
Commercial Off-the-Shelf Components (COTS) in Realizing Miniature Implantable Wireless Medical Devices: A Review


Institute of Integrated Micro and Nano Systems, School of Engineering, University of Edinburgh, Edinburgh EH9 3FF, UK
*
Author to whom correspondence should be addressed.
Sensors 2022, 22(10), 3635; https://doi.org/10.3390/s22103635
Submission received: 22 March 2022
/
Revised: 25 April 2022
/
Accepted: 30 April 2022
/
Published: 10 May 2022
(This article belongs to the Special Issue Selected Papers from the 8th International Electronic Conference on Sensors and Applications)
Abstract
:Over the past decade, there has been exponential growth in the per capita rate of medical patients around the world, and this is significantly straining the resources of healthcare institutes. Therefore, the reliance on smart commercial off-the-shelf (COTS) implantable wireless medical devices (IWMDs) is increasing among healthcare institutions to provide routine medical services, such as monitoring patients’ physiological signals and the remote delivery of therapeutic drugs. These smart COTS IWMDs reduce the necessity of recurring visits of patients to healthcare institutions and also mitigate physical contact, which can minimize the possibility of any potential spread of contagious diseases. Furthermore, the devices provide patients with the benefit of recuperating in familiar surroundings. As such, low-cost, ubiquitous COTS IWMDs have engendered the proliferation of telemedicine in healthcare to provide routine medical services. In this paper, a review work on COTS IWMDs is presented at a macro level to discuss the history of IWMDs, different networked COTS IWMDs, health and safety regulations of COTS IWMDs and the importance of organized procurement. Furthermore, we discuss the basic building blocks of IWMDs and how COTS components can contribute to build these blocks over widely researched custom-built application-specific integrated circuits.
1. Introduction
Telemedicine paves the way for routine healthcare inspection and facilities the provision of care to patients from remote locations. Wearable and in-body medical devices are increasingly used to provide telemedicine services for routine diagnostic and drug delivery services for elderly, vulnerable and disabled patients. Such devices minimize patients’ commute frequency to healthcare centers and ensure that patients can be monitored either for regular checkup or any post-surgery recovery in their familiar surroundings. Therefore, telemedicine services can prevent healthcare institutions from being overwhelmed and overcrowded in regular conditions or any pandemic situation. The effective functioning of a telemedicine ecosystem depends on four key sectors [1], which are consumers, innovators, investors and regulators. Consumers include patients, physicians and hospitals. Innovators are mainly the tech start-ups, incubators and global corporations. Furthermore, investors are venture capitalists, non-profit bodies or banks. The regulator sector includes organizations, such as the Food and Drug Administration (FDA), the Federal Communication Commission (FCC) and the World Health Organization (WHO). The telemedicine ecosystem has evolved significantly as the demand for remote access to e-health services grows [2]. Additionally, point of care (POC) represents a key part of the improvement of telemedicine and healthcare management. It is crucial to manage a disease, in terms of progression and monitoring evaluation, according to the patient’s profile [3]. Wireless and implantable POC devices can facilitate this by regular monitoring and providing quick acquisition of test results so that the patient can be treated in the right direction at the earliest [4], which can improve telemedicine significantly.
One of the major influences on the advancement of telemedicine is the development cycle of different implantable devices. Compared to wearable medical sensors, implantable devices take longer to develop and reach the customer. Implantable devices are generally classified as tethered (also known as wired) and wireless implants. Implantable wireless medical devices (IWMDs) are a more suitable choice in lieu of wired implants due to the high risk of infections caused by tethered implants [5]. Furthermore, tethered implants are prone to bio-signal artifacts caused by patient movement [6]. A patient with an IWMD is less likely to develop a catheterized infection or cause motion-triggered bio-signal artifacts compared to a tethered implant. All these features have increased the acceptance of IWMDs among patients over the past decade.
In the past two decades, custom-built application-specific integrated circuit (ASIC) remains the primary choice for the development of IWMDs [5,6,7,8,9]. Most of these chips intend to develop RF-integrated circuits (RFIC) for wireless connectivity within miniature implantable medical devices. However, custom designed ASIC-based IWMDs tend to be encumbered with challenges such as time consuming development cycles, repeatability and reliability challenges. Furthermore, high costs associated with software support and hardware prototyping is another major issue associated with custom-built ASIC-based IWMDs. Alternatively, recent advancements in micro- and nano-scale semiconductor technologies have been instrumental in the rapid development of low-cost and miniaturized commercial off-the-shelf (COTS)-enabled IWMDs [10,11]. Driven by Moore’s law [12], the computational performance, efficiency and precision of COTS components have grown exponentially, as their associated manufacturing costs have fallen in proportion. The ubiquity of low-cost COTS components used in developing IWMDs [13] benefits from economies of scale derived from short development cycles, low development costs, high yield from mass manufacturing, robust and replaceable devices and manufacturers’ support from hardware and software development tools.
In this review, Section 2 describes the brief history of wireless implants, how IWMDs contribute to the healthcare network and safety aspects of the IWMDS. Section 3 explains the basic building blocks of COTS-enabled IWMDs and their operation principle. Section 4 compiles recent publications on RF transceivers for COTS-enabled IWMDs and offers a brief suggestion regarding the usage of these devices, followed by conclusions.
2. Macro Purview of COTS-Enabled IWMDs
2.1. History of Wireless Implants
IWMDs date as early as 1948 when Fuller et al. presented an innovative device which performed sample recordings of human carotid pulses and human heart rate during a period of apnea, measured human finger pulse and performed a canine pneumogram [14]. This research led to multiple historical advancements in custom IWMDs, illustrated in Table 1.
With advances in manufacturing processes and integration techniques, the commercialization of low-cost miniaturized COTS-based IWMDs emerged circa 1966. Table 2 illustrates a historical timeline of commercial COTS-enabled IWMDs. Technological advances have engendered an era of smart networked IWMDs.
2.2. Role of IWMDs in Healthcare Networks
The proliferation of COTS-enabled hardware platforms across healthcare networks accelerated the convergence of information technology in the medical industry [25]. Commercial wireless biosensors have emerged significantly in the past decade to fulfil the demand for wireless medical equipment for patient monitoring and personal healthcare [26]. Figure 1 illustrates the contribution of COTS-enabled IWMDs in a tiered healthcare network. Tier-1 comprises wireless body area network (WBAN) nodes. The WBAN nodes represent both wearables and IWMDs, which collect and process bio-signals prior to transferring the biotelemetry data to a secured WBAN gateway. The primary aim of WBAN is to ensure continuous monitoring of the patient’s vital parameters while giving them the freedom of movement, which results in the enhancement of the quality of healthcare [27]. Furthermore, Tier-2 bridges WBAN nodes to medical databases via access points such as Wi-Fi. Finally, Tier-3 represents a medical server infrastructure from which healthcare providers can access patient records. IWMDs play a significant role in the improvement of the overall efficiency of the healthcare network by allowing the data management of patients through a single standard wireless device (e.g., smart phone or a hand-held antenna), as shown in Figure 1 [26].
2.3. Regulatory Guidelines for Medical Devices
The World Health Organization (WHO) provides the global medical device nomenclature (GMDN) online repository for certified implantable medical devices [28]. Furthermore, the Food and Drug Administration (FDA) is responsible for publishing federal guidelines on medical device safety. Additionally, regulatory requirements and policies on operating wireless medical devices are coordinated by the Federal Communications Commission (FCC) [29]. These are the primary regulatory organizations to recognize a medical device to be certified for human use. Due to their maturity and established development cycle, COTS-enabled IWMDs have a significant advantage in acquiring regulatory approvals. It should be noted that substantial resources have also been assigned to the procurement of COTS components. The U.S. Air Force Materiel Command published a COTS procurement document which provides guidelines for the identification, selection, acquisition, logistics support and testing of COTS equipment [30]. Original equipment manufacturers (OEMs), such as Texas Instruments (TI), have product portfolios on advanced and sophisticated COTS components for medical, avionics, defense and space electronics industries, as illustrated in [31].
2.4. Health and Safety
2.4.1. Effects of Electromagnetic (EM) Energy on Human Body
COTS-enabled IWMDs must adhere to guidelines on health and safety with respect to EM energy exposure and absorption [32,33,34,35,36]. Tissue safety regulations for IWMDs is measured with near-field specific absorption rate (SAR) and far-field power density (PD). However, SAR is the most commonly used metric [35] to quantify the tissue safety against any IWMD. Widely accepted IEEE standards for SAR levels are FCC-approved 1.6 W/kg averaged over 1 g of tissue and European Union-approved 2 W/kg averaged over 10 g of tissue [37].
2.4.2. Encapsulation
Robust encapsulation ensures the safe and stable operation of IWMDs inside the human body. Commercially available organic polymers such as polyimide, parylene and polydimethylsiloxane (PDMS) are frequently used to encapsulate implantable devices. In Figure 2, an IWMD intraocular pressure (IOP) monitoring system is presented [38], where the overall system is encapsulated using parylene-on-oil. A COTS ST-Microelectronics LPS25H pressure sensor [39] is used for IOP monitoring.
2.4.3. Failure Due to Multiple Medical Steam Sterilization
Medical steam sterilizers (MSSs) utilize extremely fast cycles of temperature, humidity and pressure to sterilize medical instruments, which represents an exceptionally harsh environment for electronics components [40]. Therefore, it is necessary to study the failure mechanisms of plastic-encapsulated modules such as IWMDs and determine the level of deterioration of encapsulant adhesion over multiple sterilization cycles. This is an important step to confirm the purity and suitability of the long-term usage of implantable medical devices. This work demonstrates a COTS-enabled steam sterilizable plastic-encapsulated wireless sensor module (WSM) used to study the root causes of failures by exposing it to multiple steam sterilization cycles. The application was reliable for 100 cycles at high-rate temperature, pressure and humidity cycles at 134 °C, 3 bar and 100% RH, respectively. Although fractures, encapsulant delamination and electrical failure were some of the stress factors observed on the WSM after 100 cycles, the application has promising attributes. The study in [40] also shows that good reliability can be achieved at 3 mm on HTFR4 Epoxy-glass PCB and FP4460 Epoxy encapsulant. Furthermore, the failure due to temperature cycling is disproportional, and larger components are more exposed to the thermomechanical stress. The humidity storage and humidity cycling produce low levels of electrical failures but higher levels of adhesion loss due to the moisture ingress to the adhesive interface.
3. Essential Building Blocks of COTS-Enabled IWMDs
It is preferable to use low-profile and compact form factor COTS due to the invasive nature of IWMDs to minimize patient discomfort. Generally, the physical dimensions of antennas and energy storage devices, such as rechargeable batteries, dominate the form factor in an IWMD. It is necessary to accurately define the specification of an IWMD’s essential blocks to achieve the optimal form factor without compromising functionality. In this section, essential blocks for a COTS-enabled IWMD are described, as shown in Figure 3. It includes an antenna unit to communicate with the wireless device, a radio frequency (RF) transceiver to process the input/output signal, a power management unit to rectify and regulate the necessary power, a microcontroller as a data acquisition and processing unit, a sensor, and any required sensor or analog front-end to collect necessary bio-signals and memory device to store data (for delayed transmission, offline data download, etc.).
3.1. Essential Blocks Description
3.1.1. Antenna
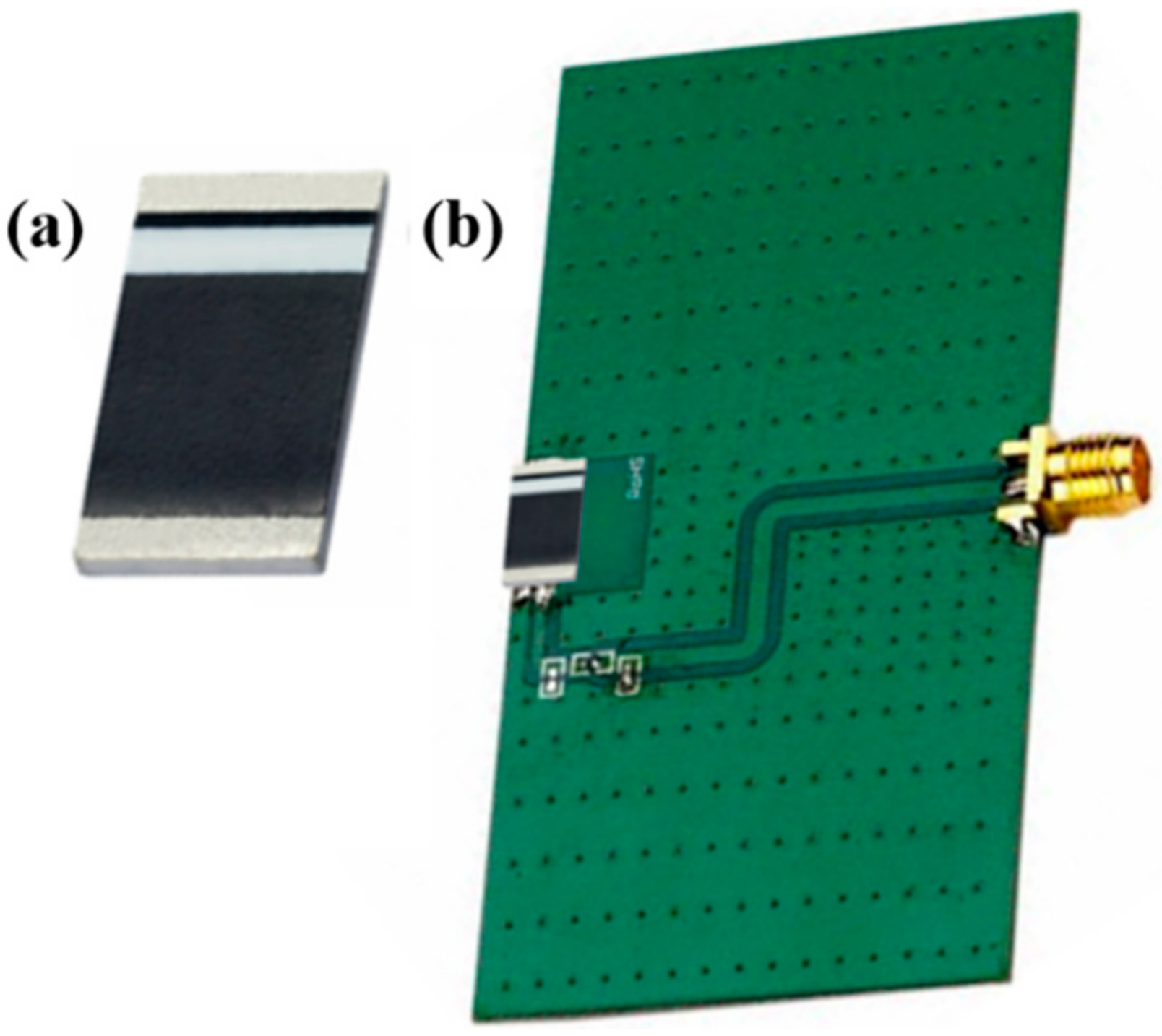
Figure 4 shows the dielectric resonant antenna (DRA) packaged in a chip form, which is increasingly used in the development of miniature COTS components for wireless applications.
Table 3 lists the DRAs compatible with COTS to be integrated with wireless system on chip (SoC) modules. DRA gain and efficiency are influenced by the IWMD’s ground plane dimensions. The evaluation board demonstrated in Figure 4 has a ground plane dimension represented as:
where λ0/4 is the free space quarter wavelength at the frequency of the antenna. Reducing the size of the ground plane to be accommodated in the miniaturized IWMD proportionally degrades the gain and efficiency of the antenna.
3.1.2. RF Transceiver
The high power consumption of RF transceivers is a major concern for battery-operated IWMDs. To conserve battery life, the transceiver section is usually disabled or forced into sleep mode until wireless connectivity is required.
In Table 4, the battery-operated COTS wireless devices mentioned in [47,48] utilize sleep mode functionality to conserve battery life while the NXP COTS [49] ultra-high frequency (UHF) radio frequency identification (RFID) chip remains off until powered by an RFID reader. In Table 4, the Ucode7 is significantly low power compared to ZL70101 and CC2541, as it is a battery-free RFID chip. However, it has lower operating distance compared to other two options. Furthermore, Ucode7 is significantly smaller than ZL70101 and CC2541, with size being an important parameter for IWMDs. It is also necessary to consider the frequency as it plays a key role in maintaining SAR limit.
Figure 5a shows the ZL770101 chip used as a wireless data link module in a WIMAGINE neurological signal capture device. The basic architecture of WIMAGINE includes 64 platinum electrodes of 4.5 mm pitch, two CINESIC32 ASIC and an MSP430 ultra-low-power microcontroller [47]. The electronic environment around the CINESIC32 ASICs is implemented using COTS components.
Figure 5b shows an IWMD electrocorticography (ECoG) system built with COTS CC2541 [22]. The proposed system was tested on the left hemisphere of the brain of a rat, and based on the recording results and signal processing, it is possible to map out the ECoG signals over the measured area to locate the exact epilepsy lesions.
In [54], a multilayer tissue model of the neck and skin is verified by using NXP UCODE 7 COTS chip.
3.1.3. Power Management Unit
The power management unit (PMU) is an important part in an IWMD as it can supply and maintain the necessary power required for optimal operation. A PMU generally consists of a rectifier, regulators, power monitoring circuit and safety unit. The use of a COTS PMU is demonstrated in a smart hip prosthesis comprising multiple energy harvesting systems [56]. In Figure 6, the power management system or PMU consists of a COTS MAXIM IntegratedTM MAX6777 low-power battery monitoring IC to track the output power of micro-power generators or energy harvesters for smart hip prostheses. There is also wireless power transfer (WPT) working as an alternative to the energy harvester. The power switches are implemented with COTS MOSFET transistors. Furthermore, the isolation between two power sources is accomplished by COTS Schottky diodes. Voltage regulation is conducted by an ultra-low-power and low-dropout MAXIM IntegratedTM MAX1963A voltage regulator. COTS Callergy CLG04P040F17 supercapacitors of 40 mF are used as energy reservoirs. In this work, the manufactured PCBs are used to test the system and subject to be miniaturized to fit in the implant.
In [57], an IWMD neuromodulation implant (bionode) is built using COTS components. To supply the required voltage to the bionode, a Texas Instruments (TI) TI7660 boost converter is used for positive output, and an inverted version of the same IC is used for negative output. Furthermore, the proposed system uses two Linear Technology LTC4071 chips as PMUs.
3.1.4. Microcontroller Unit
The microcontroller unit (MCU) is an essential building block for most COTS-enabled IWMDs. Since processing speed and volume of the data are the key factors determining the higher power consumption, MCUs should be carefully chosen to match the requirement of the signal being sensed. Low clock rates (<10 kHz) are often sufficient for processing bio-signals in the range of a few Hz to 500 Hz. It should be noted that apart from the action potentials generated in a neuron, most bio-signals fall within this frequency range. It is also essential to factor in the MCU power consumption in sleep state (or deep sleep), since bio-signals rarely need continuous monitoring. As most physiological signals vary at a very low frequency, it is likely that the IWMDs can often be kept in a sleep state. A COTS-based MCU-enabled telemetry system for brain glucose measurements is presented in [58]. The application uses a COTS Microchip-PIC12F683 MCU [59].
In [23], a wireless ingestible capsule is presented with a telemetry module and a conformal helical antenna, as shown in Figure 7a. The size of the capsule is 30 mm in length and 10 mm in diameter. Figure 7b shows the position of the radio frequency (RF) and thermistor board inside the capsule; the RF board includes a COTS TI ARM Cortex-M3-based wireless microcontroller combined with an ultra-low-power RF transceiver (CC1310).
In [57], a closed-loop neuromodulation implant is presented with only COTS components. This device can record and transmit up to four channels of biopotential data while simultaneously providing biphasic constant current stimulation. In this work, a Nordic semiconductor nRF51822 Bluetooth low-energy microcontroller is used to process the electrode recording data amplified by a front-end amplifier.
3.1.5. Analog Front-End (AFE) and Sensors
The AFE’s primary functions are to power up, detect and process low-frequency signals from external sensors. Comprehensive AFE functions include sensor biasing, multiplexing of sensor array output signals, linearization, amplification, offset control and temperature compensation [60,61,62]. Signals from external sensors are detected, captured and formatted by the AFE. To conserve energy, external sensors are usually deactivated, placed in sleep mode or a hibernation state until an external stimulus from an AFE activates the sensors.
In [63], a wireless implantable ECG monitoring system is proposed and tested inside a mini-pig, as show in Figure 8a. Furthermore, Figure 8b,c shows the configuration of the implantable device and a two-sided view of the PCB, respectively. In this work, a COTS TI INA333 instrumentation amplifier is used to amplify the ECG differential signal.
Ref. [64] presents a wireless electrophysiological recordings and optogenetic stimulation platform where an Instant Technologies COTS RHD2132 is used, which includes a fully integrated electrophysiology amplifier with an on-chip 16-bit analog-to-digital converter (ADC). In [57], the AFE features high differential input impedance, low noise, a high common mode rejection ratio (CMRR) and sufficient gain and bandwidth. It includes two parallel dual-ended AFEs where each AFE consists of passive front-end filtering followed by two gain stages. The first and second stages are built with a COTS TI INA333 instrumentation amplifier and a TI OPA2313 general purpose opamp, respectively.
Additionally, there are different sensors used in IWMDs including ECG, EEG, electromyogram (EMG), bioimpedance analyzers, etc. IWMDs with COTS-based sensors are presented in [57,65,66,67,68]. Figure 9 illustrates an example in the form of a COTS digital barometric pressure sensor used to measure lip pressure.
In [38], a COTS STMicroelectronics digital output pressure sensor LPS25H [39] is used with internal temperature calibration. It is A 2.5 mm × 2.5 mm × 0.8 mm sized low-power sensor which can achieve a pressure resolution of 0.08 mmHg in the lowest power mode. Ref. [23] includes four COTS TDK Group negative temperature coefficient (NTC) thermistors B57540G1 used to monitor the temperature inside gastrointestinal (GI) tracts for capsule endoscopy application.
3.2. Consideration of the Number of COTS Components in IWMDs
Compared to a completely custom-built IWMD, in COTS-enabled IWMDs, the device can be built with single or multiple COTS. A hybrid IWMD with both custom-built chip and COTS components is present in the literature. The SL900A SoC manufactured by Austria Microsystems AG (AMS) [69] is a COTS UHF-RFID sensory tag that can be implemented as a single chip solution for an IWMD. The AMS SL900A chip requires only an external antenna with the required matching elements. The 5 mm × 5 mm × 0.9 mm SL900A is remotely activated by a UHF RFID reader and can be operated as a battery-free IWMD. Figure 10a illustrates the implementation of the SL900A as part of an IWMD inserted in a prosthetic implant. Furthermore, Ref. [70] presented a wireless biofuel cell monitoring system using SL900A tested in vivo in a 12–16-week-old female Sprague–Dawley rat.
A battery-operated subcutaneous implantable device is presented in [73]. The implantable application includes a single Simblee™ Bluetooth® smart module RFD77101, which is a 10 mm × 7 mm × 2.2 mm COTS SoC module with an integrated antenna [74]. The implant harvests solar energy ex vivo through 3 mm of porcine bio-tissue to replenish a 7 mAh rechargeable battery. The rechargeable battery powers a temperature sensor inside the RFD77101. In [24], a single Axzon Magnus S3 passive RFID chip is used with an antenna to wirelessly monitor local deep infections in orthopedic bone plates.
Although IWMDs are commonly assembled with multiple COTS components, in [75], the authors demonstrated a hermetically sealed wireless implantable neural interface realized using multiple COTS devices. The application consists of four key COTS system blocks for recording, stimulating, wireless telemetry and a power supply. Table 5 is a BoM for the implantable neural interface.
In [72], a low data rate transmission method is demonstrated for devices implanted in the body using backscattered long range (LoRa) signals, as shown in Figure 10b. The proof of concept includes analog devices ADG902 and LTC6907 used as the CMOS switch and oscillator, respectively. It also includes a COTS Semtech SX1278 LoRa transceiver.
A hybrid COTS–custom implantable wireless neuroprosthetic is presented in [76]. The application’s neuroprosthetic implantable device is custom designed and utilizes a COTS USRP B210 software defined radio (SDR) for telemetry.
3.3. Considerations of Power Supplies for IWMDs
Selection of the power supply for an IWMD is one of the most challenging decisions to make. The transceiver section in a battery-operated and compact wireless device consumes the largest portion of the application’s current. To maximize battery life, the transceiver block is enabled only when wireless connectivity is required, i.e., duty cycled to minimize current consumption. Power supply requirements for a miniaturized IWMD impact the device’s form factor. This also influences how long the device can operate for and the distance over which a robust wireless link for communication and power transfer can be maintained. To achieve prolonged use, rechargeable energy devices are the most demanding power source choice for battery-operated miniaturized IWMDs. This section describes some important parameters for IWMD power sourcing.
3.3.1. Rechargeable Batteries for IWMD
Contemporary cardiac pacemakers rely on rechargeable batteries to operate continuously over several years. Innovative designs for pacemaker rechargeable batteries using lithium/iodine cells technology were presented in [77]. The authors reported rechargeable batteries with a volumetric energy density of 1.0 Wh/cm3 and an energy density of 270 mWh/g. Novel rechargeable batteries with a capacity of 3 mAh, a volume less than 0.1 cm3 and 3000 recharge cycles have been realized for potential use in IWMD [78]. A rechargeable COTS Li-ion battery QL0003 developed by Quallion LCC [79] was presented in [80] in which the authors demonstrated that the QL0003 could potentially be operated in an IWMD for up to 10 years on a single daily recharge. Figure 11a shows an example of QL0003B rechargeable batteries generally used in pacemakers.
3.3.2. Regular Batteries for IWMD
Regular or non-rechargeable battery-powered IWMDs operate over a wider distance in comparison to their battery-free IWMD complements. A battery’s capacity (mAh) impacts an IWMD’s physical volume (form factor) and operational longevity. Pacemakers are the most notable battery-operated IWMDs. In [82], two commercially available pacemakers by St. Jude Medical are presented, the Micra transcatheter pacing system (Medtronic) and the Nanostim leadless cardiac pacemaker. The Micra and Nanostim, shown in Figure 11b, were meticulously evaluated for ventricular sensing, pacing and rate responsiveness. Both devices exhibited remarkable safety and efficacy results as an alternative to transvenous pacemakers.
3.3.3. Battery-Free or Wirelessly Powered Transfer
Battery-free IWMDs are activated when in proximity to an energy source and thus are less likely to require internal energy storage devices. This type of device is called a passive mode device. The advantages of battery-free IWMDs are reduced form factors and absolutely no current consumption in the absence of external excitation. In contrast, battery-operated IWMDs continue to draw current in the nanoamps to microamps range when the device’s wireless transceiver is inactive. Examples of battery-free IWMDs realized using COTS UHF RFID devices were demonstrated in [83,84,85]. In comparison to battery-operated devices, the operating distance for battery-free wireless charging and telemetry are significantly shorter. Battery-free IWMDs have receive sensitivity of −7 dBm to −10 dBm whereas battery-operated IWMDs’ receive sensitivity ranges from −60 dBm to −90 dBm. UHF RFID battery-free IWMDs can be operated as battery-assisted passives (BAPs) [86,87] with −20 dBm receive sensitivity.
Furthermore, wireless power transfer (WPT) technology has increasingly become the choice for powering battery-free and battery-operated wireless devices [88,89]. In WPT, time-varying EM energy from a source or transmitter propagates across free space and bio-tissue to replenish and/or power up an IWMD. In [90,91,92], the authors demonstrated how WPT sources are optimized to maximize power transfer efficiency (PTE) across free space and multiple layers of bio-tissue (skin, fat, muscle and bones) of varying physical dimensions. The wireless power consortium (WPC) is a collaborative group that develops standards for worldwide compatibility of wireless chargers which uses inductive coupling for power transfer. The WPC’s Qi specification is the world’s de facto wireless charging standard for small personal electronics. In [93], the health and safety considerations are presented for Qi-enabled devices. The authors also assessed the potential EM interference of a COTS-based NXP Qi-A13-enabled device as shown in Figure 12, when operated in the presence of active cardiovascular implantable electronic devices (CIEDs) with wireless power sources [94]. The authors also investigated whether permanent pacemakers (PPMs) and implantable cardioverter defibrillators (ICDs) were susceptible to EM fields generated by an active Qi-A13 device. The Avid Technologies Qi WPT receiver stimulator is used inside the torso, as shown in Figure 12c. The results indicate that inhomogeneous exposure of IWMDs to active Qi-A13 devices was within 46% of the performance limit even under worst-case conditions in a torso phantom. A 10 cm distance between the phantom and the Qi-A13 board guaranteed a safety margin for induced voltage levels 50 times below the permissible limit.
4. Compilation of Recent Publications on RF Transceiver-Based COTS-Enabled IWMDs
Table 6 represents an assortment of OEM and vendor RF transceiver-based COTS components which have been used to manufacture miniaturized IWMDs presented in the literature. RF transceivers are the most popular COTS components in IWMDs compared to PMU, microcontrollers and AFE due to their widely accepted custom-built chip counterparts. Table 6 lists the important parameters, such as manufacturer, wireless standard, source of power and the IWMD operation range for each of these RF transceiver COTS components. In addition to the following suggestions, the information provided in Table 6 can assist researchers and designers with the selection of COTS components for IWMD development.
- Near-field communications (NFC) and UHF RFID standards are suitable choices for battery-free IWMDs which operate over a very short-range (and contact-based) wireless connectivity and power transfer. In comparison with battery-operated MICS and BLE-enabled devices (ranging between −70 dBm and −100 dBm), implantable RFID devices have very poor RF receiver sensitivity levels (ranging between −10 and −20 dBm). This limits the operating range of battery-free RFID devices to a range of a few cm.
- Battery-operated COTS IWMDs can achieve wireless connectivity at distances greater than 1 m. However, they must contend with larger form factors and require rechargeable energy storage devices to operate over the desired application’s lifetime.
- A solar-powered implant potentially has an unlimited energy source and unlimited operating range [73] subject to the availability of direct sunlight. Additionally, the size of the solar cells to be used for IWMD is a concern.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 6.
List of COTS-enabled IWMDs.
| Compilation of Recent Publications on RF Transceiver-Based COTS-Enabled IWMDs | |||||
|---|---|---|---|---|---|
| Ref | COTS Component | Manufacturer (Vendor) | Wireless Standard | Power Source | Operating Range |
| [71] | SL900A RFID Sensory Tag | Austria Microsystems | UHF RFID | Battery-free | 60 cm |
| [98] | EM4325 RFID Sensory Tag | EM Microelectronics | UHF RFID | WPT: 6.78 MHz | Not mentioned |
| [99] | MONZA-4 RFID Chip | IMPINJ | UHF RFID | Battery-free | ≈35 cm |
| [100] | MONZA-4 RFID Die | IMPINJ | UHF RFID | Battery-free | ≈35 cm |
| [101] | G2X RFID Chip | NXP | UHF RFID | Battery-free | 20 cm |
| [102] | Alien Higgs-4 RFID Chip | Alien Technology | UHF RFID | Battery-free | 10 cm |
| [103] | Alien Higgs-4 RFID Chip | Alien Technology | UHF RFID | Battery-free | Not mentioned |
| [104] | Alien Higgs-4 RFID Chip | Alien Technology | UHF RFID | Battery-free | Not mentioned |
| [92] | CC430F5137 SoC, PIC12LF1552 | TI, Microchip | 433 MHz NFC RFID | WPT: 6.67 MHz, Rechargeable battery | 10 cm 8.8 cm |
| [105] | USRP B210 SDR | Ettus Research | UHF RFID | WPT: 13.56 MHz | 5 mm |
| [47] | ZL70101 | Microsemi | MICS 402 MHz | WPT 13.56 MHz | 2 m |
| [106] | ZL70102 | Microsemi | MICS 402 MHz | WPT TI: BQ51013 | 5 mm |
| [107] | ZL70101 | Microsemi | Implant 2.45 GHz WuR: 420 MHz | WPT: 13.56 MHz | ≈2 m |
| [108] | ZL70123 | Microsemi | MICS 402 MHz WuR: 420 MHz | 600 mAh Li-ion | ≈2.5 m |
| [75] | ZL70102 | Microsemi | MICS 402 MHz WuR: 2.45 GHz | WPT TI: BQ51013 | 1.98 m |
| [73] | RFD77101 | SIMBLEE | BLE: 2.45 GHz | 7 mAh rechargeable battery (VL1220) with solar panel | N/A |
| [96] | CC2640 | TI | BLE: 2.45 GHz | Battery | Not mentioned |
| [97] | nRF51822 | NORDIC | BLE: 2.45 GHz | Rechargeable Li-ion, WPT: 1.056 MHz | 10 mm |
5. Conclusions
This review highlights the versatility with which COTS components can be used for the development of IWMDs. Advances in material technologies and the development of novel micro- and nano-scale devices have been fundamental in the innovation of low-power miniaturized COTS components. Automated high-yield manufacturing processes have engendered the ubiquity of COTS used in the development of IWMDs. COTS components, particularly fully-integrated SoC modules, minimize BoM component count and associated time and costs for large-volume manufacture. Most manufacturers of COTS components provide hardware and software development tools and support resources throughout the application development process. Compared to a custom-built ASIC, the COTS components can significantly reduce the design cycle of an IWMD. Furthermore, the manufacturing cost of a single custom-built IC is extravagantly high.
COTS-enabled IWMDs play a fundamental role in healthcare networks, providing remote patient diagnostics and drug delivery services. In response to novel global epidemics such as COVID-19, the rapid development and deployment of high-quality first responder test equipment are crucial, where COTS components can offer robustness, reliability and significantly accelerate the development cycle for IWMDs. However, there are number of challenges associated with the utilization of COTS components for IWMDs. Current COTS components available on the market provide less opportunity for customization. Therefore, in many instances, it is difficult to find a COTS component that completely matches the requirements of a specific application. Furthermore, there are limited manufacturers of these COTS components, which can cause a monopoly during any pandemic situation and significantly increase costs. Higher demand from other industries can also limit the supply of a particular COTS component for IWMDs.
Although the majority of COTS components used to develop IWMDs are not designed for medical applications, research-generated concepts have demonstrated how versatile COTS components are. Commonly used ISM license-free wireless connectivity standards RIFD, BLE and MICS provide additional support for the development of IWMDs for better functionality, low cost and faster yield. Therefore, COTS-enabled devices offer promising research and manufacturing support for IWMDs as an alternative to custom building ASICs. Additionally, there are many promising opportunities for COTS components for IWMDs in the future. Modern programmable system on chip (PSoC) and field programmable gate array (FPGA) COTS devices provide designers the opportunity to customize IWMDs as per their requirements. Furthermore, many manufacturers are focusing on the production of significantly smaller form factor and low-power COTS components which can considerably reduce the size of the IWMDs and the power requirements, respectively. Manufacturers are also working to produce more flexible COTS sensors which can easily fit in critically curved body parts inside humans for IWMDs. The wireless aspects of the COTS-enabled IWMDs are also improving, as there are multiple new components emerging with higher bandwidth, distance requirements and significantly high-efficiency power supply.
Author Contributions
Conceptualization, A.J.M., S.R.K. and S.M.; methodology, A.J.M. and S.R.K.; resources, S.M.; writing—original draft preparation, A.J.M. and S.R.K.; writing—review and editing, A.T. and S.M.; supervision, S.M.; project administration, S.M.; funding acquisition, S.M. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by Legal and General PLC as part of their corporate social responsibility (CSR) programme, providing a research grant to establish the independent Advanced Care Research Centre at the University of Edinburgh. The funder had no role in conduct of the study, interpretation or the decision to submit for publication. The views expressed are those of the authors and not necessarily those of Legal and General PLC.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- John, O. Maintaining and sustaining a telehealth-based ecosystem. In Fundamentals of Telemedicine and Telehealth; Academic Press: Cambridge, MA, USA, 2020; pp. 127–143. [Google Scholar] [CrossRef]
- World Health Organization Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth. 2010. Available online: https://apps.who.int/iris/bitstream/handle/10665/44497/9789241564144_eng.pdf?sequence=1&isAllowed=y (accessed on 10 December 2021).
- Kaushik, A.; Mujawar, M.A. Point of Care Sensing Devices: Better Care for Everyone. Sensors 2018, 18, 4303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghafar-Zadeh, E. Wireless integrated biosensors for point-of-care diagnostic applications. Sensors 2015, 15, 3236–3261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trautner, B.W.; Darouiche, R.O. Catheter-associated infections: Pathogenesis affects prevention. Arch. Intern. Med. 2004, 164, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.C.; Gambini, S.; Izyumin, I.; Moin, A.; Zhou, A.; Alexandrov, G.; Santacruz, S.R.; Rabaey, J.M.; Carmena, J.M.; Muller, R. An implanTable 700μW 64-channel neuromodulation IC for simultaneous recording and stimulation with rapid artifact recovery. In Proceedings of the 2017 Symposium on VLSI Circuits, Kyoto, Japan, 5–8 June 2017; pp. C48–C49. [Google Scholar] [CrossRef] [Green Version]
- Bhamra, H.; Tsai, J.W.; Huang, Y.W.; Yuan, Q.; Shah, J.V.; Irazoqui, P. A Subcubic Millimeter Wireless Implantable Intraocular Pressure Monitor Microsystem. IEEE Trans. Biomed. Circ. Syst. 2017, 11, 1204–1215. [Google Scholar] [CrossRef]
- Chow, E.Y.; Chlebowski, A.L.; Chakraborty, S.; Chappell, W.J.; Irazoqui, P.P. Fully wireless implantable cardiovascular pressure monitor integrated with a medical stent. IEEE Trans. Biomed. Eng. 2010, 57, 1487–1496. [Google Scholar] [CrossRef]
- Charthad, J.; Chang, T.C.; Liu, Z.; Sawaby, A.; Weber, M.J.; Baker, S.; Gore, F.; Felt, S.A.; Arbabian, A. A mm-Sized wireless implantable device for electrical stimulation of peripheral nerves. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 257–270. [Google Scholar] [CrossRef]
- Bisht, R.; Mandal, A.; Mitra, A.K. Micro-and Nanotechnology-Based Implantable Devices and Bionics. In Emerging Nanotechnologies for Diagnostics, Drug Delivery and Medical Devices; Elsevier: Amsterdam, The Netherlands, 2017; pp. 249–290. [Google Scholar] [CrossRef]
- Meng, E.; Hoang, T. Micro- and nano-fabricated implantable drug-delivery systems. Ther. Deliv. 2012, 3, 1457–1467. [Google Scholar] [CrossRef] [Green Version]
- Kwong, D.-L. Bringing the Benefits of Moore’s Law to Medicine; Institute of Microelectronics, Agency for Science, Technology, and Research: Singapore, 2011. [Google Scholar]
- Kazmi, A.; Arslan, B.R.; Tulgar, M.; Pedersen, P.C.; Pahlavan, K.; Cengiz, B.; Arslan, A. Advances in wireless telemedicine: Improvements and challenges facing wireless ultrasound. In Proceedings of the 2000 IEEE EMBS International Conference on Information Technology Applications in Biomedicine, ITAB-ITIS, Arlington, VA, USA, 9–10 November 2000. [Google Scholar] [CrossRef]
- Fuller, J.L.; Gordon, T.M. The Radio Inductograph—A Device for Recording Physiological Activity in Unrestrained Animals. Science 1948, 108, 287–288. [Google Scholar] [CrossRef]
- Jacobson, B.; Mackay, R.S. A pH-endoradiosonde. Lancet 1957, 269, 1224. [Google Scholar] [CrossRef]
- Watson, B.W.; Ross, B.; Kay, A.W. Telemetering from within the body using a pressure-sensitive radio pill. Gut 1962, 3, 181. [Google Scholar] [CrossRef] [Green Version]
- Ko, W.H.; Neuman, M.R. Implant Biotelemetry and Microelectronics. Science 1967, 156, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Pipes, E.W. Miniaturuzed Radiotelemetry Device for Monitoring Temperatures; Union Carbide Corp.: Oak Ridge, TN, USA, 1966. [Google Scholar]
- Fryer, T. Implantable Biotelemetry Systems: A Report; NASA SP-5094; NASA: Pasadena, CA, USA, 1970. [Google Scholar]
- Troyk, P.R. Injectable electronic identification, monitoring, and stimulation systems. Annu. Rev. Biomed. Eng. 1999, 1, 177–209. [Google Scholar] [CrossRef] [PubMed]
- Fulford-Jones, T.; Welsh, M.; Moulton, S.; Malan, D. CodeBlue: An Ad Hoc Sensor Network Infrastructure for Emergency Medical Care. In Proceedings of the International Workshop on Wearable and Implantable Body Sensor Networks, London, UK, 6–7 April 2004. [Google Scholar]
- Xie, K.; Zhang, S.; Dong, S.; Li, S.; Yu, C.; Xu, K.; Chen, W.; Guo, W.; Luo, J.; Wu, Z. Portable wireless electrocorticography system with a flexible microelectrodes array for epilepsy treatment. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Faerber, J.; Cummins, G.; Pavuluri, S.K.; Record, P.; Rodriguez, A.R.A.; Lay, H.S.; McPhillips, R.; Cox, B.F.; Connor, C.; Gregson, R.; et al. In Vivo Characterization of a Wireless Telemetry Module for a Capsule Endoscopy System Utilizing a Conformal Antenna. IEEE Trans. Biomed. Circ. Syst. 2017, 12, 95–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avaltroni, P.; Nappi, S.; Marrocco, G.; Member, S. Antennifying Orthopedic Bone-Plate Fixtures for the Wireless Monitoring of Local Deep Infections. IEEE Sens. J. 2021, 21, 21012–21021. [Google Scholar] [CrossRef]
- Cohen, T. Medical and information technologies converge. IEEE Eng. Med. Biol. Mag. 2004, 23, 59–65. [Google Scholar] [CrossRef]
- Mahfouz, M.R.; Kuhn, M.J.; To, G. Wireless medical devices: A review of current research and commercial systems. In Proceedings of the IEEE Topical Conference on Biomedical Wireless Technologies, Networks, and Sensing Systems, Austin, TX, USA, 23–25 January 2013; pp. 16–18. [Google Scholar] [CrossRef]
- Elayan, H.; Shubair, R.M.; Kiourti, A. Wireless sensors for medical applications: Current status and future challenges. In Proceedings of the 11th European Conference on Antennas and Propagation (EUCAP), Paris, France, 19–24 March 2017; pp. 2478–2482. [Google Scholar] [CrossRef]
- WHO. A comprehensive guide to the Global Medical Device Nomenclature. 2010. Available online: https://www.who.int/medical_devices/innovation/GMDN_Agency_User_Guide_v120810.pdf (accessed on 14 July 2021).
- FDA Medical Device Databases. 2022. Available online: https://www.fda.gov/medical-devices/device-advice-comprehensive-regulatory-assistance/medical-device-databases (accessed on 14 July 2021).
- US Airforce Material Command: COTS Guide. 1993. Available online: https://nepp.nasa.gov/DocUploads/1219C61B-7337-48C4-8760E6456F861839/COTSguide.pdf (accessed on 14 July 2021).
- Texas Instruments INC Components for Space, Avionics and Defense. 2022. Available online: www.ti.com/SpaceAvionicsDefense (accessed on 14 July 2021).
- IEC/IEEE 62704-1. IEC/IEEE International Standard—Determining the Peak Spatial-Average Specific Absorption Rate (SAR) in the Human Body from Wireless Communications Devices, 30 MHz to 6 GHz—Part 1: General Requirements for Using the Finite-differ. 2017. Available online: https://standards.ieee.org/ieee/62704-1/5747 (accessed on 14 July 2021).
- Health Effects from Radiofrequency Electromagnetic Fields Report of the Independent Advisory Group on Non-Ionising Radiation. 2012. Available online: https://www.gov.uk/government/publications/radiofrequency-electromagnetic-fields-health-effects (accessed on 14 July 2021).
- Scenihr Opinion on Potential health effects of exposure to electromagnetic fields (EMF). EU Sci. Comm. 2015, 36, 480–484. [CrossRef]
- Madjar, H.M. Human radio frequency exposure limits: An update of reference levels in Europe, USA, Canada, China, Japan and Korea. IEEE Int. Symp. Electromagn. Compat. 2016, 2016, 467–473. [Google Scholar] [CrossRef]
- ICNIRP. Guidelines for Limiting Exposure to Electromagnetic Fields (100 kHz to 300 GHz). Health Phys. 2020, 118, 483–524. [Google Scholar] [CrossRef]
- Bocan, K.N.; Mickle, M.H.; Sejdic, E. Multi-Disciplinary Challenges in Tissue Modeling for Wireless Electromagnetic Powering: A Review. IEEE Sens. J. 2017, 17, 6498–6509. [Google Scholar] [CrossRef]
- Agarwal, A.; Shapero, A.; Rodger, D.; Humayun, M.; Tai, Y.C.; Emami, A. A wireless, low-drift, implantable intraocular pressure sensor with parylene-on-oil encapsulation. In Proceedings of the 2018 IEEE Custom Integrated Circuits Conference (CICC), San Diego, CA, USA, 8–11 April 2018. [Google Scholar] [CrossRef]
- LPS25H. MEMS Pressure Sensor: 260-1260 hPa Absolute Digital Output Barometer—STMicroelectronics. 2018. Available online: https://www.st.com/en/mems-and-sensors/lps25h.html (accessed on 7 March 2022).
- George, J.; Compagno, T.; Rodgers, K.; Waldron, F.; Barrett, J. Reliability of Plastic-Encapsulated Electronic Components in Supersaturated Steam Environments. IEEE Trans. Components Packag. Manuf. Technol. 2015, 5, 1423–1431. [Google Scholar] [CrossRef]
- 868 MHz Embedded Ceramic Loop Antenna for ISM/Lora/LPWAN/Sigfox. 2021. Available online: https://www.taoglas.com/product/530-5-ila-08-868mhz-embedded-ceramic-loop-antenna-ismloralpwansigfox (accessed on 14 July 2021).
- Johanson Technology. 868 MHz Antenna for Small Form Factor Applications. Available online: http://www.farnell.com/datasheets/2280483.pdf (accessed on 14 July 2021).
- 868/915 MHz. KIRBII, ISM SMD antenna—Antenova. 2016. Available online: http://antenova.com/wp-content/uploads/2015/11/Kirbii-A10472-PS-5.1.pdf?__hstc=176912634.486337ce428aefc1c912f83df14de3df.1626276596230.1626276596230.1626276596230.1&__hssc=176912634.1.1626276596231&__hsfp=2875711223&hsCtaTracking=459d335a-4319-4a90-bd00 (accessed on 14 July 2021).
- Surface Mount Ceramic Chip Antennas for 868 MHz. 2013. Available online: https://media.digikey.com/pdf/DataSheets/VishayVitramon/VJ5601M868MXBSR.pdf (accessed on 14 July 2021).
- WE-MCA Multilayer Chip Antenna. 2021. Available online: https://www.we-online.com/catalog/datasheet/7488910092.pdf (accessed on 19 April 2022).
- Cheng, K. Molex 2081420001-ISM 868/915 MHz Ceramic Antenna. 2020. Available online: https://www.molex.com/pdm_docs/ps/2081420001-PS.pdf (accessed on 19 April 2022).
- Charvet, G.; Foerster, M.; Filipe, S.; Porcherot, J.; Beche, J.F.; Guillemaud, R.; Audebert, P.; Regis, G.; Zongo, B.; Robinet, S.; et al. WIMAGINE: A wireless, low power, 64-channel ECoG recording platform for implantable BCI applications. In Proceedings of the 5th International IEEE/EMBS Conference on Neural Engineering, Cancun, Mexico, 27 April–1 May 2011; pp. 356–359. [Google Scholar] [CrossRef]
- 4-GHz BluetoothTM Low Energy and Proprietary System-on-Chip. 2013. Available online: https://www.ti.com/lit/ds/symlink/cc2541.pdf?ts=1640439778669&ref_url=https%253A%252F%252Fwww.google.com%252F (accessed on 3 December 2021).
- NXP Semiconductors UCODE® 7/7m. 2019. Available online: https://www.nxp.com/products/rfid-nfc/ucode-rain-rfid-uhf/ucode-7-7m:SL3S1204 (accessed on 14 July 2021).
- Higgins, H. Two way wireless communication with implanted sensors and therapeutic devices. IET Semin. Dig. 2009, 2009, 4. [Google Scholar] [CrossRef]
- Higgins, H. Body implant communication—Is it a reality? IET Semin. Dig. 2007, 2007, 33–36. [Google Scholar] [CrossRef]
- Ghomashchi, A.; Zheng, Z.; Majaj, N.; Trumpis, M.; Kiorpes, L.; Viventi, J. A low-cost, open-source, wireless electrophysiology system. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 27–31 August 2014; Volume 2014, pp. 3138–3141. [Google Scholar]
- Sun, X.C.; Tao, W.J.; Zhu, C.Q.; Zhao, L.L.; Wang, M.; Lu, X.Y.; Wang, Z.G.; Fan, Z.N. System design and experimental research of lower esophageal sphincter stimulator for treatment of gastroesophageal reflux disease. In Proceedings of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Korea, 11–15 July 2017; pp. 2177–2180. [Google Scholar] [CrossRef]
- Gottardi, D.; Wienstroer, V.; Kronberger, R. Animal Skin Phantom for RFID UHF Transponder Development. In Proceedings of the 2018 International Symposium on Antennas and Propagation (ISAP), Busan, Korea, 23–26 October 2018. [Google Scholar]
- ZL70101 Medical Implantable RF Transceiver Features. 2015. Available online: https://www.microsemi.com/document-portal/doc_view/127877-zl70101-1645-19-fullds-datasheet (accessed on 14 July 2021).
- Silva, N.M.; Santos, P.M.; Ferreira, J.A.F.; Soares Dos Santos, M.P.; Ramos, A.; Simões, J.A.O.; Reis, M.J.C.S.; Morais, R. Power management architecture for smart hip prostheses comprising multiple energy harvesting systems. Sens. Actuators A Phys. 2013, 202, 183–192. [Google Scholar] [CrossRef]
- Pederson, D.J.; Quinkert, C.J.; Arafat, M.A.; Somann, J.P.; Williams, J.D.; Bercich, R.A.; Wang, Z.; Albors, G.O.; Jefferys, J.G.R.; Irazoqui, P.P. The Bionode. ACM Trans. Embed. Comput. Syst. 2019, 18, 400. [Google Scholar] [CrossRef]
- Serra, P.A.; Rocchitta, G.; Bazzu, G.; Manca, A.; Puggioni, G.M.; Lowry, J.P.; O’Neill, R.D. Design and construction of a low cost single-supply embedded telemetry system for amperometric biosensor applications. Sens. Actuators B 2007, 122, 118–126. [Google Scholar] [CrossRef] [Green Version]
- PIC12F683 8-Pin flash-based, 8-Bit CMOS Microcontrollers with NanoWatt Technology. 2004. Available online: http://ww1.microchip.com/downloads/en/devicedoc/41211b.pdf (accessed on 14 July 2021).
- Arshak, K.; Lyons, G.; Cavanagh, L.; Clifford, S. Front-end signal conditioning used for resistance-based sensors in electronic nose systems: A review. Sens. Rev. 2003, 23, 230–241. [Google Scholar] [CrossRef] [Green Version]
- Horn, G.V.D.; Huijsing, J.H. Integrated Smart Sensor Calibration. Analog. Integr. Circ. Sign. Process. 1997, 14, 207–222. [Google Scholar] [CrossRef]
- Wilson, A.D.; Baietto, M. Applications and Advances in Electronic-Nose Technologies. Sensors 2009, 9, 5099–5148. [Google Scholar] [CrossRef]
- Lee, J.H.; Seo, D.W. Development of ECG Monitoring System and Implantable Device with Wireless Charging. Micromachines 2019, 10, 38. [Google Scholar] [CrossRef] [Green Version]
- Bilodeau, G.; Gagnon-Turcotte, G.; Gagnon, L.L.; Keramidis, I.; Timofeev, I.; De Koninck, Y.; Ethier, C.; Gosselin, B. A Wireless Electro-Optic Platform for Multimodal Electrophysiology and Optogenetics in Freely Moving Rodents. Front. Neurosci. 2021, 15, 990. [Google Scholar] [CrossRef] [PubMed]
- Ukkonen, L.; Sydänheimo, L.; Ma, S.; Björninen, T. Backscattering-based wireless communication and power transfer to small biomedical implants. In Proceedings of the Microfluidics, BioMEMS, and Medical Microsystems XVIII, San Francisco, CA, USA, 1–4 February 2020; Volume 11235, p. 112350A. [Google Scholar] [CrossRef]
- Großmann, S.; Ott, R.; Kosub, R.; Schmitz, K.-P.; Siewert, S.; Schmidt, W.; Grabow, N. Numerical investigation of stent designs for wireless access to integrated sensors. Curr. Dir. Biomed. Eng. 2019, 5, 497–499. [Google Scholar] [CrossRef]
- Shapero, A.; Agarwal, A.; Martinez, J.C.; Emami, A.; Humayun, M.S.; Tai, Y.C. Wireless Implantable Intraocular Pressure Sensor with Parylene-Oil-Encapsulation and Forward-Angled RF Coil. In Proceedings of the IEEE 32nd International Conference on Micro Electro Mechanical Systems, Seoul, Korea, 27–31 January 2019; pp. 21–24. [Google Scholar] [CrossRef]
- Becker, J.; Pellhammer, D.; Preißner, P.; Glöggler, J.C.; Lapatki, B.G.; Ortmanns, M. An implant for wireless in situ measurement of lip pressure with 12 sensors. In Proceedings of the 2017 IEEE Biomedical Circuits and Systems Conference, Turin, Italy, 19–21 October 2018; pp. 1–4. [Google Scholar] [CrossRef]
- SL900A EPC Sensor Tag and Data Logger IC. 2018. Available online: https://ams.com/sl900a (accessed on 14 July 2021).
- Di Trocchio, L.; Carucci, C.; Sindhu, K.R.; Morel, C.; Lachaud, J.L.; Bichon, S.; Gounel, S.; Mano, N.; Boiziau, C.; Dejous, C.; et al. Wireless in Vivo Biofuel Cell Monitoring. IEEE J. Electromagn. RF Microw. Med. Biol. 2021, 5, 25–34. [Google Scholar] [CrossRef]
- Vena, A.; Sorli, B.; Charlot, B.; Naudi, S. An RFID-based implant for identification and pressure sensing of orthopedic prosthesis. In Proceedings of the 1st URSI Atlantic Radio Science Conference (URSI AT-RASC); Institute of Electrical and Electronics Engineers (IEEE), Gran Canaria, Spain, 16–24 May 2015. [Google Scholar]
- Lazaro, M.; Lazaro, A.; Villarino, R. Feasibility of backscatter communication using LoRAWAN signals for deep implanted devices and wearable applications. Sensors 2020, 20, 6342. [Google Scholar] [CrossRef]
- Wu, T.; Redouté, J.M.; Yuce, M.R. A Wireless Implantable Sensor Design With Subcutaneous Energy Harvesting for Long-Term IoT Healthcare Applications. IEEE Access 2018, 6, 35801–35808. [Google Scholar] [CrossRef]
- Bluetooth, S. SimbleeTM RFD77101 IoT for Connecting Everyone and Everything. 2015. Available online: https://cdn.sparkfun.com/datasheets/IoT/Simblee%20RFD77101%20Datasheet%20v1.0.pdf (accessed on 14 July 2021).
- Shon, A.; Chu, J.-U.; Jung, J.; Kim, H.; Youn, I. An Implantable Wireless Neural Interface System for Simultaneous Recording and Stimulation of Peripheral Nerve with a Single Cuff Electrode. Sensors 2017, 18, 1. [Google Scholar] [CrossRef] [Green Version]
- Bentler, C.; Stieglitz, T. Building wireless implantable neural interfaces within weeks for neuroscientists. In Proceedings of the 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 1078–1081. [Google Scholar] [CrossRef]
- Bock, D.C.; Marschilok, A.C.; Takeuchi, K.J.; Takeuchi, E.S. Batteries used to Power Implantable Biomedical Devices. Electrochim. Acta 2012, 84, 155–164. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, E.S.; Leising, R.A. Lithium Batteries for Biomedical Applications. MRS Bull. 2002, 27, 624–627. [Google Scholar] [CrossRef]
- Qualliion Medical Batteries: Powering Life. 2016. Available online: https://www.enersys.com/en/products/batteries/quallion/quallion-lithium (accessed on 14 July 2021).
- Young, D.J.; Cong, P.; Suster, M.A.; Damaser, M. Implantable wireless battery recharging system for bladder pressure chronic monitoring. Lab Chip 2015, 15, 4338. [Google Scholar] [CrossRef]
- J. Macsalka. Micro3—QL0003B Rechargeable Lithium Ion Battery. Available online: https://medical.enersys.com/products (accessed on 13 December 2021).
- Bhatia, N.; El-Chami, M. Leadless pacemakers: A contemporary review. J. Geriatr. Cardiol. 2018, 15, 249. [Google Scholar] [CrossRef]
- Liu, G.; Mao, L.; Chen, L.; Xie, S. Locatable-Body Temperature Monitoring Based on Semi-Active UHF RFID Tags. Sensors 2014, 14, 5952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Salmerón, J.; Rivadeneyra, A.; Martínez-Martí, F.; Capitán-Vallvey, L.F.; Palma, A.J.; Carvajal, M.A. Passive UHF RFID Tag with Multiple Sensing Capabilities. Sensors 2015, 15, 26769–26782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rennane, A.; Fonseca, N.; Abdelnour, A.; Benmahmoud, F.; Kaddour, D.; Touhami, R.; Tedjini, S. Passive UHF RFID Sensor Tag for Pressure and Temperature Conditions Monitoring. In Proceedings of the 2nd URSI Atlantic Radio Science Meeting (AT-RASC), Gran Canaria, Spain, 28 May–1 June 2018. [Google Scholar] [CrossRef]
- De Donno, D.; Catarinucci, L.; Tarricone, L. RAMSES: RFID augmented module for smart environmental sensing. IEEE Trans. Instrum. Meas. 2014, 63, 1701–1708. [Google Scholar] [CrossRef]
- Jung, J.Y.; Kim, H.; Lee, H.S.; Yeom, K.W. An UHF RFID tag with long read range. In Proceedings of the 2009 European Microwave Conference (EuMC), Rome, Italy, 29 September–1 October 2009; pp. 1113–1116. [Google Scholar] [CrossRef]
- Khan, S.R.; Desmulliez, M.P.Y. Implementation of a Dual Wireless Power Transfer and Rotation Monitoring System for Prosthetic Hands. IEEE Access 2019, 7, 1. [Google Scholar] [CrossRef]
- Khan, S.R.; Desmulliez, M.P.Y. Towards a Miniaturized 3D Receiver WPT System for Capsule Endoscopy. Micromachines 2019, 10, 545. [Google Scholar] [CrossRef] [Green Version]
- Biswas, D.K.; Tasneem, N.T.; Mahbub, I. Optimization of Miniaturized Wireless Power Transfer System to Maximize Efficiency for Implantable Biomedical Devices. In Proceedings of the IEEE Texas Symposium on Wireless and Microwave Circuits and Systems (WMCS), Waco, TX, USA, 28–29 March 2019. [Google Scholar] [CrossRef]
- Ahmadi, M.M.; Sarbandi-Farahani, M. A Class-E Power and Data Transmitter with On–Off Keying Data Modulation for Wireless Power and Data Transmission to Medical Implants. Circ. Syst. Signal Process. 2020, 39, 4174–4186. [Google Scholar] [CrossRef]
- Bakula, M.; Pelgrims, P.; Puers, R. Wireless powering and communication for implants, based on a Royer oscillator with radio and near-field links. Sens. Actuators A 2016, 250, 273–280. [Google Scholar] [CrossRef]
- Seckler, T.; Jagielski, K.; Stunder, D. Assessment of Electromagnetic Interference with Active Cardiovascular Implantable Electronic Devices (CIEDs) Caused by the Qi A13 Design Wireless Charging Board. Int. J. Environ. Res. Public Health 2015, 12, 5886–5904. [Google Scholar] [CrossRef] [Green Version]
- Wireless Power Consortium. 2018. Available online: https://www.wirelesspowerconsortium.com (accessed on 14 July 2021).
- WCT1001A/WCT1003A. Automotive A13 Wireless Charging Application User’s Guide. 2014. Available online: https://www.nxp.com/docs/en/user-guide/WCT100XAWCAUG_V3.5.pdf (accessed on 14 July 2021).
- Zhou, L.; Chen, X.; Li, Y.; Li, J. Bluetooth low energy 4. 0-based communication method for implants. In Proceedings of the 10th International Congress on Image and Signal Processing, BioMedical Engineering and Informatics CISP-BMEI, Beijing, China, 13–15 October 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Su, Y.; Routhu, S.; Moon, K.S.; Lee, S.Q.; Youm, W.; Ozturk, Y. A Wireless 32-Channel Implantable Bidirectional Brain Machine Interface. Sensors 2016, 16, 1582. [Google Scholar] [CrossRef]
- Kracek, J.; Švanda, M.; Mazanek, M.; Machac, J. Implantable Semi-Active UHF RFID Tag with Inductive Wireless Power Transfer. IEEE Antennas Wirel. Propag. Lett. 2016, 15, 1657–1660. [Google Scholar] [CrossRef]
- Lodato, R.; Marrocco, G. Close Integration of a UHF-RFID Transponder into a Limb Prosthesis for Tracking and Sensing. IEEE Sens. J. 2016, 16, 1806–1813. [Google Scholar] [CrossRef]
- Lodato, R.; Lopresto, V.; Pinto, R.; Marrocco, G. Numerical and experimental characterization of through-the-body UHF-RFID links for passive tags implanted into human limbs. IEEE Trans. Antennas Propag. 2014, 62, 5298–5306. [Google Scholar] [CrossRef]
- Occhiuzzi, C.; Contri, G.; Marrocco, G. Design of implanted RFID tags for passive sensing of human body: The STENTag. IEEE Trans. Antennas Propag. 2012, 60, 3146–3154. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Miquel, A.; Medina-Rodriguez, B.; Vidal, N.; Ramos, F.M.; Roca, E.; Lopez-Villegas, J.M. Design and characterization of a miniaturized implantable UHF RFID tag based on LTCC technology. In Proceedings of the 11th European Conference on Antennas and Propagation (EUCAP), Paris, France, 19–24 March 2017; pp. 1024–1026. [Google Scholar] [CrossRef]
- Xu, J.; Sato, H.; Motoyoshi, M.; Suematu, N.; Kanetaka, H.; Yasui, K.; Chen, Q. Development of Denture Implanted RFID Tag Antennas. In Proceedings of the IEEE International Workshop on Electromagnetics: Applications and Student Innovation Competition (iWEM), Nagoya, Japan, 29–31 August 2018. [Google Scholar] [CrossRef]
- Rajagopalan, H.; Rahmat-Samii, Y. Ingestible RFID bio-capsule tag design for medical monitoring. In Proceedings of the IEEE Antennas and Propagation Society International Symposium, Toronto, ON, Canada, 11–17 July 2010. [Google Scholar] [CrossRef]
- Kampianakis, E.; Sharma, A.; Arenas, J.; Reynolds, M.S. A dual-band wireless power transfer and backscatter communication approach for implantable neuroprosthetic devices. IEEE J. Radio Freq. Identif. 2017, 1, 100–107. [Google Scholar] [CrossRef]
- Rotermund, D.; Pistor, J.; Hoeffmann, J.; Schellenberg, T.; Boll, D.; Tolstosheeva, E.; Gauck, D.; Stemmann, H.; Peters-Drolshagen, D.; Kreiter, A.K.; et al. Open Hardware: Towards a Fully-Wireless Sub-Cranial Neuro-Implant for Measuring Electrocorticography Signals. bioRxiv 2017, 15, 036855. [Google Scholar] [CrossRef] [Green Version]
- Fang, Q.; Lee, S.Y.; Permana, H.; Ghorbani, K.; Cosic, I. Developing a wireless implantable body sensor network in MICS band. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 567–576. [Google Scholar] [CrossRef]
- Tantin, A.; Letourneau, A.; Zgaren, M.; Hached, S.; Clausen, I.; Sawan, M. Implantable MICS-based wireless solution for bladder pressure monitoring. In Proceedings of the 2017 IEEE Biomedical Circuits and Systems Conference (BioCAS), Torino, Italy, 19–21 October 2017; pp. 1–4. [Google Scholar] [CrossRef]
Figure 1.
Contribution of IWMDs in a WBAN-based healthcare network.

Figure 2.
Example of an encapsulated wireless implant [38]. (a) Continuous IOP monitoring system. (b) Overall implemented system. (c) Proposed system encapsulated in parylene-on-oil.
Figure 2.
Example of an encapsulated wireless implant [38]. (a) Continuous IOP monitoring system. (b) Overall implemented system. (c) Proposed system encapsulated in parylene-on-oil.

Figure 3.
Essential blocks for a COTS-enabled IWMD.

Figure 4.
COTS Taoglas 868 MHz ceramic chip antenna: (a) 5 mm × 3 mm × 0.5 mm form factor; (b) 80 mm × 40 mm × 0.8 mm evaluation board [41].
Figure 4.
COTS Taoglas 868 MHz ceramic chip antenna: (a) 5 mm × 3 mm × 0.5 mm form factor; (b) 80 mm × 40 mm × 0.8 mm evaluation board [41].

Figure 5.
(a) The COTS Zarlink ZL70101 RF transceiver by Microsemi INC [55] used in wireless multi-channel acquisition system for generic interface with neurons (WIMAGINE) [47]. (b) Implantable flexible ECoG system using CC2541 tested on the left hemisphere of the brain of a Sprague–Dawley rat [22].
Figure 5.
(a) The COTS Zarlink ZL70101 RF transceiver by Microsemi INC [55] used in wireless multi-channel acquisition system for generic interface with neurons (WIMAGINE) [47]. (b) Implantable flexible ECoG system using CC2541 tested on the left hemisphere of the brain of a Sprague–Dawley rat [22].
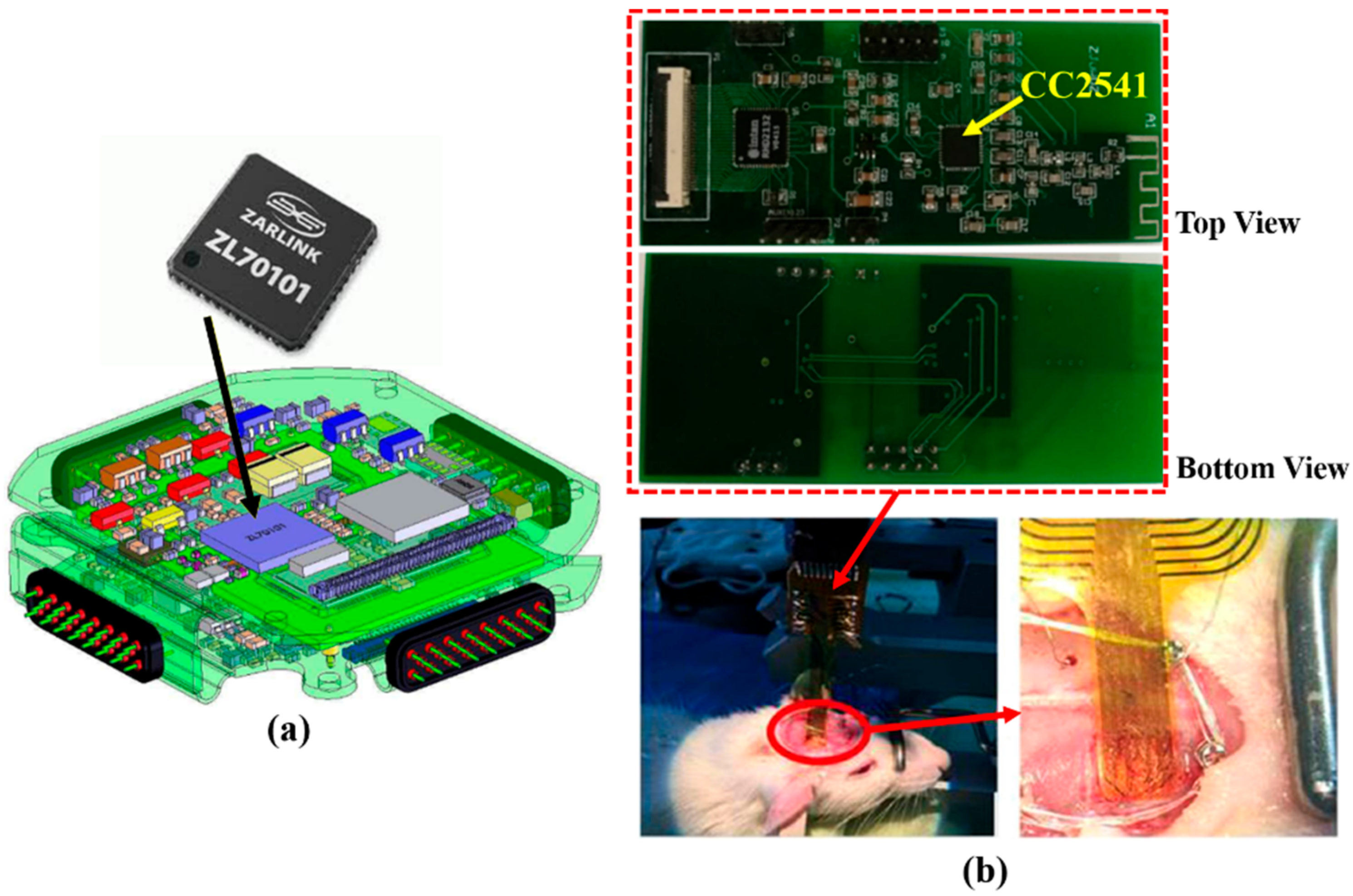
Figure 6.
(a) Smart hip prosthesis prototype. (b) Modules and subsystems used to characterize and validate PMU performance [56].
Figure 6.
(a) Smart hip prosthesis prototype. (b) Modules and subsystems used to characterize and validate PMU performance [56].

Figure 7.
(a) Ingestible wireless capsule. (b) Position of the RF and thermistor PCB boards inside capsule [23].
Figure 7.
(a) Ingestible wireless capsule. (b) Position of the RF and thermistor PCB boards inside capsule [23].

Figure 8.
Implantable ECG monitoring system. (a) Experimental setup with the system implanted into subcutaneous fat in a mini-pig. (b) Overall system configuration. (c) PCB of the proposed system [63].
Figure 8.
Implantable ECG monitoring system. (a) Experimental setup with the system implanted into subcutaneous fat in a mini-pig. (b) Overall system configuration. (c) PCB of the proposed system [63].

Figure 9.
(a) A 2 mm × 2 mm× 0.95 mm BMP 280 digital barometric pressure sensor. (b) Implant application for wireless in situ measurement of lip pressure using BMP280 [68].
Figure 9.
(a) A 2 mm × 2 mm× 0.95 mm BMP 280 digital barometric pressure sensor. (b) Implant application for wireless in situ measurement of lip pressure using BMP280 [68].

Figure 10.
(a) Single COTS-based SoC IWMD implant [71] demonstrating fabricated IWMD including antenna and SL900A chip [69]. (b) Demonstration of LORAWAN signal for IWMD built with multiple COTS [72].

Figure 11.
(a) A COTS 3.6 V 3 mAh QL0003B miniature rechargeable Li-ion battery used in pacemakers. The radius and height of the battery are 2.9 mm and 11.9 mm, respectively [81]. (b) State-of-the-art pacemakers: top left is the Micra and bottom right is the Nanostim [82].

Figure 12.
(a) EM interference test using a Qi-A13-Board. Test performed on torso phantom with CIED implant [93]. (b) NXP Qi-A13-Board [95]. (c) Avid Technologies Qi receiver stimulator [93].

Table 1.
Legacy of initial custom-built IWMDs.
| Year | Application | Reference |
|---|---|---|
| 1948 | Radio Inductograph | [14] |
| 1957 | pH-Endoradiosonde | [15] |
| 1962 | Telemetry pill | [16] |
| 1967 | Electrocardiogram (ECG), electroencephalogram (EEG), wireless biotelemetry | [17] |
Table 2.
Legacy of commercial COTS-enabled IWMDs.
| Year | Application | Reference |
|---|---|---|
| 1966 | A radio-telemetry device for monitoring temperature | [18] |
| 1970 | Implantable bio-telemetry systems | [19] |
| 1999 | Injectable electronic identification, monitoring and stimulation systems | [20] |
| 2000 | Advances in wireless telemedicine | [13] |
| 2002 | Wireless network for emergency medical care | [21] |
| 2011 | Wireless and implantable electrocorticogram recording system | [22] |
| 2018 | Wireless telemetry ingestible capsule | [23] |
| 2021 | Wireless monitoring of local deep infection | [24] |
Table 3.
COTS DRAs for miniaturized IWMDs.
| 868 MHz DRAs | ||
|---|---|---|
| Reference | Gain (dBi) | Size |
| [41] | −0.5 | 5 mm× 3 mm × 0.5 mm |
| [42] | −1 | 7 mm × 2 mm × 1.2 mm |
| [43] | +0.7 | 10 mm × 3 mm × 2 mm |
| [44] | +1.73 | 15.5 mm × 10.5 mm × 1.2 mm |
| [45] | −0.7 | 11 mm × 5.1 mm × 1.5 mm |
| [46] | 1.5 | 9 mm × 3 mm × 0.63 mm |
Table 4.
COTS wireless transceivers.
| Parameters | ZL70101 | CC2541 | Ucode7 |
|---|---|---|---|
| Manufacturer | Microsemi | TI | NXP |
| Standard | *** MICS | ** BLE 4.0 | * UHF RFID |
| Frequency | 402 to 405 MHz | 2.4 GHz | 860 to 960 MHz |
| Transmit current (mA) | 5 | 18 | Battery-free |
| Distance (m) free space | 1000 | 100 | 15 |
| Form factor | 7 mm × 7 mm × 0.9 mm | 6 mm × 6 mm × 1 mm | 1.5 mm × 1 mm × 0.5 mm |
| Application | ECG | ECoG, EEG, GERD | Tracking |
| References | [47,50,51] | [22,52,53] | [54] |
*** MICS: medical implant communication service. ** BLE: Bluetooth low energy. * UHF RFID: ultra-high-frequency radio frequency identification.
Table 5.
COTS-enabled implantable neural interface.
| Bill of Materials | |||
|---|---|---|---|
| VENDOR | Part Number | Description | Block |
| Intan Tech | RHD2164 | 64 CH. Chip | Recorder |
| Analog Devices | AD5863 | 16-bit DAC | Stimulus |
| ADG506A | Multiplexer | ||
| LT1638 | Opamp | ||
| N/A | N/A | 1 Zener Diode | Power Supply |
| N/A | 5 Capacitors | ||
| N/A | 4 Diodes | ||
| Lattice Semi | LCMX03LF-1300E | FPGA | Radio/MCU |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Khan, S.R.; Mugisha, A.J.; Tsiamis, A.; Mitra, S. Commercial Off-the-Shelf Components (COTS) in Realizing Miniature Implantable Wireless Medical Devices: A Review. Sensors 2022, 22, 3635. https://doi.org/10.3390/s22103635
AMA Style
Khan SR, Mugisha AJ, Tsiamis A, Mitra S. Commercial Off-the-Shelf Components (COTS) in Realizing Miniature Implantable Wireless Medical Devices: A Review. Sensors. 2022; 22(10):3635. https://doi.org/10.3390/s22103635
Chicago/Turabian StyleKhan, Sadeque Reza, Andrew J. Mugisha, Andreas Tsiamis, and Srinjoy Mitra. 2022. "Commercial Off-the-Shelf Components (COTS) in Realizing Miniature Implantable Wireless Medical Devices: A Review" Sensors 22, no. 10: 3635. https://doi.org/10.3390/s22103635
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.