1. Introduction
According to the report presented by the World Health Organization (WHO) in 2016, diabetes is a high-prevalence disease, affecting 8.5% of the global population [
1]. Diabetes may either prevent the pancreas from producing insulin or prevent the body cells from responding to insulin properly. In both cases, diabetes leads to an alteration in the patient’s blood glucose (BG) level, which needs to be controlled through a combination of diet, physical activity, and medication [
1,
2].
To optimize therapy for individuals, diabetologists need to monitor their BG values over time. Recently, new devices for continuous glucose monitoring (CGM) have been proposed. This reduces the need to perform BG tests using the traditional glucometer, while providing deeper insight on the patient’s BG trends by monitoring the BG value around the clock [
3]. Intuitively, deeper understanding of the patient’s glycemic profile results in a better ability to maintain the BG value in a target range, thus reducing the number or duration of the episodes of hypoglycemia and hyperglycemia experienced by the patient [
4,
5]. Several wearable devices for CGM are available on the market. Usually, such devices exploit a subcutaneous sensor, which detects BG concentration in the interstitial fluid. While CGM devices return the BG value continuously, other devices apply flash glucose monitoring (FGM), which means they require a scanner to periodically collect the BG values from the sensor. Generally, FGM and CGM systems are complemented with proprietary software, which allows visualizing reports over a pre-defined time interval (e.g., latest 2 weeks), such as the daily glycemic profiles and the ambulatory glucose profile (AGP), an internationally recognized visual representation that combines BG data from multiple days and collates them into a single 24-h period [
6].
It is well known that the BG profile over the day is influenced by multiple factors related to the patient’s daily routine, which alter the glucose metabolism and/or the body response to insulin [
6]. Besides the consumption of meals and the therapy intake, such factors include, for example, physical activity and sleep, in terms of both quality and quantity. In fact, low sleep quality may cause hyperglycemic effects up to several hours after the awakening. Physical activity may lead either to hypoglycemic episodes or to hyperglycemic episodes up to 48 h afterwards [
7]. Since their effects on the BG value do not run out immediately, it is fundamental to keep track of the patient’s sleep and activity over time. Nowadays, this is possible thanks to the use of activity trackers that can be comfortably worn by the patient around the clock. Several brands of activity trackers are available, including Fitbit [
8], Polar [
9], and Garmin [
10]. Regardless of the brand, activity trackers usually record multiple parameters related to the user’s sleep, including start time, end time, and number of night-time arousals. They also distinguish deep sleep from light sleep, although the accuracy of this classification is not high [
11]. With regard to physical activity, they record start time, end time, and intensity for each detected workout (i.e., activity lasting more than a threshold duration, which may be brand-specific). They also provide a summary of the overall daily activity, including the total number of steps. In addition, most trackers also monitor the subject’s heart rate (HR) continuously. Collecting data from diabetic patients wearing both a BG monitoring device and an activity tracker may help to better understand the relationship between BG values and HR, which is a debated research topic in the literature [
12,
13,
14].
The importance of providing innovative approaches, able to take into account the most recent technological solutions and to promote integrated care by involving both patients and care providers, has been recently identified as one of the main points of action by the European Diabetes Forum [
15]. The need to complement the glycemic profile with information on the subject’s lifestyle has been recently discussed by Rodríguez-Rodríguez et al. [
7]. In their work, the authors monitored a diabetic patient (male, 25 years old) for 2 weeks, using both the Abbott FreeStyle Libre system and a Fitbit activity tracker, which collected information on the subject’s sleep and physical activity. The subject was also asked to report meals and insulin intake. The graph integrating all the collected data helped interpreting BG values in relation to the patient’s lifestyle factors, which are known to influence the subject’s status.
Since the interest in integrating the BG profile with lifestyle information has been increasing, smart applications to facilitate data integration are needed. For example, the web-applications presented in [
16,
17] allow the patients to autonomously report performed physical activity, insulin intake, and details on the consumption of carbohydrates. The collected data can be accessed both by the patient and by his/her diabetologist, who can remotely monitor the progress of the patient in diabetes management. Using the web-application developed by Hidalgo et al. [
16], the patient can also share with the clinician the results of a set of clinical tests (e.g., eye examination) that are usually carried out to identify the onset of possible complications due to diabetes. However, rather than continuous BG monitoring, these systems consider data collected using a glucometer and a manual data entry is required for the other parameters. Such manual daily data collection can fatigue the patients, who, in the long run, might stop providing this data [
18,
19]. Thus, since the use of wearable sensors has intensified in recent years, the most recent applications designed for chronic patients aim to automatically collect as much data as possible from such devices. For example, several commercial platforms focus on supporting patients affected by Type 2 diabetes [
20,
21,
22,
23,
24] by tracking both BG measurements collected using glucometers and activity data collected by trackers. Such applications usually provide dashboards for the integrated visualization of the collected information, and sometimes allow the patient to share the data with the physician. Recent applications intended for Type 1 diabetes collect and visualize CGM or FGM monitoring data [
3]. Such applications usually provide daily reports, including the number and the duration of hypoglycemic and hyperglycemic episodes, possibly filtered by time of occurrence (e.g., nighttime or daytime). They also provide other summaries, such as AGPs. However, few applications integrate BG monitoring (either CGM or FGM) with activity and sleep tracking. One of the first solutions proposed in this area was Nightscout [
25], an open source project developed by volunteers in 2014 to help the patient, or his/her family, set up a custom system for collecting and visualizing both BG monitoring data and activity tracking. However, this solution was not suitable to all patients, since it required the ability to build and maintain such a system, which includes a website and a database. Other solutions [
26,
27] include commercial (integrated) systems, which include a sensor for CGM and proprietary software to process the collected data. Such systems gather information on physical activity using proprietary insulin pumps [
27], or commercial activity trackers [
26]. To our knowledge, such systems provide an integrated visualization of data, but do not provide any tool for performing advanced analyses that combine data from both the sources. The same consideration holds for recent applications, such as the M:Diabetes mobile application [
28], which was not developed by the same companies that produce the sensors, and aims to be compatible with multiple brands of sensors, insulin pumps, and wearable devices for activity tracking.
Recently, we have developed AID-GM (Advanced Intelligent Distant—Glucose Monitoring), a web application that allows diabetic patients and their clinicians to share and analyze FGM data [
29,
30]. In this work, we describe the extended version of AID-GM, providing advanced data analyses that combine FGM data with the information collected by Fitbit activity trackers (i.e., HR profile, activity, and sleep tracking). We also evaluated the usability of our application in a real-world pilot study involving 30 pediatric patients receiving care at the Fondazione IRCCS Policlinico San Matteo Hospital in Pavia, Italy.
3. Results
The usability of the system was evaluated in a 6-month pilot study carried out in collaboration with the Pediatric Diabetology outpatient service of the IRCCS Policlinico San Matteo hospital in Pavia, Italy. The study was approved by the Institutional Review Board (IRB) of the hospital. The subjects enrolled in the study were already being followed by the center and were already using the FreeStyle Libre device for monitoring their BG. The patients involved in the study were asked to use the system to periodically upload their BG data and, if they wanted to, for visualizing information related to BG profiles. Some of the patients were wearing a Fitbit tracker, and provided their consent to download their Fitbit data and analyze it together with their BG data. After 2 and 6 months from enrollment, patients were asked to fill in the System Usability Scale (SUS), a well-known 10-item questionnaire that asks users to assess the perceived ease of use of the system and their willingness to continue using it in the future [
41]. For patients aged less than 18 years, the questionnaires were filled in by their parents, whereas patients older than 18 filled in the questionnaires themselves. Patients were then treated following the usual practice. In addition to patients, 3 doctors were also asked to fill-in the SUS questionnaire at the end of the study. Of the 30 patients originally enrolled in the study, 3 dropped out at the beginning of the study, leaving us with a sample of 27 subjects, whose characteristics are shown in
Table 3. As shown by the statistics on the duration, not all the patients were continuously using the monitoring devices.
To further characterize the patients’ population, we used AID-GM to perform an analysis of the BG profiles through pattern detection.
Table 4 provides a snapshot of the total number of BG patterns detected in the dataset using the system. The patterns were computed on all the patients taking part in the study. As already stated, thresholds for defining hypoglycemic and hyperglycemic episodes are patient-specific and are defined by the diabetologists through the system.
Severe Hypoglycemia is defined as an episode of at least one measurement of BG < 50 mg/dL, whereas
Severe Hyperglycemia is defined as an episode of BG > 250 mg/dL.
BG Increasing and
BG Decreasing episodes are defined as a variation of the BG level of at least 15 mg/dL every 15 min, lasting for at least 35 min. The values of the parameters needed to compute the patterns were agreed with the physicians and validated on a sample of the available time series.
Table 4 shows that there are some patterns that happen more frequently than others in our population, and that different patterns have different durations. In particular,
Increasing and
Decreasing BG trends are the most frequent of the considered patterns, but the episodes that last longer are the
Hyperglycemia ones.
The patterns on BG can also be used as indicators of glycemic control in our patients. As an example,
Figure 13 shows the percentage of time spent in Normal BG range,
Hyperglycemia, and Hypoglycemia for 3 representative patients in the study. From this picture it is possible to easily identify a subject who spends the majority of time with high BG values and less than 1% of time in hypoglycemic episodes (Patient 9), a subject who has long periods of normal BG values (Patient 22), and a patient who experiences several hypoglycemic episodes (Patient 1). This type of analysis could allow diabetologists to quickly divide the patients in groups, which can be managed with different interventions or treatment strategies.
To be able to fully exploit the potential of the TA framework, it is interesting to analyze data for the six patients who were wearing both the FGM and the Fitbit devices simultaneously (Patients 1, 2, 5, 6, and 10). In this case, it is possible to extract several additional patterns, involving multiple variables (BG, HR, and tracked sleep).
As an example of a pattern involving BG and sleep, it is possible to compare the patients in terms of episodes of nighttime hypoglycemia. This is very important, especially for children, since it is crucial to quickly identify who are experiencing this pattern more frequently than others.
Table 5 presents the number of nights with at least one hypoglycemic episode and the total number of nights, for the six patients. Thanks to the advanced analysis functionalities offered by AID-GM, it was easy for the physician to identify the patients who were more prone to a specific type of episode. For example, comparing Patient 5 to Patient 10, it is possible to see that the first one has used the Fitbit for less nights than the second (56 vs. 165), but the proportion of nights with at least one hypoglycemic episode is higher.
Another interesting analysis, which makes it possible to understand the importance and usefulness of integrating different devices, is the comparison between the patterns extracted by the system when using the
profile tag or the
Fitbit tag.
Table 6 shows this comparison for the six patients wearing a Fitbit tracker. The Table reveals that, for patients with irregular sleep habits, such as Patient 1, the difference between the number of hypoglycemic episodes can be significant. For critical episodes, such as those of low BG levels during sleep, a proper monitoring is of crucial importance. Moreover, excluding Patient 1, for the other patients the algorithm is not able to detect Dawn Effect without the sleep information detected by Fitbit.
To evaluate the system use, we analyzed the log files of AID-GM. These files include information about the type of action performed by the user, together with the date and the time of execution. The available types of actions are Login, Logout, Data visualization, Modify, Upload BG data, and Find pattern.
Figure 14 shows the frequency of each action, distinguishing patients and physicians as user types. As shown by the bar chart, besides the
Login, the most frequent action performed by both users is the
Data visualization action. This action refers to the several types of visualization available in AID-GM, which include the visualization of BG profiles and summaries, and the visualization of patients’ demographic and clinical information. As regards
Find pattern, each occurrence of this type of action may concern the search for single or multiple patterns over a single patient or a group of patients.
Figure 15 illustrates the detailed distribution of the available visualization actions, indicating that patients are mostly interested in checking their daily BG trends. For doctors, we registered several visualizations of the patients’ information (
Patient info), and visualizations of daily BG trends.
In addition to the overall number of actions, we also considered the weekly trend, computed as the total number of actions for each week of enrollment. This analysis, reported in
Table 7, showed that the average number of actions in the first week was higher than the average number of actions in all the following weeks, both for patients and for physicians. Doctors use the system more during weekdays and in the morning, whereas patients have a more uniform distribution of usage throughout the week and during the day, with an almost equal number of actions in the morning, afternoon, and in the evening.
Table 8 shows the average session and training durations. The duration of sessions was computed as the time interval between a login and a logout when the latter was available, and as the time interval between a login and the last action before the next login, when logout was not available. In fact, when the user does not use the application for more than 30 consecutive minutes, the work session expires automatically, and no logout activity is recorded in the AID-GM system log. Furthermore, since the first access to the system is performed by the patient together with the physician, who trains the new user by illustrating the functionalities of the system, we finally evaluated the duration of the first session for each patient to have an estimate of the training time.
As anticipated, the system usability was assessed using the SUS questionnaire, which was delivered both to physicians and patients. For patients, we carried out an assessment at 2 months from the beginning of the study and one at the end of the study. The average SUS score at 2 months was 82.6, whereas at 6 months, we registered a slight decrease in the average score, which was 76.4. Even though both scores are considered above average with respect to the threshold of 68 [
41], we investigated the obtained results to better explain the reasons for this decrease. First of all, from the analysis of the system logs, we observed that, even though all the patients filled in the questionnaire at the end of the study, 8 of them never used the system after two months. Considering only the patients who performed at least one access after two months of usage, the average SUS score at 6 months was 81.3. For 11 patients belonging to this group, the SUS score increased or remained stable, whereas for 8 patients we registered a decrease in the score. Analyzing the individual questions, the one that we found most critical was the following: “I found the various functions in this system were well integrated”. For this question, 7 patients gave a lower score after 6 months than at 2 months. Perhaps this question was not entirely understood by the patients, because of its technical formulation. Three physicians completed the questionnaire at the end of our study. In this case, we had the maximum SUS scores for all three (100). The motivation for such high scores could partially be due to the fact that 2 out of 3 users also participated in the development of the system. The third user instead started to use the system at the beginning of the study, without any previous knowledge.
4. Discussion
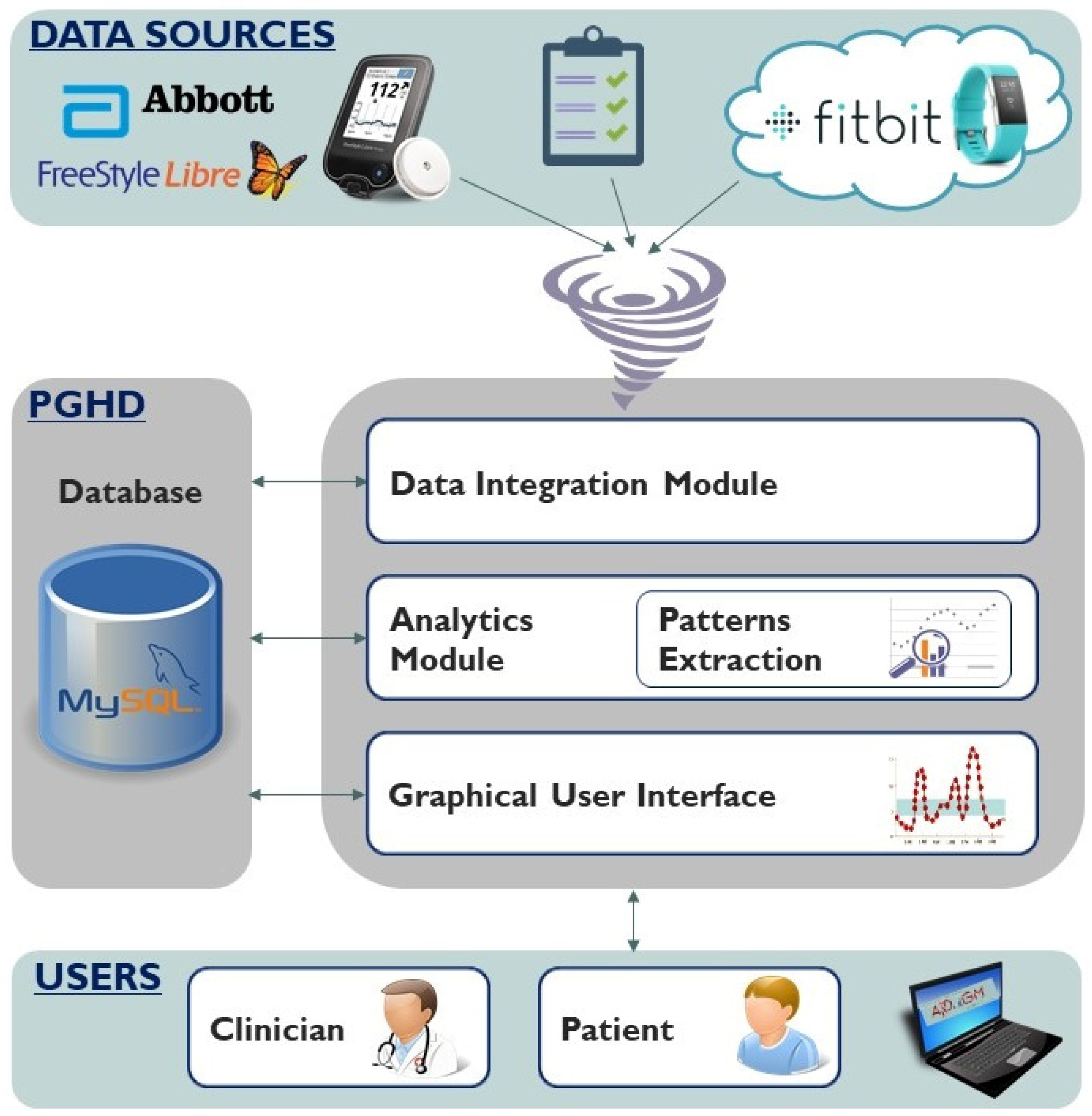
In this paper, we presented AID-GM, a web application for managing patients with diabetes that enables the integration of BG and activity data, provides advanced temporal data analysis functionalities, and encourages communication between patients and their care providers.
Thanks to the Data Integration Module, AID-GM is able to jointly analyze data coming from different sources. This offers several advantages and novelties. First, Fitbit data are used to complement BG measurements providing information about the actual lifestyle of a patient in terms of sleep and physical activity. As shown in
Figure 5 and
Figure 6, the availability of such information also allows the identification of irregularities in the habits, which could be an important factor not usually included in applications for monitoring diabetic patients, for interpreting the metabolic response. In addition, the availability of HR data offers the possibility to perform multivariate analysis to investigate the relation between the reaction of HR to variations in BG levels. To our knowledge, AID-GM is the first application that uses Fitbit data to contextualize BG data and carry out advanced multivariate temporal analysis. To fully appreciate the novelty of the AID-GM application, it should be compared with the other tools available for collecting and analyzing CGM or FGM data, rather than tools that consider data collected using glucometers. As anticipated in the introduction, few applications are available for analyzing CGM or FGM data, and fewer applications integrate it with information on the subject’s sleep and activities collected automatically from wearable devices. Among these applications, some solutions [
25] are not ready to use, while others [
27] are not applicable to all patients, since they gather activity data from proprietary insulin pumps. We believe that collecting data from widely used activity trackers, instead of specific insulin pumps, may make the solution accessible to a higher number of patients. Several efforts are converging towards this goal. For example, we are aware that Fitbit and Medtronic reached an agreement, that resulted in a mobile application for visualizing both Fitbit data and BG data collected by a professional device for CGM monitoring, iPro™2 [
42,
43]. However, the iPro™2 device is only intended for diagnostic purposes, and not for long-term remote monitoring. We are aware of another application that is aiming to integrate FGM data with Fitbit data [
28]. However, this feature is not yet listed among the functionalities available in the current version of the system. To the best of our knowledge, there are no available long-term solutions that offer multiple data views combining both BG and activity data, and that allow both the patient and the clinician to perform multivariate analysis through pattern detection. Thus, we believe that the integrated view offered by AID-GM opens a new perspective on the exploitation of PGHD, which can be used to perform, in a realistic day-by-day setting, analyses that have traditionally been limited to clinical studies. In particular, for adolescents and for parents of children, AID-GM can guide clinical decisions regarding therapy and could represent an interactive system to learn diabetes self-monitoring potentially enhancing patient care, especially immediately after the disease onset. Moreover, the automatic collection of BG and lifestyle data ensures an objective picture of the real patient’s behavior and metabolic response, preventing from errors that can occur when manually reporting the daily diary both in paper and electronic form.
AID-GM includes an Analytics Module designed to carry out advanced data analytics through Temporal Abstractions. Thanks to this technique, it is possible to formalize the qualitative patterns that clinicians frequently already have in mind, and automatically extract the behaviors of interest from the available data. The patterns that can be extracted range from basic and univariate to complex and multivariate, like the Dawn Effect. Despite its clinical relevance, the Dawn Effect is difficult to manually detect in a large amount of data without accurate information on the sleep and wake up time. Thanks to AID-GM, it is possible to formally define the pattern, and automatically extract it from the available data.
In addition to the flexibility offered by JTSA for patterns definition, another convenient feature of AID-GM is related to the temporal filtering functionalities available for data exploration and analysis. In fact, differently from other available tools that provide a view on data over fixed time ranges, the patterns can be dynamically extracted on user defined time-windows or on specific days of the week, which can be selected over the complete follow-up of the patient. Moreover, for each detected pattern, it is possible to inspect the raw data it was generated from (
Figure 10), thus offering complete control over the obtained results. These features enable the users to dynamically perform their analyses, potentially exploiting the tool to discuss the progression of the disease together during encounters or comparing the metabolic control in different periods and day or week slices (working days/weekend, sleep, routine, workout).
Finally, differently from other tools, AID-GM enables the extraction of temporal patterns over a group of patients. This can be useful in two ways. First of all, considering a single pattern, the tool can be used to highlight those patients who experience it more frequently. Second, considering multiple patterns, this feature allows the detection of the groups that need closer attention. In this paper, we have shown several examples of how the analysis results can be used to identify groups of critical patients. In the future, a careful analysis of the occurrence of the patterns over a larger cohort of patients could be used to propose some pattern-based indicators to quickly characterize patients based on their metabolic control.
As shown by the results of the SUS questionnaires, the AID-GM system was considered to be user-friendly both by patients and physicians during the real-world pilot study. This result is particularly positive, considering that the tool introduces a change in the workflow related to the FreeStyle Libre data management for both user types. Before the introduction of the system, patients used to download their BG summary report from the FreeStyle system only before periodic face-to-face encounters, in order to discuss their BG profile with the diabetologist. During the visit, the diabetologist would consider those reports in order to plan future interventions and treatment. Even though the FreeStyle software offers the possibility of downloading the time series of the collected BG measures from the patient’s sensor, this was rarely performed during encounters because of the lack of tools for data analysis. During the pilot study, the possibility of remotely sharing BG data with the clinician motivated the patients to download their data frequently, and to upload it into the AID-GM system on a regular basis. The obtained SUS scores and the analysis of the actions performed by the users point out that patients believe it is worth investing time in uploading data to the system to facilitate remote monitoring of their health condition, and possibly to receive better care. The advantage derived from the use of the AID-GM system is even more evident when considering health care personnel, who are able to gain deeper insights into how the patient’s condition has evolved between visits and, potentially, during the entire follow-up of the patient. While the data stored within the FreeStyle Libre device include only the most recent three months, the AID-GM system maintains the complete history of BG data uploaded by the patients, of the Fitbit data, and any other information that was provided through the FreeStyle system’s BG reader, like insulin intake and meals. This allows the collection of long histories, which may be used in the future to train and personalize data-driven systems for supporting decision making in the context of Type 1 diabetes.
The work presented in this paper describes ongoing research, which still has some limitations that will be addressed in future work. First of all, AID-GM currently works on a set of temporal patterns that is predefined on the basis of clinical knowledge. Even though this set might be arbitrarily and easily extended, the inclusion of a new pattern would need to be hypothesis-driven. Using only this approach prevents the system from discovering potentially unknown behaviors. Given the peculiarities of the data being considered, which have only recently started to be collected and jointly analyzed, the possibility of mining unknown multivariate patterns is a desirable feature. For example, it is widely acknowledged that lifestyle habits have an impact on metabolism, but evidence on how this reflects subjective parameters such as HR, BG, and sleep is still lacking. Considering our previous work on temporal association rules mining [
39], we are planning to include a module with this functionality in the AID-GM system.
Currently, the Data Integration Module retrieves data from the sensors by using the Application Programming Interfaces (APIs) made available by Fitbit, and dedicated readers specifically designed for storing the data in the AID-GM DB. Even though this custom solution fits well with the system deployed for the pilot study, we are aware of the importance of devices interoperability, especially in remote patient monitoring scenarios. Such importance has been acknowledged by several international projects, such as the open mHealth to FHIR project promoted by HL7 [
44], or the Remote Patient Monitoring supplement to the Technical Framework developed by the IHE Patient Care Coordination domain [
45]. Taking into account these initiatives, future work will be devoted to the development of a standardization component within the Data Integration Module, responsible for making the exchanged data available in a standardized format to promote interoperability among devices and other systems.
An additional aspect to be considered is that, in order to have a complete picture of a patient’s condition, it is important to also consider those events, usually reported in paper diaries, which cannot be automatically monitored. Up until now, AID-GM has supported the inclusion of some events (meals, insulin intake, health related issues) that could be recorded manually by the patient using the FreeStyle Libre reader. Our experience, though, is that patients do not frequently enter data through the reader, probably due to the time it takes to access the functionality and store the information. To overcome this limitation and motivate the patients to provide the necessary information, we are working on a mobile app where the patient could record a voice message reporting any relevant event. The system will then automatically process and store the information, integrating it with the rest of the data available for that subject.
Finally, in this study we focused on the assessment of the system from a usability perspective, without analyzing the impact of the introduction of the system from a clinical viewpoint. To this end, a larger study, possibly including both children and adult patients, should be planned. Depending on the study duration, it will be possible to evaluate outcomes such as the time in range, the time in target [
46,
47,
48], or the variations of glycated hemoglobin.

 ,
, 















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









