Fiber Bragg Grating Sensors for Millimetric-Scale Temperature Monitoring of Cardiac Tissue Undergoing Radiofrequency Ablation: A Feasibility Assessment

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Fiber Bragg Grating Sensors: Working Principle and Temperature Calibration
2.1. Fiber Bragg Grating’s Working Principle
2.2. Temperature Calibration of the FBG Sensors
3. Radiofrequency Ablation of Ex Vivo Porcine Myocardium
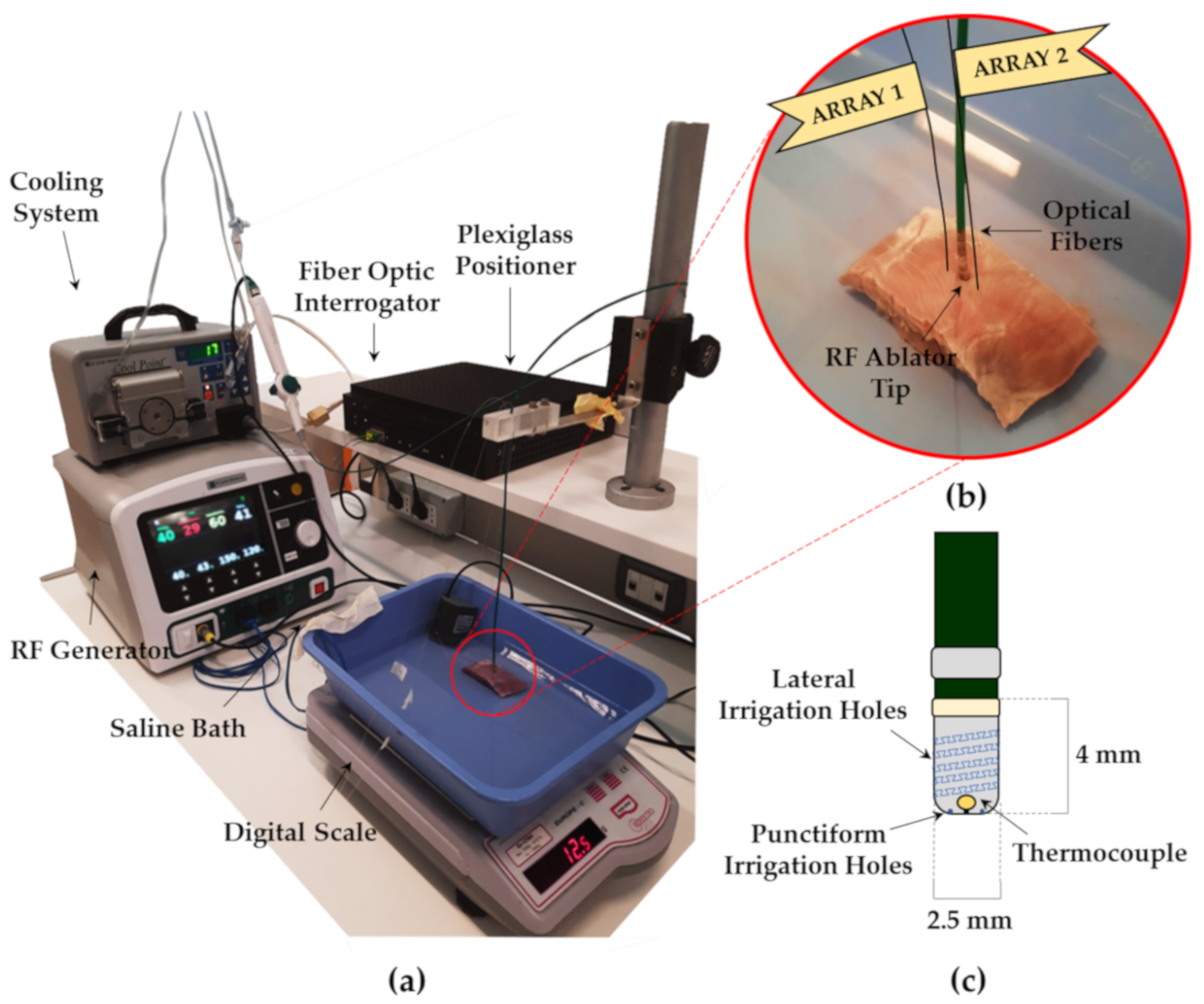
3.1. Experimental Setup
3.2. Sensors and Antenna Positioning into the Tissue during Radiofrequency Ablation
4. Results
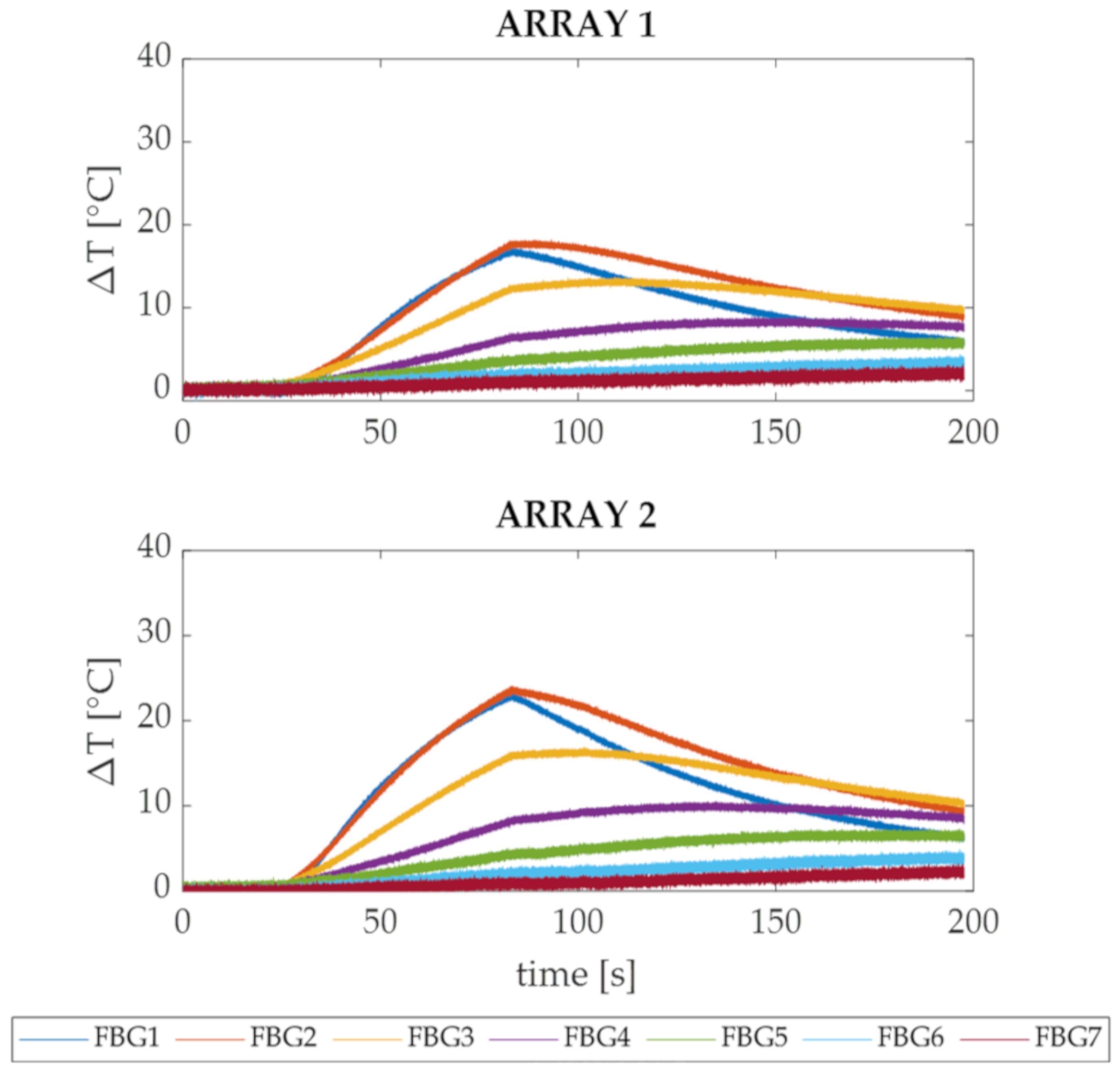
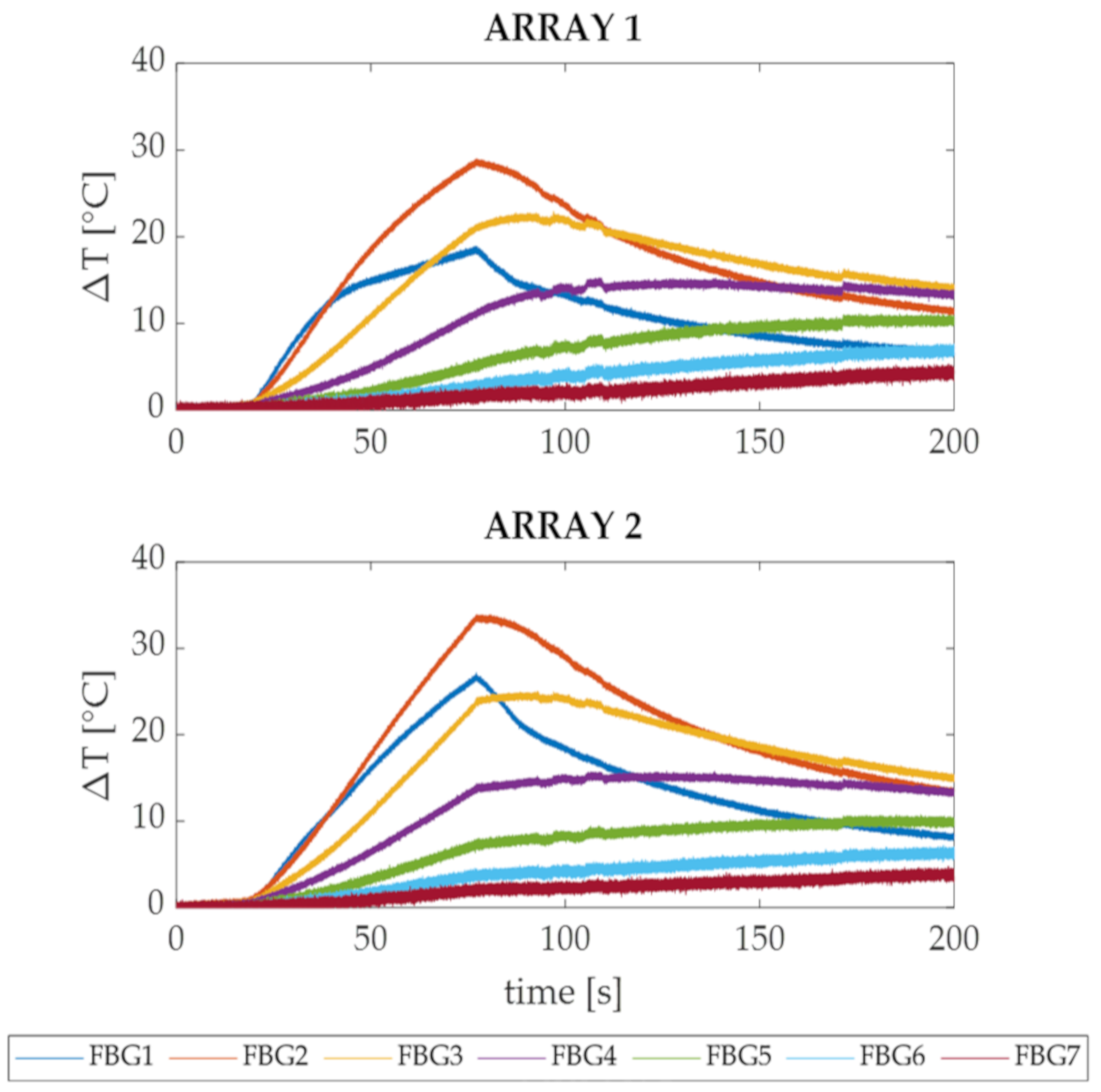
4.1. High-Resolved Thermal Evaluation of Ex Vivo Myocardium Subjected to Radiofrequency Ablation
4.2. Visual Evaluation of Ex Vivo Myocardium Subjected to Radiofrequency Ablation
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Murakoshi, N.; Aonuma, K. Epidemiology of arrhythmias and sudden cardiac death in Asia. Circ. J. 2013, 77, 2419–2431. [Google Scholar] [CrossRef] [Green Version]
- Lesh, M.D.; Van Hare, G.F.; Epstein, L.M.; Fitzpatrick, A.P.; Scheinman, M.M.; Lee, R.J.; Kwasman, M.A.; Grogin, H.R.; Griffin, J.C. Radiofrequency catheter ablation of atrial arrhythmias. Results and mechanisms. Circulation 1994, 89, 1074–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eick, O.J. Temperature controlled radiofrequency ablation. Indian Pacing Electrophysiol. J. 2002, 2, 66. [Google Scholar] [CrossRef] [PubMed]
- Wood, M.; Goldberg, S.; Lau, M.; Goel, A.; Alexander, D.; Han, F.; Feinstein, S. Direct measurement of the lethal isotherm for radiofrequency ablation of myocardial tissue. Circ. Arrhythm. Electrophysiol. 2011, 4, 373–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, J.M.; Sapp, J.L.; Tedrow, U.; Pellegrini, C.P.; Robinson, D.; Epstein, L.M.; Stevenson, W.G. Ablation with an internally irrigated radiofrequency catheter: Learning how to avoid steam pops. Heart Rhythm 2004, 1, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Dinerman, J.L.; Berger, R.D.; Calkins, H. Temperature monitoring during radiofrequency ablation. J. Cardiovasc. Electrophysiol. 1996, 7, 163–173. [Google Scholar] [CrossRef]
- Morady, F. Radio-frequency ablation as treatment for cardiac arrhythmias. N. Engl. J. Med. 1999, 340, 534–544. [Google Scholar] [CrossRef]
- Bunch, T.J.; Asirvatham, S.J.; Friedman, P.A.; Monahan, K.H.; Munger, T.M.; Rea, R.F.; Sinak, L.J.; Packer, D.L. Outcomes after cardiac perforation during radiofrequency ablation of the atrium. J. Cardiovasc. Electrophysiol. 2005, 16, 1172–1179. [Google Scholar] [CrossRef]
- Olson, M.D.; Phreaner, N.; Schuller, J.L.; Nguyen, D.T.; Katz, D.F.; Aleong, R.G.; Tzou, W.S.; Sung, R.; Varosy, P.D.; Sauer, W.H. Effect of catheter movement and contact during application of radiofrequency energy on ablation lesion characteristics. J. Interv. Card. Electrophysiol. 2013, 38, 123–129. [Google Scholar] [CrossRef]
- Haines, D.E. Determinants of lesion size during radiofrequency catheter ablation: The role of electrode-tissue contact pressure and duration of energy delivery. J. Cardiovasc. Electrophysiol. 1991, 2, 509–515. [Google Scholar] [CrossRef]
- Borne, R.T.; Sauer, W.H.; Zipse, M.M.; Zheng, L.; Tzou, W.; Nguyen, D.T. Longer duration versus increasing power during radiofrequency ablation yields different ablation lesion characteristics. JACC Clin. Electrophysiol. 2018, 4, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Langberg, J.J.; Calkins, H.; el-Atassi, R.; Borganelli, M.; Leon, A.; Kalbfleisch, S.J.; Morady, F. Temperature monitoring during radiofrequency catheter ablation of accessory pathways. Circulation 1992, 86, 1469–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calkins, H.; Prystowsky, E.; Carlson, M.; Klein, L.S.; Saul, J.P.; Gillette, P. Temperature monitoring during radiofrequency catheter ablation procedures using closed loop control. Atakr Multicenter Investigators Group. Circulation 1994, 90, 1279–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Haverkamp, W.; Gülker, H.; Rissel, U.; Budde, T.; Richter, K.D.; Borggrefe, M.; Breithardt, G. Radiofrequency coagulation of ventricular myocardium: Improved prediction of lesion size by monitoring catheter tip temperature. Eur. Heart J. 1989, 10, 972–984. [Google Scholar] [CrossRef] [PubMed]
- Anter, E.; Neužil, P.; Rackauskas, G.; Peichl, P.; Aidietis, A.; Kautzner, J.; Nakagawa, H.; Jackman, W.M.; Natale, A.; Reddy, V.Y. A lattice-tip temperature-controlled radiofrequency ablation catheter for wide thermal lesions: First-in-human experience with atrial fibrillation. JACC Clin. Electrophysiol. 2020, 6, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Eick, O.J.; Bierbaum, D. Tissue Temperature-Controlled Radiofrequency Ablation. Pacing Clin. Electrophysiol. 2003, 26, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Toupin, S.; Bour, P.; Lepetit-Coiffé, M.; Ozenne, V.; de Senneville, B.D.; Schneider, R.; Vaussy, A.; Chaumeil, A.; Cochet, H.; Sacher, F.; et al. Feasibility of real-time MR thermal dose mapping for predicting radiofrequency ablation outcome in the myocardium in vivo. J. Cardiovasc. Magn. Reson. 2017, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kolandaivelu, A.; Zviman, M.M.; Castro, V.; Lardo, A.C.; Berger, R.D.; Halperin, H.R. Noninvasive assessment of tissue heating during cardiac radiofrequency ablation using MRI thermography. Circ. Arrhythm. Electrophysiol. 2010, 3, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Varghese, T.; Zagzebski, J.A.; Chen, Q.; Techavipoo, U.; Frank, G.; Johnson, C.; Wright, A.; Lee, F.T., Jr. Ultrasound monitoring of temperature change during radiofrequency ablation: Preliminary in-vivo results. Ultrasound Med. Biol. 2002, 28, 321–329. [Google Scholar] [CrossRef]
- Seip, R.; Ebbini, E.S. Noninvasive estimation of tissue temperature response to heating fields using diagnostic ultrasound. IEEE Trans. Biomed. Eng. 1995, 42, 828–839. [Google Scholar] [CrossRef]
- Arthur, R.M.; Straube, W.L.; Trobaugh, J.W.; Moros, E.G. Non-invasive estimation of hyperthermia temperatures with ultrasound. Int. J. Hyperth. 2005, 21, 589–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fani, F.; Schena, E.; Saccomandi, P.; Silvestri, S. CT-based thermometry: An overview. Int. J. Hyperth. 2014, 30, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Tosi, D.; Schena, E.; Molardi, C.; Korganbayev, S. Fiber optic sensors for sub-centimeter spatially resolved measurements: Review and biomedical applications. Opt. Fiber Technol. 2018, 43, 6–19. [Google Scholar] [CrossRef]
- De Vita, E.; Zaltieri, M.; De Tommasi, F.; Massaroni, C.; Faiella, E.; Zobel, B.B.; Iadicicco, A.; Schena, E.; Grasso, R.F.; Campopiano, S. Multipoint Temperature Monitoring of Microwave Thermal Ablation in Bones through Fiber Bragg Grating Sensor Arrays. Sensors 2020, 20, 3200. [Google Scholar] [CrossRef] [PubMed]
- FiSens FBGs Inscribing Technology. Available online: https://fisens.com/technology/ (accessed on 4 November 2020).
- Rao, Y.-J. Fiber Bragg grating sensors: Principles and applications. Opt. Fiber Sens. Technol. 1998, 2, 355–379. [Google Scholar] [CrossRef]
- Hill, K.O.; Fujii, Y.; Johnson, D.C.; Kawasaki, B.S. Photosensitivity in optical fiber waveguides: Application to reflection filter fabrication. Appl. Phys. Lett. 1978. [Google Scholar] [CrossRef]
- Khaled, A.-R.; Vafai, K. The role of porous media in modeling flow and heat transfer in biological tissues. Int. J. Heat Mass Transf. 2003, 46, 4989–5003. [Google Scholar] [CrossRef]
- Calzolari, V.; De Mattia, L.; Indiani, S.; Crosato, M.; Furlanetto, A.; Licciardello, C.; Squasi, P.A.M.; Olivari, Z. In vitro validation of the lesion size index to predict lesion width and depth after irrigated radiofrequency ablation in a porcine model. JACC Clin. Electrophysiol. 2017, 3, 1126–1135. [Google Scholar] [CrossRef]
- Seo, C.H.; Stephens, D.N.; Cannata, J.; Dentinger, A.; Lin, F.; Park, S.; Wildes, D.; Thomenius, K.E.; Chen, P.; Nguyen, T.; et al. The feasibility of using thermal strain imaging to regulate energy delivery during intracardiac radio-frequency ablation. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 1406–1417. [Google Scholar]
- Schena, E.; Tosi, D.; Saccomandi, P.; Lewis, E.; Kim, T. Fiber optic sensors for temperature monitoring during thermal treatments: An overview. Sensors 2016, 16, 1144. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ST [nm·°C−1] | ||
|---|---|---|
| # FBGs | Array 1 | Array 2 |
| FBG 1 | 0.0098 | 0.010 |
| FBG 2 | 0.0097 | 0.010 |
| FBG 3 | 0.0098 | 0.010 |
| FBG 4 | 0.0098 | 0.0099 |
| FBG 5 | 0.010 | 0.010 |
| FBG 6 | 0.010 | 0.010 |
| FBG 7 | 0.0099 | 0.010 |
| Trial 1 at 50 W | Trial 2 at 60 W | |||
|---|---|---|---|---|
| Array 1 | x [mm] | y [mm] | x [mm] | y [mm] |
| FBG 1 | −6.30 | −2 | −6.50 | 0 |
| FBG 2 | −6.30 | −5 | −6.50 | −3 |
| FBG 3 | −6.30 | −8 | −6.50 | −6 |
| FBG 4 | −6.30 | −11 | −6.50 | −9 |
| FBG 5 | −6.30 | −14 | −6.50 | −12 |
| FBG 6 | −6.30 | −17 | −6.50 | −15 |
| FBG 7 | −6.30 | −20 | −6.50 | −18 |
| Array 2 | x [mm] | y [mm] | x [mm] | y [mm] |
| FBG 1 | 3.30 | −2 | 6.30 | 0 |
| FBG 2 | 3.30 | −5 | 6.30 | −3 |
| FBG 3 | 3.30 | −8 | 6.30 | −6 |
| FBG 4 | 3.30 | −11 | 6.30 | −9 |
| FBG 5 | 3.30 | −14 | 6.30 | −12 |
| FBG 6 | 3.30 | −17 | 6.30 | −15 |
| FBG 7 | 3.30 | −20 | 6.30 | −18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaltieri, M.; Allegretti, G.; Massaroni, C.; Schena, E.; Cauti, F.M. Fiber Bragg Grating Sensors for Millimetric-Scale Temperature Monitoring of Cardiac Tissue Undergoing Radiofrequency Ablation: A Feasibility Assessment. Sensors 2020, 20, 6490. https://doi.org/10.3390/s20226490
Zaltieri M, Allegretti G, Massaroni C, Schena E, Cauti FM. Fiber Bragg Grating Sensors for Millimetric-Scale Temperature Monitoring of Cardiac Tissue Undergoing Radiofrequency Ablation: A Feasibility Assessment. Sensors. 2020; 20(22):6490. https://doi.org/10.3390/s20226490
Chicago/Turabian StyleZaltieri, Martina, Greta Allegretti, Carlo Massaroni, Emiliano Schena, and Filippo Maria Cauti. 2020. "Fiber Bragg Grating Sensors for Millimetric-Scale Temperature Monitoring of Cardiac Tissue Undergoing Radiofrequency Ablation: A Feasibility Assessment" Sensors 20, no. 22: 6490. https://doi.org/10.3390/s20226490