
Evaluating the Safety of Herbal Medicine on Renal Function: A Comprehensive Analysis from Six Randomized Controlled Trials Conducted with Four Formulations from Traditional Korean Medicine


Abstract
:1. Introduction
2. Results
2.1. Participants Characteristics
2.2. Changes in BUN, Serum Creatinine, and eGFR
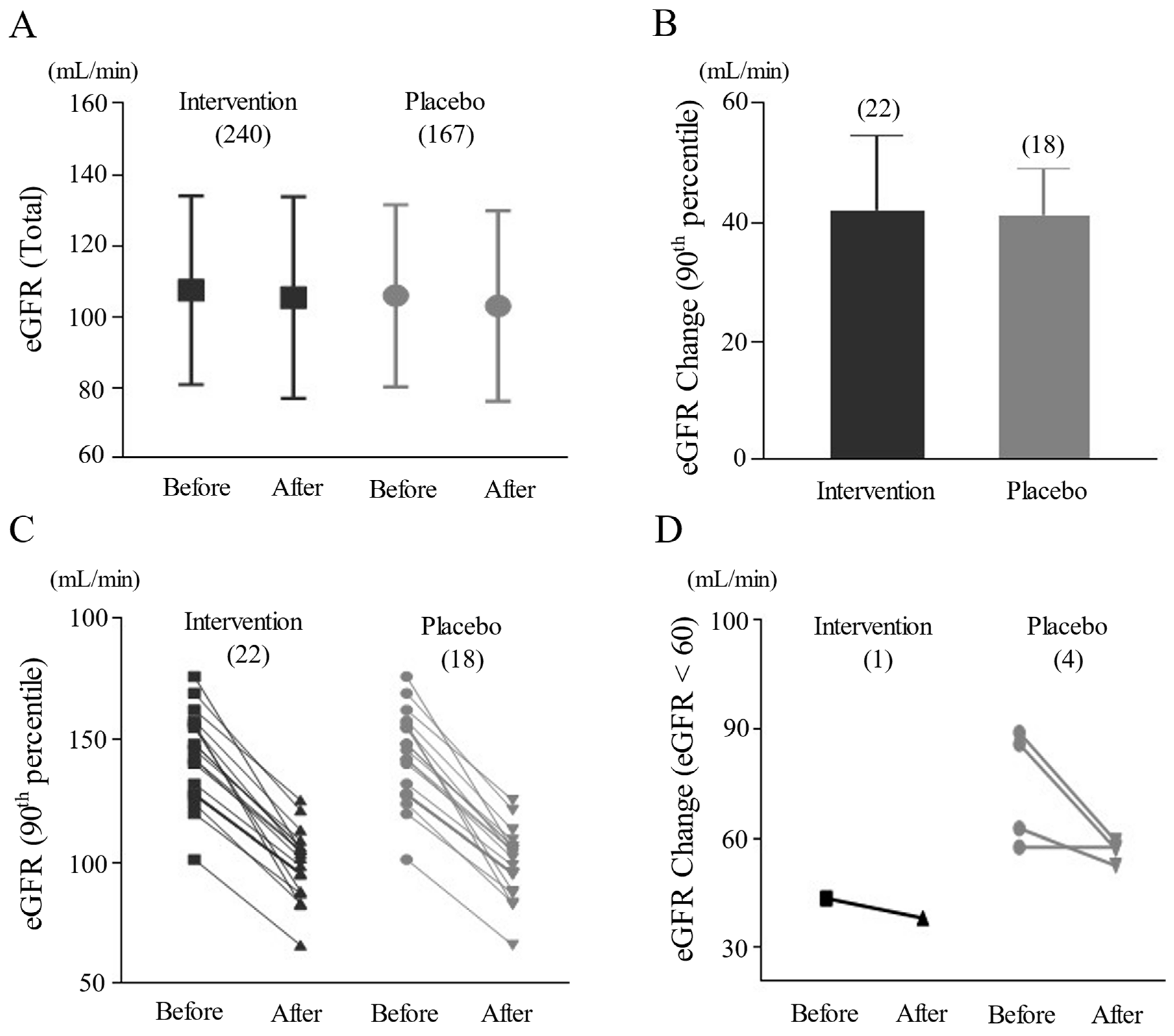
2.3. Change in eGFR in 90th-Percentile and Frequency of Notable Reduction
3. Discussion
4. Materials and Methods
4.1. Study Design and Ethics Approval
4.2. Preparation of Herbal Prescription and Placebos
4.3. Participants Criteria
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Touiti, N.; Houssaini, T.S.; Achour, S. Overview on Pharmacovigilance of Nephrotoxic Herbal Medicines Used Worldwide. Clin. Phytosci. 2021, 7, 9. [Google Scholar] [CrossRef]
- Kim, J.; Jang, W. Safety of Prescribed Herbal Medicines for Hepatic and Renal Function of Polypharmacy Patients with Stroke: A Single-Center Retrospective Study. Medicine 2022, 101, e32147. [Google Scholar] [CrossRef]
- Lee, J.; Shin, J.-S.; Kim, M.-R.; Byun, J.-H.; Lee, S.-Y.; Shin, Y.-S.; Kim, H.; Byung Park, K.; Shin, B.-C.; Lee, M.S.; et al. Liver Enzyme Abnormalities in Taking Traditional Herbal Medicine in Korea: A Retrospective Large Sample Cohort Study of Musculoskeletal Disorder Patients. J. Ethnopharmacol. 2015, 169, 407–412. [Google Scholar] [CrossRef]
- Santos, G.; Gasca, J.; Parana, R.; Nunes, V.; Schinnoni, M.; Medina-Caliz, I.; Cabello, M.R.; Lucena, M.I.; Andrade, R.J. Profile of Herbal and Dietary Supplements Induced Liver Injury in Latin America: A Systematic Review of Published Reports. Phytother. Res. 2021, 35, 6–19. [Google Scholar] [CrossRef]
- Patel-Rodrigues, P.A.; Cundra, L.; Alhaqqan, D.; Gildea, D.T.; Woo, S.M.; Lewis, J.H. Herbal- and Dietary-Supplement-Induced Liver Injury: A Review of the Recent Literature. Livers 2024, 4, 94–118. [Google Scholar] [CrossRef]
- Cho, J.-H.; Oh, D.-S.; Hong, S.-H.; Ko, H.; Lee, N.-H.; Park, S.-E.; Han, C.-W.; Kim, S.-M.; Kim, Y.-C.; Kim, K.-S.; et al. A Nationwide Study of the Incidence Rate of Herb-Induced Liver Injury in Korea. Arch. Toxicol. 2017, 91, 4009–4015. [Google Scholar] [CrossRef]
- Pazhayattil, G.S.; Shirali, A.C. Drug-Induced Impairment of Renal Function. Int. J. Nephrol. Renov. Dis. 2014, 7, 457–468. [Google Scholar] [CrossRef]
- Xu, X.; Zhu, R.; Ying, J.; Zhao, M.; Wu, X.; Cao, G.; Wang, K. Nephrotoxicity of Herbal Medicine and Its Prevention. Front. Pharmacol. 2020, 11, 569551. [Google Scholar] [CrossRef]
- Yang, B.; Xie, Y.; Guo, M.; Rosner, M.H.; Yang, H.; Ronco, C. Nephrotoxicity and Chinese Herbal Medicine. Clin. J. Am. Soc. Nephrol. 2018, 13, 1605–1611. [Google Scholar] [CrossRef]
- Barnes, J.; Anderson, L.A.; Gibbons, S.; Phillipson, J.D. Echinacea Species (Echinacea Angustifolia (DC.) Hell., Echinacea Pallida (Nutt.) Nutt.,Echinacea Purpurea (L.) Moench): A Review of Their Chemistry, Pharmacology and Clinical Properties. J. Pharm. Pharmacol. 2005, 57, 929–954. [Google Scholar] [CrossRef]
- Canenguez Benitez, J.S.; Hernandez, T.E.; Sundararajan, R.; Sarwar, S.; Arriaga, A.J.; Khan, A.T.; Matayoshi, A.; Quintanilla, H.A.; Kochhar, H.; Alam, M.; et al. Advantages and Disadvantages of Using St. John’s Wort as a Treatment for Depression. Cureus 2022, 14, e29468. [Google Scholar] [CrossRef]
- Adibelli, Z.; Karacay, I.; Demir, M.; Duran, C.S. John’s Wort (Hypericum Perforatum)-Related Acute Kidney Injury. Blood Purif. 2022, 51, 520–522. [Google Scholar] [CrossRef]
- Rezaie, A.; Fazlara, A.; Haghi Karamolah, M.; Shahriari, A.; Najaf Zadeh, H.; Pashmforosh, M. Effects of Echinacea Purpurea on Hepatic and Renal Toxicity Induced by Diethylnitrosamine in Rats. Jundishapur J. Nat. Pharm. Prod. 2013, 8, 60–64. [Google Scholar] [CrossRef]
- Kovesdy, C.P. Epidemiology of Chronic Kidney Disease: An Update 2022. Kidney Int. Suppl. (2011) 2022, 12, 7–11. [Google Scholar] [CrossRef]
- Zhang, S.; Ren, H.-F.; Du, R.-X.; Sun, W.-L.; Fu, M.-L.; Zhang, X.-C. Global, Regional, and National Burden of Kidney Dysfunction from 1990 to 2019: A Systematic Analysis from the Global Burden of Disease Study 2019. BMC Public Health 2023, 23, 1218. [Google Scholar] [CrossRef]
- Sidorenkov, G.; Navis, G. Safety of ACE Inhibitor Therapies in Patients with Chronic Kidney Disease. Expert. Opin. Drug Saf. 2014, 13, 1383–1395. [Google Scholar] [CrossRef]
- Zhao, J.; Sun, W.; Chen, J.; Sun, Z.; Chen, D.; Cao, C.; Yang, M.; Ma, J.; Wang, L.; Xing, C.; et al. Efficacy and Safety of Chinese Herbal Formula Granules in Treating Chronic Kidney Disease Stage 3: A Multicenter, Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Evid. Based Complement. Altern. Med. 2020, 2020, 4073901. [Google Scholar] [CrossRef]
- Liu, X.; Chen, J.; Liu, X.; Wang, D.; Zheng, P.; Qi, A.; Yi, T.; Li, S. Jian-Pi-Yi-Shen Formula Ameliorates Chronic Kidney Disease: Involvement of Mitochondrial Quality Control Network. BMC Complement. Altern. Med. 2018, 18, 340. [Google Scholar] [CrossRef]
- Li, H.-D.; Meng, X.-M.; Huang, C.; Zhang, L.; Lv, X.-W.; Li, J. Application of Herbal Traditional Chinese Medicine in the Treatment of Acute Kidney Injury. Front. Pharmacol. 2019, 10, 376. [Google Scholar] [CrossRef]
- Byard, R.W.; Musgrave, I.; Maker, G.; Bunce, M. What Risks Do Herbal Products Pose to the Australian Community? Med. J. Aust. 2017, 206, 86–90. [Google Scholar] [CrossRef]
- Cai, P.; Qiu, H.; Qi, F.; Zhang, X. The Toxicity and Safety of Traditional Chinese Medicines: Please Treat with Rationality. Biosci. Trends 2019, 13, 367–373. [Google Scholar] [CrossRef]
- Jang, S.; Kim, K.H.; Sun, S.-H.; Go, H.-Y.; Lee, E.-K.; Jang, B.-H.; Shin, Y.-C.; Ko, S.-G. Characteristics of Herbal Medicine Users and Adverse Events Experienced in South Korea: A Survey Study. Evid. Based Complement. Altern. Med. 2017, 2017, 4089019. [Google Scholar] [CrossRef]
- Pereira, M.; Rodrigues, N.; Godinho, I.; Gameiro, J.; Neves, M.; Gouveia, J.; Costa E Silva, Z.; Lopes, J.A. Acute Kidney Injury in Patients with Severe Sepsis or Septic Shock: A Comparison between the “Risk, Injury, Failure, Loss of Kidney Function, End-Stage Kidney Disease” (RIFLE), Acute Kidney Injury Network (AKIN) and Kidney Disease: Improving Global Outcomes (KDIGO) Classifications. Clin. Kidney J. 2017, 10, 332–340. [Google Scholar] [CrossRef]
- Joung, J.-Y.; Lee, J.-S.; Cho, J.-H.; Lee, D.-S.; Ahn, Y.-C.; Son, C.-G. The Efficacy and Safety of Myelophil, an Ethanol Extract Mixture of Astragali Radix and Salviae Radix, for Chronic Fatigue Syndrome: A Randomized Clinical Trial. Front. Pharmacol. 2019, 10, 991. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, J.Y.; Kwon, O.-J.; Jung, S.Y.; Joung, J.-Y.; Yang, C.S.; Lee, J.-H.; Cho, J.-H.; Son, C.-G. Efficacy of a Traditional Herbal Formula, Banha-Sasim-Tang in Functional Dyspepsia Classified as Excess Pattern. Front. Pharmacol. 2021, 12, 698887. [Google Scholar] [CrossRef]
- Kim, S.-K.; Joung, J.-Y.; Ahn, Y.-C.; Jung, I.-C.; Son, C.-G. Beneficial Potential of Banha-Sasim-Tang for Stress-Sensitive Functional Dyspepsia via Modulation of Ghrelin: A Randomized Controlled Trial. Front. Pharmacol. 2021, 12, 636752. [Google Scholar] [CrossRef]
- Joung, J.-Y.; Kim, H.-G.; Lee, J.-S.; Cho, J.-H.; Ahn, Y.-C.; Lee, D.-S.; Son, C.-G. Anti-Hepatofibrotic Effects of CGX, a Standardized Herbal Formula: A Multicenter Randomized Clinical Trial. Biomed. Pharmacother. 2020, 126, 110105. [Google Scholar] [CrossRef]
- Kim, H.-G.; Yoo, S.-R.; Park, H.-J.; Lee, N.-H.; Shin, J.-W.; Sathyanath, R.; Cho, J.-H.; Son, C.-G. Antioxidant Effects of Panax Ginseng C.A. Meyer in Healthy Subjects: A Randomized, Placebo-Controlled Clinical Trial. Food Chem. Toxicol. 2011, 49, 2229–2235. [Google Scholar] [CrossRef]
- Kim, H.-G.; Cho, J.-H.; Yoo, S.-R.; Lee, J.-S.; Han, J.-M.; Lee, N.-H.; Ahn, Y.-C.; Son, C.-G. Antifatigue Effects of Panax Ginseng C.A. Meyer: A Randomised, Double-Blind, Placebo-Controlled Trial. PLoS ONE 2013, 8, e61271. [Google Scholar] [CrossRef]
- Hayashi, P.H.; Lucena, M.I.; Fontana, R.J.; Bjornsson, E.S.; Aithal, G.P.; Barnhart, H.; Jimenez, A.G.; Yang, Q.; Gu, J.; Andrade, R.J.; et al. A Revised Electronic Version of RUCAM for the Diagnosis of Drug Induced Liver Injury. Hepatology 2022, 76, 18–31. [Google Scholar] [CrossRef]
- Perazella, M.A.; Rosner, M.H. Drug-Induced Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2022, 17, 1220–1233. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Han, J.H.; Choi, K.M.; Kim, S.M. Relation between Elevated Serum Alanine Aminotransferase and Metabolic Syndrome in Korean Adolescents. Am. J. Clin. Nutr. 2005, 82, 1046–1051. [Google Scholar] [CrossRef] [PubMed]
- Makary, S.; Abd El Moez, K.; Elsayed, M.; Hassan, H. Second-Generation Antipsychotic Medications and Metabolic Disturbance in Children and Adolescents. Egypt. J. Neurol. Psychiatry Neurosurg. 2023, 59, 14. [Google Scholar] [CrossRef]
- Stevens, P.E.; Levin, A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Ghane Shahrbaf, F.; Assadi, F. Drug-Induced Renal Disorders. J. Ren. Inj. Prev. 2015, 4, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Naughton, C.A. Drug-Induced Nephrotoxicity. Am. Fam. Physician 2008, 78, 743–750. [Google Scholar] [PubMed]
- Yousif, Z.K.; Koola, J.D.; Macedo, E.; Cerda, J.; Goldstein, S.L.; Chakravarthi, R.; Lewington, A.; Selewski, D.; Zappitelli, M.; Cruz, D.; et al. Clinical Characteristics and Outcomes of Drug-Induced Acute Kidney Injury Cases. Kidney Int. Rep. 2023, 8, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Amacher, D.E. Female Gender as a Susceptibility Factor for Drug-Induced Liver Injury. Hum. Exp. Toxicol. 2014, 33, 928–939. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-Y.; Hsiao, C.-H.; Chen, Y.-C.; Ho, C.-H.; Wang, J.-J.; Hsing, C.-H.; Wang, H.-Y.; Kan, W.-C.; Wu, C.-C. Cisplatin Nephrotoxicity Might Have a Sex Difference. An Analysis Based on Women’s Sex Hormone Changes. J. Cancer 2017, 8, 3939–3944. [Google Scholar] [CrossRef]
- El-Bassossy, H.M.; Eid, B.G. Cyclosporine A Exhibits Gender-Specific Nephrotoxicity in Rats: Effect on Renal Tissue Inflammation. Biochem. Biophys. Res. Commun. 2018, 495, 468–472. [Google Scholar] [CrossRef]
- Hosohata, K. Role of Oxidative Stress in Drug-Induced Kidney Injury. Int. J. Mol. Sci. 2016, 17, 1826. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, S.; Azushima, K.; Yamaji, T.; Urate, S.; Suzuki, T.; Abe, E.; Tanaka, S.; Tsukamoto, S.; Kamimura, D.; Kinguchi, S.; et al. Effects of Tumor Necrosis Factor-α Inhibition on Kidney Fibrosis and Inflammation in a Mouse Model of Aristolochic Acid Nephropathy. Sci. Rep. 2021, 11, 23587. [Google Scholar] [CrossRef] [PubMed]
- Kiliś-Pstrusińska, K.; Wiela-Hojeńska, A. Nephrotoxicity of Herbal Products in Europe—A Review of an Underestimated Problem. Int. J. Mol. Sci. 2021, 22, 4132. [Google Scholar] [CrossRef] [PubMed]
- Baudoux, T.; Jadot, I.; Declèves, A.-E.; Antoine, M.-H.; Colet, J.-M.; Botton, O.; De Prez, E.; Pozdzik, A.; Husson, C.; Caron, N.; et al. Experimental Aristolochic Acid Nephropathy: A Relevant Model to Study AKI-to-CKD Transition. Front. Med. 2022, 9, 822870. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, D.-M.; Liu, J.-H.; Hu, L.-S.; Xue, Q.-C.; Ding, X.-Q.; Kong, L.-D. Wuling San Protects Kidney Dysfunction by Inhibiting Renal TLR4/MyD88 Signaling and NLRP3 Inflammasome Activation in High Fructose-Induced Hyperuricemic Mice. J. Ethnopharmacol. 2015, 169, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Kassianos, A.J.; Hoy, W.E.; Alam, A.K.; Healy, H.G.; Gobe, G.C. Promoting Plant-Based Therapies for Chronic Kidney Disease. J. Evid. Based Complement. Altern. Med. 2022, 27, 2515690X221079688. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yan, Z.; Xiong, Q.; Chen, X.; Lin, Y.; Xu, Y.; Bai, L.; Jiang, W.; Zheng, D.; Xing, C. Renoprotective Effect and Mechanism of Polysaccharide from Polyporus Umbellatus Sclerotia on Renal Fibrosis. Carbohydr. Polym. 2019, 212, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Yong, T.; Diao, X.; Chen, S.; Chen, D.; Xiao, C.; Zuo, D.; Xie, Y.; Zhou, X.; Hu, H. Hypouricaemic and Nephroprotective Effects of Poria Cocos in Hyperuricemic Mice by Up-Regulating ATP-Binding Cassette Super-Family G Member 2. Pharm. Biol. 2021, 59, 273–284. [Google Scholar] [CrossRef]
- Sung, S.-H.; Han, J.-E.; Ryu, J.-Y.; Sung, A.D.-M.; Park, J.-Y.; Ha, I.-H.; Kim, K.H.; Park, J.-K.; Shin, B.-C. Current Status and Future Perspective of External Herbal Dispensaries Preparing Traditional Herbal Medicine in South Korea: The First National-Wide Survey Results. BMC Complement. Med. Ther. 2020, 20, 354. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Chronic Kidney Disease Epidemiology Collaboration Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]


{kind=link}
| Intervention Group | Placebo Group | Total | |
|---|---|---|---|
| Male/Female | Male/Female | Male/Female | |
| Number participants (%) | 240 (59.0%) 89/151 | 167 (41.0%) 53/114 | 407 142/265 |
| Mean age (year) | 44.0 ± 10.7 46.0 ± 11.9/42.9 ± 9.7 | 44.5 ± 11.8 46.7 ± 11.5/43.5 ± 11.9 | 44.2 ± 11.1 46.3 ± 11.7/43.1 ± 10.7 |
| Mean BMI | 22.7 ± 3.0 23.6 ± 2.8/22.2 ± 2.9 | 23.1 ± 2.9 23.9 ± 3.0/22.7 ± 2.9 | 22.9 ± 3.0 23.7 ± 2.9/22.4 ± 2.9 |
| Intervention (weeks of treatment, daily dose gram/adult) and participants (male/female) | |||
| CGX (12, 1 or 2) | 42 (34/8) | 23 (18/5) | 65 (52/13) |
| Myelophil (12, 2) | 48 (16/32) | 49 (10/39) | 97 (26/71) |
| BST (4, 10) | 40 (12/28) | 39 (12/27) | 79 (24/55) |
| Ginseng (4, 1 or 2) | 110 (27/83) | 56 (13/43) | 166 (40/126) |
| Participants (N.) (Int. vs. Plac.) | Before (Top) and after Treatment (Bottom) | |||||
|---|---|---|---|---|---|---|
| BUN (mg/dL) | Creatinine (mg/dL) | eGFR (mL/min) | ||||
| Intervention | Placebo | Intervention | Placebo | Intervention | Placebo | |
| Total | 13.1 ± 3.3 | 13.5 ± 3.5 | 0.81 ± 0.17 | 0.81 ± 0.17 | 107.2 ± 26.7 | 105.8 ± 25.5 |
| (240 vs. 167) | 13.5 ± 7.0 | 13.3 ± 3.4 | 0.83 ± 0.18 | 0.84 ± 0.17 | 105.2 ± 28.5 | 102.8 ± 26.7 |
| Male | 13.9 ± 3.5 | 14.3 ± 3.2 | 0.91 ± 0.16 | 0.92 ± 0.18 | 93.6 ± 19.7 | 93.2 ± 20.5 |
| (89 vs. 53) | 13.7 ± 4.2 | 13.4 ± 3.0 | 0.91 ± 0.19 | 0.94 ± 0.18 | 95.9 ± 24.4 | 91.8 ± 23.5 |
| Female | 12.6 ± 3.0 | 13.1 ± 3.6 | 0.75 ± 0.14 | 0.76 ± 0.14 | 115.4 ± 27.1 | 111.6 ± 25.5 |
| (151 vs. 114) | 12.6 ± 3.4 | 13.2 ± 3.6 | 0.78 ± 0.16 | 0.79 ± 0.15 | 110.8 ± 29.4 | 108.0 ± 26.7 |
| CGX | 14.4 ± 3.5 | 15.1 ± 2.5 | 0.90 ± 0.18 | 0.89 ± 0.20 | 92.1 ± 21.7 | 95.0 ± 25.2 |
| (44 vs. 23) | 15.1 ± 4.3 | 14.6 ± 2.3 | 0.89 ± 0.15 | 0.90 ± 0.15 | 93.6 ± 21.2 | 91.6 ± 17.2 |
| BST | 14.0 ± 4.5 | 13.4 ± 3.2 | 0.81 ± 0.22 | 0.82 ± 0.19 | 97.2 ± 31.7 | 92.5 ± 23.1 |
| (40 vs. 39) | 13.8 ± 4.8 | 13.9 ± 3.6 | 0.81 ± 0.23 | 0.86 ± 0.16 | 96.2 ± 28.3 | 86.1 ± 20.2 |
| Myelophil | 12.3 ± 2.4 | 13.0 ± 3.9 | 0.77 ± 0.15 | 0.77 ± 0.13 | 117.3 ± 28.6 | 116.8 ± 24.1 |
| (48 vs. 49) | 12.5 ± 3.4 | 13.0 ± 3.4 | 0.76 ± 0.16 | 0.80 ± 0.16 | 121.8 ± 33.3 | 112.9 ± 24.0 |
| Ginseng | 12.6 ± 2.7 | 13.3 ± 3.5 | 0.80 ± 0.14 | 0.82 ± 0.16 | 112.3 ± 9.2 | 110.7 ± 23.2 |
| (110 vs. 56) | 13.1 ± 9.2 | 12.6 ± 3.6 | 0.85 ± 0.16 | 0.83 ± 0.20 | 105.6 ± 25.2 | 110.3 ± 29.3 |
| Sub-Group | Intervention Group (n = 240) | Placebo Group (n = 167) | Statistics (p Value) |
|---|---|---|---|
| Participants in 90th-percentile Analysis (male/female) | 22 (2/20) | 18 (2/16) | 0.591 |
| eGFR in 90th-percentile analysis (mL/min) | |||
| 141.0 ± 17.9 99.1 ± 13.1 41.9 ± 12.7 | 140.4 ± 21.7 99.1 ± 21.8 41.3 ± 7.7 | 0.835 |
| Participants with eGFR < 60 | |||
| 4 1 | 3 4 | 0.939 0.075 |
| Participants with ≥20% reduction in eGFR | |||
| 44 (18.3%) 0 | 35 (21.0%) 2 | 0.510 0.185 |
| eGFR in ≥20% reduction group (mL/min) | |||
| 123.2 ± 24.5 90.5 ± 15.1 32.7 ± 13.4 | 123.0 ± 27.1 89.3 ± 22.0 33.6 ± 10.0 | 0.736 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joung, J.-Y.; Son, C.-G. Evaluating the Safety of Herbal Medicine on Renal Function: A Comprehensive Analysis from Six Randomized Controlled Trials Conducted with Four Formulations from Traditional Korean Medicine. Pharmaceuticals 2024, 17, 544. https://doi.org/10.3390/ph17050544
Joung J-Y, Son C-G. Evaluating the Safety of Herbal Medicine on Renal Function: A Comprehensive Analysis from Six Randomized Controlled Trials Conducted with Four Formulations from Traditional Korean Medicine. Pharmaceuticals. 2024; 17(5):544. https://doi.org/10.3390/ph17050544
Chicago/Turabian StyleJoung, Jin-Yong, and Chang-Gue Son. 2024. "Evaluating the Safety of Herbal Medicine on Renal Function: A Comprehensive Analysis from Six Randomized Controlled Trials Conducted with Four Formulations from Traditional Korean Medicine" Pharmaceuticals 17, no. 5: 544. https://doi.org/10.3390/ph17050544