The Taste of Commercially Available Clarithromycin Oral Pharmaceutical Suspensions in the Palestinian Market: Electronic Tongue and In Vivo Evaluation

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Formulations
2.2. Chemical and Reagents
2.3. Instruments
2.4. Methods
2.4.1. Quality Control of Evaluated Suspensions
2.4.2. In Vitro Assessment of Taste Using ET
2.4.3. In Vivo Assessment of Taste
Study Design and Inclusion Criteria
Data Collection and Statistical Analysis
3. Results
3.1. Visual and Pharmacopoeial Assessment
3.2. ET Assessment
3.3. In Vivo Taste Assessment
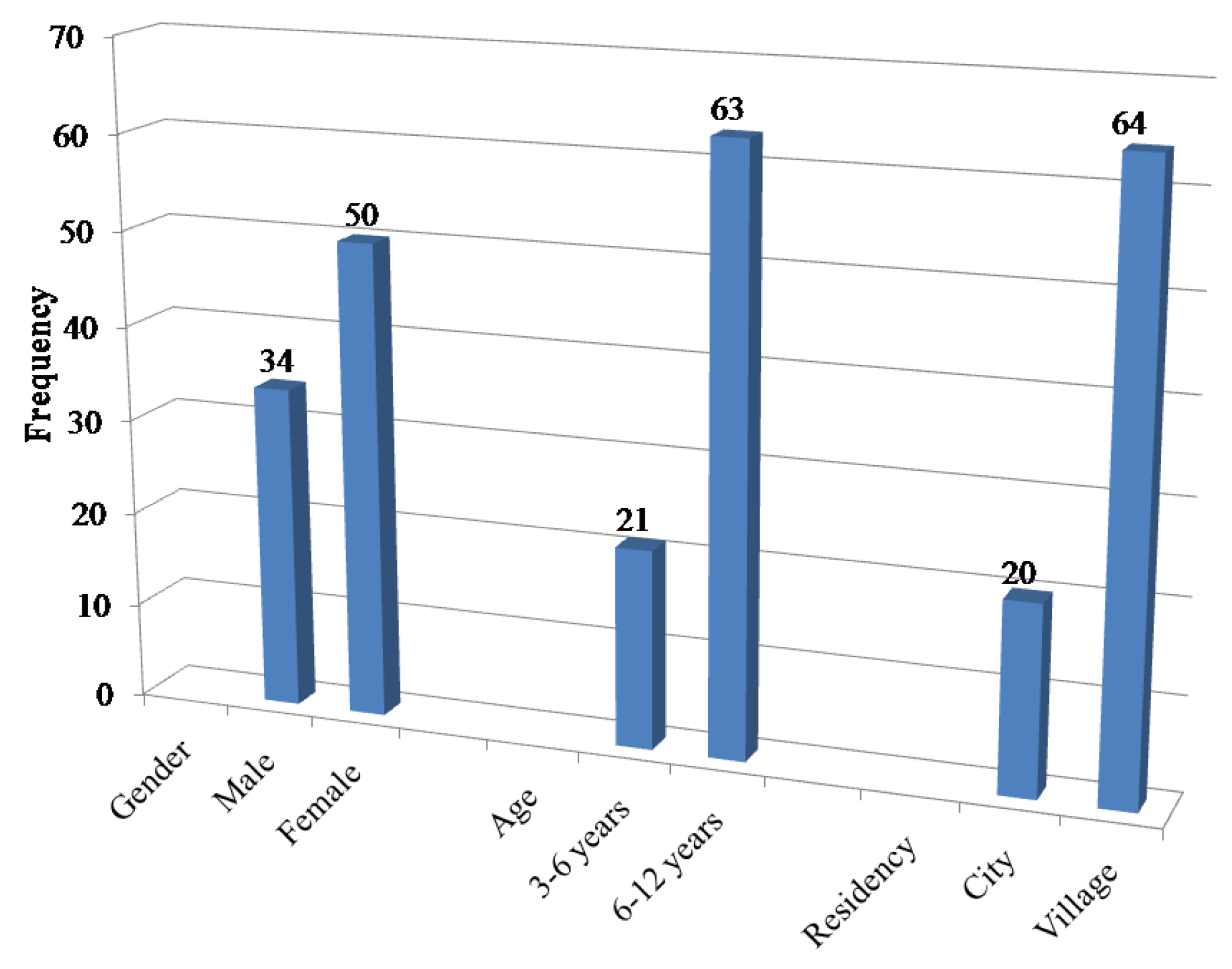
Demographic Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Ethical Statements
References
- Draft Guideline on Pharmaceutical Development of Medicines for Paediatric Use. EMA/CHMP/QWP/180157/2011 Committee for Medicinal Products for Human Use (CHMP). 2011. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2011/06/WC500107908.pdf (accessed on 24 December 2017).
- Hilton, M.J.; Thomas, K.V. Determination of selected human pharmaceutical compounds in effluent and surface water samples by high-performance liquid chromatography-electrospray tandem mass spectrometry. J. Chromatogr. A 2003, 1015, 129–141. [Google Scholar] [CrossRef]
- Peng, F.; Wang, W.; Luo, W.; Liu, Y.; Li, H. Application of near-infrared spectroscopy for monitoring the formulation process of low-dose tablets. Anal. Methods 2014, 6, 1905–1913. [Google Scholar] [CrossRef]
- Mohamed-Ahmed, A.H.; Soto, J.; Ernest, T.; Tuleu, C. Non-human tools for the evaluation of bitter taste in the design and development of medicines: A systematic review. Drug Discov. Today 2016, 21, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.N.; Khar, R.K.; Ajayakumar, P. Diffuse reflectance near infrared-chemometric methods development and validation of amoxicillin capsule formulations. J. Pharm. Bioallied Sci. 2016, 8, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Zontov, Y.; Balyklova, K.; Titova, A.; Rodionova, O.Y.; Pomerantsev, A. Chemometric aided nir portable instrument for rapid assessment of medicine quality. J. Pharm. Biomed. Anal. 2016, 131, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Jank, L.; Martins, M.T.; Arsand, J.B.; Motta, T.M.C.; Feijó, T.C.; dos Santos Castilhos, T.; Hoff, R.B.; Barreto, F.; Pizzolato, T.M. Liquid chromatography-tandem mass spectrometry multiclass method for 46 antibiotics residues in milk and meat: Development and validation. Food Anal. Methods 2017, 10, 2152–2164. [Google Scholar] [CrossRef]
- Vlasov, Y.; Legin, A.; Rudnitskaya, A.; Di Natale, C.; D’amico, A. Nonspecific sensor arrays (“electronic tongue”) for chemical analysis of liquids (IUPAC technical report). Pure Appl. Chem. 2005, 77, 1965–1983. [Google Scholar] [CrossRef]
- Gebicki, J. Application of electrochemical sensors and sensor matrixes for measurement of odorous chemical compounds. Trends Anal. Chem. 2016, 77, 1–13. [Google Scholar] [CrossRef]
- Cetó, X.; González-Calabuig, A.; Crespo, N.; Pérez, S.; Capdevila, J.; Puig-Pujol, A.; del Valle, M. Electronic tongues to assess wine sensory descriptors. Talanta 2017, 162, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Preedy, V.R.; Mendez, M.L.R. Electronic Noses and Tongues in Food Science; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Smyth, H.; Cozzolino, D. Instrumental methods (spectroscopy, electronic nose, and tongue) as tools to predict taste and aroma in beverages: Advantages and limitations. Chem. Rev. 2012, 113, 1429–1440. [Google Scholar] [CrossRef] [PubMed]
- Kirsanov, D.; Korepanov, A.; Dorovenko, D.; Legin, E.; Legin, A. Indirect monitoring of protein a biosynthesis in E. coli using potentiometric multisensor system. Sens. Actuator B Chem. 2017, 238, 1159–1164. [Google Scholar] [CrossRef]
- Del Valle, M. Materials for electronic tongues: Smart sensor combining different materials and chemometric tools. In Mater Chemlsens; Springer: Berlin/Heidelberg, Germany, 2017; pp. 227–265. [Google Scholar]
- Altan, S.; Francois, M.; Inghelbrecht, S.; Manola, A.; Shen, Y. An application of serially balanced designs for the study of known taste samples with the α-astree electronic tongue. AAPS PharmSciTech 2014, 15, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Legin, A.; Rudnitskaya, A.; Clapham, D.; Seleznev, B.; Lord, K.; Vlasov, Y. Electronic tongue for pharmaceutical analytics: Quantification of tastes and masking effects. Anal Bioanal. Chem. 2004, 380, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Abu-Khalaf, N.; Iversen, J.J.L. Calibration of a sensor array (an electronic tongue) for identification and quantification of odorants from livestock buildings. Sensors 2007, 7, 103–128. [Google Scholar] [CrossRef]
- Abu-Khalaf, N.; Iversen, J.J.L. Classification of mixtures of odorants from livestock buildings by a sensor array (an electronic tongue). Sensors 2007, 7, 129–143. [Google Scholar] [CrossRef]
- Baldwin, E.A.; Bai, J.; Plotto, A.; Dea, S. Electronic noses and tongues: Applications for the food and pharmaceutical industries. Sensors 2011, 11, 4744–4766. [Google Scholar] [CrossRef] [PubMed]
- Eckert, C.; Lutz, C.; Breitkreutz, J.; Woertz, K. Quality control of oral herbal products by an electronic tongue—Case study on sage lozenges. Sens. Actuator B Chem. 2011, 156, 204–212. [Google Scholar] [CrossRef]
- Woertz, K.; Tissen, C.; Kleinebudde, P.; Breitkreutz, J. A comparative study on two electronic tongues for pharmaceutical formulation development. J. Pharm. Biomed. Anal. 2011, 55, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Kutyła-Olesiuk, A.; Wawrzyniak, U.E.; Ciosek, P.; Wróblewski, W. Electrochemical monitoring of citric acid production by aspergillusniger. Anal Chim. Acta 2014, 823, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Sliwinska, M.; Wisniewska, P.; Dymerski, T.; Namiesnik, J.; Wardencki, W. Food analysis using artificial senses. J. Agric. Food Chem. 2014, 62, 1423–1448. [Google Scholar] [CrossRef] [PubMed]
- Wiziack, N.K.; Soares, J.C.; Padovan, B.D.; Oliveira, O.N., Jr.; Leite, F.L. Electronic tongue: Applications and advances. In Advances in Biosensors Research; Nova Science Publishers: Hauppauge, NY, USA, 2014. [Google Scholar]
- Woertz, K.; Tissen, C.; Kleinebudde, P.; Breitkreutz, J. Taste sensing systems (electronic tongues) for pharmaceutical applications. Int. J. Pharm. 2011, 417, 256–271. [Google Scholar] [CrossRef] [PubMed]
- Pein, M.; Preis, M.; Eckert, C.; Kiene, F.E. Taste-masking assessment of solid oral dosage forms—A critical review. Int. J. Pharm. 2014, 465, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Woertz, K.; Tissen, C.; Kleinebudde, P.; Breitkreutz, J. Performance qualification of an electronic tongue based on ICH guideline Q2. J. Pharm. Biomed. Anal. 2010, 51, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Medicine, N.L.O. Macrolide Antibiotics. Available online: https://livertox.nih.gov/MacrolideAntibiotics.htm (accessed on 11 April 2017).
- Tuberculosis Clarithromycin. Available online: http://www.tuberculosisjournal.com/article/S1472-9792(08)70005-2/abstract (accessed on 12 April 2017).
- Uchida, T.; Tanigake, A.; Miyanaga, Y.; Matsuyama, K.; Kunitomo, M.; Kobayashi, Y.; Ikezaki, H.; Taniguchi, A. Evaluation of the bitterness of antibiotics using a taste sensor. J. Pharm. Pharmacol. 2003, 55, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Pharmacopoeia Clarithromycin for Oral Suspension. Available online: http://www.drugfuture.com/Pharmacopoeia/usp36/PDF/1702-1703.pdf (accessed on 12 April 2017).
- Anand, V.; Kharb, V.; Kataria, M.; Kukka, V.; Choudhury, P.K. Taste assessment trials for sensory analysis of oral pharmaceutical products. Pak. J. Pharm. Sci. 2008, 21, 438–450. [Google Scholar] [PubMed]
- Gee, S.C.; Hagemann, T.M. Palatability of liquid anti-infectives: Clinician and student perceptions and practice outcomes. J. Pediatr. Pharmacol. Ther. 2007, 12, 216–223. [Google Scholar] [PubMed]
- Bagger-Sjöbäck, D.; Bondesson, G. Taste evaluation and compliance of two paediatric formulations of phenoxymethylpenicillin in children. Scand. J. Prim. Health Care 1989, 7, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Zhang, B.; Hu, L.; Zhuang, L.; Hu, N.; Wang, P. A novel bioelectronic tongue in vivo for highly sensitive bitterness detection with brain-machine interface. Biosens. Bioelectron. 2016, 78, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Ha, D.; Sun, Q.; Su, K.; Wan, H.; Li, H.; Xu, N.; Sun, F.; Zhuang, L.; Hu, N.; Wang, P. Recent achievements in electronic tongue and bioelectronic tongue as taste sensors. Sens. Actuator B Chem. 2015, 207, 1136–1146. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Product Name | Reference | Distance | p-Value | Pattern Discrimination Index (%) |
|---|---|---|---|---|---|
| 1 | K1 | Klacid® | 0.64 | <0.001 | 8.81 |
| 2 | K1 | K2 | 2.78 | <0.001 | 65.75 |
| 3 | Klacid® | K2 | 3.13 | <0.001 | 71.94 |
| Variable | Klacid Median (Q1–Q3) | K1 Median (Q1–Q3) | K2 Median (Q1–Q3) | p-Value |
|---|---|---|---|---|
| Colour | 4.5 (4–5) | 4 (3–5) | 4 (4–5) | 0.382 |
| Smell | 4 (3–5) | 4.5 (3–5) | 4 (4–5) | 0.209 |
| Taste | 1.5 (1–3) | 1 (1–3) | 1 (1–1) | 0.011 |
| General acceptance | 3 (1–4) | 3 (2–3.75) | 1.5 (1–2.75) | 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Khalaf, N.; Zaid, A.N.; Jaradat, N.; AlKilany, A.; Abu Rumaila, B.; Al Ramahi, R.; Shweiki, S.; Nidal, S.; Surakhi, N. The Taste of Commercially Available Clarithromycin Oral Pharmaceutical Suspensions in the Palestinian Market: Electronic Tongue and In Vivo Evaluation. Sensors 2018, 18, 454. https://doi.org/10.3390/s18020454
Abu-Khalaf N, Zaid AN, Jaradat N, AlKilany A, Abu Rumaila B, Al Ramahi R, Shweiki S, Nidal S, Surakhi N. The Taste of Commercially Available Clarithromycin Oral Pharmaceutical Suspensions in the Palestinian Market: Electronic Tongue and In Vivo Evaluation. Sensors. 2018; 18(2):454. https://doi.org/10.3390/s18020454
Chicago/Turabian StyleAbu-Khalaf, Nawaf, Abdel Naser Zaid, Nidal Jaradat, Alaaldin AlKilany, Basima Abu Rumaila, Rowa Al Ramahi, Shrouq Shweiki, Safaa Nidal, and Nibal Surakhi. 2018. "The Taste of Commercially Available Clarithromycin Oral Pharmaceutical Suspensions in the Palestinian Market: Electronic Tongue and In Vivo Evaluation" Sensors 18, no. 2: 454. https://doi.org/10.3390/s18020454