
Non-Invasive Blood Glucose Estimation System Based on a Neural Network with Dual-Wavelength Photoplethysmography and Bioelectrical Impedance Measuring


Abstract
:1. Introduction
2. Physiological Parameter Feature Extraction
3. Analyses of Measurement Data Preprocessing Technology
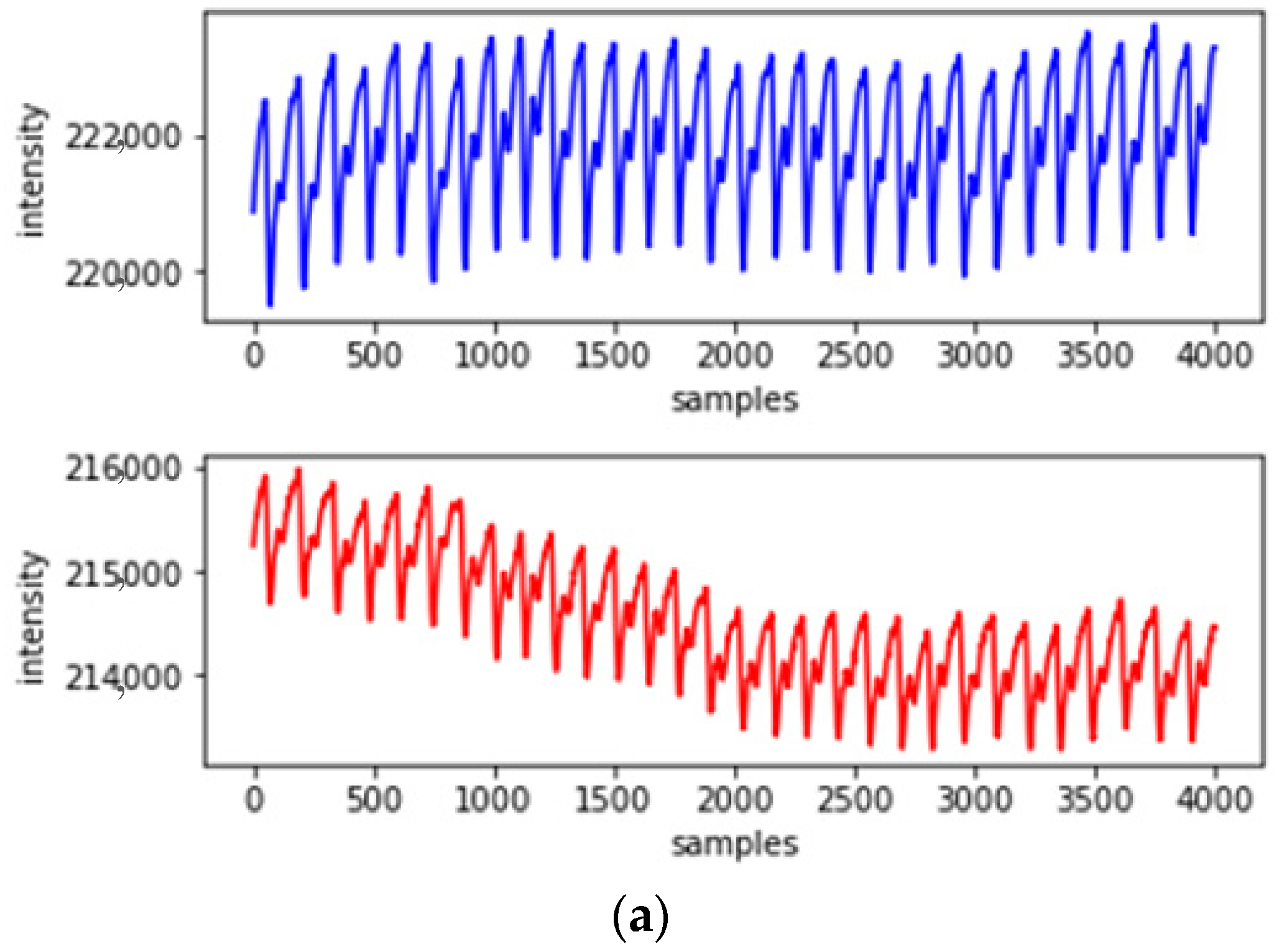
3.1. Motion Artifact Suppression Technology
3.2. Use of Principal Component Analyses to Reduce Dimensionality
- (1)
- Normalize and subtract the mean value from the data;
- (2)
- Calculate the covariance matrix through eigenvalue decomposition;
- (3)
- Calculate the eigenvalues and eigenvectors of the covariate matrix;
- (4)
- Select features and establish eigenvectors;
- (5)
- Map the original data to the selected principal component space to obtain the data after dimensionality reduction.
4. Experimental Method and System Configuration
4.1. Research Participants
- (1)
- Explain the research protocol and experimental method to each volunteer, and confirm that they met the inclusion criteria, after which they are asked to sign a consent form.
- (2)
- Participants placed their hands flat and at the same height as their hearts and sat still quietly for 3 min while PPG waveforms and bioelectrical impedance values were being collected.
- (3)
- After the PPG waveform and bioelectrical impedance measurement, the commercially available noninvasive glucose meter ESER GlucoGenius was used to conduct a 2 min measurement to obtain participants’ blood glucose values.
- (4)
- After the experiment, the participants’ characteristics such as age, height, weight, heart rate, blood flow velocity, hemoglobin, and blood oxygen saturation were obtained for neural network use.
4.2. Experimental System Architecture Diagram
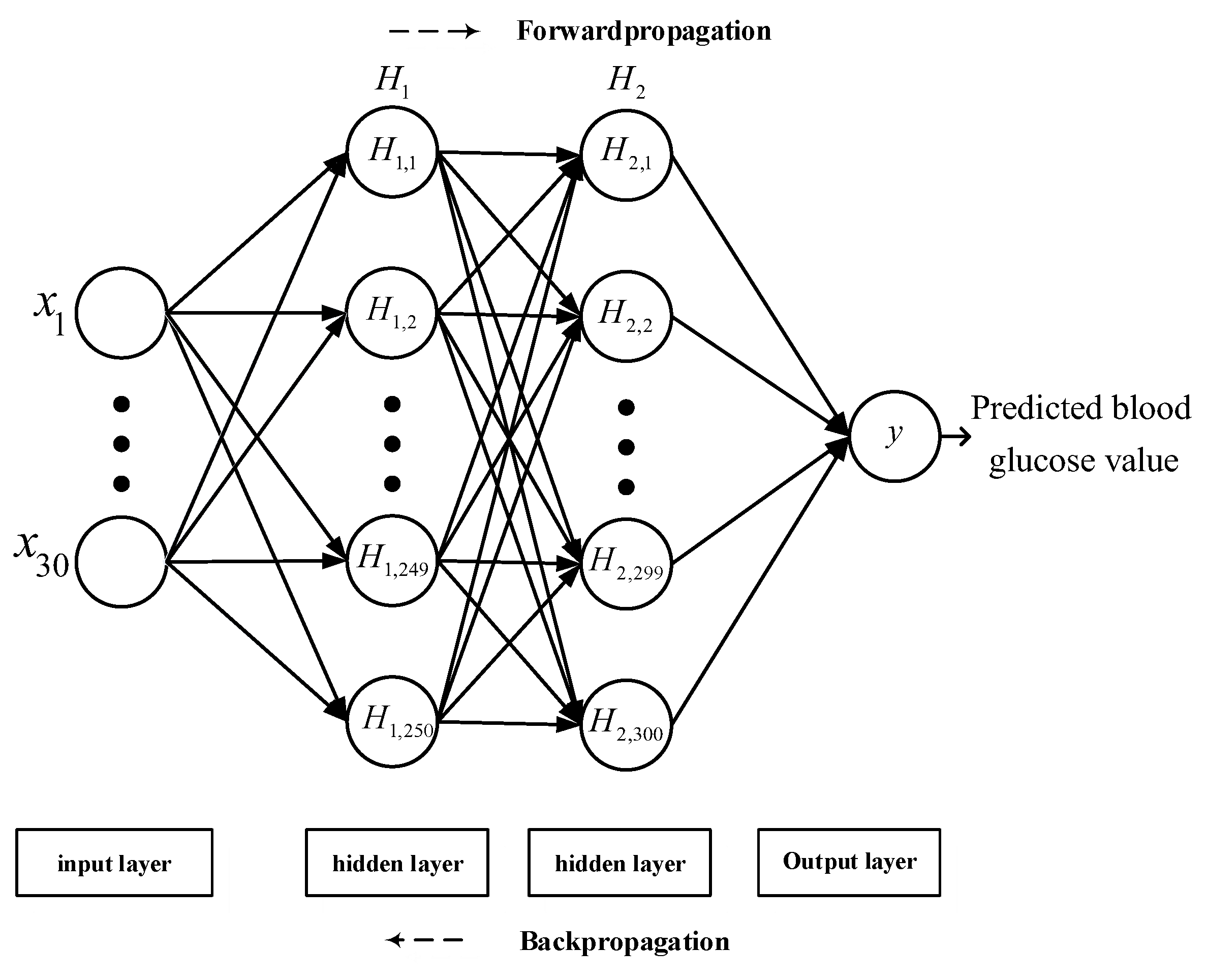
4.3. Back-Propagation Neural Network Design
4.4. Model Performance Evaluation
- (1)
- Mean squared error (MSE): The regression loss function used in machine learning, also known as L2 loss. It can judge the degree of change in the data through the sum of squares of the distance between the actual value and the predicted value. Therefore, a smaller MSE indicates a more favorable accuracy of model prediction.
- (2)
- Root mean squared error (RMSE): RMSE is used to measure the deviation between the actual quality and the predicted value. By calculating the sum of squares of the distance between the actual value and the predicted value, RMSE is equivalent to the square root of MSE, and its effect is to produce a more favorable description of the data.
- (3)
- Mean absolute error (MAE), also known as L1 loss: After taking the absolute value of all actual values and predicted values, the arithmetic mean is obtained. The presence of positive and negative errors during error calculation provides opportunities for the two types of errors to offset each other. Therefore, the absolute value is added for evaluation.
- (4)
- Mean absolute relative difference (MARD): MARD is an indicator used to assess continuous blood glucose monitoring. A lower value of the average difference between the actual and predicted values signifies a higher accuracy of the designed instrument.
- (5)
- Coefficient of determination (R2): The coefficient of determination is used to indicate the similarity of the actual data to the predicted data. A value between 0 and 1 is obtained by dividing the predicted variable by the target variable, with a value closer to 1 representing higher similarity.
- (6)
- Clarke EGA: Clarke EGA is the standard to determine the accuracy of blood glucose meters, which is achieved by quantifying the blood glucose values obtained by the glucose meter and comparing them with reference values. The grid consists of five regions. The values in region A indicate that the blood glucose level can be determined and used to enable the patient to receive the appropriate treatment. Region B indicates that the values have a large deviation from the reference values but will not cause adverse effects if they are used to determine treatments. Regions C, D, and E indicate that the values have deviated to the extent that should treatment be based on the values, the treatment will be unnecessary or harmful. Therefore, general precision blood glucose meter measurements should fall in regions A or B of the Clarke EGA.
5. Analyses and Discussion of Network Experiment Results
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nickerson, H.D.; Dutta, S. Diabetic Complications: Current Challenges and Opportunities. J. Cardiovasc. Transl. Res. 2012, 5, 375–379. [Google Scholar] [CrossRef] [Green Version]
- Abd Salam, N.A.B.; Bin Mohd Saad, W.H.; Manap, Z.B.; Salehuddin, F. The Evolution of Non-Invasive Blood Glucose Monitoring System for Personal Application. J. Telecommun. Electron. Comput. Eng. 2016, 8, 59–65. [Google Scholar]
- Park, E.-Y.; Baik, J.; Kim, H.; Park, S.-M.; Kim, C. Ultrasound-modulated optical glucose sensing using a 1645 nm laser. Sci. Rep. 2020, 10, 13361. [Google Scholar] [CrossRef] [PubMed]
- Rodbard, D. Continuous Glucose Monitoring: A Review of Successes, Challenges, and Opportunities. Diabetes Technol. Ther. 2016, 18 (Suppl. S2), S3–S13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villena Gonzales, W.; Mobashsher, A.T.; Abbosh, A. The Progress of Glucose Monitoring—A Review of Invasive to Minimally and Non-Invasive Techniques, Devices and Sensors. Sensors 2019, 19, 800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, V.; Liu, H.; Chen, F.; Qiu, Q.; Hughes, S.; Zheng, D. Quantitative Comparison of Photoplethysmographic Waveform Characteristics: Effect of Measurement Site. Front. Physiol. 2019, 10, 198. [Google Scholar] [CrossRef] [PubMed]
- Sen, P.K.; Laskar, M.R.; Das Mandal, S.K. Non-invasive Estimation of Blood Glucose Level in Visible-NIR Spectrum: System and Software Design. In Proceedings of the 2019 International Conference on Wireless Communications Signal Processing and Networking (WiSPNET), Chennai, India, 21–23 March 2019; pp. 416–420. [Google Scholar] [CrossRef]
- Deepthi, S.; Valke, N.S.; Parvathy, J.P.; Sai, A.K.; Sajjan, G. Non-invasive Blood Glucose Measurement System. In Proceedings of the 2019 IEEE International WIE Conference on Electrical and Computer Engineering (WIECON-ECE), Bangalore, India, 15–16 November 2019; pp. 1–4. [Google Scholar] [CrossRef]
- Hamdi, T.; Ali, J.B.; Fnaiech, N.; Di Costanzo, V.; Fnaiech, F.; Moreau, E.; Ginoux, J.-M. Artificial neural network for blood glucose level prediction. In Proceedings of the 2017 International Conference on Smart, Monitored and Controlled Cities (SM2C), Sfax, Tunisia, 17–19 February 2017; pp. 91–95. [Google Scholar] [CrossRef]
- Prabhu, P.; Selvabharathi, S. Deep Belief Neural Network Model for Prediction of Diabetes Mellitus. In Proceedings of the 2019 3rd International Conference on Imaging, Signal Processing and Communication (ICISPC), Singapore, 27–29 July 2019; pp. 138–142. [Google Scholar] [CrossRef]
- Manurung, B.E.; Munggaran, H.R.; Ramadhan, G.F.; Koesoema, A.P. Non-Invasive Blood Glucose Monitoring using Near-Infrared Spectroscopy based on Internet of Things using Machine Learning. In Proceedings of the 2019 IEEE R10 Humanitarian Technology Conference (R10-HTC), Depok, Indonesia, 12–14 November 2019; pp. 5–11. [Google Scholar] [CrossRef]
- Hina, A.; Saadeh, W. A Noninvasive Glucose Monitoring SoC Based on Single Wavelength Photoplethysmography. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Li, J.; Igbe, T.; Liu, Y.; Yan, C.; Nie, Z. Investigation on Dielectric Properties of Glucose Aqueous Solutions at 500 KHz-5MHz for Noninvasive Blood Glucose Monitoring. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Li, J.; Igbe, T.; Liu, Y.; Nie, Z.; Qin, W.; Wang, L.; Hao, Y. An Approach for Noninvasive Blood Glucose Monitoring Based on Bioimpedance Difference Considering Blood Volume Pulsation. IEEE Access 2018, 6, 51119–51129. [Google Scholar] [CrossRef]
- Fouad, M.M.; Mahmoud, D.Y.; Abd El Ghany, M.A. Joint NIR-BIS Based Non-Invasive Glucose Monitoring System. In Proceedings of the 2018 30th International Conference on Microelectronics (ICM), Sousse, Tunisia, 16–19 December 2018; pp. 88–91. [Google Scholar] [CrossRef]
- Nanayakkara, N.D.; Munasingha, S.C.; Ruwanpathirana, G.P. Non-Invasive Blood Glucose Monitoring using a Hybrid Technique. In Proceedings of the 2018 Moratuwa Engineering Research Conference (MERCon), Moratuwa, Sri Lanka, 30 May–1 June 2018; pp. 7–12. [Google Scholar] [CrossRef]
- Pathirage, K.D.; Roopasinghe, P.; Sooriyaarachchi, J.J.; Weththasinghe, R.; Nanayakkara, N.D. Removing subject dependencies on Non-Invasive Blood Glucose Measurement using Hybrid Techniques. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 7197–7200. [Google Scholar] [CrossRef]
- Krishnan, S.H.; Vinupritha, P.; Kathirvelu, D. Non-Invasive Glucose Monitoring using Machine Learning. In Proceedings of the 2020 International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 28–30 July 2020; pp. 780–783. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhu, J.-M.; Liang, Y.-B.; Chen, H.-B.; Yin, S.-M.; Chen, Z.-C. Non-invasive blood glucose detection system based on conservation of energy method. Physiol. Meas. 2017, 38, 325–342. [Google Scholar] [CrossRef] [PubMed]
- Nampoothiri, S.N.; Pathinarupothi, R.K.; Ramesh, M.V.; Menon, K.A.U. Comparison of Infrared and Red Photoplethysmography signals for Non-calibrated Non-invasive Blood Glucose Monitoring. In Proceedings of the 2020 IEEE Region 10 Symposium (TENSYMP), Dhaka, Bangladesh, 5–7 June 2020; pp. 1568–1571. [Google Scholar] [CrossRef]
- Gupta, S.S.; Hossain, S.; Haque, C.A.; Kim, K.-D. In-Vivo Estimation of Glucose Level Using PPG Signal. In Proceedings of the 2020 International Conference on Information and Communication Technology Convergence (ICTC), Jeju, Korea, 21–23 October 2020; pp. 733–736. [Google Scholar] [CrossRef]
- Habbu, S.; Dale, M.; Ghongade, R. Estimation of blood glucose by non-invasive method using photoplethysmography. Sādhanā 2019, 44, 135. [Google Scholar] [CrossRef] [Green Version]
- Siam, A.I.; Sedik, A.; El-Shafai, W.; Elazm, A.A.; El-Bahnasawy, N.A.; El Banby, G.M.; Khalaf, A.A.M.; El-Samie, F.E.A. Biosignal classification for human identification based on convolutional neural networks. Int. J. Commun. Syst. 2021, 34, e4685. [Google Scholar] [CrossRef]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef] [PubMed]
- Hina, A.; Saadeh, W. A 186μW Glucose Monitoring SoC using Near-Infrared Photoplethysmography. In Proceedings of the 2020 IEEE Asian Solid-State Circuits Conference (A-SSCC), Hiroshima, Japan, 9–10 November 2020; pp. 1–4. [Google Scholar] [CrossRef]
- Guzman, L.; Cazares, A.M.G.; Martinez-Torteya, A. Model for Glycemic Level Detection using Heart Rate Variability in a Mexican Sample. In Proceedings of the 2020 IEEE-EMBS Conference on Biomedical Engineering and Sciences (IECBES), Langkawi Island, Malaysia, 1–3 March 2021; pp. 505–510. [Google Scholar] [CrossRef]
- Zhu, J.; Zhou, Y.; Huang, J.; Zhou, A.; Chen, Z. Noninvasive Blood Glucose Concentration Measurement Based on Conservation of Energy Metabolism and Machine Learning. Sensors 2021, 21, 6989. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Daily Activity |
|---|---|
| Age Range (years) | 18–25 |
| Height (cm) | 165 ± 20 |
| Weight (kg) | 65 ± 30 |
| Heart rate (bpm) | 70 ± 28 |
| Blood flow rate (mm/s) | 280 ± 100 |
| Hemoglobin (g/L) | 160 ± 20 |
| Pulse oximetry (%) | 94 ± 5 |
| blood glucose (mg/dL) | 110 ± 15 |
| 1 | Infrared light PPG mean | 2 | Red light PPG mean | 3 | Infrared light variance |
| 4 | Infrared light PPG variance | 5 | Infrared light PPG skewness | 6 | Red light PPG skewness |
| 7 | Infrared light PPG kurtosis | 8 | Red light PPG kurtosis | 9 | Infrared light PPG standard deviation |
| 10 | Red light PPG standard deviation | 11 | Infrared light PPG Information Entropy | 12 | Red light PPG Information Entropy |
| 13 | Age (years) | 14 | Height (cm) | 15 | Weight (kg) |
| 16 | Heart rate (bpm) | 17 | Blood flow rate (mm/s) | 18 | Hemoglobin (g/L) |
| 19 | Pulse oximetry (%) | 20 | Frequency 50k Bioelectrical Impedance values | 21 | Frequency 55k Bioelectrical Impedance values |
| 22 | Frequency 60k Bioelectrical Impedance values | 23 | Frequency 65k Bioelectrical Impedance values | 24 | Frequency 70k Bioelectrical Impedance values |
| 25 | Frequency 75k Bioelectrical Impedance values | 26 | Frequency 80k Bioelectrical Impedance values | 27 | Frequency 85k Bioelectrical Impedance values |
| 28 | Frequency 90k Bioelectrical Impedance values | 29 | Frequency 95k Bioelectrical Impedance values | 30 | Frequency 100k Bioelectrical Impedance values |
| Reference | Modality | MSE | RMSE | MAE | MARD | Clarke EGA | |
|---|---|---|---|---|---|---|---|
| Hina et al. [12] | NIRS | N/A | 11.20 | N/A | 7.62% | 0.937 | 95% in the A area |
| Hina et al. [25] | NIRS | N/A | 10.20 | N/A | 6.9% | 0.955 | N/A |
| Gupta et al. [21] | NIRS | N/A | N/A | N/A | N/A | 0.88 | N/A |
| Guzman et al. [26] | NIRS | N/A | 18.6621 | 16.4540 | N/A | N/A | N/A |
| Zhu et al. [27] | NIRS | N/A | N/A | N/A | 5.453% | 0.936 | 98.413% in the A area |
| Zeng et al. [13] | BIS | N/A | N/A | N/A | N/A | 0.99 | N/A |
| Nanayakkara et al. [16] | BIS + NIRS | N/A | 10.24 | N/A | N/A | 0.58 | 90% in the A area |
| Pathirage et al. [17] | BIS + NIRS | N/A | N/A | N/A | 9.3% | N/A | 86.1% in the A area |
| Fouad et al. [15] | BIS + NIRS | N/A | N/A | N/A | N/A | 0.918 | 100% in the A area |
| This work | BIS + NIRS | 40.736 | 6.3824 | 5.0896 | 4.4321% | 0.9970 | 100% in the A area |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, C.-T.; Chen, U.-H.; Wang, G.-C.; Chen, Z.-X. Non-Invasive Blood Glucose Estimation System Based on a Neural Network with Dual-Wavelength Photoplethysmography and Bioelectrical Impedance Measuring. Sensors 2022, 22, 4452. https://doi.org/10.3390/s22124452
Yen C-T, Chen U-H, Wang G-C, Chen Z-X. Non-Invasive Blood Glucose Estimation System Based on a Neural Network with Dual-Wavelength Photoplethysmography and Bioelectrical Impedance Measuring. Sensors. 2022; 22(12):4452. https://doi.org/10.3390/s22124452
Chicago/Turabian StyleYen, Chih-Ta, Un-Hung Chen, Guo-Chang Wang, and Zong-Xian Chen. 2022. "Non-Invasive Blood Glucose Estimation System Based on a Neural Network with Dual-Wavelength Photoplethysmography and Bioelectrical Impedance Measuring" Sensors 22, no. 12: 4452. https://doi.org/10.3390/s22124452