Disentangling the Contribution of Spatial Reference Frames to Executive Functioning in Healthy and Pathological Aging: An Experimental Study with Virtual Reality


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Executive Functions Assessment
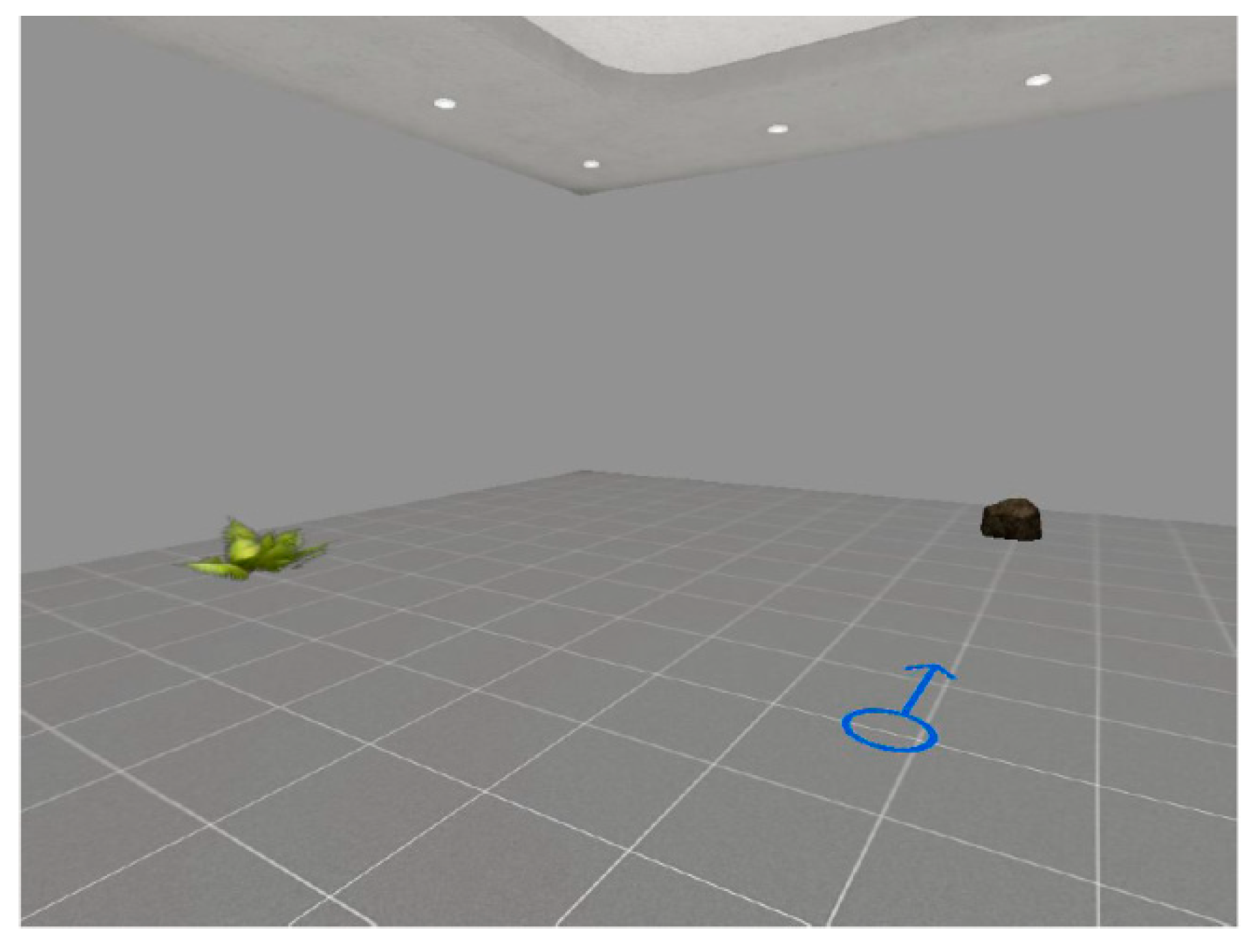
2.3. Virtual Reality Procedure
2.4. Procedure
2.5. Data Analyses
3. Results
Group Differences Executive Functions and Spatial Reference Frames
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Klatzky, R.L. Allocentric and egocentric spatial representations: Definitions, distinctions, and interconnections. In Spatial Cognition. An Interdisciplinary Approach to Representing and Processing Spatial Knowledge; Freksa, C., Habel, C., Wender, K.F., Eds.; Springer: Berlin/Heidelberg, Germany, 1998; pp. 1–17. [Google Scholar]
- Paillard, J. Brain and Space; OxfordScience Publications: Oxford, UK, 1991. [Google Scholar]
- Gallistel, C.R. Language and spatial frames of reference in mind and brain. Trends Cogn. Sci. 2002, 6, 321–322. [Google Scholar] [CrossRef] [Green Version]
- Shelton, A.L.; McNamara, T.P. Systems of spatial reference in human memory. Cogn. Psychol. 2001, 43, 274–310. [Google Scholar] [CrossRef] [PubMed]
- Galati, G.; Pelle, G.; Berthoz, A.; Committeri, G. Multiple reference frames used by the human brain for spatial perception and memory. Exp. Brain Res. 2010, 206, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Byrne, P.; Becker, S.; Burgess, N. Remembering the past and imagining the future: A neural model of spatial memory and imagery. Psychol. Rev. 2007, 114, 340. [Google Scholar] [CrossRef] [PubMed]
- Acredolo, L.P. Developmental changes in the ability to coordinate perspectives of a large-scale space. Dev. Psychol. 1977, 13, 1. [Google Scholar] [CrossRef]
- Piaget, J. He Child’s Conception of the World. London: Kegan Paul Trench Trubner; Original Work Published in 1926; La Concorde: Lausanne, Switzerland, 1929. [Google Scholar]
- Burgess, N. Spatial memory: How egocentric and allocentric combine. Trends Cogn. Sci. 2006, 10, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Zaehle, T.; Jordan, K.; Wüstenberg, T.; Baudewig, J.; Dechent, P.; Mast, F.W. The neural basis of the egocentric and allocentric spatial frame of reference. Brain Res. 2007, 1137, 92–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchette, S.A.; Vass, L.K.; Ryan, J.; Epstein, R.A. Anchoring the neural compass: Coding of local spatial reference frames in human medial parietal lobe. Nat. Neurosci. 2014, 17, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Riva, G. Getting lost in Alzheimer’s Disease: A break in the mental frame syncing. Med. Hypotheses 2013, 80, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Riva, G. What is the role of spatial processing in the decline of episodic memory in Alzheimer’s Disease? The “mental frame syncing” hypothesis. Front. Aging Neurosci. 2014, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Riva, G. The proactive self in space: How egocentric and allocentric spatial impairments contribute to anosognosia in Alzheimer’s Disease. J. Alzheimers Dis. 2016, 55, 881–892. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Cipresso, P.; Morganti, F.; Riva, G. The role of egocentric and allocentric abilities in Alzheimer’s Disease: A systematic review. Ageing Res. Rev. 2014, 16, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Lithfous, S.; Dufour, A.; Després, O. Spatial navigation in normal aging and the prodromal stage of Alzheimer’s Disease: Insights from imaging and behavioral studies. Ageing Res. Rev. 2013, 12, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Braak, E. Neuropathological stageing of alzheimer-related changes. Acta Neuropathol. 1991, 82, 239–259. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Braak, E. Evolution of the neuropathology of Alzheimer’s Disease. Acta Neurol. Scand. 1996, 94, 3–12. [Google Scholar] [CrossRef]
- Alafuzoff, I.; Arzberger, T.; Al-Sarraj, S.; Bodi, I.; Bogdanovic, N.; Braak, H.; Bugiani, O.; DelTredici, K.; Ferrer, I.; Gelpi, E. Staging of neurofibrillary pathology in Alzheimer’s Disease: A study of the brainnet europe consortium. Brain Pathol. 2008, 18, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Dickson, D.W. The pathogenesis of senile plaques. J. Neuropathol. Exp. Neurol. 1997, 56, 321–339. [Google Scholar] [CrossRef] [PubMed]
- Thal, D.R.; Rüb, U.; Schultz, C.; Sassin, I.; Ghebremedhin, E.; Del Tredici, K.; Braak, E.; Braak, H. Sequence of aβ protein deposition in the human medial temporal lobe. J. Neuropathol. Exp. Neurol. 2000, 59, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Wolbers, T.; Dudchenko, P.A.; Wood, E.R. Spatial memory-a unique window into healthy and pathological aging. Front. Aging Neurosci. 2014, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Iachini, I.; Iavarone, A.; Senese, V.P.; Ruotolo, F.; Ruggiero, G. Visuospatial memory in healthy elderly, ad and mci: A review. Curr. Aging Sci. 2009, 2, 43–59. [Google Scholar] [CrossRef] [PubMed]
- Nemmi, F.; Boccia, M.; Guariglia, C. Does aging affect the formation of new topographical memories? Evidence from an extensive spatial training. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2017, 24, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Gazova, I.; Laczó, J.; Rubinova, E.; Mokrisova, I.; Hyncicova, E.; Andel, R.; Vyhnalek, M.; Sheardova, K.; Coulson, E.J.; Hort, J. Spatial navigation in young versus older adults. Front. Aging Neurosci. 2013, 5, 94. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, G.; D’Errico, O.; Iachini, T. Development of egocentric and allocentric spatial representations from childhood to elderly age. Psychol. Res. 2016, 80, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Montefinese, M.; Sulpizio, V.; Galati, G.; Committeri, G. Age-related effects on spatial memory across viewpoint changes relative to different reference frames. Psychol. Res. 2015, 79, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Wiener, J.M.; Kmecova, H.; de Condappa, O. Route repetition and route retracing: Effects of cognitive aging. Front. Aging Neurosci. 2012, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Laczó, J.; Andel, R.; Nedelska, Z.; Vyhnalek, M.; Vlcek, K.; Crutch, S.; Harrison, J.; Hort, J. Exploring the contribution of spatial navigation to cognitive functioning in older adults. Neurobiol. Aging 2017, 51, 67–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moffat, S.D.; Elkins, W.; Resnick, S.M. Age differences in the neural systems supporting human allocentric spatial navigation. Neurobiol. Aging 2006, 27, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Moffat, S.D.; Kennedy, K.M.; Rodrigue, K.M.; Raz, N. Extrahippocampal contributions to age differences in human spatial navigation. Cereb. Cortex 2006, 17, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403. [Google Scholar] [CrossRef] [PubMed]
- Finkel, D.; Reynolds, C.A.; McArdle, J.J.; Pedersen, N.L. Age changes in processing speed as a leading indicator of cognitive aging. Psychol. Aging 2007, 22, 558. [Google Scholar] [CrossRef] [PubMed]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752. [Google Scholar] [CrossRef] [PubMed]
- Bosco, A.; Picucci, L.; Caffo, A.O.; Lancioni, G.E.; Gyselinck, V. Assessing human reorientation ability inside virtual reality environments: The effects of retention interval and landmark characteristics. Cogn. Process. 2008, 9, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Caffò, A.O.; De Caro, M.F.; Picucci, L.; Notarnicola, A.; Settanni, A.; Livrea, P.; Lancioni, G.E.; Bosco, A. Reorientation deficits are associated with amnestic mild cognitive impairment. Am. J. Alzheimers Dis. Other Dement. 2012, 27, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Pedroli, E.; Tuena, C.; De Leo, G.; Stramba-Badiale, M.; Goulene, K.; Mariotti, N.G.; Riva, G. A novel virtual reality-based training protocol for the enhancement of the “mental frame syncing” in individuals with Alzheimer’s Disease: A development-of-concept trial. Front. Aging Neurosci. 2017, 9, 240. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Riva, G. How different spatial representations interact in virtual environments: The role of mental frame syncing. Cogn. Process. 2015, 16, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Morganti, F.; Di Stefano, F.; Riva, G. Detecting early egocentric and allocentric impairments deficits in Alzheimer’s Disease: An experimental study with virtual reality. Front. Aging Neurosci. 2015, 7, 88. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Robins, L.N.; Helzer, J.E. The mini-mental state examination. Arch. Gen. Psychiatry 1983, 40, 812. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s Disease report of the nincds-adrda work group* under the auspices of department of health and human services task force on Alzheimer’s Disease. Neurology 1984, 34, 939. [Google Scholar] [CrossRef] [PubMed]
- Brazzelli, M.; Capitani, E.; Della Sala, S.; Spinnler, H.; Zuffi, M. A neuropsychological instrument adding to the description of patients with suspected cortical dementia: The milan overall dementia assessment. J. Neurol. Neurosurg. Psychiatry 1994, 57, 1510–1517. [Google Scholar] [CrossRef] [PubMed]
- Shallice, T. Specific impairments of planning. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1982, 298, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail making test: Normative values from 287 normal adult controls. Ital. J. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Cipresso, P.; Serino, S.; Pallavicini, P.; Gaggioli, A.; Riva, G. Neurovirtual 3d: A multiplatform 3d simulation system for application in psychology and neuro-rehabilitation. In Virtual, Augmented Reality and Serious Games for Healthcare 1; Springer: Berlin, Germany, 2014; pp. 275–286. [Google Scholar]
- Riva, G.; Gaggioli, A.; Grassi, A.; Raspelli, S.; Cipresso, P.; Pallavicini, F.; Vigna, C.; Gagliati, A.; Gasco, S.; Donvito, G. NeuroVR 2-A free virtual reality platform for the assessment and treatment in behavioral health care. In Studies in Health Technology and Informatics; IOS Press: Amsterdam, The Netherlands, 2011; Volume 163, pp. 493–495. [Google Scholar]
- Ahrmeir, L.; Tutz, G. Multivariate Statistical Modelling Based on Generalized Linear Models; Springer Science & Business Media: Berlin, Germany, 2013. [Google Scholar]
- Colombo, D.; Serino, S.; Tuena, C.; Pedroli, E.; Dakanalis, A.; Cipresso, P.; Riva, G. Egocentric and allocentric spatial reference frames in aging: A systematic review. Neurosci. Biobehav. Rev. 2017, 80, 605–621. [Google Scholar] [CrossRef] [PubMed]
- West, R. In defense of the frontal lobe hypothesis of cognitive aging. J. Int. Neuropsychol. Soc. 2000, 6, 727–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, R.L. An application of prefrontal cortex function theory to cognitive aging. Psychol. Bull. 1996, 120, 272. [Google Scholar] [CrossRef] [PubMed]
- Allison, S.L.; Fagan, A.M.; Morris, J.C.; Head, D. Spatial navigation in preclinical Alzheimer’s Disease. J. Alzheimers Dis. 2016, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Gazova, I.; Vlcek, K.; Laczo, J.; Nedelska, Z.; Hyncicova, E.; Mokrisova, I.; Sheardova, K.; Hort, J. Spatial navigation—A unique window into physiological and pathological aging. Front. Aging Neurosci. 2012, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Boccia, M.; Silveri, M.C.; Sabatini, U.; Guariglia, C.; Nemmi, F. Neural underpinnings of the decline of topographical memory in mild cognitive impairment. Am. J. Alzheimers Dis. Other Dement. 2016, 31, 618–630. [Google Scholar] [CrossRef] [PubMed]
- Baudic, S.; Dalla Barba, G.; Thibaudet, M.C.; Smagghe, A.; Remy, P.; Traykov, L. Executive function deficits in early Alzheimer’s Disease and their relations with episodic memory. Arch. Clin. Neuropsychol. 2006, 21, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Binetti, G.; Magni, E.; Padovani, A.; Cappa, S.F.; Bianchetti, A.; Trabucchi, M. Executive dysfunction in early Alzheimer’s Disease. J. Neurol. Neurosurg. Psychiatry 1996, 60, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Collette, F.; Van der Linden, M.; Salmon, E. Executive dysfunction in Alzheimer’s Disease. Cortex 1999, 35, 57–72. [Google Scholar] [CrossRef]
- Lafleche, G.; Albert, M.S. Executive function deficits in mild Alzheimer’s Disease. Neuropsychology 1995, 9, 313. [Google Scholar] [CrossRef]
- Possin, K.L.; Feigenbaum, D.; Rankin, K.P.; Smith, G.E.; Boxer, A.L.; Wood, K.; Hanna, S.M.; Miller, B.L.; Kramer, J.H. Dissociable executive functions in behavioral variant frontotemporal and alzheimer dementias. Neurology 2013, 80, 2180–2185. [Google Scholar] [CrossRef] [PubMed]
- Bastin, C.; Salmon, E. Early neuropsychological detection of Alzheimer’s Disease. Eur. J. Clin. Nutr. 2014, 68, 1192. [Google Scholar] [CrossRef] [PubMed]
- Morganti, F.; Stefanini, S.; Riva, G. From allo-to egocentric spatial ability in early Alzheimer’s Disease: A study with virtual reality spatial tasks. Cogn. Neurosci. 2013, 4, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Jernigan, T.L.; Archibald, S.L.; Fennema-Notestine, C.; Gamst, A.C.; Stout, J.C.; Bonner, J.; Hesselink, J.R. Effects of age on tissues and regions of the cerebrum and cerebellum. Neurobiol. Aging 2001, 22, 581–594. [Google Scholar] [CrossRef] [Green Version]
- Raz, N.; Lindenberger, U.; Rodrigue, K.M.; Kennedy, K.M.; Head, D.; Williamson, A.; Dahle, C.; Gerstorf, D.; Acker, J.D. Regional brain changes in aging healthy adults: General trends, individual differences and modifiers. Cereb. Cortex 2005, 15, 1676–1689. [Google Scholar] [CrossRef] [PubMed]
- Park, D.C.; Reuter-Lorenz, P. The adaptive brain: Aging and neurocognitive scaffolding. Annu. Rev. Psychol. 2009, 60, 173. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.J.D.; Powell, A.L.; Holmes, J.D.; Vann, S.D.; Aggleton, J.P. What does spatial alternation tell us about retrosplenial cortex function? Front. Behav. Neurosci. 2015, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vann, S.D.; Aggleton, J.P.; Maguire, E.A. What does the retrosplenial cortex do? Nat. Rev. Neurosci. 2009, 10, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Dillen, K.N.H.; Jacobs, H.I.L.; Kukolja, J.; von Reutern, B.; Richter, N.; Onur, Ö.A.; Dronse, J.; Langen, K.J.; Fink, G.R. Aberrant functional connectivity differentiates retrosplenial cortex from posterior cingulate cortex in prodromal Alzheimer’s Disease. Neurobiol. Aging 2016, 44, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.D.; Woldorff, M.G.; Mangun, G.R. Control networks and hemispheric asymmetries in parietal cortex during attentional orienting in different spatial reference frames. Neuroimage 2005, 25, 668–683. [Google Scholar] [CrossRef] [PubMed]
- Pouliot, S.; Gagnon, S. Is egocentric space automatically encoded? Acta Psychol. 2005, 118, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Lithfous, S.; Dufour, A.; Blanc, F.; Despres, O. Allocentric but not egocentric orientation is impaired during normal aging: An erp study. Neuropsychology 2014, 28, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Parkin, A.J.; Walter, B.M.; Hunkin, N.M. Relationships between normal aging, frontal lobe function, and memory for temporal and spatial information. Neuropsychology 1995, 9, 304. [Google Scholar] [CrossRef]
- Parsons, T.D.; Carlew, A.R.; Magtoto, J.; Stonecipher, K. The potential of function-led virtual environments for ecologically valid measures of executive function in experimental and clinical neuropsychology. Neuropsychol. Rehabil. 2017, 27, 777–807. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.D.; Gaggioli, A.; Riva, G. Virtual reality for research in social neuroscience. Brain Sci. 2017, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.; Gamito, P.; Rosa, B.; Bértolo, D.; Ribeiro, J.; Sousa, T.; Morais, D.; Ferreira, F.; Lopes, P. Ecologically-Oriented Approach for Cognitive Assessment in the Elderly. In Proceedings of the 4th Workshop on ICTs for Improving Patients Rehabilitation Research Techniques, Lisbon, Portugal, 13–14 October 2016; ACM: New York, NY, USA, 2017; pp. 32–35. [Google Scholar]
- García-Betances, R.I.; Arredondo Waldmeyer, M.T.; Fico, G.; Cabrera-Umpiérrez, M.F. A succinct overview of virtual reality technology use in Alzheimer’s Disease. Front. Aging Neurosci. 2015, 7, 80. [Google Scholar] [PubMed]
- Riva, G.; Baños, R.M.; Botella, C.; Mantovani, F.; Gaggioli, A. Transforming experience: the potential of augmented reality and virtual reality for enhancing personal and clinical change. Front. Psychiatry Front. 2016, 7, 164. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.J.; Francis, H.M.; Oaten, M.J.; Schilt, R. Hippocampal dependent neuropsychological tests and their relationship to measures of cardiac and self-report interoception. Brain Cognit. 2018, 123, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Serino, S.; Di Lernia, D.; Pavone, E.F.; Dakanalis, A. Embodied medicine: Mens sana in corpore virtuale sano. Front. Hum. Neurosci. 2017, 11, 120. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Healthy Elderly Group | AD Group | F | p | Partial ηp ² | |
|---|---|---|---|---|---|
| Tower of London (ToL) 1 | 23.13 2 (7.76) | 18.38 2 (8.37) | 10.678 | 0.002 | 0.100 |
| Trail Making Test—TMT-A 1 | 101.64 2 (70.23) | 236.94 2 (182.31) | 17.865 | <0.001 | 0.164 |
| Trail Making Test—TMT-B 1 | 261.01 2 (195.19) | 530.27 2 (272.55) | 11.704 | 0.001 | 0.122 |
| Allocentric Abilities | 89.6% 3 | 71.2% 3 | 5.298 4 | 0.021 | 0.23 5 |
| Syncing Abilities | 35.4% 3 | 19.2% 3 | 3.318 4 | 0.060 | 0.181 5 |
| B | Standard Error | χ2 | p | |
|---|---|---|---|---|
| Tower of London | ||||
| Allocentric Abilities | 21.507 | 109.160 | 3.882 | 0.049 |
| MMSE | 0.942 | 0.2276 | 17.127 | <0.001 |
| Allocentric Abilities * MMSE | −0.788 | 0.4576 | 0.2966 | 0.085 |
| Trail Making Test—TMT-A | ||||
| Allocentric Abilities | 10.079 | 1,852.216 | 0.003 | 0.957 |
| MMSE | −16.716 | 3.919 | 18.240 | <0.001 |
| Allocentric Abilities * MMSE | 1.338 | 77.624 | 0.030 | 0.863 |
| Trail Making Test—TMT-B | ||||
| Allocentric Abilities | 419.823 | 4,405.849 | 0.908 | 0.341 |
| MMSE | −22.863 | 95.138 | 5.775 | 0.016 |
| Allocentric Abilities * MMSE | −11.997 | 184.083 | 0.425 | 0.515 |
| B | Standard Error | χ2 | p | |
|---|---|---|---|---|
| Tower of London | ||||
| Syncing Abilities | 77.392 | 107.488 | 0.518 | 0.47 |
| MMSE | 0.798 | 0.3455 | 5.341 | 0.021 |
| Syncing Abilities * MMSE | −0.246 | 0.4145 | 0.352 | 0.553 |
| Trail MakingTest—TMT-A | ||||
| Syncing Abilities | −378.637 | 1,845.662 | −16.894 | 0.040 |
| MMSE | −27.474 | 60.083 | 20.909 | <0.001 |
| Syncing Abilities * MMSE | 13.354 | 71.118 | 3.526 | 0.060 |
| Trail Making Test—TMT-B | ||||
| Syncing Abilities | −572.617 | 4,549.136 | 1.584 | 0.208 |
| MMSE | −45.045 | 146.802 | 9.415 | 0.002 |
| Syncing Abilities * MMSE | 20.693 | 174.524 | 1.406 | 0.236 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serino, S.; Morganti, F.; Colombo, D.; Pedroli, E.; Cipresso, P.; Riva, G. Disentangling the Contribution of Spatial Reference Frames to Executive Functioning in Healthy and Pathological Aging: An Experimental Study with Virtual Reality. Sensors 2018, 18, 1783. https://doi.org/10.3390/s18061783
Serino S, Morganti F, Colombo D, Pedroli E, Cipresso P, Riva G. Disentangling the Contribution of Spatial Reference Frames to Executive Functioning in Healthy and Pathological Aging: An Experimental Study with Virtual Reality. Sensors. 2018; 18(6):1783. https://doi.org/10.3390/s18061783
Chicago/Turabian StyleSerino, Silvia, Francesca Morganti, Desirée Colombo, Elisa Pedroli, Pietro Cipresso, and Giuseppe Riva. 2018. "Disentangling the Contribution of Spatial Reference Frames to Executive Functioning in Healthy and Pathological Aging: An Experimental Study with Virtual Reality" Sensors 18, no. 6: 1783. https://doi.org/10.3390/s18061783
APA StyleSerino, S., Morganti, F., Colombo, D., Pedroli, E., Cipresso, P., & Riva, G. (2018). Disentangling the Contribution of Spatial Reference Frames to Executive Functioning in Healthy and Pathological Aging: An Experimental Study with Virtual Reality. Sensors, 18(6), 1783. https://doi.org/10.3390/s18061783