

A Computer Vision-Based System to Help Health Professionals to Apply Tests for Fall Risk Assessment
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hardware Architecture
2.2. Software Architecture
2.3. Using the MediaPipe Pose Solution
2.4. Parameters’ Computation
- Speed: To measure speed, the midpoint of the hip is taken and the displacement it experiences is calculated in 1-s time intervals.
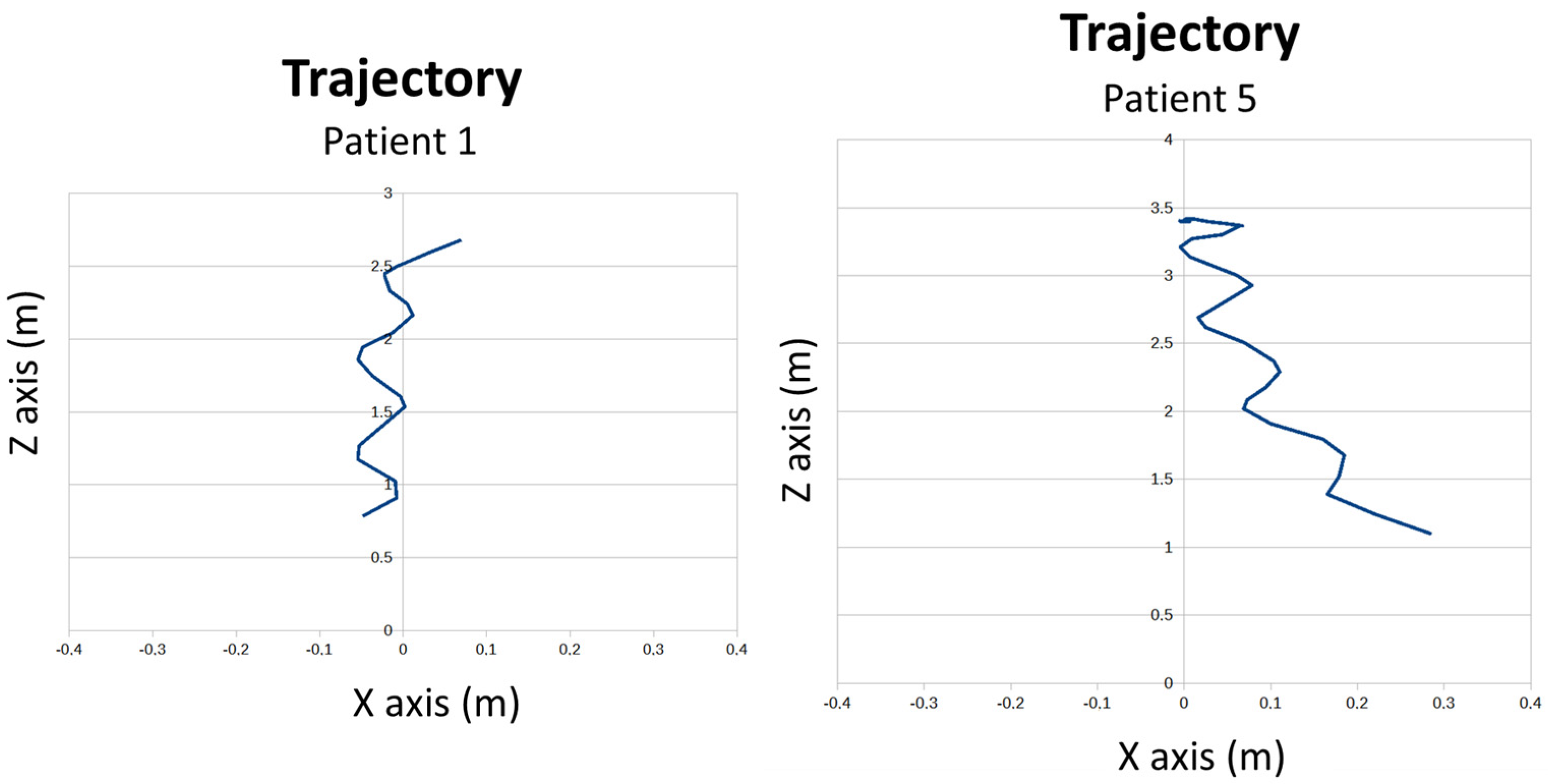
- Trajectory. To measure the trajectory, the midpoint of the hip is taken and projected onto the ground.
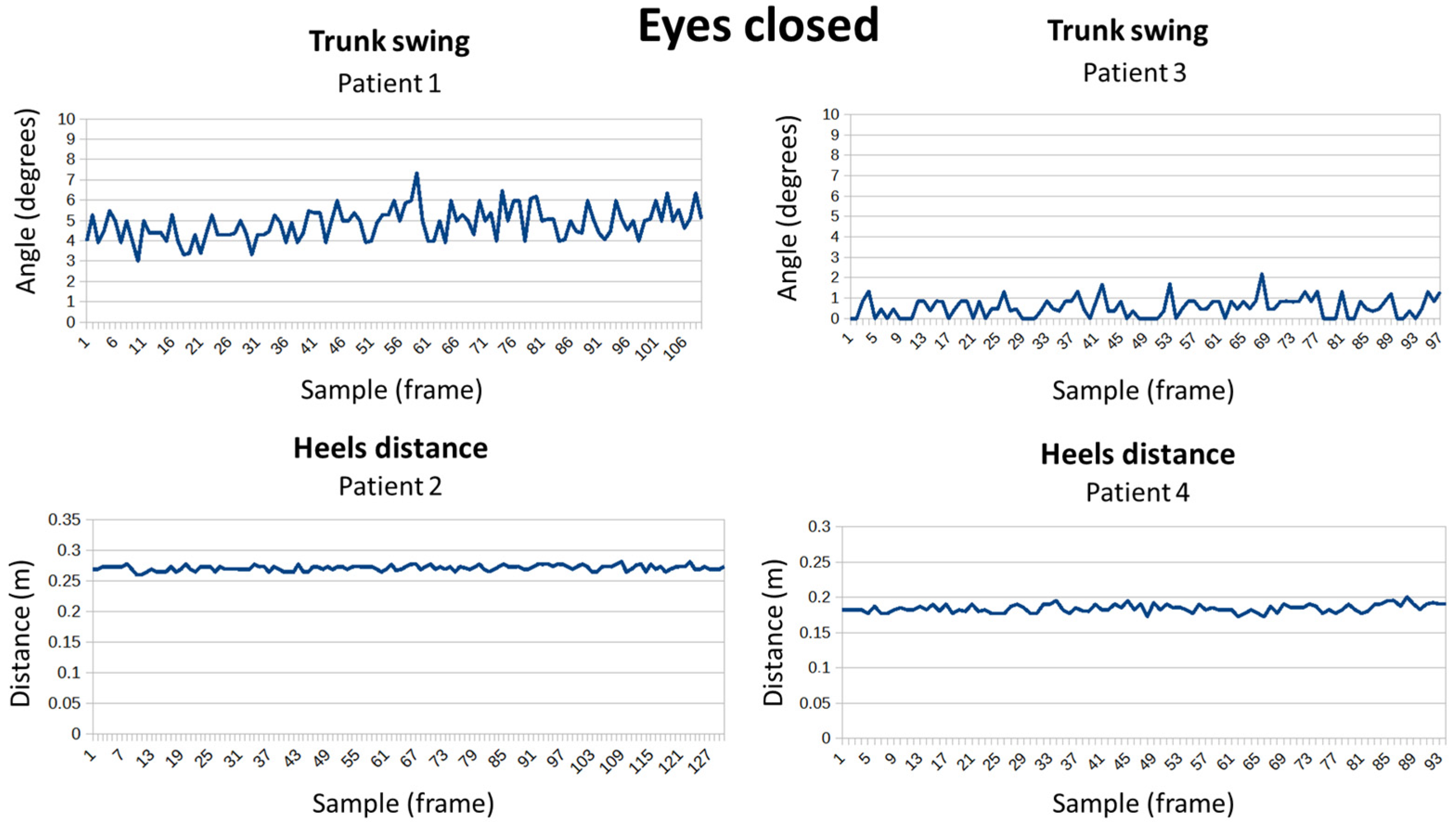
- Trunk swing (see Figure 4a): It is measured through the angle of inclination of the shoulders.
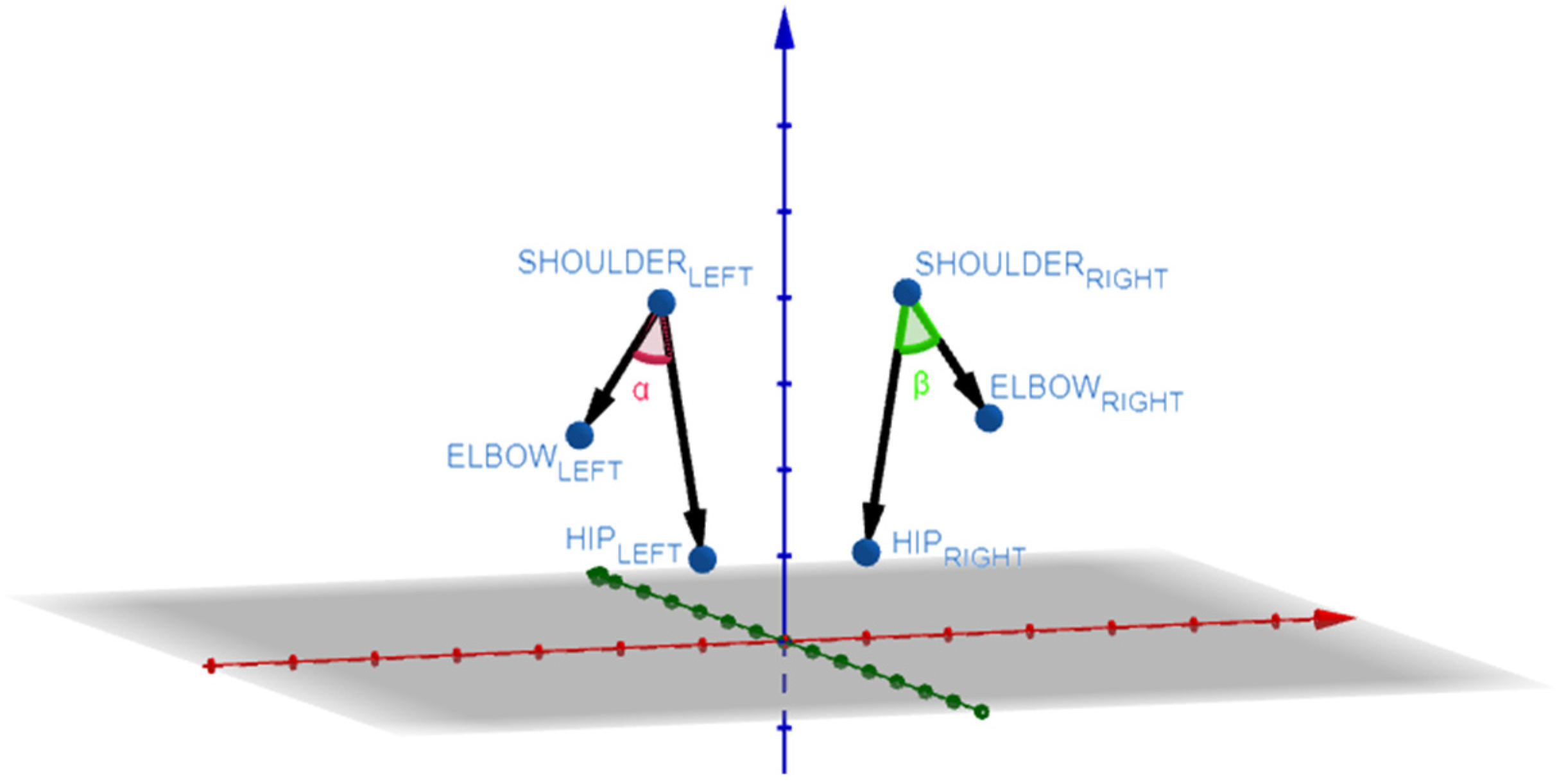
- Separation of the arms (see Figure 4b): The separation of the arms with respect to the trunk is calculated from two angles, one for each side. Using the points of the elbow, shoulder, and hip.
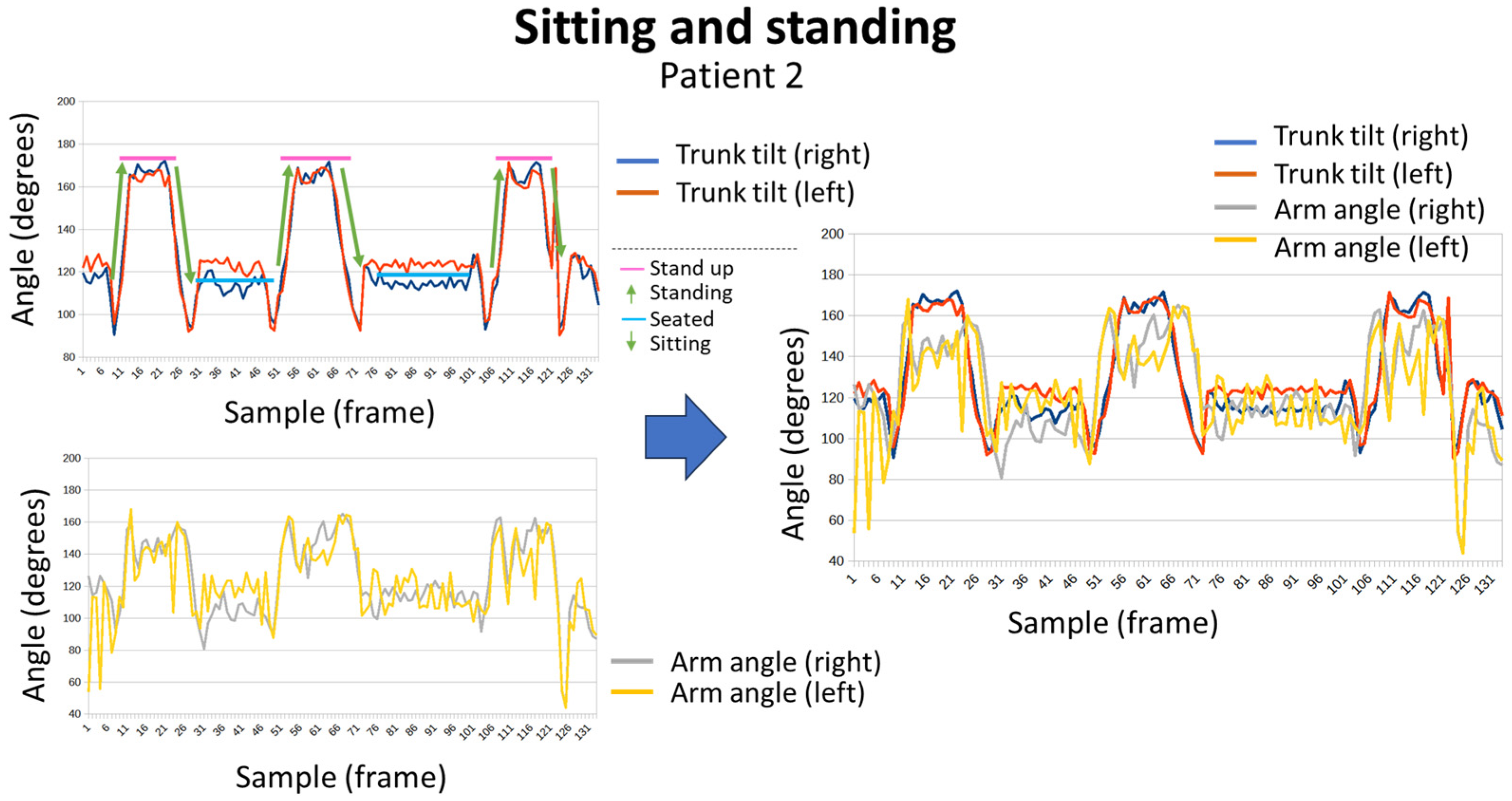
- Arm support (see Figure 4c): To measure whether the user uses their arms to get up from a chair, the angle formed by the shoulder, elbow, and wrist is calculated.
- Separation of the heels (see Figure 4d): The horizontal distance between the ankle points is calculated.
- Stride (see Figure 4e): To measure the amplitude of the steps, the depth difference between the ankle joints is calculated.
- Hand separation (see Figure 4f): The movement of the hands while walking is measured by calculating the distance between the wrists.
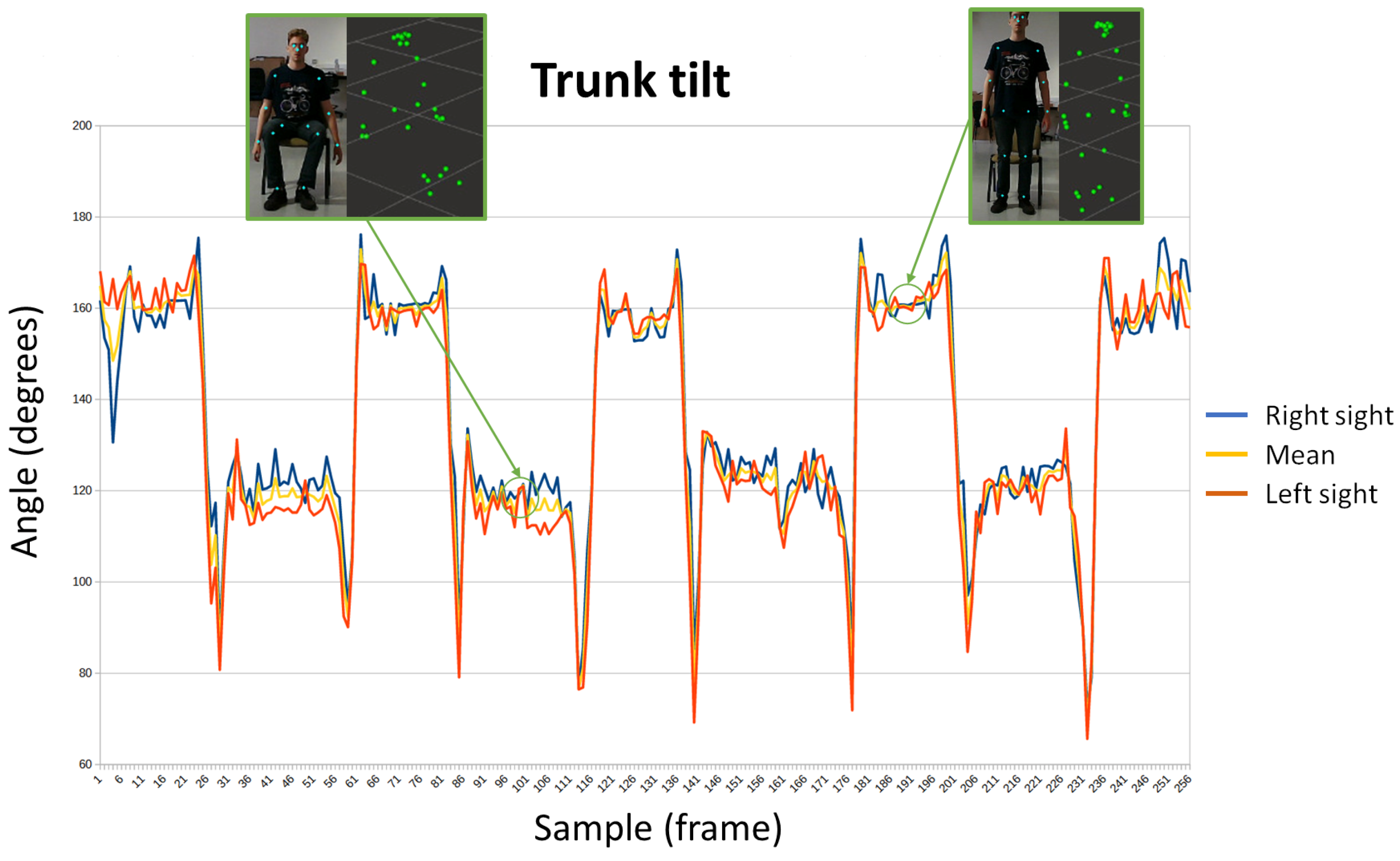
- Trunk tilt (see Figure 4g): To measure trunk tilt, the angle formed by the shoulder, hip, and knee is measured. Both on the right and left side.
2.5. Relation between Parameters and Items of Tests Used for Gait and Balance Evaluation
3. Results and Discussion
3.1. Controlled Laboratory Tests
3.2. Testing in a Real Environment
4. Limitations and Future Enhancement
- Currently, the system is ready to be mainly used in elderly institutions. The deployment of the system needs the involvement of some institution’s workers. Preventing the overload of such members’ work tasks is a goal for getting a better acceptance of the system. Therefore, the prototype will be used as a part of the rehabilitation programs existing in the institution. In the near future, when several robots are deployed as a result of the research project JUNO+, an improvement will be developed to allow assistant robots to autonomously guide the procedure for executing the tests. In this case, the therapist will only have to design the set of exercises that are included in each evaluated item (in a specific test) and to schedule the activity as a part of the rest of help tasks that the robot needs to carry out.
- The prototype has been designed after analyzing the needs and solutions found in the literature. However, it would be interesting to empirically study how the need for the digital transformation of health systems is perceived by clinicians (mainly in the context of elderly people monitoring and rehabilitation). In the near future, a usability study, which allows the comparison between applying tests in a traditional way and by using the proposed system, will be carried out. This usability test will be used to improve the prototype, adapting the user interface to the needs of therapists and caregivers (both formal and informal). Thus, the system could be used outside of the elderly institutions, for example with patients who live at home and are cared for by informal caregivers (for instance relatives).
- Table 1 shows the mapping between items and parameters calculated from raw data acquired the RGB-D sensor. Such mapping has been designed by the researchers, but it is expected to be empirically validated by clinicians and adapted, if needed, in a future work.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Envejecimiento y Salud. Available online: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health (accessed on 11 July 2023).
- Caídas. Available online: https://www.who.int/es/news-room/fact-sheets/detail/falls (accessed on 11 July 2023).
- Dyer, S.M.; Crotty, M.; Fairhall, N.; Magaziner, J.; Beaupre, L.A.; Cameron, I.D.; Sherrington, C. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016, 16, 158. [Google Scholar] [CrossRef]
- Pi, H.-Y.; Hu, M.-M.; Zhang, J.; Peng, P.-P.; Nie, D. Circumstances of falls and fall-related injuries among frail elderly under home care in China. Int. J. Nurs. Sci. 2015, 2, 237–242. [Google Scholar] [CrossRef]
- Soukola, S.K.; Jämsen, E.R.K.; Pauniaho, S.L.K.; Ukkonen, M.T. A population-based study of 2347 fall-related injuries among older people in a Finnish emergency department. Eur. Geriatr. Med. 2020, 11, 315–320. [Google Scholar] [CrossRef]
- KorKorenhof, S.; van Grieken, A.; Franse, C.; Tan, S.S.; Verma, A.; Alhambra, T.; Raat, H. The association of fear of falling and physical and mental Health-Related Quality of Life (HRQoL) among community-dwelling older persons; a cross-sectional study of Urban Health Centres Europe (UHCE). BMC Geriatr. 2023, 23, 291. [Google Scholar] [CrossRef]
- Dokuzlar, O.; Okudur, S.K.; Smith, L.; Soysal, P.; Yavuz, I.; Aydin, A.E.; Isik, A.T. Assessment of factors that increase risk of falling in older women by four different clinical methods. Aging Clin. Exp. Res. 2020, 32, 483–490. [Google Scholar] [CrossRef]
- Sotoudeh, G.R.; Mohammadi, R.; Mosallanezhad, Z.; Viitasara, E.; Soares, J.J. The prevalence, circumstances and consequences of unintentional falls among elderly Iranians: A population study. Arch. Gerontol. Geriatr. 2018, 79, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Burns, E.R.; Stevens, J.A.; Lee, R. The direct costs of fatal and non-fatal falls among older adults—United States. J. Saf. Res. 2016, 58, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Winser, S.J.; Chan, H.T.F.; Ho, L.; Chung, L.S.; Ching, L.T.; Felix, T.K.L.; Kannan, P. Dosage for cost-effective exercise-based falls prevention programs for older people: A systematic review of economic evaluations. Ann. Phys. Rehabil. Med. 2020, 63, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Ghezeljeh, T.N.; Yekta, Z.P.; Mehran, A.; Oori, M.J. Effect of a multidimensional fall prevention program on incidence of falling and quality of life among elderly. Hayat 2014, 20, 14–24. [Google Scholar]
- Deverall, E.; Kvizhinadze, G.; Pega, F.; Blakely, T.; Wilson, N. Exercise programmes to prevent falls among older adults: Modelling health gain, cost-utility and equity impacts. Inj. Prev. 2019, 25, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Laurent, L.; Koskas, P.; Estrada, J.; Sebbagh, M.; Lacaille, S.; Raynaud-Simon, A.; Lilamand, M. Tinetti balance performance is associated with mortality in older adults with late-onset Parkinson’s disease: A longitudinal study. BMC Geriatr. 2023, 23, 54. [Google Scholar] [CrossRef]
- Chawan, V.R.; Huber, M.; Burns, N.; Daniel, K. Person Identification and Tinetti Score Prediction Using Balance Parameters: A Machine Learning Approach to Determine Fall Risk. In Proceedings of the 15th International Conference on PErvasive Technologies Related to Assistive Environments, Corfu, Greece, 29 June–1 July 2022; pp. 203–212. [Google Scholar] [CrossRef]
- Lee, E.Y.; Na, Y.; Cho, M.; Hwang, Y.M.; Kim, H.-S.; An, H.; Pyun, S.-B. Short-term and long-term predictors of balance function in stroke patients: A 6-month follow-up study. Int. J. Rehabil. Res. 2023, 46, 163–169. [Google Scholar] [CrossRef] [PubMed]
- El-Bagalaty, A.E.; Mohamed, M.E.-S.; Abdelraouf, O.R.; Ghafar, M.A.A.; Abdelaal, A.K.; Abdelgalil, A.A.; Mousa, G.S. Balance and Fall Risk Assessment in Community-Dwelling Older Adults after Recovery from COVID-19: A Cross-Sectional Study. Sports 2023, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- Evkaya, A.; Karadag-Saygi, E.; Bingul, D.K.; Giray, E. Validity and reliability of the Dynamic Gait Index in children with hemiplegic cerebral palsy. Gait Posture 2020, 75, 28–33. [Google Scholar] [CrossRef]
- Jonsdottir, J.; Mattos, F.G.M.; Torchio, A.; Corrini, C.; Cattaneo, D. Fallers after stroke: A retrospective study to investigate the combination of postural sway measures and clinical information in faller’s identification. Front. Neurol. 2023, 14, 1157453. [Google Scholar] [CrossRef] [PubMed]
- Zirek, E.; Mustafaoglu, R.; Cicek, A.; Ahmed, I.; Mavromoustakos, S. Reliability and Validity of the Turkish Version of the Modified Dynamic Gait Index in the Elderly. Eval. Health Prof. 2023, 46, 135–139. [Google Scholar] [CrossRef]
- Tavares, J.E.d.R.; Ullrich, M.; Roth, N.; Kluge, F.; Eskofier, B.M.; Gaßner, H.; Klucken, J.; Gladow, T.; Marxreiter, F.; da Costa, C.A.; et al. uTUG: An unsupervised Timed Up and Go test for Parkinson’s disease. Biomed. Signal Process. Control 2023, 81, 104394. [Google Scholar] [CrossRef]
- Rössler, R.; Rommers, N.; Kim, E.-K.; Iendra, L.; Sofios, A.; Giannouli, E.; Portegijs, E.; Rantanen, T.; Infanger, D.; Bridenbaugh, S.; et al. Timed up-and-go performance is associated with objectively measured life space in patients 3 months after ischemic stroke: A cross-sectional observational study. J. Neurol. 2023, 270, 1999–2009. [Google Scholar] [CrossRef]
- Mutchie, H.L.; Orwig, D.L.; Beamer, B.; Conroy, V.; Guralnik, J.; Magaziner, J.; Gruber-Baldini, A.L. Four Square Step Test Performance in Hip Fracture Patients. J. Geriatr. Phys. Ther. 2022, 45, 81–89. [Google Scholar] [CrossRef]
- Kim, J.; Kim, I.; Kim, Y.E.; Koh, S.-B. The four square step test for assessing cognitively demanding dynamic balance in parkinson’s disease patients. J. Mov. Disord. 2021, 14, 208–213. [Google Scholar] [CrossRef]
- Ferreira, S.; Raimundo, A.; Marmeleira, J. Test-retest reliability of the functional reach test and the hand grip strength test in older adults using nursing home services. Ir. J. Med Sci. 2021, 190, 1625–1632. [Google Scholar] [CrossRef] [PubMed]
- Papa, E.V.; Dong, X.; Hassan, M. Resistance training for activity limitations in older adults with skeletal muscle function deficits: A systematic review. Clin. Interv. Aging 2017, 12, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Jamal, A.; Ahmad, I.; Ahamed, N.; Azharuddin, M.; Alam, F.; Hussain, M.E. Whole body vibration showed beneficial effect on pain, balance measures and quality of life in painful diabetic peripheral neuropathy: A randomized controlled trial. J. Diabetes Metab. Disord. 2020, 19, 61–69. [Google Scholar] [CrossRef]
- Mustafaoğlu, R.; Erhan, B.; Yeldan, İ.; Hüseyinsinoğlu, B.E.; Gündüz, B.; Özdinçler, A.R. The effects of body weight-supported treadmill training on static and dynamic balance in stroke patients: A pilot, single-blind, randomized trial. Turk. J. Phys. Med. Rehabil. 2018, 64, 344–352. [Google Scholar] [CrossRef]
- Su, Z.; Guo, Z.; Wang, W.; Liu, Y.; Liu, Y.; Chen, W.; Zheng, M.; Michael, N.; Lu, S.; Wang, W.; et al. The effect of telerehabilitation on balance in stroke patients: Is it more effective than the traditional rehabilitation model? A meta-analysis of randomized controlled trials published during the COVID-19 pandemic. Front. Neurol. 2023, 14, 1156473. [Google Scholar] [CrossRef] [PubMed]
- Zasadzka, E.; Trzmiel, T.; Pieczyńska, A.; Hojan, K. Modern Technologies in the Rehabilitation of Patients with Multiple Sclerosis and Their Potential Application in Times of COVID-19. Medicina 2021, 57, 549. [Google Scholar] [CrossRef]
- Van Jaarsveld, G.M. The Effects of COVID-19 Among the Elderly Population: A Case for Closing the Digital Divide. Front. Psychiatry 2020, 11, 577427. [Google Scholar] [CrossRef]
- Aydoğan, Z.; Baş, B.; Aksoy, S. Investigation of the Effects of COVID-19 on Perception, Attention, Memory, Balance, and Quality of Life in the Elderly. Top. Geriatr. Rehabil. 2022, 38, 270–276. [Google Scholar] [CrossRef]
- Ismail, A.M.A. Cancelled elderly exercise sessions during the COVID-19 crisis: Can physical therapists help from their homes? Eur. J. Physiother. 2020, 22, 235. [Google Scholar] [CrossRef]
- Frishammar, J.; Essén, A.; Bergström, F.; Ekman, T. Digital health platforms for the elderly? Key adoption and usage barriers and ways to address them. Technol. Forecast. Soc. Change 2023, 189, 122319. [Google Scholar] [CrossRef]
- Mozumder, A.I.; Armand, T.P.T.; Uddin, S.M.I.; Athar, A.; Sumon, R.I.; Hussain, A.; Kim, H.-C. Metaverse for Digital Anti-Aging Healthcare: An Overview of Potential Use Cases Based on Artificial Intelligence, Blockchain, IoT Technologies, Its Challenges, and Future Directions. Appl. Sci. 2023, 13, 5127. [Google Scholar] [CrossRef]
- Álvarez, M.N.; Ruiz, A.R.J.; Neira, G.G.-V.; Huertas-Hoyas, E.; Cerda, M.T.E.; Delgado, L.P.; Robles, E.R.; Del-Ama, A.J.; Ruiz-Ruiz, L.; García-De-Villa, S.; et al. Assessing falls in the elderly population using G-STRIDE foot-mounted inertial sensor. Sci. Rep. 2023, 13, 9208. [Google Scholar] [CrossRef]
- Liuzzi, P.; Carpinella, I.; Anastasi, D.; Gervasoni, E.; Lencioni, T.; Bertoni, R.; Carrozza, M.C.; Cattaneo, D.; Ferrarin, M.; Mannini, A. Machine learning based estimation of dynamic balance and gait adaptability in persons with neurological diseases using inertial sensors. Sci. Rep. 2023, 13, 8640. [Google Scholar] [CrossRef]
- Müller, R.; Hamacher, D.; Keune, P.M.; Oschmann, P. Stability of sensor-based gait parameters reassessed after a period of one year in people with multiple sclerosis. BMC Neurol. 2023, 23, 120. [Google Scholar] [CrossRef]
- Pan, Z.; Gao, H.; Chen, Y.; Xie, Z.; Xie, L. Evaluation of Hemiplegic Gait Based on Plantar Pressure and Inertial Sensors. IEEE Sens. J. 2023, 23, 12008–12017. [Google Scholar] [CrossRef]
- Tsakanikas, V.; Ntanis, A.; Rigas, G.; Androutsos, C.; Boucharas, D.; Tachos, N.; Skaramagkas, V.; Chatzaki, C.; Kefalopoulou, Z.; Tsiknakis, M.; et al. Evaluating Gait Impairment in Parkinson’s Disease from Instrumented Insole and IMU Sensor Data. Sensors 2023, 23, 3902. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Gao, C.; Li, H.; Huang, P.; Ling, Y.; Chen, Z.; Ren, K.; Chen, S. Wearable sensor-based gait analysis to discriminate early Parkinson’s disease from essential tremor. J. Neurol. 2023, 270, 2283–2301. [Google Scholar] [CrossRef]
- Horak, F.B.; Laird, A.; Carlson-Kuhta, P.; Abrahamson, M.; Mancini, M.; Orwoll, E.S.; Lapidus, J.A.; Shah, V.V. The Instrumented Stand and Walk (ISAW) test to predict falls in older men. GeroScience 2023, 45, 823–836. [Google Scholar] [CrossRef]
- Ko, J.B.; Hong, J.S.; Shin, Y.S.; Kim, K.B. Machine Learning-Based Predicted Age of the Elderly on the Instrumented Timed Up and Go Test and Six-Minute Walk Test. Sensors 2022, 22, 5957. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.; Kelly, P.; Huang, C.; Pearlmutter, A.; Izmailova, E.S. Sensor Verification and Analytical Validation of Algorithms to Measure Gait and Balance and Pronation/Supination in Healthy Volunteers. Sensors 2022, 22, 6275. [Google Scholar] [CrossRef]
- Kim, J.-K.; Bae, M.-N.; Lee, K.; Kim, J.-C.; Hong, S.G. Explainable Artificial Intelligence and Wearable Sensor-Based Gait Analysis to Identify Patients with Osteopenia and Sarcopenia in Daily Life. Biosensors 2022, 12, 167. [Google Scholar] [CrossRef] [PubMed]
- Aqueveque, P.; Gomez, B.; Ortega-Bastidas, P.; Pena, G.; Retamal, G.; Cano-De-La-Cuerda, R. Predicting risk of falls in elderly using a single Inertial Measurement Unit on the lower-back by estimating spatio-temporal gait parameters. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Glasgow, UK, 11–15 July 2022; pp. 2390–2394. [Google Scholar] [CrossRef]
- Greene, B.R.; Premoli, I.; McManus, K.; McGrath, D.; Caulfield, B. Predicting fall counts using wearable sensors: A novel digital biomarker for parkinson’s disease. Sensors 2022, 22, 54. [Google Scholar] [CrossRef] [PubMed]
- Rashid, U.; Barbado, D.; Olsen, S.; Alder, G.; Elvira, J.L.L.; Lord, S.; Niazi, I.K.; Taylor, D. Validity and reliability of a smartphone app for gait and balance assessment. Sensors 2022, 22, 124. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Parker, S.M.; Knarr, B.A.; Gwon, Y.; Youn, J.-H. Wearable sensor-based prediction model of timed up and go test in older adults. Sensors 2021, 21, 6831. [Google Scholar] [CrossRef] [PubMed]
- Baker, N.; Gough, C.; Gordon, S.J. Inertial sensor reliability and validity for static and dynamic balance in healthy adults: A systematic review. Sensors 2021, 21, 5167. [Google Scholar] [CrossRef] [PubMed]
- García-Villamil, G.; Neira-Álvarez, M.; Huertas-Hoyas, E.; Ramón-Jiménez, A.; Rodríguez-Sánchez, C. A pilot study to validate a wearable inertial sensor for gait assessment in older adults with falls. Sensors 2021, 21, 4334. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.-L.; Chen, H.-J.; Chen, P.-Y.; Chou, L.-W.; Lai, C.-H.; Lu, Y.-H.; Chiang, S.-L.; Lin, C.-H.; Wang, X.-M.; Lin, C.-H. Validating stroke-induced bilateral ankle coordination deficits using bilateral ankle measure relationship with motor functions in lower limbs. J. Neuroeng. Rehabil. 2023, 20, 32. [Google Scholar] [CrossRef]
- Park, G.-M.; Cho, S.-H.; Hong, J.-T.; Kim, D.-H.; Shin, J.-C. Effects and Safety of Wearable Exoskeleton for Robot-Assisted Gait Training: A Retrospective Preliminary Study. J. Pers. Med. 2023, 13, 676. [Google Scholar] [CrossRef]
- Miyagawa, D.; Matsushima, A.; Maruyama, Y.; Mizukami, N.; Tetsuya, M.; Hashimoto, M.; Yoshida, K. Gait training with a wearable powered robot during stroke rehabilitation: A randomized parallel-group trial. J. Neuroeng. Rehabil. 2023, 20, 54. [Google Scholar] [CrossRef]
- Pavón-Pulido, N.; López-Riquelme, J.A.; Feliú-Batlle, J.J. IoT Architecture for Smart Control of an Exoskeleton Robot in Rehabilitation by Using a Natural User Interface Based on Gestures. J. Med. Syst. 2020, 44, 144. [Google Scholar] [CrossRef]
- Osterloh, J.; Knaack, F.; Bader, R.; Behrens, M.; Peschers, J.; Nawrath, L.; Bergschmidt, P.; Darowski, M. The effect of a digital-assisted group rehabilitation on clinical and functional outcomes after total hip and knee arthroplasty—A prospective randomized controlled pilot study. BMC Musculoskelet. Disord. 2023, 24, 190. [Google Scholar] [CrossRef] [PubMed]
- Shayestegan, M.; Kohout, J.; Trnková, K.; Chovanec, M.; Mareš, J. Motion Tracking in Diagnosis: Gait Disorders Classification with a Dual-Head Attentional Transformer-LSTM. Int. J. Comput. Intell. Syst. 2023, 16, 98. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Josman, N.; Bitterman, N.; Rosenblum, S.; Naaman, S.; Gilboa, Y. The development of a home-based technology to improve gait in people with Parkinson’s disease: A feasibility study. Biomed. Eng. Online 2023, 22, 2. [Google Scholar] [CrossRef] [PubMed]
- Duncan, L.; Zhu, S.; Pergolotti, M.; Giri, S.; Salsabili, H.; Faezipour, M.; Ostadabbas, S.; Mirbozorgi, S.A. Camera-Based Short Physical Performance Battery and Timed Up and Go Assessment for Older Adults with Cancer. IEEE Trans. Biomed. Eng. 2023, 70, 2529–2539. [Google Scholar] [CrossRef]
- Lau, X.L.; Connie, T.; Goh, M.K.O.; Lau, S.H. Fall Detection and Motion Analysis Using Visual Approaches. Int. J. Technol. 2022, 13, 1173–1182. [Google Scholar] [CrossRef]
- Seifallahi, M.; Mehraban, A.H.; Galvin, J.E.; Ghoraani, B. Alzheimer’s Disease Detection Using Comprehensive Analysis of Timed Up and Go Test via Kinect V.2 Camera and Machine Learning. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 1589–1600. [Google Scholar] [CrossRef]
- Yamada, A.; Jeong, S.; Aoyama, H.; Yonenobu, K.; Ogawa, K. Measurement and Evaluation Method of Gait Parameters for Timed Up and Go Test using an IoRT Care-Walker. In Proceedings of the International Conference on Control, Automation and Systems, Busan, Republic of Korea, 27–30 November 2022; pp. 278–280. [Google Scholar] [CrossRef]
- Zhao, Q.; Chen, Z.; Landis, C.D.; Lytle, A.; Rao, A.K.; Guo, Y.; Zanottot, D. Gait Analysis with an Integrated Mobile Robot and Wearable Sensor System Reveals Associations between Cognitive Ability and Dynamic Balance in Older Adults. In Proceedings of the IEEE RAS and EMBS International Conference on Biomedical Robotics and Biomechatronics, Seoul, Republic of Korea, 21–24 August 2022. [Google Scholar] [CrossRef]
- Balta, D.; Figari, G.; Paolini, G.; Pantzar-Castilla, E.; Riad, J.; Della Croce, U.; Cereatti, A. A Model-Based Markerless Protocol for Clinical Gait Analysis Based on a Single RGB-Depth Camera: Concurrent Validation on Patients With Cerebral Palsy. IEEE Access 2023, 11, 144377–144393. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Wu, G.; Van Der Helm, F.C.; Veeger, H.E.J.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Mobarak, R.; Tigrini, A.; Verdini, F.; Al-Timemy, A.H.; Fioretti, S.; Burattini, L.; Mengarelli, A. A Minimal and Multi-Source Recording Setup for Ankle Joint Kinematics Estimation during Walking Using Only Proximal Information From Lower Limb. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 812–821. [Google Scholar] [CrossRef]
- Duraffourg, C.; Bonnet, X.; Dauriac, B.; Pillet, H. Real Time Estimation of the Pose of a Lower Limb Prosthesis from a Single Shank Mounted IMU. Sensors 2019, 19, 2865. [Google Scholar] [CrossRef] [PubMed]
- MediaPipe Pose Solution. Available online: https://developers.google.com/mediapipe/solutions/vision/pose_landmarker (accessed on 15 October 2023).
- Quigley, M.; Conley, K.; Gerkey, B.P.; Faust, J.; Foote, T.; Leibs, J.; Wheeler, R.; Ng, A.Y. ROS: An open-source Robot Operating System. In Proceedings of the 2009 IEEE International Conference on Robotics and Automation (ICRA2009), Kobe, Japan, 12–17 May 2009. [Google Scholar]
- Kim, J.-W.; Choi, J.-Y.; Ha, E.-J.; Choi, J.-H. Human Pose Estimation Using MediaPipe Pose and Optimization Method Based on a Humanoid Model. Appl. Sci. 2023, 13, 2700. [Google Scholar] [CrossRef]
- Bazarevsky, V.; Grishchenko, I.; Raveendran, K.; Zhu, T.; Zhang, F.; Grundmann, M. BlazePose: On-device Real-time Body Pose tracking. In Proceedings of the CVPR Workshop on Computer Vision for Augmented and Virtual Reality, Seattle, WA, USA, 13–19 June 2020. [Google Scholar]
- Xu, H.; Bazavan, E.G.; Zanfir, A.; Freeman, W.T.; Sukthankar, R.; Sminchisescu, C. GHUM & GHUML: Generative 3D Human Shape and Articulated Pose Models. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 14–19 June 2020; pp. 6184–6193. [Google Scholar]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| S | T | TS | SA | SH | S | TT | HS | AS | ||
| TINETTI ITEMS | 1 | × | ||||||||
| 2 | × | × | ||||||||
| 3 | × | |||||||||
| 4 | × | × | ||||||||
| 5 | × | × | ||||||||
| 6 | × | × | ||||||||
| 7 | × | × | ||||||||
| 8 | × | × | × | × | ||||||
| 9 | × | × | × | |||||||
| 10 | × | |||||||||
| 11 | × | |||||||||
| 12 | × | |||||||||
| 13 | × | |||||||||
| 14 | × | |||||||||
| 15 | × | × | × | |||||||
| 16 | × | |||||||||
| BERG ITEMS | 1 | × | × | |||||||
| 2 | × | |||||||||
| 3 | × | × | ||||||||
| 4 | × | × | ||||||||
| 5 | × | × | ||||||||
| 6 | × | |||||||||
| 7 | × | × | ||||||||
| 8 | × | × | ||||||||
| 9 | × | |||||||||
| 10 | × | |||||||||
| 11 | × | × | ||||||||
| 12 | × | × | ||||||||
| 13 | × | × | ||||||||
| 14 | × | × | ||||||||
| DGI ITEMS | 1 | × | × | × | ||||||
| 2 | × | × | × | |||||||
| 3 | × | × | × | |||||||
| 4 | × | × | × | |||||||
| 5 | × | × | × | × | ||||||
| 6 | × | × | × | |||||||
| 7 | × | × | × | × | ||||||
| 8 | × | × | ||||||||
| TUG | × | × | ||||||||
| FRT | × | × | ||||||||
| FSST | × | × | × | |||||||
| SLS | × | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blasco-García, J.D.; García-López, G.; Jiménez-Muñoz, M.; López-Riquelme, J.A.; Feliu-Batlle, J.J.; Pavón-Pulido, N.; Herrero, M.-T. A Computer Vision-Based System to Help Health Professionals to Apply Tests for Fall Risk Assessment. Sensors 2024, 24, 2015. https://doi.org/10.3390/s24062015
Blasco-García JD, García-López G, Jiménez-Muñoz M, López-Riquelme JA, Feliu-Batlle JJ, Pavón-Pulido N, Herrero M-T. A Computer Vision-Based System to Help Health Professionals to Apply Tests for Fall Risk Assessment. Sensors. 2024; 24(6):2015. https://doi.org/10.3390/s24062015
Chicago/Turabian StyleBlasco-García, Jesús Damián, Gabriel García-López, Marta Jiménez-Muñoz, Juan Antonio López-Riquelme, Jorge Juan Feliu-Batlle, Nieves Pavón-Pulido, and María-Trinidad Herrero. 2024. "A Computer Vision-Based System to Help Health Professionals to Apply Tests for Fall Risk Assessment" Sensors 24, no. 6: 2015. https://doi.org/10.3390/s24062015