
Are Proton Pump Inhibitors Contributing in Emerging New Hypertensive Population?
 , ,
, ,
Abstract
:1. Introduction
2. Proton Pump Inhibitor and Overuse
3. PPIs over Time: Risks of Extended Use and High Dosages
4. Impacting Blood Pressure: PPIs and Their Potential Association with Hypertension
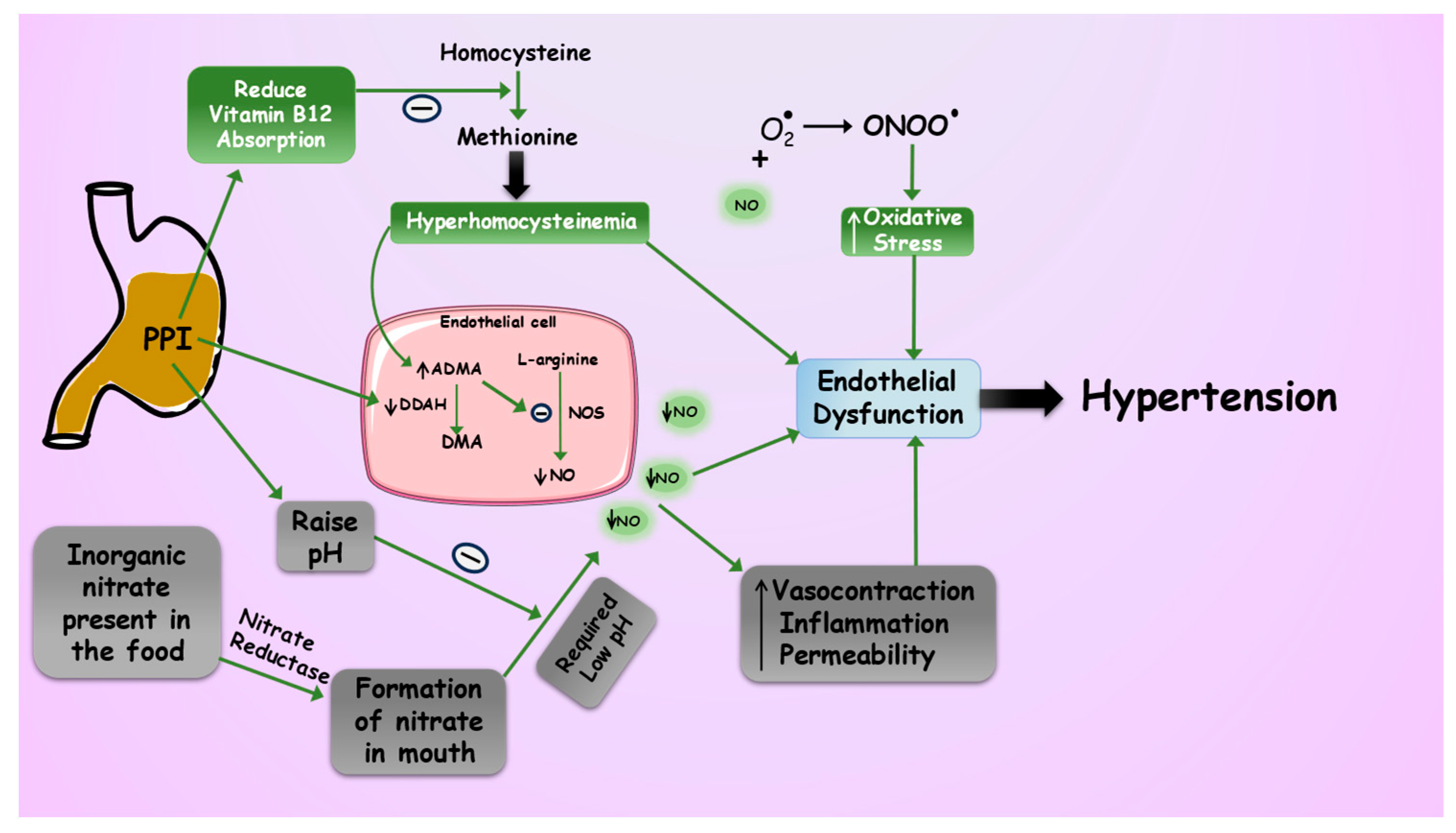
4.1. PPIs and Their Influence on Dimethylarginine Dimethylaminohydrolase Enzyme: Implications for Endothelial Dysfunction
4.2. PPIs and Reduced Nitric Oxide Bioavailability via Vitamin B Deficiency
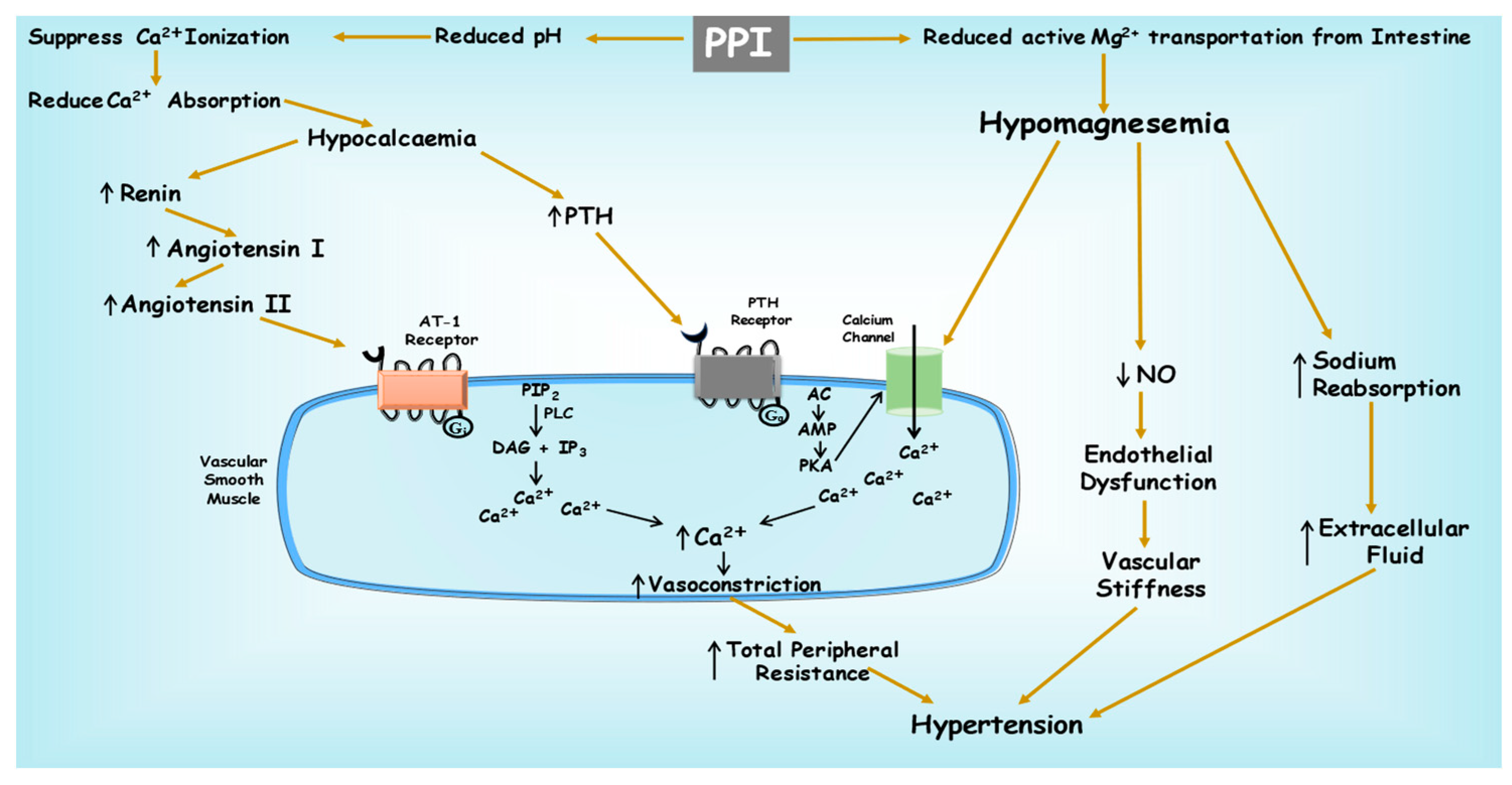
4.3. PPIs Potentially Enhance Vasoconstriction through Hypocalcaemia
4.4. PPI-Induced Hypomagnesemia and Damage to Vascular Function
5. Conclusions and Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scarpignato, C.; Gatta, L.; Zullo, A.; Blandizzi, C.; SIF-AIGO-FIMMG Group; Italian Society of Pharmacology, the Italian Association of Hospital Gastroenterologists, and the Italian Federation of General Practitioners. Effective and Safe Proton Pump Inhibitor Therapy in Acid-Related Diseases—A Position Paper Addressing Benefits and Potential Harms of Acid Suppression. BMC Med. 2016, 14, 179. [Google Scholar] [CrossRef]
- Strand, D.S.; Kim, D.; Peura, D.A. 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017, 11, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Raghunath, A.S.; O’Morain, C.; McLoughlin, R.C. Review Article: The Long-Term Use of Proton-Pump Inhibitors. Aliment. Pharmacol. Ther. 2005, 22 (Suppl. S1), 55–63. [Google Scholar] [CrossRef]
- Yu, L.-Y.; Sun, L.-N.; Zhang, X.-H.; Li, Y.-Q.; Yu, L.; Yuan, Z.-Q.-Y.; Meng, L.; Zhang, H.-W.; Wang, Y.-Q. A Review of the Novel Application and Potential Adverse Effects of Proton Pump Inhibitors. Adv. Ther. 2017, 34, 1070–1086. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Ma, M.; Chen, Y.; Zhang, J.; Li, J.; Jiang, S.; Wang, Y.; Huang, H.; He, Y. The Efficacy and Safety of Proton Pump Inhibitors Combining Dual Antiplatelet Therapy in Patients with Coronary Intervention: A Systematic Review, Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials. Rev. Cardiovasc. Med. 2023, 24, 230. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Ishimura, N.; Ishihara, S. Advantages and Disadvantages of Long-Term Proton Pump Inhibitor Use. J. Neurogastroenterol. Motil. 2018, 24, 182–196. [Google Scholar] [CrossRef]
- Sukhovershin, R.A.; Cooke, J.P. How may proton pump inhibitors impair cardiovascular health? Am. J. Cardiovasc. Drugs 2016, 16, 153–161. [Google Scholar] [CrossRef]
- Arora, A.; Behl, T.; Sehgal, A.; Singh, S.; Sharma, N.; Bhatia, S.; Sobarzo-Sanchez, E.; Bungau, S. Unravelling the Involvement of Gut Microbiota in Type 2 Diabetes Mellitus. Life Sci. 2021, 273, 119311. [Google Scholar] [CrossRef]
- Behl, T.; Bungau, S.; Kumar, K.; Zengin, G.; Khan, F.; Kumar, A.; Kaur, R.; Venkatachalam, T.; Tit, D.M.; Vesa, C.M.; et al. Pleotropic Effects of Polyphenols in Cardiovascular System. Biomed. Pharmacother. 2020, 130, 110714. [Google Scholar] [CrossRef]
- Staessen, J.A.; Wang, J.; Bianchi, G.; Birkenhäger, W.H. Essential Hypertension. Lancet 2003, 361, 1629–1641. [Google Scholar] [CrossRef]
- Diaconu, C.C.; Dediu, G.N.; Iancu, M.A. Drug-Induced Arterial Hypertension—A Frequently Ignored Cause of Secondary Hypertension: A Review. Acta Cardiol. 2018, 73, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Foy, M.C.; Vaishnav, J.; Sperati, C.J. Drug-Induced Hypertension. Endocrinol. Metab. Clin. N. Am. 2019, 48, 859–873. [Google Scholar] [CrossRef] [PubMed]
- Ladd, A.M.; Panagopoulos, G.; Cohen, J.; Mar, N.; Graham, R. Potential Costs of Inappropriate Use of Proton Pump Inhibitors. Am. J. Med. Sci. 2014, 347, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, D.; Behrens, G.; Himmel, W.; Kochen, M.M.; Chenot, J.-F. Appropriateness of Proton Pump Inhibitor Recommendations at Hospital Discharge and Continuation in Primary Care. Int. J. Clin. Pract. 2012, 66, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Parente, F.; Cucino, C.; Gallus, S.; Bargiggia, S.; Greco, S.; Pastore, L.; Bianchi Porro, G. Hospital Use of Acid-Suppressive Medications and Its Fall-out on Prescribing in General Practice: A 1-Month Survey. Aliment. Pharmacol. Ther. 2003, 17, 1503–1506. [Google Scholar] [CrossRef]
- Heidelbaugh, J.J.; Metz, D.C.; Yang, Y.-X. Proton Pump Inhibitors: Are They Overutilised in Clinical Practice and Do They Pose Significant Risk? Int. J. Clin. Pract. 2012, 66, 582–591. [Google Scholar] [CrossRef]
- Savarino, V.; Dulbecco, P.; de Bortoli, N.; Ottonello, A.; Savarino, E. The Appropriate Use of Proton Pump Inhibitors (PPIs): Need for a Reappraisal. Eur. J. Intern. Med. 2017, 37, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Othman, F.; Card, T.R.; Crooks, C.J. Proton Pump Inhibitor Prescribing Patterns in the UK: A Primary Care Database Study. Pharmacoepidemiol. Drug Saf. 2016, 25, 1079–1087. [Google Scholar] [CrossRef]
- Barron, J.J.; Tan, H.; Spalding, J.; Bakst, A.W.; Singer, J. Proton Pump Inhibitor Utilization Patterns in Infants. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 421–427. [Google Scholar] [CrossRef]
- Pottegård, A.; Broe, A.; Hallas, J.; de Muckadell, O.B.S.; Lassen, A.T.; Lødrup, A.B. Use of Proton-Pump Inhibitors among Adults: A Danish Nationwide Drug Utilization Study. Ther. Adv. Gastroenterol. 2016, 9, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Aznar-Lou, I.; Reilev, M.; Lødrup, A.B.; Rubio-Valera, M.; Haastrup, P.F.; Pottegård, A. Use of Proton Pump Inhibitors among Danish Children: A 16-Year Register-Based Nationwide Study. Basic Clin. Pharmacol. Toxicol. 2019, 124, 704–710. [Google Scholar] [CrossRef]
- Mazer-Amirshahi, M.; Mullins, P.M.; van den Anker, J.; Meltzer, A.; Pines, J.M. Rising Rates of Proton Pump Inhibitor Prescribing in US Emergency Departments. Am. J. Emerg. Med. 2014, 32, 618–622. [Google Scholar] [CrossRef]
- Torres-Bondia, F.; de Batlle, J.; Galván, L.; Buti, M.; Barbé, F.; Piñol-Ripoll, G. Evolution of the Consumption Trend of Proton Pump Inhibitors in the Lleida Health Region between 2002 and 2015. BMC Public Health 2022, 22, 818. [Google Scholar] [CrossRef]
- Luo, H.; Fan, Q.; Xiao, S.; Chen, K. Changes in Proton Pump Inhibitor Prescribing Trend over the Past Decade and Pharmacists’ Effect on Prescribing Practice at a Tertiary Hospital. BMC Health Serv. Res. 2018, 18, 537. [Google Scholar] [CrossRef] [PubMed]
- Muheim, L.; Signorell, A.; Markun, S.; Chmiel, C.; Neuner-Jehle, S.; Blozik, E.; Ursprung, P.; Rosemann, T.; Senn, O. Potentially Inappropriate Proton-Pump Inhibitor Prescription in the General Population: A Claims-Based Retrospective Time Trend Analysis. Ther. Adv. Gastroenterol. 2021, 14, 1756284821998928. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.D.; Ahmad, A. A Retrospective Study on Prescribing Pattern and Cost Analysis of Proton-Pump Inhibitors Used among Adults of Saudi Arabia. J. Pharm. Health Serv. Res. 2020, 11, 343–347. [Google Scholar] [CrossRef]
- Yibirin, M.; De Oliveira, D.; Valera, R.; Plitt, A.E.; Lutgen, S. Adverse Effects Associated with Proton Pump Inhibitor Use. Cureus 2021, 13, e12759. [Google Scholar] [CrossRef]
- Savarino, V.; Dulbecco, P.; Savarino, E. Are Proton Pump Inhibitors Really so Dangerous? Dig. Liver Dis. 2016, 48, 851–859. [Google Scholar] [CrossRef]
- Thong, B.K.S.; Ima-Nirwana, S.; Chin, K.-Y. Proton Pump Inhibitors and Fracture Risk: A Review of Current Evidence and Mechanisms Involved. Int. J. Environ. Res. Public Health 2019, 16, 1571. [Google Scholar] [CrossRef]
- Heidelbaugh, J.J. Proton Pump Inhibitors and Risk of Vitamin and Mineral Deficiency: Evidence and Clinical Implications. Ther. Adv. Drug Saf. 2013, 4, 125–133. [Google Scholar] [CrossRef]
- Jaynes, M.; Kumar, A.B. The Risks of Long-Term Use of Proton Pump Inhibitors: A Critical Review. Ther. Adv. Drug Saf. 2018, 10, 2042098618809927. [Google Scholar] [CrossRef]
- Casula, M.; Scotti, L.; Galimberti, F.; Mozzanica, F.; Tragni, E.; Corrao, G.; Catapano, A.L. Use of Proton Pump Inhibitors and Risk of Ischemic Events in the General Population. Atherosclerosis 2018, 277, 123–129. [Google Scholar] [CrossRef]
- Sehested, T.S.G.; Gerds, T.A.; Fosbøl, E.L.; Hansen, P.W.; Charlot, M.G.; Carlson, N.; Hlatky, M.A.; Torp-Pedersen, C.; Gislason, G.H. Long-Term Use of Proton Pump Inhibitors, Dose-Response Relationship and Associated Risk of Ischemic Stroke and Myocardial Infarction. J. Intern. Med. 2018, 283, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Cui, Z.; Zhou, M.; Li, R.; Li, H.; Zhang, S.; Ba, Y.; Cheng, G. Proton Pump Inhibitor Monotherapy and the Risk of Cardiovascular Events in Patients with Gastro-Esophageal Reflux Disease: A Meta-Analysis. Neurogastroenterol. Motil. 2017, 29, e12926. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Ye, X.; Hu, F.; Xu, J.; Guo, X.; Lin, Z.; Zhou, X.; Guo, Z.; Cao, Y.; He, J. Updated Insights on Cardiac and Vascular Risks of Proton Pump Inhibitors: A Real-World Pharmacovigilance Study. Front. Cardiovasc. Med. 2022, 9, 767987. [Google Scholar] [CrossRef] [PubMed]
- Hermann, M.; Flammer, A.; Lüscher, T.F. Nitric Oxide in Hypertension. J. Clin. Hypertens. 2006, 8, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Trimm, E.; Red-Horse, K. Vascular Endothelial Cell Development and Diversity. Nat. Rev. Cardiol. 2023, 20, 197–210. [Google Scholar] [CrossRef]
- Chen, K.; Pittman, R.N.; Popel, A.S. Nitric Oxide in the Vasculature: Where Does It Come From and Where Does It Go? A Quantitative Perspective. Antioxid. Redox Signal 2008, 10, 1185–1198. [Google Scholar] [CrossRef]
- Förstermann, U.; Sessa, W.C. Nitric Oxide Synthases: Regulation and Function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef]
- Tousoulis, D.; Kampoli, A.-M.; Tentolouris, C.; Papageorgiou, N.; Stefanadis, C. The Role of Nitric Oxide on Endothelial Function. Curr. Vasc. Pharmacol. 2012, 10, 4–18. [Google Scholar] [CrossRef]
- Böger, R.H. Association of Asymmetric Dimethylarginine and Endothelial Dysfunction. Clin. Chem. Lab. Med. 2003, 41, 1467–1472. [Google Scholar] [CrossRef] [PubMed]
- Cooke, J.P.; Ghebremariam, Y.T. DDAH Says NO to ADMA. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 1462–1464. [Google Scholar] [CrossRef] [PubMed]
- Dayoub, H.; Achan, V.; Adimoolam, S.; Jacobi, J.; Stuehlinger, M.C.; Wang, B.; Tsao, P.S.; Kimoto, M.; Vallance, P.; Patterson, A.J.; et al. Dimethylarginine Dimethylaminohydrolase Regulates Nitric Oxide Synthesis: Genetic and Physiological Evidence. Circulation 2003, 108, 3042–3047. [Google Scholar] [CrossRef]
- Nolde, M.; Bahls, M.; Friedrich, N.; Dörr, M.; Dreischulte, T.; Felix, S.B.; Rückert-Eheberg, I.-M.; Ahn, N.; Amann, U.; Schwedhelm, E.; et al. Association of Proton Pump Inhibitor Use with Endothelial Function and Metabolites of the Nitric Oxide Pathway: A Cross-Sectional Study. Pharmacotherapy 2021, 41, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Ghebremariam, Y.T.; LePendu, P.; Lee, J.C.; Erlanson, D.A.; Slaviero, A.; Shah, N.H.; Leiper, J.; Cooke, J.P. Unexpected Effect of Proton Pump Inhibitors: Elevation of the Cardiovascular Risk Factor Asymmetric Dimethylarginine. Circulation 2013, 128, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Tommasi, S.; Elliot, D.J.; Hulin, J.A.; Lewis, B.C.; McEvoy, M.; Mangoni, A.A. Human Dimethylarginine Dimethylaminohydrolase 1 Inhibition by Proton Pump Inhibitors and the Cardiovascular Risk Marker Asymmetric Dimethylarginine: In Vitro and in Vivo Significance. Sci. Rep. 2017, 7, 2871. [Google Scholar] [CrossRef] [PubMed]
- Böger, R.H. The Emerging Role of Asymmetric Dimethylarginine as a Novel Cardiovascular Risk Factor. Cardiovasc. Res. 2003, 59, 824–833. [Google Scholar] [CrossRef]
- Gallo, G.; Volpe, M.; Savoia, C. Endothelial Dysfunction in Hypertension: Current Concepts and Clinical Implications. Front. Med. 2022, 8, 798958. [Google Scholar] [CrossRef]
- Yepuri, G.; Sukhovershin, R.; Nazari-Shafti, T.Z.; Petrascheck, M.; Ghebre, Y.T.; Cooke, J.P. Proton Pump Inhibitors Accelerate Endothelial Senescence. Circ. Res. 2016, 118, e36–e42. [Google Scholar] [CrossRef]
- Lundberg, J.O.; Weitzberg, E.; Gladwin, M.T. The Nitrate-Nitrite-Nitric Oxide Pathway in Physiology and Therapeutics. Nat. Rev. Drug Discov. 2008, 7, 156–167. [Google Scholar] [CrossRef]
- Oliveira-Paula, G.H.; Tanus-Santos, J.E. Nitrite-Stimulated Gastric Formation of S-Nitrosothiols As An Antihypertensive Therapeutic Strategy. Curr. Drug Targets 2019, 20, 431–443. [Google Scholar] [CrossRef]
- Pinheiro, L.C.; Amaral, J.H.; Ferreira, G.C.; Portella, R.L.; Ceron, C.S.; Montenegro, M.F.; Toledo, J.C.; Tanus-Santos, J.E. Gastric S-Nitrosothiol Formation Drives the Antihypertensive Effects of Oral Sodium Nitrite and Nitrate in a Rat Model of Renovascular Hypertension. Free Radic. Biol. Med. 2015, 87, 252–262. [Google Scholar] [CrossRef]
- Sanches-Lopes, J.M.; Ferreira, G.C.; Pinheiro, L.C.; Kemp, R.; Tanus-Santos, J.E. Consistent Gastric PH-Dependent Effects of Suppressors of Gastric Acid Secretion on the Antihypertensive Responses to Oral Nitrite. Biochem. Pharmacol. 2020, 177, 113940. [Google Scholar] [CrossRef]
- Amaral, J.H.; Montenegro, M.F.; Pinheiro, L.C.; Ferreira, G.C.; Barroso, R.P.; Costa-Filho, A.J.; Tanus-Santos, J.E. TEMPOL Enhances the Antihypertensive Effects of Sodium Nitrite by Mechanisms Facilitating Nitrite-Derived Gastric Nitric Oxide Formation. Free Radic. Biol. Med. 2013, 65, 446–455. [Google Scholar] [CrossRef]
- Pinheiro, L.C.; Montenegro, M.F.; Amaral, J.H.; Ferreira, G.C.; Oliveira, A.M.; Tanus-Santos, J.E. Increase in Gastric PH Reduces Hypotensive Effect of Oral Sodium Nitrite in Rats. Free Radic. Biol. Med. 2012, 53, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Stover, P.J. Vitamin B12 and Older Adults. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.R.; Schneider, J.L.; Zhao, W.; Corley, D.A. Proton Pump Inhibitor and Histamine 2 Receptor Antagonist Use and Vitamin B12 Deficiency. JAMA 2013, 310, 2435–2442. [Google Scholar] [CrossRef] [PubMed]
- Kachhawa, K.; Kumar, A.M. Homocysteine as an Independent and Dependent Causative Factor of Cardio Vascular Diseases. IJFANS Int. J. Food Nutr. Sci. 2022, 11, 859–869. [Google Scholar]
- Miller, J.W. Proton Pump Inhibitors, H2-Receptor Antagonists, Metformin, and Vitamin B-12 Deficiency: Clinical Implications. Adv. Nutr. 2018, 9, 511S–518S. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.M.; Hoey, L.; Hughes, C.F.; Ward, M.; Clements, M.; Strain, J.; Cunningham, C.; Casey, M.C.; Tracey, F.; O’Kane, M.; et al. Associations of Atrophic Gastritis and Proton-Pump Inhibitor Drug Use with Vitamin B-12 Status, and the Impact of Fortified Foods, in Older Adults. Am. J. Clin. Nutr. 2021, 114, 1286–1294. [Google Scholar] [CrossRef]
- Swarnakari, K.M.; Bai, M.; Manoharan, M.P.; Raja, R.; Jamil, A.; Csendes, D.; Gutlapalli, S.D.; Prakash, K.; Desai, D.M.; Desai, A.; et al. The Effects of Proton Pump Inhibitors in Acid Hypersecretion-Induced Vitamin B12 Deficiency: A Systematic Review (2022). Cureus 2022, 14, e31672. [Google Scholar] [CrossRef]
- Kanyal Butola, L.; Kute, P.; Anjankar, A.; Dhok, A.; Gusain, N.; Vagga, A. Vitamin B12 -Do You Know Everything? J. Evol. Med. Dent. Sci. 2020, 9, 3139–3146. [Google Scholar] [CrossRef]
- Ganguly, P.; Alam, S.F. Role of Homocysteine in the Development of Cardiovascular Disease. Nutr. J. 2015, 14, 6. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, L.; Miao, Y.; Yang, J.; Wang, X.; Wang, C.; Feng, J.; Wang, L. Homocysteine Causes Vascular Endothelial Dysfunction by Disrupting Endoplasmic Reticulum Redox Homeostasis. Redox Biol. 2019, 20, 46–59. [Google Scholar] [CrossRef] [PubMed]
- Lentz, S.R.; Rodionov, R.N.; Dayal, S. Hyperhomocysteinemia, Endothelial Dysfunction, and Cardiovascular Risk: The Potential Role of ADMA. Atheroscler. Suppl. 2003, 4, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N. Mechanisms of Increased Vascular Oxidant Stress in Hyperhomocys-Teinemia and Its Impact on Endothelial Function. Curr. Drug Metab. 2005, 6, 27–36. [Google Scholar] [CrossRef]
- Baszczuk, A.; Kopczyński, Z.; Thielemann, A. Endothelial dysfunction in patients with primary hypertension and hyperhomocysteinemia. Adv. Hyg. Exp. Med. 2014, 68, 91–100. [Google Scholar] [CrossRef]
- Weiss, N.; Heydrick, S.J.; Postea, O.; Keller, C.; Keaney, J.F.; Loscalzo, J. Influence of Hyperhomocysteinemia on the Cellular Redox State--Impact on Homocysteine-Induced Endothelial Dysfunction. Clin. Chem. Lab. Med. 2003, 41, 1455–1461. [Google Scholar] [CrossRef]
- Austin, R.C.; Lentz, S.R.; Werstuck, G.H. Role of Hyperhomocysteinemia in Endothelial Dysfunction and Atherothrombotic Disease. Cell Death Differ. 2004, 11 (Suppl. S1), S56–S64. [Google Scholar] [CrossRef]
- Rodrigo, R.; Passalacqua, W.; Araya, J.; Orellana, M.; Rivera, G. Homocysteine and Essential Hypertension. J. Clin. Pharmacol. 2003, 43, 1299–1306. [Google Scholar] [CrossRef]
- Aboukhater, D.; Morad, B.; Nasrallah, N.; Nasser, S.A.; Sahebkar, A.; Kobeissy, F.; Boudaka, A.; Eid, A.H. Inflammation and Hypertension: Underlying Mechanisms and Emerging Understandings. J. Cell. Physiol. 2023, 238, 1148–1159. [Google Scholar] [CrossRef]
- Tahir, R.; Patel, P.N. Role of Proton Pump Inhibitors in Calcium Absorption, Bone Resorption, and Risk of Hip Fracture. J. Pharm. Technol. 2007, 23, 275–280. [Google Scholar] [CrossRef]
- Insogna, K.L. The Effect of Proton Pump-Inhibiting Drugs on Mineral Metabolism. Am. J. Gastroenterol. 2009, 104 (Suppl. S2), S2–S4. [Google Scholar] [CrossRef]
- Ito, T.; Jensen, R.T. Association of Long-Term Proton Pump Inhibitor Therapy with Bone Fractures and Effects on Absorption of Calcium, Vitamin B12, Iron, and Magnesium. Curr. Gastroenterol. Rep. 2010, 12, 448–457. [Google Scholar] [CrossRef]
- Sipponen, P.; Härkönen, M. Hypochlorhydric Stomach: A Risk Condition for Calcium Malabsorption and Osteoporosis? Scand. J. Gastroenterol. 2010, 45, 133–138. [Google Scholar] [CrossRef]
- Chonan, O.; Takahashi, R.; Yasui, H.; Watanuki, M. Effect of L-Lactic Acid on Calcium Absorption in Rats Fed Omeprazole. J. Nutr. Sci. Vitaminol. 1998, 44, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Matuszewska, A.; Nowak, B.; Rzeszutko, M.; Zduniak, K.; Szandruk, M.; Jędrzejuk, D.; Landwójtowicz, M.; Bolanowski, M.; Pieśniewska, M.; Kwiatkowska, J.; et al. Effects of Long-Term Administration of Pantoprazole on Bone Mineral Density in Young Male Rats. Pharmacol. Rep. 2016, 68, 1060–1064. [Google Scholar] [CrossRef]
- Memon, R.A.; Memon, F.R.; Memon, A.R.; Memon, J.U.Q.; Laghari, J.H.; Shams, S.; Memon, A.R. Effects of Proton Pump Inhibitors on Serum Calcium Level: A Study on Rabbit Model. J. Pharm. Res. Int. 2021, 33, 361–366. [Google Scholar] [CrossRef]
- O’Connell, M.B.; Madden, D.M.; Murray, A.M.; Heaney, R.P.; Kerzner, L.J. Effects of Proton Pump Inhibitors on Calcium Carbonate Absorption in Women: A Randomized Crossover Trial. Am. J. Med. 2005, 118, 778–781. [Google Scholar] [CrossRef] [PubMed]
- Graziani, G.; Como, G.; Badalamenti, S.; Finazzi, S.; Malesci, A.; Gallieni, M.; Brancaccio, D.; Ponticelli, C. Effect of Gastric Acid Secretion on Intestinal Phosphate and Calcium Absorption in Normal Subjects. Nephrol. Dial. Transplant. 1995, 10, 1376–1380. [Google Scholar] [PubMed]
- Chawla, B.K.; Cohen, R.E.; Yerke, L.M. Association between Proton Pump Inhibitors and Periodontal Disease Severity. Clin. Exp. Dent. Res. 2022, 8, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Cheteu Wabo, T.M.; Wu, X.; Sun, C.; Boah, M.; Ngo Nkondjock, V.R.; Kosgey Cheruiyot, J.; Amporfro Adjei, D.; Shah, I. Association of Dietary Calcium, Magnesium, Sodium, and Potassium Intake and Hypertension: A Study on an 8-Year Dietary Intake Data from the National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2022, 16, 74–93. [Google Scholar] [CrossRef]
- Gul, S.; Shaikh, S.N.; Rani, K.; Shaikh, K. Correlation of Serum Calcium Level with Hypertension. Pak. J. Med. Health Sci. 2021, 15, 608–610. [Google Scholar]
- Jorde, R.; Sundsfjord, J.; Haug, E.; Bønaa, K.H. Relation Between Low Calcium Intake, Parathyroid Hormone, and Blood Pressure. Hypertension 2000, 35, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-H.; Bu, S.Y.; Choi, M.-K. Daily Calcium Intake and Its Relation to Blood Pressure, Blood Lipids, and Oxidative Stress Biomarkers in Hypertensive and Normotensive Subjects. Nutr. Res. Pract. 2012, 6, 421–428. [Google Scholar] [CrossRef]
- Centeno, V.; de Barboza, G.D.; Marchionatti, A.; Rodríguez, V.; Tolosa de Talamoni, N. Molecular Mechanisms Triggered by Low-Calcium Diets. Nutr. Res. Rev. 2009, 22, 163–174. [Google Scholar] [CrossRef]
- Villa-Etchegoyen, C.; Lombarte, M.; Matamoros, N.; Belizán, J.M.; Cormick, G. Mechanisms Involved in the Relationship between Low Calcium Intake and High Blood Pressure. Nutrients 2019, 11, 1112. [Google Scholar] [CrossRef]
- Toh, J.W.T.; Ong, E.; Wilson, R. Hypomagnesaemia Associated with Long-Term Use of Proton Pump Inhibitors. Gastroenterol. Rep. 2015, 3, 243–253. [Google Scholar] [CrossRef]
- Mackay, J.D.; Bladon, P.T. Hypomagnesaemia Due to Proton-Pump Inhibitor Therapy: A Clinical Case Series. QJM 2010, 103, 387–395. [Google Scholar] [CrossRef]
- Nakamura, N.; Yoneda, K.; Higo, T.; Kusumoto, M. Monitoring of Serum Magnesium Levels during Long-Term Use of Proton Pump Inhibitors in Elderly Japanese Patients: Is It Really Necessary or Not? J. Pharm. Health Care Sci. 2022, 8, 35. [Google Scholar] [CrossRef]
- Cundy, T.; Mackay, J. Proton Pump Inhibitors and Severe Hypomagnesaemia. Curr. Opin. Gastroenterol. 2011, 27, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Cundy, T.; Dissanayake, A. Severe Hypomagnesaemia in Long-Term Users of Proton-Pump Inhibitors. Clin. Endocrinol. 2008, 69, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Semb, S.; Helgstrand, F.; Hjørne, F.; Bytzer, P. Persistent Severe Hypomagnesemia Caused by Proton Pump Inhibitor Resolved after Laparoscopic Fundoplication. World J. Gastroenterol. 2017, 23, 6907–6910. [Google Scholar] [CrossRef] [PubMed]
- Mk, C.; Yj, B. Association of Magnesium Intake with High Blood Pressure in Korean Adults: Korea National Health and Nutrition Examination Survey 2007–2009. PLoS ONE 2015, 10, e0130405. [Google Scholar] [CrossRef]
- Rodríguez-Ramírez, M.; Simental-Mendía, L.E.; González-Ortiz, M.; Martínez-Abundis, E.; Madero, A.; Brito-Zurita, O.; Pérez-Fuentes, R.; Revilla-Monsalve, C.; Islas-Andrade, S.; Rodríguez-Morán, M.; et al. Prevalence of Prehypertension in Mexico and Its Association With Hypomagnesemia. Am. J. Hypertens. 2015, 28, 1024–1030. [Google Scholar] [CrossRef]
- Cunha, A.R.; Umbelino, B.; Correia, M.L.; Neves, M.F. Magnesium and Vascular Changes in Hypertension. Int. J. Hypertens. 2012, 2012, 754250. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Barbagallo, M. Magnesium and Hypertension in Old Age. Nutrients 2020, 13, 139. [Google Scholar] [CrossRef]
- Oost, L.J.; Tack, C.J.; de Baaij, J.H.F. Hypomagnesemia and Cardiovascular Risk in Type 2 Diabetes. Endocr. Rev. 2023, 44, 357–378. [Google Scholar] [CrossRef]
- Oparil, S.; Acelajado, M.C.; Bakris, G.L.; Berlowitz, D.R.; Cífková, R.; Dominiczak, A.F.; Grassi, G.; Jordan, J.; Poulter, N.R.; Rodgers, A.; et al. Hypertension. Nat. Rev. Dis. Primers 2018, 4, 18014. [Google Scholar] [CrossRef]
- Grossman, E.; Messerli, F.H. Drug-Induced Hypertension: An Unappreciated Cause of Secondary Hypertension. Am. J. Med. 2012, 125, 14–22. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Study Type | Population | Country | Time Period | Inference | Reference |
|---|---|---|---|---|---|
| Cohort analysis | Population of age more than 18 years | UK | 1990–2014 | PPI prevalence increased up to 15%, in which 26% used PPI long term and 3.9% used it for 5 years. | [18] |
| Retrospective observational study | Infants of age less than 1 year | United States of America | 1999–2004 | PPI usage increases four times in infants; lansoprazole and omeprazole are used mainly. | [19] |
| Prescription analysis | Adults aged between 5 and 15 with a median age 12 | Denmark | 2000–2014 | PPI use raised to 4 times | [20] |
| Prescription analysis | Children of Denmark aged between 0–17 years | Denmark | 2000–2015 | A total of 8 times increment in the dispensing rate of PPI in Danish children’s prescriptions, and omeprazole is the most frequently used PPI | [21] |
| Retrospective analysis | Patients of the emergency department aged more than 65 | United States of America | 2001–2010 | Increase in prescription rate from 3% to 7.2%, with pantoprazole being the most utilized. | [22] |
| Prescription analysis | Individuals of any age group with a mean age 62 | Spain | 2002–2015 | Increase in the global dispensing of PPIs from 12.5% in 2002 to 18.1% in 2015. Omeprazole is the most prescribed PPI in this period, and the most frequent age group was above 65 | [23] |
| Retrospective study | Population of age between 18 and 80 | China | 2007–2016 | Prescription rate in inpatient increased from 20.41% to 37.21%. | [24] |
| Retrospective study | Population of age 18 or older with mean age 51.2 | Switzerland | 2012–2017 | Inappropriate PPI prescription increased from 4.8% to 6.4%, and the annual incidence of PPI also rose to 4% | [25] |
| Cross-sectional retrospective study | Adult population of age 30–40 years | Saudi Arabia | 2019 | Increase in the use of PPI, with pantoprazole being the most prescribed | [26] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tayal, R.; Yasmin, S.; Chauhan, S.; Singh, T.G.; Saini, M.; Shorog, E.; Althubyani, M.M.; Alsaadi, B.H.; Aljohani, F.; Alenazi, M.A.; et al. Are Proton Pump Inhibitors Contributing in Emerging New Hypertensive Population? Pharmaceuticals 2023, 16, 1387. https://doi.org/10.3390/ph16101387
Tayal R, Yasmin S, Chauhan S, Singh TG, Saini M, Shorog E, Althubyani MM, Alsaadi BH, Aljohani F, Alenazi MA, et al. Are Proton Pump Inhibitors Contributing in Emerging New Hypertensive Population? Pharmaceuticals. 2023; 16(10):1387. https://doi.org/10.3390/ph16101387
Chicago/Turabian StyleTayal, Rohit, Sabina Yasmin, Samrat Chauhan, Thakur Gurjeet Singh, Monika Saini, Eman Shorog, Maryam M. Althubyani, Baiaan H. Alsaadi, Fatimah Aljohani, Maram A. Alenazi, and et al. 2023. "Are Proton Pump Inhibitors Contributing in Emerging New Hypertensive Population?" Pharmaceuticals 16, no. 10: 1387. https://doi.org/10.3390/ph16101387