
The Optimal Management of Patients with Atrial Fibrillation and Acute Heart Failure in the Emergency Department

 ,
,
Abstract
:1. Introduction
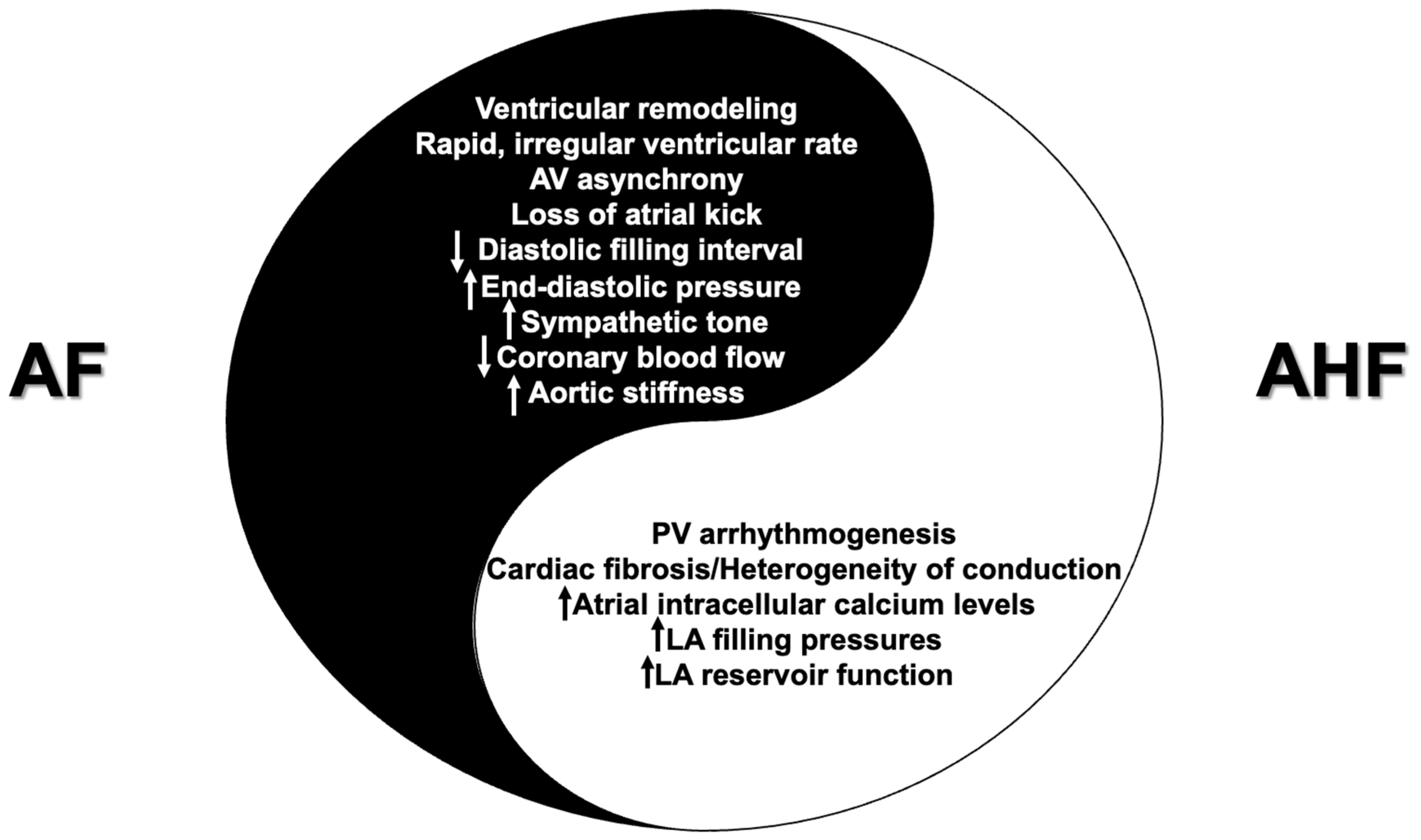
2. The Interplay between AF and AHF
2.1. AF as the Triggering Factor of AHF
2.2. AF as the Consequence of AHF
2.3. AF as an Innocent Bystander of AHF
3. The Management of AF in AHF Patients in the ED
3.1. Rate Control
3.2. Rhythm Control
3.3. Anticoagulation
4. Early Rhythm Control versus Acute Rate Control
5. AF in Cardiogenic Shock
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Capucci, A.; Wong, J.A.; Gold, M.R.; Boehmer, J.; Ahmed, R.; Kwan, B.; Thakur, P.H.; Zhang, Y.; Jones, P.W.; Healey, J.S. Temporal Association of Atrial Fibrillation With Cardiac Implanted Electronic Device Detected Heart Failure Status. JACC Clin. Electrophysiol. 2022, 8, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.; Swedberg, K.; Follath, F.; Komajda, M.; Cohen-Solal, A.; Aguilar, J.C.; Dietz, R.; Gavazzi, A.; Hobbs, R.; Korewicki, J.; et al. The EuroHeart Failure survey programme—A survey on the quality of care among patients with heart failure in Europe. Part 1: Patient characteristics and diagnosis. Eur. Heart J. 2003, 24, 442–463. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Committee, A.S.A. The Acute Decompensated Heart Failure National Registry (ADHERE): Opportunities to improve care of patients hospitalized with acute decompensated heart failure. Rev. Cardiovasc. Med. 2003, 4 (Suppl. 7), S21–S30. [Google Scholar] [PubMed]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Stough, W.G.; Abraham, W.T.; Albert, N.M.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B.; et al. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: A report from the OPTIMIZE-HF Registry. J. Am. Coll. Cardiol. 2007, 50, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, A.P.; Dahlstrom, U.; Filippatos, G.; Chioncel, O.; Leiro, M.C.; Drozdz, J.; Fruhwald, F.; Gullestad, L.; Logeart, D.; Metra, M.; et al. EURObservational Research Programme: The Heart Failure Pilot Survey (ESC-HF Pilot). Eur. J. Heart Fail. 2010, 12, 1076–1084. [Google Scholar] [CrossRef]
- Follath, F.; Yilmaz, M.B.; Delgado, J.F.; Parissis, J.T.; Porcher, R.; Gayat, E.; Burrows, N.; McLean, A.; Vilas-Boas, F.; Mebazaa, A. Clinical presentation, management and outcomes in the Acute Heart Failure Global Survey of Standard Treatment (ALARM-HF). Intensive Care Med. 2011, 37, 619–626. [Google Scholar] [CrossRef]
- Damasceno, A.; Mayosi, B.M.; Sani, M.; Ogah, O.S.; Mondo, C.; Ojji, D.; Dzudie, A.; Kouam, C.K.; Suliman, A.; Schrueder, N.; et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries. Arch. Intern. Med. 2012, 172, 1386–1394. [Google Scholar] [CrossRef]
- Sato, N.; Kajimoto, K.; Keida, T.; Mizuno, M.; Minami, Y.; Yumino, D.; Asai, K.; Murai, K.; Muanakata, R.; Aokage, T.; et al. Clinical features and outcome in hospitalized heart failure in Japan (from the ATTEND Registry). Circ. J. 2013, 77, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Harikrishnan, S.; Sanjay, G.; Anees, T.; Viswanathan, S.; Vijayaraghavan, G.; Bahuleyan, C.G.; Sreedharan, M.; Biju, R.; Nair, T.; Suresh, K.; et al. Clinical presentation, management, in-hospital and 90-day outcomes of heart failure patients in Trivandrum, Kerala, India: The Trivandrum Heart Failure Registry. Eur. J. Heart Fail. 2015, 17, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Abualnaja, S.; Podder, M.; Hernandez, A.F.; McMurray, J.J.; Starling, R.C.; O’Connor, C.M.; Califf, R.M.; Armstrong, P.W.; Ezekowitz, J.A. Acute Heart Failure and Atrial Fibrillation: Insights From the Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (ASCEND-HF) Trial. J. Am. Heart Assoc. 2015, 4, e002092. [Google Scholar] [CrossRef]
- Diaz, J.; Martinez, F.; Calderon, J.M.; Fernandez, A.; Sauri, I.; Uso, R.; Trillo, J.L.; Redon, J.; Forner, M.J. Incidence and impact of atrial fibrillation in heart failure patients: Real-world data in a large community. ESC Heart Fail. 2022, 9, 4230–4239. [Google Scholar] [CrossRef] [PubMed]
- Chantrarat, T.; Ayudhya, R.K.N.; Phrominthikul, A.; Ariyachaipanich, A.; Krittayaphong, R. Heart Failure Council of Thailand (HFCT) 2019 Heart Failure Guideline: Atrial Fibrillation in Heart Failure Guidelines. J. Med. Assoc. Thai 2019, 102, 513–517. [Google Scholar]
- Kornej, J.; Borschel, C.S.; Benjamin, E.J.; Schnabel, R.B. Epidemiology of Atrial Fibrillation in the 21st Century: Novel Methods and New Insights. Circ. Res. 2020, 127, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Caldarola, P.; De Iaco, F.; Pugliese, F.R.; De Luca, L.; Fabbri, A.; Riccio, C.; Scicchitano, P.; Vanni, S.; Di Pasquale, G.; Gulizia, M.M.; et al. ANMCO-SIMEU consensus document: Appropriate management of atrial fibrillation in the emergency department. Eur. Heart J. Suppl. 2023, 25 (Suppl. D), D255–D277. [Google Scholar] [CrossRef]
- Fountoulaki, K.; Ventoulis, I.; Drokou, A.; Georgarakou, K.; Parissis, J.; Polyzogopoulou, E. Emergency department risk assessment and disposition of acute heart failure patients: Existing evidence and ongoing challenges. Heart Fail. Rev. 2023, 28, 781–793. [Google Scholar] [CrossRef]
- Gorenek, B.; Halvorsen, S.; Kudaiberdieva, G.; Bueno, H.; Van Gelder, I.C.; Lettino, M.; Marin, F.; Masip, J.; Mueller, C.; Okutucu, S.; et al. Atrial fibrillation in acute heart failure: A position statement from the Acute Cardiovascular Care Association and European Heart Rhythm Association of the European Society of Cardiology. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 348–357. [Google Scholar] [CrossRef]
- Sugumar, H.; Nanayakkara, S.; Prabhu, S.; Voskoboinik, A.; Kaye, D.M.; Ling, L.H.; Kistler, P.M. Pathophysiology of Atrial Fibrillation and Heart Failure: Dangerous Interactions. Cardiol. Clin. 2019, 37, 131–138. [Google Scholar] [CrossRef]
- Van Gelder, I.C.; Rienstra, M.; Crijns, H.J.; Olshansky, B. Rate control in atrial fibrillation. Lancet 2016, 388, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Huizar, J.F.; Ellenbogen, K.A.; Tan, A.Y.; Kaszala, K. Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2328–2344. [Google Scholar] [CrossRef]
- Kotecha, D.; Piccini, J.P. Atrial fibrillation in heart failure: What should we do? Eur. Heart J. 2015, 36, 3250–3257. [Google Scholar] [CrossRef] [PubMed]
- Scarsoglio, S.; Gallo, C.; Saglietto, A.; Ridolfi, L.; Anselmino, M. Impaired coronary blood flow at higher heart rates during atrial fibrillation: Investigation via multiscale modelling. Comput. Methods Programs Biomed. 2019, 175, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Gronda, E.; Dusi, V.; D’Elia, E.; Iacoviello, M.; Benvenuto, E.; Vanoli, E. Sympathetic activation in heart failure. Eur. Heart J. Suppl. 2022, 24 (Suppl. E), E4–E11. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.C.; Hung, T.C.; Kusayama, T.; Han, S.; Fishbein, M.C.; Chen, L.S.; Chen, P.S. Autonomic Modulation of Atrial Fibrillation. JACC Basic Transl. Sci. 2023, 8, 1398–1410. [Google Scholar] [CrossRef]
- Triposkiadis, F.; Xanthopoulos, A.; Lampropoulos, K.; Briasoulis, A.; Sarafidis, P.; Skoularigis, J.; Boudoulas, H. Aortic Stiffness: A Major Risk Factor for Multimorbidity in the Elderly. J. Clin. Med. 2023, 12, 2321. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.L.; Chen, Y.C.; Yeh, Y.H.; Lin, Y.K.; Wu, T.J.; Lin, C.I.; Chen, S.A.; Chen, Y.J. Heart failure enhanced pulmonary vein arrhythmogenesis and dysregulated sodium and calcium homeostasis with increased calcium sparks. J. Cardiovasc. Electrophysiol. 2011, 22, 1378–1386. [Google Scholar] [CrossRef]
- Lehnart, S.E.; Wehrens, X.H.; Kushnir, A.; Marks, A.R. Cardiac ryanodine receptor function and regulation in heart disease. Ann. N. Y. Acad. Sci. 2004, 1015, 144–159. [Google Scholar] [CrossRef]
- Federico, M.; Valverde, C.A.; Mattiazzi, A.; Palomeque, J. Unbalance Between Sarcoplasmic Reticulum Ca(2+) Uptake and Release: A First Step Toward Ca(2+) Triggered Arrhythmias and Cardiac Damage. Front. Physiol. 2019, 10, 1630. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Obokata, M.; Verbrugge, F.H.; Lin, G.; Borlaug, B.A. Atrial Dysfunction in Patients With Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 76, 1051–1064. [Google Scholar] [CrossRef]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Alsagaff, M.Y.; Susilo, H.; Pramudia, C.; Juzar, D.A.; Amadis, M.R.; Julario, R.; Raharjo, S.B.; Dharmadjati, B.B.; Lusida, T.T.E.; Azmi, Y.; et al. Rapid Atrial Fibrillation in the Emergency Department. Heart Int. 2022, 16, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Oliva, F.; Sormani, P.; Contri, R.; Campana, C.; Carubelli, V.; Ciro, A.; Morandi, F.; Di Tano, G.; Mortara, A.; Senni, M.; et al. Heart rate as a prognostic marker and therapeutic target in acute and chronic heart failure. Int. J. Cardiol. 2018, 253, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, B.A.; Kim, S.; Thomas, L.; Fonarow, G.C.; Gersh, B.J.; Holmqvist, F.; Hylek, E.; Kowey, P.R.; Mahaffey, K.W.; Naccarelli, G.; et al. Increased Heart Rate Is Associated With Higher Mortality in Patients With Atrial Fibrillation (AF): Results From the Outcomes Registry for Better Informed Treatment of AF (ORBIT-AF). J. Am. Heart Assoc. 2015, 4, e002031. [Google Scholar] [CrossRef]
- Jondeau, G.; Milleron, O. Beta-Blockers in Acute Heart Failure: Do They Cause Harm? JACC Heart Fail. 2015, 3, 654–656. [Google Scholar] [CrossRef] [PubMed]
- Bezati, S.; Velliou, M.; Polyzogopoulou, E.; Boultadakis, A.; Parissis, J. The role of landiolol in the management of atrial tachyarrhythmias in patients with acute heart failure and cardiogenic shock: Case reports and review of literature. Eur. Heart J. Suppl. 2022, 24 (Suppl. D), D22–D33. [Google Scholar] [CrossRef] [PubMed]
- Nagai, R.; Kinugawa, K.; Inoue, H.; Atarashi, H.; Seino, Y.; Yamashita, T.; Shimizu, W.; Aiba, T.; Kitakaze, M.; Sakamoto, A.; et al. Urgent management of rapid heart rate in patients with atrial fibrillation/flutter and left ventricular dysfunction: Comparison of the ultra-short-acting beta1-selective blocker landiolol with digoxin (J-Land Study). Circ. J. 2013, 77, 908–916. [Google Scholar] [CrossRef]
- Kinugawa, K.; Nagai, R.; Inoue, H.; Atarashi, H.; Seino, Y.; Yamashita, T.; Shimizu, W.; Aiba, T.; Kitakaze, M.; Sakamoto, A.; et al. Impacts of patient characteristics on the effectiveness of landiolol in AF/AFL patients complicated with LV dysfunction: Subgroup analysis of the J-Land study. Adv. Ther. 2014, 31, 426–439. [Google Scholar] [CrossRef]
- Iwahashi, N.; Takahashi, H.; Abe, T.; Okada, K.; Akiyama, E.; Matsuzawa, Y.; Konishi, M.; Maejima, N.; Hibi, K.; Kosuge, M.; et al. Urgent Control of Rapid Atrial Fibrillation by Landiolol in Patients With Acute Decompensated Heart Failure With Severely Reduced Ejection Fraction. Circ. Rep. 2019, 1, 422–430. [Google Scholar] [CrossRef]
- Kiuchi, S.; Aikawa, H.; Hisatake, S.; Kabuki, T.; Oka, T.; Dobashi, S.; Fujii, T.; Ikeda, T. Efficacy of Intravenous Administration of Landiolol in Patients With Acute Heart Failure and Supraventricular Tachyarrhythmia. J. Clin. Med. Res. 2017, 9, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Matsui, Y.; Suzuki, A.; Shiga, T.; Arai, K.; Hagiwara, N. Effects of Intravenous Landiolol on Heart Rate and Outcomes in Patients with Atrial Tachyarrhythmias and Acute Decompensated Heart Failure: A Single-Center Experience. Drugs Real World Outcomes 2019, 6, 19–26. [Google Scholar] [CrossRef]
- Oka, E.; Iwasaki, Y.K.; Maru, E.; Fujimoto, Y.; Ito-Hagiwara, K.; Hayashi, H.; Yamamoto, T.; Yodogawa, K.; Hayashi, M.; Shimizu, W. Differential Effectiveness of Landiolol Between Atrial Fibrillation and Atrial Flutter/Atrial Tachycardia Patients with Left Ventricular Dysfunction. Circ. J. 2019, 83, 793–800. [Google Scholar] [CrossRef]
- Shinohara, M.; Wada, R.; Yano, K.; Akitsu, K.; Koike, H.; Kinoshita, T.; Suzuki, T.; Fujino, T.; Ikeda, T. Comparison of Landiolol and Digoxin as an Intravenous Drug for Controlling the Heart Rate in Patients with Atrial Fibrillation and Severely Depressed Left Ventricular Function. Int. Heart J. 2020, 61, 944–950. [Google Scholar] [CrossRef]
- Wada, Y.; Aiba, T.; Tsujita, Y.; Itoh, H.; Wada, M.; Nakajima, I.; Ishibashi, K.; Okamura, H.; Miyamoto, K.; Noda, T.; et al. Practical applicability of landiolol, an ultra-short-acting beta1-selective blocker, for rapid atrial and ventricular tachyarrhythmias with left ventricular dysfunction. J. Arrhythm. 2016, 32, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Krumpl, G.; Ulc, I.; Trebs, M.; Kadlecova, P.; Hodisch, J. Bolus application of landiolol and esmolol: Comparison of the pharmacokinetic and pharmacodynamic profiles in a healthy Caucasian group. Eur. J. Clin. Pharmacol. 2017, 73, 417–428. [Google Scholar] [CrossRef]
- McKeever, R.G.; Hamilton, R.J. Calcium Channel Blockers. In StatPearls; Ineligible Companies: Treasure Island, FL, USA, 2023. [Google Scholar]
- Medeiros, T.; Bui, V.; Almekdash, M.H.; Keesari, R.; Lee, Y.R. Rate control with intravenous diltiazem, verapamil, and metoprolol in acute atrial fibrillation with rapid ventricular rate. SAGE Open Med. 2021, 9, 20503121211017756. [Google Scholar] [CrossRef] [PubMed]
- Forshay, C.M.; Michael Boyd, J.; Rozycki, A.; Pilz, J. The Safety and Efficacy of Verapamil Versus Diltiazem Continuous Infusion for Acute Rate Control of Atrial Fibrillation at an Academic Medical Center. Hosp. Pharm. 2021, 56, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Rajput, F.A.; Du, L.; Chappell, R.J.; Berei, T.J.; Goldberger, Z.D.; Wright, J.M. Comparative Efficacy and Safety of Intravenous Verapamil and Diltiazem for Rate Control in Rapidly Conducted Atrial Fibrillation and Atrial Flutter. J. Gen. Intern. Med. 2020, 35, 3721–3723. [Google Scholar] [CrossRef] [PubMed]
- Mujovic, N.; Dobrev, D.; Marinkovic, M.; Russo, V.; Potpara, T.S. The role of amiodarone in contemporary management of complex cardiac arrhythmias. Pharmacol. Res. 2020, 151, 104521. [Google Scholar] [CrossRef]
- Hofmann, R.; Steinwender, C.; Kammler, J.; Kypta, A.; Leisch, F. Effects of a high dose intravenous bolus amiodarone in patients with atrial fibrillation and a rapid ventricular rate. Int. J. Cardiol. 2006, 110, 27–32. [Google Scholar] [CrossRef]
- Horiuchi, D.; Sasaki, S.; Kinjo, T.; Ishida, Y.; Itoh, T.; Sasaki, K.; Owada, S.; Kimura, M.; Okumura, K. Rhythm and rate control effects of intravenous amiodarone for atrial fibrillation complicated by acutely decompensated heart failure. J. Arrhythm. 2014, 30, 167–172. [Google Scholar] [CrossRef]
- Ferrari, F.; Santander, I.; Stein, R. Digoxin in Atrial Fibrillation: An Old Topic Revisited. Curr. Cardiol. Rev. 2020, 16, 141–146. [Google Scholar] [CrossRef]
- Shrestha, S.; Lopez-Ayala, P.; Schaefer, I.; Nardiello, S.S.; Papachristou, A.; Aliyeva, F.; Simmen, C.; Wussler, D.; Belkin, M.; Gualandro, D.M.; et al. Efficacy and safety of digoxin in acute heart failure triggered by tachyarrhythmia. J. Intern. Med. 2022, 292, 969–972. [Google Scholar] [CrossRef] [PubMed]
- Abdel Jalil, M.; Abdullah, N.; Alsous, M.; Abu-Hammour, K. Population Pharmacokinetic Studies of Digoxin in Adult Patients: A Systematic Review. Eur. J. Drug Metab. Pharmacokinet 2021, 46, 325–342. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Naccarelli, G.V.; Mittal, S.; Crijns, H.; Hohnloser, S.H.; Ma, C.S.; Natale, A.; Turakhia, M.P.; Kirchhof, P. The Increasing Role of Rhythm Control in Patients With Atrial Fibrillation: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 1932–1948. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Oh, I.Y.; Park, J.J.; Oh, B.H.; Jeon, E.S.; Kim, J.J.; Hwang, K.K.; Cho, M.C.; Chae, S.C.; Baek, S.H.; et al. Impact of successful restoration of sinus rhythm in patients with atrial fibrillation and acute heart failure: Results from the Korean Acute Heart Failure registry. Cardiol. J. 2022, 29, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Dan, G.A.; Dan, A.R.; Ivanescu, A.; Buzea, A.C. Acute rate control in atrial fibrillation: An urgent need for the clinician. Eur. Heart J. Suppl. 2022, 24, D3–D10. [Google Scholar] [CrossRef]
- Crijns, H.J.; Bash, L.D.; Chazelle, F.; Le Heuzey, J.Y.; Lewalter, T.; Lip, G.Y.; Maggioni, A.P.; Martin, A.; Ponikowski, P.; Rosenqvist, M.; et al. RHYTHM-AF: Design of an international registry on cardioversion of atrial fibrillation and characteristics of participating centers. BMC Cardiovasc. Disord. 2012, 12, 85. [Google Scholar] [CrossRef]
- Hernandez-Madrid, A.; Svendsen, J.H.; Lip, G.Y.; Van Gelder, I.C.; Dobreanu, D.; Blomstrom-Lundqvist, C.; Scientific Initiatives Committee, E.H.R.A. Cardioversion for atrial fibrillation in current European practice: Results of the European Heart Rhythm Association survey. Europace 2013, 15, 915–918. [Google Scholar] [CrossRef]
- Hall, A.J.; Mitchell, A.R. Introducing Vernakalant into Clinical Practice. Arrhythm. Electrophysiol. Rev. 2019, 8, 70–74. [Google Scholar] [CrossRef]
- Savelieva, I.; Graydon, R.; Camm, A.J. Pharmacological cardioversion of atrial fibrillation with vernakalant: Evidence in support of the ESC Guidelines. Europace 2014, 16, 162–173. [Google Scholar] [CrossRef]
- Camm, A.J.; Capucci, A.; Hohnloser, S.H.; Torp-Pedersen, C.; Van Gelder, I.C.; Mangal, B.; Beatch, G.; Investigators, A. A randomized active-controlled study comparing the efficacy and safety of vernakalant to amiodarone in recent-onset atrial fibrillation. J. Am. Coll. Cardiol. 2011, 57, 313–321. [Google Scholar] [CrossRef]
- Levy, S.; Hartikainen, J.; Ritz, B.; Juhlin, T.; Carbajosa-Dalmau, J.; Domanovits, H. Vernakalant for Rapid Cardioversion of Recent-Onset Atrial Fibrillation: Results from the SPECTRUM Study. Cardiovasc. Drugs Ther. 2021, 35, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Calvert, P.; Gupta, D.; Lip, G.Y.H. Antazoline: The Lazarus of antiarrhythmic drugs? Pol. Arch. Intern. Med. 2022, 132, 16264. [Google Scholar] [CrossRef] [PubMed]
- Frommeyer, G.; Sterneberg, M.; Dechering, D.G.; Kaese, S.; Bogeholz, N.; Pott, C.; Fehr, M.; Bogossian, H.; Milberg, P.; Eckardt, L. Effective suppression of atrial fibrillation by the antihistaminic agent antazoline: First experimental insights into a novel antiarrhythmic agent. Cardiovasc. Ther. 2017, 35, e12244. [Google Scholar] [CrossRef] [PubMed]
- Ellermann, C.; Sterneberg, M.; Kochhauser, S.; Dechering, D.G.; Fehr, M.; Eckardt, L.; Frommeyer, G. Antiarrhythmic effect of antazoline in experimental models of acquired short- and long-QT-syndromes. Europace 2018, 20, 1699–1706. [Google Scholar] [CrossRef] [PubMed]
- Wybraniec, M.T.; Maciag, A.; Miskowiec, D.; Ceynowa-Sielawko, B.; Balsam, P.; Wojcik, M.; Wrobel, W.; Farkowski, M.; Cwiek-Rebowska, E.; Szolkiewicz, M.; et al. Efficacy and safety of antazoline for cardioversion of atrial fibrillation: Propensity score matching analysis of a multicenter registry (CANT II Study). Pol. Arch. Intern. Med. 2022, 132, 16234. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Wu, Y.Y.; Lip, G.Y.; Yin, P.; Hu, Y. Heart failure and risk of venous thromboembolism: A systematic review and meta-analysis. Lancet Haematol. 2016, 3, e30–e44. [Google Scholar] [CrossRef]
- Garg, A.; Khunger, M.; Seicean, S.; Chung, M.K.; Tchou, P.J. Incidence of Thromboembolic Complications Within 30 Days of Electrical Cardioversion Performed Within 48 Hours of Atrial Fibrillation Onset. JACC Clin. Electrophysiol. 2016, 2, 487–494. [Google Scholar] [CrossRef]
- Wyse, D.G.; Waldo, A.L.; DiMarco, J.P.; Domanski, M.J.; Rosenberg, Y.; Schron, E.B.; Kellen, J.C.; Greene, H.L.; Mickel, M.C.; Dalquist, J.E.; et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N. Engl. J. Med. 2002, 347, 1825–1833. [Google Scholar] [CrossRef]
- Hohnloser, S.H.; Kuck, K.H.; Lilienthal, J. Rhythm or rate control in atrial fibrillation—Pharmacological Intervention in Atrial Fibrillation (PIAF): A randomised trial. Lancet 2000, 356, 1789–1794. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, I.C.; Hagens, V.E.; Bosker, H.A.; Kingma, J.H.; Kamp, O.; Kingma, T.; Said, S.A.; Darmanata, J.I.; Timmermans, A.J.; Tijssen, J.G.; et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N. Engl. J. Med. 2002, 347, 1834–1840. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, J.; Miketic, S.; Windeler, J.; Cuneo, A.; Haun, S.; Micus, S.; Walter, S.; Tebbe, U.; Investigators, S. Randomized trial of rate-control versus rhythm-control in persistent atrial fibrillation: The Strategies of Treatment of Atrial Fibrillation (STAF) study. J. Am. Coll. Cardiol. 2003, 41, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Opolski, G.; Torbicki, A.; Kosior, D.A.; Szulc, M.; Wozakowska-Kaplon, B.; Kolodziej, P.; Achremczyk, P.; Investigators of the Polish How to Treat Chronic Atrial Fibrillation, S. Rate control vs rhythm control in patients with nonvalvular persistent atrial fibrillation: The results of the Polish How to Treat Chronic Atrial Fibrillation (HOT CAFE) Study. Chest 2004, 126, 476–486. [Google Scholar] [CrossRef]
- Roy, D.; Talajic, M.; Nattel, S.; Wyse, D.G.; Dorian, P.; Lee, K.L.; Bourassa, M.G.; Arnold, J.M.; Buxton, A.E.; Camm, A.J.; et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N. Engl. J. Med. 2008, 358, 2667–2677. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, S.; Yamashita, T.; Yamazaki, T.; Aizawa, Y.; Atarashi, H.; Inoue, H.; Ohe, T.; Ohtsu, H.; Okumura, K.; Katoh, T.; et al. Optimal treatment strategy for patients with paroxysmal atrial fibrillation: J-RHYTHM Study. Circ. J. 2009, 73, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef]
- Rillig, A.; Magnussen, C.; Ozga, A.K.; Suling, A.; Brandes, A.; Breithardt, G.; Camm, A.J.; Crijns, H.; Eckardt, L.; Elvan, A.; et al. Early Rhythm Control Therapy in Patients With Atrial Fibrillation and Heart Failure. Circulation 2021, 144, 845–858. [Google Scholar] [CrossRef]
- Kirchhof, P.; Camm, A.J.; Crijns, H.J.G.M.; Piccini, J.P.; Torp-Pedersen, C.; McKindley, D.; Stewart, J.; Wieloch, M.; Hohnloser, S.H. Dronedarone as early rhythm control: Post-hoc analysis of the ATHENA trial using EAST-AFNET4 criteria. Eur. Heart J. Suppl. 2022, 43, ehac544.433. [Google Scholar] [CrossRef]
- Kany, S.; Cardoso, V.R.; Bravo, L.; Williams, J.A.; Schnabel, R.; Fabritz, L.; Gkoutos, G.V.; Kirchhof, P. Eligibility for early rhythm control in patients with atrial fibrillation in the UK Biobank. Heart 2022, 108, 1873–1880. [Google Scholar] [CrossRef] [PubMed]
- Adachi, T.; Sato, A.; Baba, M.; Hiraya, D.; Hasegawa, T.; Kuroki, K.; Hoshi, T.; Aonuma, K. Novel use of the ultra-short-acting intravenous beta1-selective blocker landiolol for supraventricular tachyarrhythmias in patients with congestive heart failure. Heart Vessel. 2014, 29, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Kakihana, Y.; Nishida, O.; Taniguchi, T.; Okajima, M.; Morimatsu, H.; Ogura, H.; Yamada, Y.; Nagano, T.; Morishima, E.; Matsuda, N.; et al. Efficacy and safety of landiolol, an ultra-short-acting beta1-selective antagonist, for treatment of sepsis-related tachyarrhythmia (J-Land 3S): A multicentre, open-label, randomised controlled trial. Lancet Respir. Med. 2020, 8, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Murakami, W.; Myoren, T.; Tateishi, H.; Okuda, S.; Doi, M.; Nao, T.; Wada, Y.; Matsuzaki, M.; Yano, M. A low-dose beta1-blocker effectively and safely slows the heart rate in patients with acute decompensated heart failure and rapid atrial fibrillation. Cardiology 2014, 127, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Myoren, T.; Kajii, T.; Kohno, M.; Nanno, T.; Ishiguchi, H.; Nishimura, S.; Fukuda, M.; Hino, A.; Fujimura, T.; et al. Addition of a beta1-Blocker to Milrinone Treatment Improves Cardiac Function in Patients with Acute Heart Failure and Rapid Atrial Fibrillation. Cardiology 2019, 142, 195–202. [Google Scholar] [CrossRef]
- Kobayashi, S.; Susa, T.; Tanaka, T.; Murakami, W.; Fukuta, S.; Okuda, S.; Doi, M.; Wada, Y.; Nao, T.; Yamada, J.; et al. Low-dose beta-blocker in combination with milrinone safely improves cardiac function and eliminates pulsus alternans in patients with acute decompensated heart failure. Circ. J. 2012, 76, 1646–1653. [Google Scholar] [CrossRef] [PubMed]
- Arita, Y.; Segawa, T.; Yamamoto, S.; Hasegawa, S. Landiolol is effective for the treatment of tachycardia-induced cardiogenic shock in patients during septic shock therapy. BMJ Case Rep. 2017, 2017, bcr-2017. [Google Scholar] [CrossRef]
- Dabrowski, W.; Siwicka-Gieroba, D.; Piasek, E.; Schlegel, T.T.; Jaroszynski, A. Successful Combination of Landiolol and Levosimendan in Patients with Decompensated Heart Failure. Int. Heart J. 2020, 61, 384–389. [Google Scholar] [CrossRef]
- Nitta, D.; Kinugawa, K.; Imamura, T.; Endo, M.; Amiya, E.; Inaba, T.; Maki, H.; Hatano, M.; Komuro, I. An Experience of Landiolol Use for an Advanced Heart Failure Patient With Severe Hypotension. Int. Heart J. 2015, 56, 564–567. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Patients | Age (years) | History of HF (%) | AF (%) |
|---|---|---|---|---|
| EHFS I, 2003 [4] | 11,327 | 71.0 | 65 | 43 |
| ADHERE, 2003 [5] | 105,388 | 72.0 ± 14.0 | 75 | 31 |
| EHFS II, 2006 [6] | 3580 | 69.9 ± 12.5 | 63 | 38.7 |
| OPTIMIZE-HF, 2007 [7] | 48,612 | 73.1 ± 14.2 | 87 | 31 |
| ESC-HF Pilot (AHF arm), 2010 [8] | 1892 | 70.0 ± 13.0 | 75 | 43.7 |
| ALARM-HF, 2011 [9] | 4953 | 66.0–70.0 | 64 | 24.4 |
| THESUS-HF, 2012 [10] | 1006 | 52.3 ± 18.3 | NA | 18.3 |
| ATTEND, 2013 [11] | 4842 | >20 | 36.2 | 39.6 |
| THER, 2015 [12] | 1232 | 61.2 ± 13.6 | 100 | 14.7 |
| ASCEND, 2016 [13] | 7007 | 56.0–76.0 | NA | De novo AF 38.2 History of AF 61.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velliou, M.; Sanidas, E.; Diakantonis, A.; Ventoulis, I.; Parissis, J.; Polyzogopoulou, E. The Optimal Management of Patients with Atrial Fibrillation and Acute Heart Failure in the Emergency Department. Medicina 2023, 59, 2113. https://doi.org/10.3390/medicina59122113
Velliou M, Sanidas E, Diakantonis A, Ventoulis I, Parissis J, Polyzogopoulou E. The Optimal Management of Patients with Atrial Fibrillation and Acute Heart Failure in the Emergency Department. Medicina. 2023; 59(12):2113. https://doi.org/10.3390/medicina59122113
Chicago/Turabian StyleVelliou, Maria, Elias Sanidas, Antonis Diakantonis, Ioannis Ventoulis, John Parissis, and Effie Polyzogopoulou. 2023. "The Optimal Management of Patients with Atrial Fibrillation and Acute Heart Failure in the Emergency Department" Medicina 59, no. 12: 2113. https://doi.org/10.3390/medicina59122113