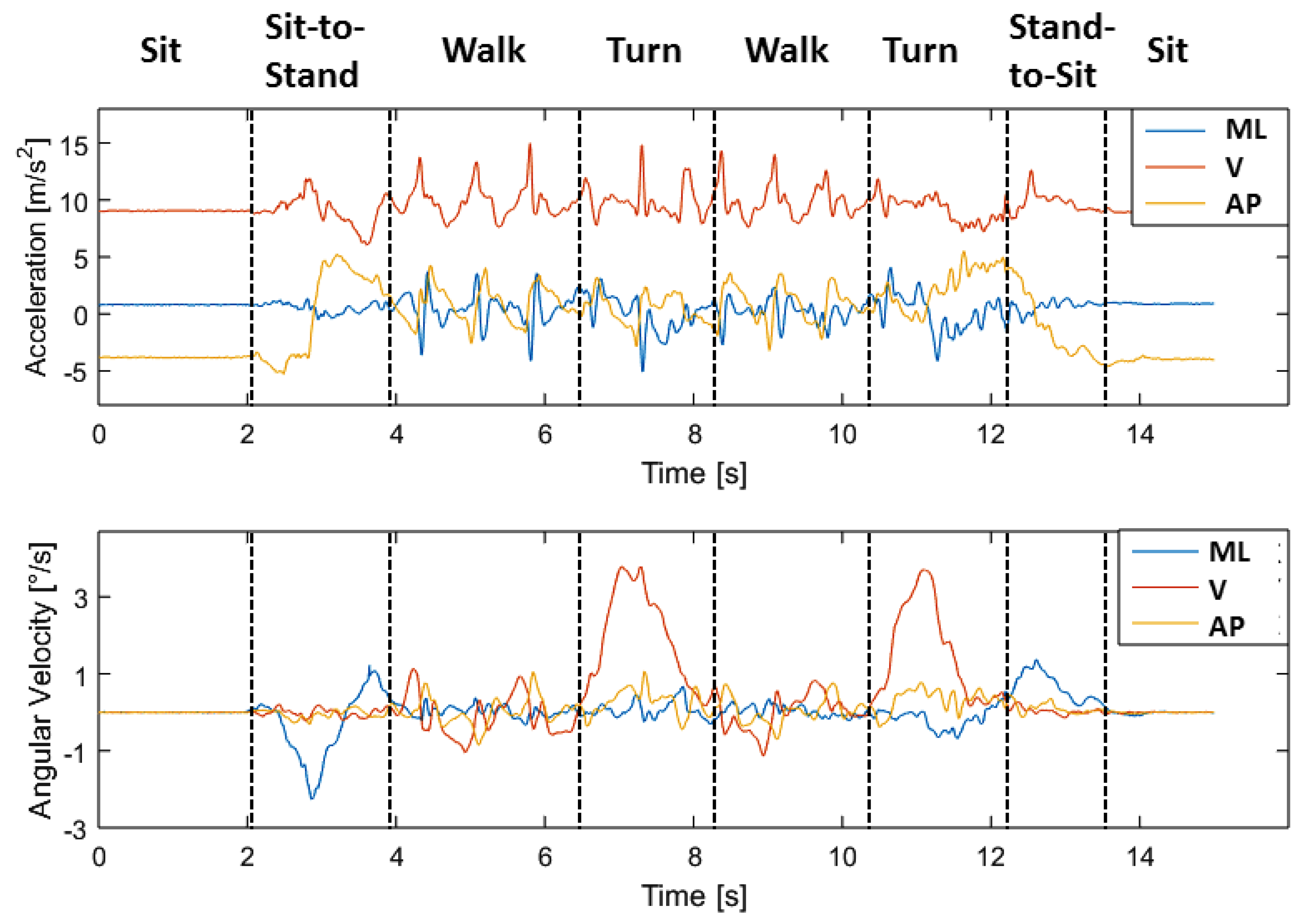
Figure 5 shows exemplarily the acceleration and gyroscope data of one person in three axes (vertical, mediolateral and anterior-posterior) during the TUG test. The coordinate orientation of the sensors is illustrated in
Figure 1. The different phases of the TUG are marked in
Figure 5. The static activity of sitting at the beginning and the end of the TUG can be easily recognized based on its nearly constant values of acceleration and angular velocity. Especially for the phases of turning, the gyroscope data in y-direction show significant peaks. The walking phases are characterized by peaks, which can be used for step detection. In the shown example are three steps before the participants starts the turning. The overall duration of this tests is about 12 s (14−2 s). The decision between turning and stand-to-sit at the end of the TUG test can be difficult, because of a possible overlay of these movements.
Supervised learning is a type of machine learning algorithm that uses a known dataset to make predictions for a new dataset. To create this training set, the TUG-phases are manually labeled by experts regarding their acceleration and gyroscope signals via a rule-based method. After labeling, features are derived for classification for each movement. In order to describe our algorithm, we will focus on the derived features, the sliding window and the classifier in the next subsection.
2.3.2. Hierarchical Classification Model
We developed a hierarchical model for classification (see
Figure 6). Therefore, four classifiers were trained. After a low pass filtering of the raw data, the first classifier (1) distinguished between static and dynamic activities, as well as transitions. If the state was classified, the other classifiers (2)–(4) characterized the activities in detail after filtering the raw data with the mentioned filters in
Table 3.
The features of the specific phases are extracted to characterize the movements. The used features are:
| • Auto Correlation (AC) | • Mean (M) |
| • Pitch (P) | • Standard Deviation (SD) |
| • Root Mean Square (RMS) | • Signal Energy (SE) |
| • Signal Magnitude Area (SMA) | • Signal Vector Magnitude (SVM) |
| • Spectral Entropy (SE) | • Correlation (C) |
A detailed description of each feature and its calculation can be found in [
23].
Since activity recognition requires a careful selection of feature combinations for classification, the number of features used is limited, so that only these are used, which significantly improves the classification model. This is done because, on the one hand, not every feature combination is suitable for each classification and, on the other hand, the computation time must remain efficient.
We used four different classification models to optimize our activity recognition: Boosted Decision Trees (BDT) [
24,
25], Boosted Decision Stump (BDS) [
26], Multilayer Perceptrons (MLP) [
27] and Adaptive Multi-Hyperplane Machine (AMM) [
28]. The
F1-score, recall, precision and accuracy are used for validations: the
F1-score is the harmonic mean of precision, and recall and is defined by:
where precision and recall are defined by:
and:
with
tp as true positive,
fp as false positive and
fn as false negative. The accuracy is defined by:
with
tn as true negative.
Table 3 sums up the parameters for our classifiers, which were determined after optimization analyses.
The methods, as well as the sliding window parameters and the feature sets are different for each classifier. The combinations with the best results are presented here (cf.
Table 4). Thereby, the features were calculated in each case for all components of Acceleration (Acc), Gyroscope (Gyro) or for both (Acc + Gyro).
2.4. TUG Analyses Algorithm
The raw data are classified via our hierarchical classification model as described in
Section 2.3.2. Since we want to detect complete TUG sequences, we used a rule-based model to identify the TUG test via its specific phases and their order. For this, the order of the automatically generated labels of the classified sub-activities will be checked. A valid TUG sequence consists of the following phases (see
Figure 1 and
Figure 5):
Sit-to-stand → walk → turn → walk → turn → stand-to-sit.
Since the sub-activities can be expected to include some classification errors, due to the false-positive rates of the trained classifiers (see
Table 4), and to take the variations of performing the TUG test into account, we included the following approach to increase the robustness of the algorithm. Nine models were specified as valid TUG sequences. Especially, doubled activities such as turn-turn were accepted as valid and were combined as one turn. Another valid model consisted of the combination sit-to-stand → stand-to-sit → walk, which is implausible and indicates a misclassification. Therefore, our model allows minor illogical classification errors. For example:
Especially regarding the aim to analyze further unsupervised-assessments in non-standardized settings, this more robust approach might be more applicable. A list of all models and their accuracies is presented in the Results
Section 3.3. The duration of each phase can be determined by these motion labels, as well as the overall duration of the TUG test. In the evaluationsection, we compare our results with stopwatch measurements by medical experts and the aTUG system.
4. Discussion
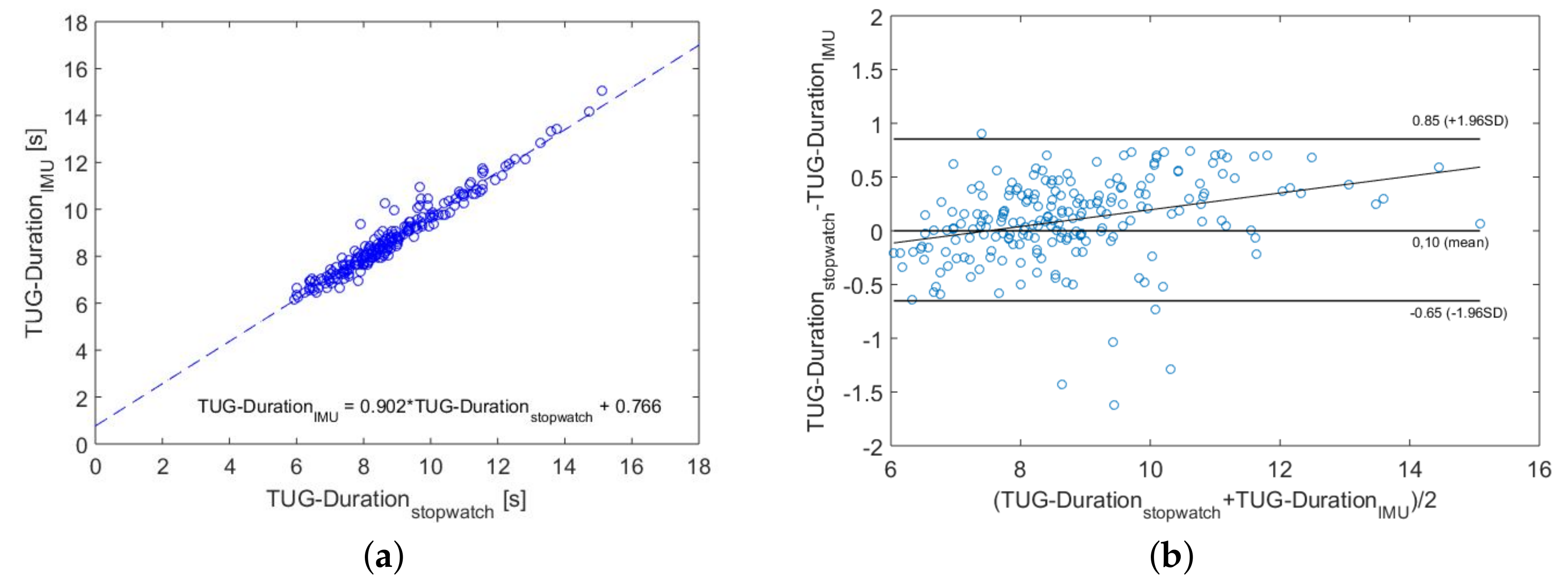
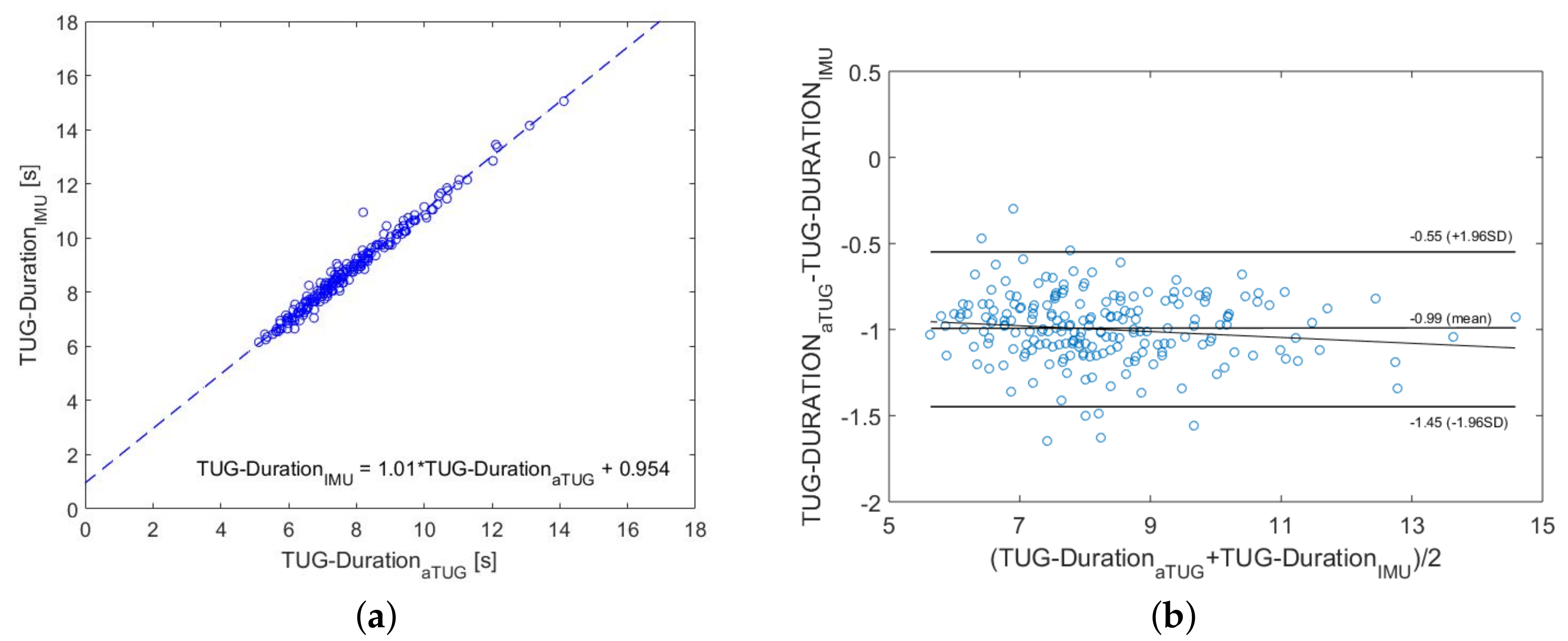
The main purpose of the present study was to develop an automated mobility assessments for older people based on inertial TUG measurements, which is able to be used in clinical environments, as well as in future unsupervised self-assessments at home. Therefore, we conducted a prospective study with 157 participants aged 70 and above and used the data to identify a suitable machine learning classifier for TUG-phases’ recognition. We achieved accuracies over 96% in the classification of the specific TUG components and for the complete TUG sequence recognition via a rule-based approach. In comparison to other studies, these results are satisfactory, especially regarding our minimalistic sensor system of one IMU, which was positioned in a belt at the hip. To validate our results, we compared the IMU-based data with two reference systems as the criterion standard, which showed significant correlations of 0.97 (stopwatch) and 0.99 (aTUG), respectively. This underlines the suitability of our system for clinical investigations. Thus, the system is a powerful, low-cost and accurate tool for automated TUG test analyses. Further analyses of the accuracy of our system to determine each TUG phase in terms of time, related to the reference system, should be done. This might be a valuable addition, especially for clinical issues, which addresses diseases with the influences of only specific phases of the TUG test.
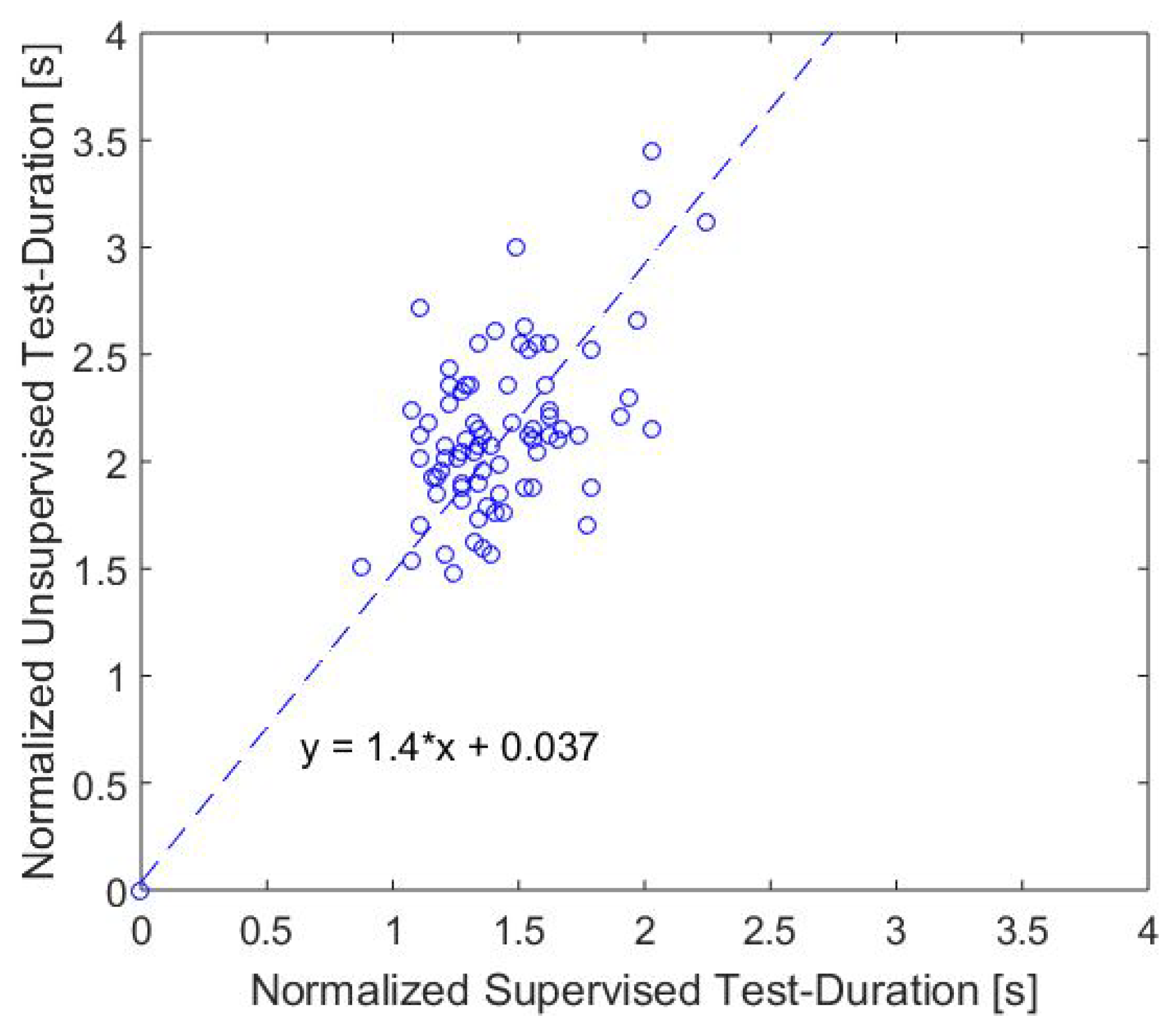
Since we want to detect both standardized TUG-sequences and similar sequences, which may occur in daily life and are more naturalistic than the standard TUG setup, we focused as an intermediate step to unsupervised home-assessments on a semi-unsupervised situation with similar sequences to the TUG test within the assessment. The most important limitation and simultaneously a great opportunity lie in our set of valid TUG models. On the one hand, this could lead to misclassifications in laboratory settings, but on the other hand, it allows detecting movement sequences that are similar to the TUG test. The comparison of the durations confirmed the expected result that the self-selected speed is lower in non-test situations, but there is a moderate correlation between these tests. Maybe the self-selected speed can be more sensitive to functional changes than assessments in a test situation, when a participant tries to perform particularly well. However, in our first analyses, we could not confirm this hypothesis. Correlation analyses between different geriatric tests and the TUG variations show a stronger correlation between the standard TUG test and the other tests than for the semi-unsupervised TUG. This had been expected, since a stronger correlation was expected between the test situations.
The attraction and the novelty of our approach lies in the combination of a high accuracy in TUG classification with only one single inertial measurement unit, the large study population, the automated analyses, the simplicity of our the system (no interaction required, easy to use) and the suitability of the investigation of unsupervised or rather unstandardized assessments.
The general suitability of our sensor system was investigated during a home-assessment following the clinical assessments, in which the participants wore the sensor-belt during the day for one week and wrote an activity diary. Most participants were able to load the battery and wear the belt in the correct position by themselves.
Further analyses of the home-assessment data are planed to analyze the significance regarding the detection of functional decline. Especially, the investigation of the single TUG phases in unsupervised situations might be worthwhile. In summary, our system is applicable for flexible measurement of the Timed Up and Go test performance in clinical settings, as well as in semi-unsupervised situations. The determined IMU-based test durations are in good agreement with the stopwatch measurements by medical experts and the aTUG-system. Assessments of non-standardized variations of TUG sequences might be a worthwhile enhancement for the identification of changes in the functional status, but need further investigations.

 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}