Automatic and Real-Time Computation of the 30-Seconds Chair-Stand Test without Professional Supervision for Community-Dwelling Older Adults

 ,
,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Supervised Validation of the Sensor
2.1.1. Participants
- A subject COULD ENTER the study if ALL the following INCLUSION CRITERIA applied:
- ◦
- The subject is willing and able to give written informed consent for participation in the study.
- ◦
- The subject is 70 years old or older.
- ◦
- The subject is able to perform the 30-s CST in a safe way.
- ◦
- The subject has not been diagnosed with cognitive impairment.
- A subject COULD NOT ENTER the study if ANY of the following EXCLUSION CRITERIA applied:
- ◦
- Subjects suffering from any major disability.
- ◦
- Subjects suffering from cognitive impairment.
2.1.2. Apparatus
2.1.2.1. The Wearable Sensor Device
- An accelerometer (a SparkFun 9DoF Sensor Stick board with an LSM9DS1 IMU chip). This SparkFun board comes with a nine degrees of freedom IMU (i.e., it comprises a triaxial accelerometer, a triaxial gyroscope, and a triaxial magnetometer). However, we did not use the gyroscope and the magnetometer because, as explained in Section 2.1.2.2, acceleration readings are enough to compute an estimation of the thigh angle.
- A control and processing unit (an Arduino Nano board with an ATmega328P microcontroller). The Arduino board acts as the processing unit in the device thanks to its onboard micro-controller. Our processing algorithm runs on board the Arduino, and is responsible for collecting the accelerometer readings, computing the estimations of the thigh angle over time, and analyzing the resulting signal to automatically detect and count SiSt and StSi transitions in real time, without storing or transmitting the individual samples.
- A communications unit: (HC-06 Bluetooth 2.0 + EDR module). End users (in this case, the researcher conducting the experiment) control the behavior of the sensing device by interacting with a mobile app in an external tablet device. This communication unit enables wireless communication between the two devices via Bluetooth. The researcher can issue calibration and measurements commands to the sensing device, and the latter automatically sends the results to the tablet once a 30 s-CST is over.
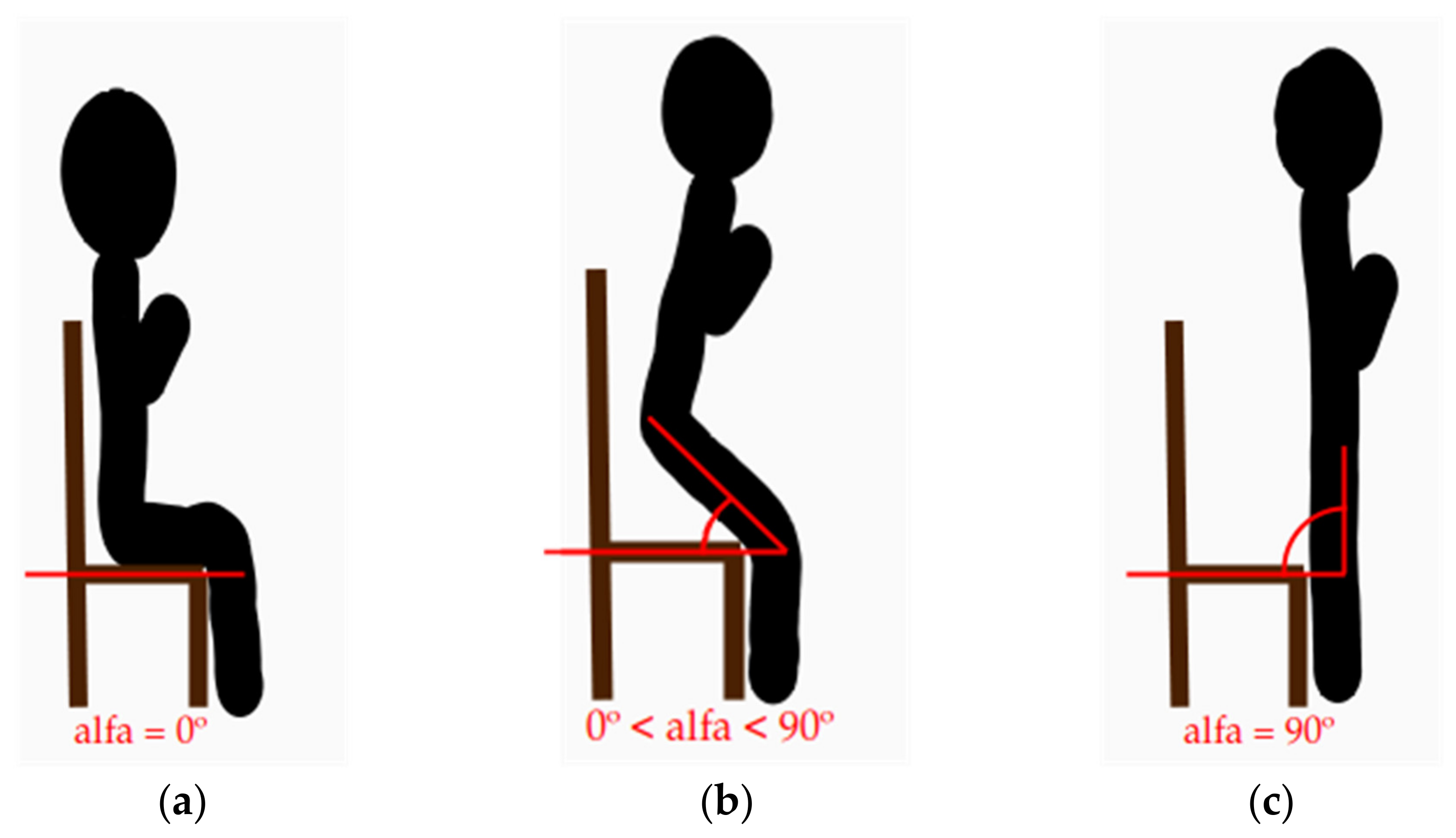
2.1.2.2. The STS Analysis Algorithm
2.1.2.3. The Tablet App
- The researcher puts the sensor into calibration mode by issuing the corresponding command with the app.
- The researcher asks the sensor to compute sitting angle readings for four seconds and send them back to the app by issuing the corresponding command with the app.
- The app computes the mean value of these sitting-angle readings and stores them as the subject’s default sitting-angle.
- The researcher asks the sensor to compute standing-angle readings for four seconds and send them back to the app by issuing the corresponding command with the app.
- The app computes the mean value of these standing-angle readings and stores them as the subject’s default standing-angle.
- The researcher enters an error tolerance value for each default angle.
- The researcher asks the sensor to set the value of the sitting-threshold and the standing-threshold by issuing the corresponding command with the app. The sitting-threshold is computed as the sum of the subject’s default sitting-angle and the error tolerance value for the sitting position. On the other hand, the standing-threshold is computed as the subtraction of the error tolerance value for the standing position from the subject’s default standing-angle.
- The researcher puts the sensor into measurement mode by issuing the corresponding command with the app.
- The researcher asks the sensor to start the 30-s CST measurement sequence by issuing the corresponding command with the app.
- The application waits idle for the results of the 30-s CST.
- The application shows the results of the 30-s CST on screen.
2.1.3. Procedure
2.1.4. Analysis
2.2. Unsupervised Validation of the Home Care System
2.2.1. Participants
- A subject COULD ENTER the study if ALL the following INCLUSION CRITERIA applied:
- ◦
- The subject is willing and able to give written informed consent for participation in the study.
- ◦
- The subject is 64 years old or older.
- ◦
- The subject is able to perform the 30-s CST in a safe way.
- ◦
- The subject has not been diagnosed with cognitive impairment.
- A subject COULD NOT ENTER the study if ANY of the following EXCLUSION CRITERIA applied:
- ◦
- Subjects suffering from any major disability.
- ◦
- Subjects suffering from cognitive impairment.
2.2.2. Apparatus
2.2.2.1. The Sensor
2.2.2.2. The Home Care Application
2.2.2.3. The Acceptability and General Impressions Questionnaires
2.2.3. Procedure
2.2.4. Analysis
3. Results
3.1. Supervised Validation of the Sensor
3.2. Unsupervised Validation of the Home Care System
3.2.1. The Acceptability Questionnaire
3.2.1.1. Question #1: What Difficulties Did You Find While Using the Sensor?
3.2.1.2. Question #2: What is Your Opinion on the Sensor?
3.2.1.3. Question #3: How Did You Feel While Using the Sensor?
3.2.1.4. Question #4: What Difficulties Did You Find While Using the Tablet?
3.2.1.5. Question #5: What is Your Opinion on the Tablet?
3.2.1.6. Question #6: How Did You Feel While Using the Tablet?
3.2.2. The General Impressions Questionnaire
3.2.2.1. Question #1: Was the Device Easy to Put on?
3.2.2.2. Question #2: Do You Find the Device Comfortable?
3.2.2.3. Question #3: Do You Think You Would Be Able to Use the Device at Home on Your Own?
3.2.2.4. Question #4: What Activities Did You Find the Most Difficult to Achieve While Using the Tablet?
3.2.2.5. Question #5: Which Features Did You Find the Hardest to Understand in the Tablet?
3.2.2.6. Question #6: What are Your General Impressions on the Tablet?
3.2.2.7. Question #7: Do You Think You Would Be Able to Use the App at Home on Your Own?
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s Chair-Stand Test as a Measure of Lower Body Strength in Community-Residing Older Adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Campbell, A.J.; Buchner, D.M. Unstable disability and the fluctuations of frailty. Age Ageing 1997, 26, 315–318. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Ehogan, D.B.; Macknight, C.; Rockwood, P.K. Conceptualisation and Measurement of Frailty in Elderly People. Drugs Aging 2000, 17, 295–302. [Google Scholar] [CrossRef]
- Walston, J.; Fried, L.P. Frailty and the Older MAN. Med. Clin. N. Am. 1999, 83, 1173–1194. [Google Scholar] [CrossRef]
- Clegg, A.P.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Kojima, G. Frailty as a predictor of disabilities among community-dwelling older people: A systematic review and meta-analysis. Disabil. Rehabil. 2016, 39, 1897–1908. [Google Scholar] [CrossRef]
- Zheng, Y.; Cheung, K.S.L.; Yip, P.S. Are We Living Longer and Healthier? J. Aging Health 2020, 0898264320950067. [Google Scholar] [CrossRef]
- Cesari, M.; Vellas, B.; Hsu, F.-C.; Newman, A.B.; Doss, H.; King, A.C.; Manini, T.M.; Church, T.; Gill, T.M.; Miller, M.E.; et al. A Physical Activity Intervention to Treat the Frailty Syndrome in Older Persons--Results From the LIFE-P Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 70, 216–222. [Google Scholar] [CrossRef]
- Rodríguez-Mañas, L.; Fried, L.P. Frailty in the clinical scenario. Lancet 2015, 385, e7–e9. [Google Scholar] [CrossRef]
- Fairhall, N.; Langron, C.; Sherrington, C.; Lord, S.R.; Kurrle, S.E.; Lockwood, K.A.; Monaghan, N.; Aggar, C.; Gill, L.; Cameron, I.D. Treating frailty-a practical guide. BMC Med. 2011, 9, 83. [Google Scholar] [CrossRef] [Green Version]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of Deficits as a Proxy Measure of Aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty in Relation to the Accumulation of Deficits. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty Defined by Deficit Accumulation and Geriatric Medicine Defined by Frailty. Clin. Geriatr. Med. 2011, 27, 17–26. [Google Scholar] [CrossRef]
- Ko, F. The Clinical Care of Frail, Older Adults. Clin. Geriatr. Med. 2011, 27, 89–100. [Google Scholar] [CrossRef]
- Batista, F.S.; Gomes, G.A.D.O.; Neri, A.L.; Guariento, M.E.; Cintra, F.A.; Sousa, M.D.L.R.D.; D’Elboux, M.J. Relationship between lower-limb muscle strength and frailty among elderly people. Sao Paulo Med. J. 2012, 130, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Song, J.; Lindquist, L.A.; Chang, R.W.; Semanik, P.A.; Ehrlich-Jones, L.S.; Lee, J.; Sohn, M.-W.; Dunlop, D.D. Sedentary Behavior as a Risk Factor for Physical Frailty Independent of Moderate Activity: Results from the Osteoarthritis Initiative. Am. J. Public Heal. 2015, 105, 1439–1445. [Google Scholar] [CrossRef]
- Hall, G.; Laddu, D.R.; Phillips, S.A.; Lavie, C.J.; Arena, R. A tale of two pandemics: How will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Prog. Cardiovasc. Dis. 2020. [Google Scholar] [CrossRef]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez-Ramirez, A.; Izquierdo, M. Kinematic Parameters to Evaluate Functional Performance of Sit-to-Stand and Stand-to-Sit Transitions Using Motion Sensor Devices: A Systematic Review. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 926–936. [Google Scholar] [CrossRef]
- Kerr, K.; White, J.; Barr, D.; Mollan, R. Standardization and definitions of the sit-stand-sit movement cycle. Gait Posture 1994, 2, 182–190. [Google Scholar] [CrossRef]
- Van Lummel, R.C.; Ainsworth, E.; Lindemann, U.; Zijlstra, W.; Chiari, L.; Van Campen, P.; Hausdorff, J.M. Automated approach for quantifying the repeated sit-to-stand using one body fixed sensor in young and older adults. Gait Posture 2013, 38, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Millor, N.; Lecumberri, P.; Gómez, M.; Martínez-Ramírez, A.; Rodríguez-Mañas, L.; García-García, F.J.; Izquierdo, M. Automatic Evaluation of the 30-s Chair Stand Test Using Inertial/Magnetic-Based Technology in an Older Prefrail Population. IEEE J. Biomed. Heal. Inform. 2013, 17, 820–827. [Google Scholar] [CrossRef]
- Millor, N.; Lecumberri, P.; Gómez, M.; Martínez-Ramírez, A.; Izquierdo, M. An evaluation of the 30-s chair stand test in older adults: Frailty detection based on kinematic parameters from a single inertial unit. J. Neuroeng. Rehabil. 2013, 10, 86. [Google Scholar] [CrossRef] [Green Version]
- Van Lummel, R.C.; Ainsworth, E.; Hausdorff, J.M.; Lindemann, U.; Beek, P.J.; Van Dieën, J.H. Validation of seat-off and seat-on in repeated sit-to-stand movements using a single-body-fixed sensor. Physiol. Meas. 2012, 33, 1855–1867. [Google Scholar] [CrossRef]
- Van Lummel, R.C.; Evers, J.; Niessen, M.; Beek, P.J.; Van Dieën, J.H. Older Adults with Weaker Muscle Strength Stand up from a Sitting Position with More Dynamic Trunk Use. Sensors 2018, 18, 1235. [Google Scholar] [CrossRef] [Green Version]
- Van Roie, E.; Van Driessche, S.; Huijben, B.; Baggen, R.; Van Lummel, R.C.; Delecluse, C. A body-fixed-sensor-based analysis of stair ascent and sit-to-stand to detect age-related differences in leg-extensor power. PLoS ONE 2019, 14, e0210653. [Google Scholar] [CrossRef] [Green Version]
- Van Lummel, R.C.; Walgaard, S.; Maier, A.B.; Ainsworth, E.; Beek, P.J.; Van Dieën, J.H. The Instrumented Sit-to-Stand Test (iSTS) Has Greater Clinical Relevance than the Manually Recorded Sit-to-Stand Test in Older Adults. PLoS ONE 2016, 11, e0157968. [Google Scholar] [CrossRef]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez, A.; Martinikorena, J.; Rodríguez-Mañas, L.; García-García, F.J.; Izquierdo, M. Gait Velocity and Chair Sit-Stand-Sit Performance Improves Current Frailty-Status Identification. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2018–2025. [Google Scholar] [CrossRef]
- Regterschot, G.R.H.; Zhang, W.; Baldus, H.; Stevens, M.; Zijlstra, W. Sensor-based monitoring of sit-to-stand performance is indicative of objective and self-reported aspects of functional status in older adults. Gait Posture 2015, 41, 935–940. [Google Scholar] [CrossRef]
- Jovanov, E.; Wright, S.; Ganegoda, H. Development of an Automated 30 Second Chair Stand Test Using Smartwatch Application. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 2474–2477. [Google Scholar]
- Cobo, A.; Villalba-Mora, E.; Hayn, D.; Ferre, X.; Pérez-Rodríguez, R.; Sánchez-Sánchez, A.; Bernabé-Espiga, R.; Sánchez-Sánchez, J.-L.; López-Diez-Picazo, A.; Moral, C.; et al. Portable Ultrasound-Based Device for Detecting Older Adults’ Sit-to-Stand Transitions in Unsupervised 30-Second Chair–Stand Tests. Sensors 2020, 20, 1975. [Google Scholar] [CrossRef] [Green Version]
- Abhayasinghe, N.; Murray, I. Human activity recognition using thigh angle derived from single thigh mounted IMU data. In Proceedings of the 2014 International Conference on Indoor Positioning and Indoor Navigation (IPIN), Busan, Korea, 27–30 October 2014; pp. 111–115. [Google Scholar]
- Steeves, J.A.; Bowles, H.R.; McClain, J.J.; Dodd, K.W.; Brychta, R.J.; Wang, J.; Chen, K.Y. Ability of Thigh-Worn ActiGraph and activPAL Monitors to Classify Posture and Motion. Med. Sci. Sports Exerc. 2015, 47, 952–959. [Google Scholar] [CrossRef]
- Martinez-Hernandez, U.; Dehghani-Sanij, A.A. Probabilistic identification of sit-to-stand and stand-to-sit with a wearable sensor. Pattern Recognit. Lett. 2019, 118, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Pickford, C.G.; Findlow, A.H.; Kerr, A.; Banger, M.; Clarke-Cornwell, A.M.; Hollands, K.L.; Quinn, T.; Granat, M.H. Quantifying sit-to-stand and stand-to-sit transitions in free-living environments using the activPAL thigh-worn activity monitor. Gait Posture 2019, 73, 140–146. [Google Scholar] [CrossRef]
- Gui, P.; Tang, L.; Mukhopadhyay, S. MEMS based IMU for tilting measurement: Comparison of complementary and kalman filter based data fusion. In Proceedings of the 2015 IEEE 10th Conference on Industrial Electronics and Applications (ICIEA), Auckland, New Zealand, 15–17 June 2015; pp. 2004–2009. [Google Scholar]
- Abhayasinghe, N.; Murray, I.; Bidabadi, S.S. Validation of Thigh Angle Estimation Using Inertial Measurement Unit Data against Optical Motion Capture Systems. Sensors 2019, 19, 596. [Google Scholar] [CrossRef] [Green Version]
- Tognetti, A.; Lorussi, F.; Carbonaro, N.; De Rossi, D. Wearable Goniometer and Accelerometer Sensory Fusion for Knee Joint Angle Measurement in Daily Life. Sensors 2015, 15, 28435–28455. [Google Scholar] [CrossRef] [Green Version]
- Rikli, R.E.; Jones, C.J. Functional Fitness Normative Scores for Community-Residing Older Adults, Ages 60–94. J. Aging Phys. Act. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of Criterion-Referenced Clinically Relevant Fitness Standards for Maintaining Physical Independence in Later Years. Gerontologist 2012, 53, 255–267. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| If a Subject Tests Positive to: | He is Diagnosed as: |
|---|---|
| 0 components | Robust. |
| 1 component | Pre-frail. |
| 2 components | |
| 3 components | Frail. |
| 4 components | |
| 5 components |
| Type of Question | Acceptability Questionnaire | General Impressions Questionnaire |
|---|---|---|
| Related to the sensor | 1. What difficulties did you find while using the sensor? | 1. Was the device easy to put on? |
| 2. What is your opinion on the sensor? | 2. Do you find the device comfortable? | |
| 3. How did you feel while using the sensor? | 3. Do you think you would be able to use the device at home on your own? | |
| Related to the application | 4. What difficulties did you find while using the tablet? | 4. Which activities did you find the most difficult to achieve while using the tablet? |
| 5. What is your opinion on the tablet? | 5. Which features did you find the hardest to understand in the tablet? | |
| 6. How did you feel while using the tablet? | 6. What are your general impressions on the tablet? | |
| 7. Do you think you would be able to use the app at home on your own? |
| Participant ID | Gender | Age | Default Sitting-Angle | Default Standing-Angle | 30 s CST Result (Manual Count) | 30 s CST Result (Automatic Count) |
|---|---|---|---|---|---|---|
| 1 | male | 88 | 25° | 55° | 5 | 5 |
| 2 | female | 87 | 25° | 70° | 6 | 6 |
| 3 | male | 81 | 27° | 87° | 13 | 13 |
| 4 | female | 79 | 25.5° | 84° | 8 | 8 |
| 5 | female | 79 | 18.7° | 85° | 8 | 8 |
| 6 | female | 81 | 44° | 81° | 9 | 9 |
| 7 | female | 88 | 19° | 82° | 18 | 18 |
| Manual Count | Automatic Count |
|---|---|
| W = 0.88227, p-value = 0.2367 | W = 0.88227, p-value = 0.2367 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cobo, A.; Villalba-Mora, E.; Pérez-Rodríguez, R.; Ferre, X.; Escalante, W.; Moral, C.; Rodriguez-Mañas, L. Automatic and Real-Time Computation of the 30-Seconds Chair-Stand Test without Professional Supervision for Community-Dwelling Older Adults. Sensors 2020, 20, 5813. https://doi.org/10.3390/s20205813
Cobo A, Villalba-Mora E, Pérez-Rodríguez R, Ferre X, Escalante W, Moral C, Rodriguez-Mañas L. Automatic and Real-Time Computation of the 30-Seconds Chair-Stand Test without Professional Supervision for Community-Dwelling Older Adults. Sensors. 2020; 20(20):5813. https://doi.org/10.3390/s20205813
Chicago/Turabian StyleCobo, Antonio, Elena Villalba-Mora, Rodrigo Pérez-Rodríguez, Xavier Ferre, Walter Escalante, Cristian Moral, and Leocadio Rodriguez-Mañas. 2020. "Automatic and Real-Time Computation of the 30-Seconds Chair-Stand Test without Professional Supervision for Community-Dwelling Older Adults" Sensors 20, no. 20: 5813. https://doi.org/10.3390/s20205813