
The Effect of Intraoperative Patient Positioning on the Success of Intertrochanteric Fracture Surgery in Older Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical and Radiological Assessment
2.2. Surgical Preparation
2.3. Nail Type
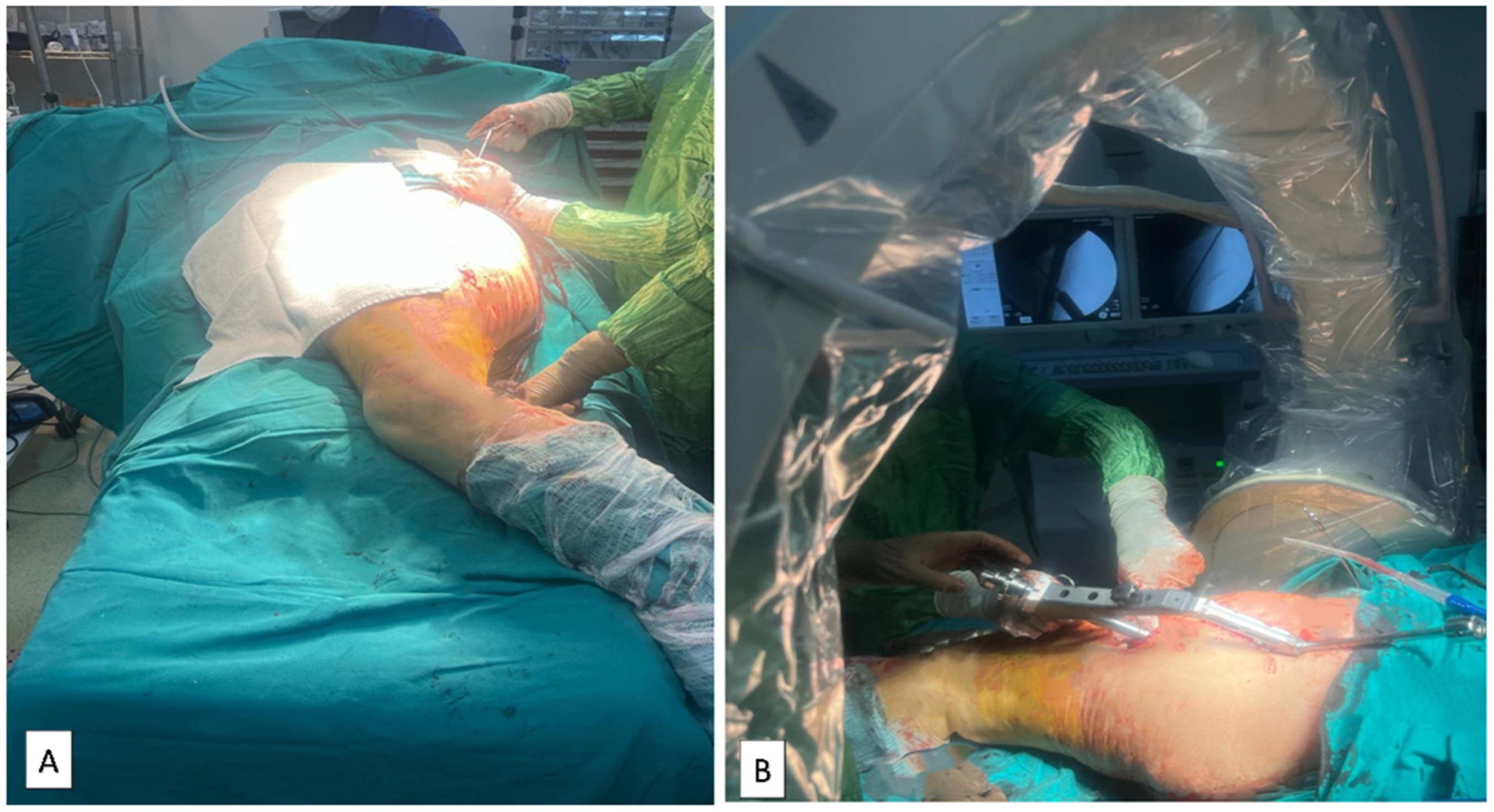
2.4. Supine Hemilithotomy Position
2.5. Using the Traction Table
2.6. Lateral Decubitus Position
2.7. Surgical Technique
2.8. Postoperative Management
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Russell, T.A.; Sanders, R. Pertrochanteric hip fractures: Time for change. J. Orthop. Trauma 2011, 25, 189–190. [Google Scholar] [CrossRef]
- Dimai, H.P.; Reichardt, B.; Zitt, E.; Concin, H.; Malle, O.; Fahrleitner-Pammer, A.; Svedbom, A.; Brozek, W. Thirty years of hip fracture incidence in Austria: Is the worst over? Osteoporos. Int. 2022, 33, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J. Epidemiology of osteoporotic fractures. Osteoporos. Int. 2005, 16 (Suppl. S2), S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Vig, K.S.; Adams, C.; Young, J.R.; Perloff, E.; O’Connor, C.M.; Czajka, C.M. Patient Positioning for Proximal Femur Fracture Fixation: A Review of Best Practices. Curr. Rev. Musculoskelet. Med. 2021, 14, 272–281. [Google Scholar] [CrossRef]
- Zhao, Z.; Song, F.; Zhu, J.; He, D.; Deng, J.; Ji, X.; Tang, P.; Pan, Y. Prone positioning for intramedullary nailing of subtrochanteric fractrures, the techniques of intraoperative fluoroscopy and reduction: A technique note. Injury 2017, 48, 2354–2359. [Google Scholar] [CrossRef]
- Li, D.Y.; Liu, C.G.; Zhang, K. Whether Assisted Intramedullary Nail Implantation without Traction Table is as Safe and Effective as Using Traction Table of Older Intertrochanteric Fracture Patients? Clin. Interv. Aging 2023, 18, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Boz, M.Ş.; Şahin, A.A. Lateral imaging technique of the femoral neck in a supine-semilithotomy position without a fracture table. Med. Sci. 2020, 9, 1061–1064. [Google Scholar] [CrossRef]
- Hutchings, L.; Fox, R.; Chesser, T. Proximal femoral fractures in the elderly: How are we measuring outcome? Injury 2011, 42, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Kashigar, A.; Vincent, A.; Gunton, M.J.; Backstein, D.; Safir, O.; Kuzyk, P.R. Predictors of failure for cephalomedullary nailing of proximal femoral fractures. Bone Jt. J. 2014, 96-B, 1029–1034. [Google Scholar] [CrossRef]
- Babhulkar, S.S. Management of trochanteric fractures. Indian J. Orthop. 2006, 40, 210–218. [Google Scholar] [CrossRef]
- Lorich, D.G.; Geller, D.S.; Nielson, J.H. Osteoporotic pertrochanteric hip fractures: Management and current controversies. Instr. Course Lect. 2004, 53, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; Hu, F.; Shen, J.; Zhang, L.; Zhang, L. Proximal femoral nail antirotation versus hemiarthroplasty: A study for the treatment of intertrochanteric fractures. Injury 2012, 43, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.R.; Kim, S.T.; Yoon, M.G.; Moon, M.S.; Heo, J.H. The stability score of the intramedullary nailed intertrochanteric fractures: Stability of nailed fracture and postoperative patient mobilization. Clin. Orthop. Surg. 2013, 5, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Zhang, K.; Qiang, M.; Chen, Y. The accuracy of intra-operative fluoroscopy in evaluating the reduction quality of intertrochanteric hip fractures. Int. Orthop. 2020, 44, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.C.; Oh, C.W.; Sim, J.A.; Oh, J.K. Intraoperative assessment of reduction quality during nail fixation of intertrochanteric fractures. Injury 2020, 51, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Baumgaertner, M.R.; Curtin, S.L.; Lindskog, D.M.; Keggi, J.M. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J. Bone. Jt. Surg. Am. 1995, 77, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Jiamton, C.; Boernert, K.; Babst, R.; Beeres, F.J.P.; Link, B.C. The nail-shaft-axis of the of proximal femoral nail antirotation (PFNA) is an important prognostic factor in the operative treatment of intertrochanteric fractures. Arch. Orthop. Trauma Surg. 2018, 138, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Marmor, M.; Liddle, K.; Buckley, J.; Matityahu, A. Effect of varus and valgus alignment on implant loading after proximal femur fracture fixation. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Turgut, A.; Kalenderer, O.; Karapinar, L.; Kumbaraci, M.; Akkan, H.A.; Agus, H. Which factor is most important for occurrence of cutout complications in patients treated with proximal femoral nail antirotation? Retrospective analysis of 298 patients. Arch. Orthop. Trauma Surg. 2016, 136, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Cepni, S.; Subasi, I.O.; Sahin, A.; Bozkurt, I.; Firat, A.; Kilicarslan, K. Tip-neck distance ratio as a novel predictor for failure in cephalomedullary nailing of unstable trochanteric fractures (UTF). Arch. Orthop. Trauma Surg. 2022, 142, 2619–2626. [Google Scholar] [CrossRef]
- John, B.; Sharma, A.; Mahajan, A.; Pandey, R. Tip-apex distance and other predictors of outcome in cephalomedullary nailing of unstable trochanteric fractures. J. Clin. Orthop. Trauma 2019, 10 (Suppl. S1), S88–S94. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Nakayama, S.; Hara, M.; Koizumi, W.; Itabashi, T.; Saito, M. Tip-Apex Distance Is Most Important of Six Predictors of Screw Cutout after Internal Fixation of Intertrochanteric Fractures in Women. JBJS Open Access 2017, 2, e0022. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.M.; Hou, Z.Y.; Hu, S.J.; Du, S.C. Intertrochanteric Femur Fracture Treatment in Asia: What We Know and What the World Can Learn. Orthop. Clin. N. Am. 2020, 51, 189–205. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.H.; Garg, A.K.; Oh, J.K.; Oh, C.W.; Lee, S.J.; Myung-Rae, C.; Kim, M.K.; Kim, H. A biomechanical evaluation of proximal femoral nail antirotation with respect to helical blade position in femoral head: A cadaveric study. Indian J. Orthop. 2012, 46, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Karapinar, L.; Turgut, A.; Kumbaraci, M.; Koca, A. Evaluation of the quadrants of femoral neck-head in the cephalomedullary fixation of intertrochanteric fractures with a helical blade: Is inferior posterior quadrant also safe? A clinical study. Jt. Dis. Relat. Surg. 2021, 32, 93–100. [Google Scholar] [CrossRef] [PubMed]
- De Bruijn, K.; den Hartog, D.; Tuinebreijer, W.; Roukema, G. Reliability of predictors for screw cutout in intertrochanteric hip fractures. J. Bone Jt. Surg. Am. 2012, 94, 1266–1272. [Google Scholar] [CrossRef] [PubMed]
- Jaffer, A.K.; Barsoum, W.K.; Krebs, V.; Hurbanek, J.G.; Morra, N.; Brotman, D.J. Duration of anesthesia and venous thromboembolism after hip and knee arthroplasty. Mayo Clin. Proc. 2005, 80, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Sahin, E.; Songur, M.; Kalem, M.; Zehir, S.; Aksekili, M.A.; Keser, S.; Bayar, A. Traction table versus manual traction in the intramedullary nailing of unstable intertrochanteric fractures: A prospective randomized trial. Injury 2016, 47, 1547–1554. [Google Scholar] [CrossRef] [PubMed]
- Sadeq, M.H.U.; Majeed, G.H.; Ali, H.O.H.; Al Bayati, M.A.; Aledanni, M.S. Fixation of unstable intertrochanteric fractures with proximal femoral nailing: Supine position with traction table versus lateral decubitus position. Rawal Med. J. 2023, 48, 863. [Google Scholar] [CrossRef]
- Kakumanu, R.K.; Kunadharaju, R.T.; Beesetty, M.; Golla, D. Ease of doing proximal femoral nailing in lateral position in the management of peri-trochanteric femoral fractures in adults: A prospective study. Int. J. Orthop. 2019, 5, 39–46. [Google Scholar] [CrossRef]
- ÖZGÜR, A.P.; POLAT, Ö. Comparison of Supine Position and Traction Table in the Surgical Treatment of Unstable Intertrochanteric Fractures with PFNA. J. Contemp. Med. 2023, 13, 561–565. [Google Scholar]
- Hoehmann, C.L.; Thompson, J.; Long, M.; DiVella, M.; Munnangi, S.; Ruotolo, C.; Galos, D.K. Unnecessary Preoperative Cardiology Evaluation and Transthoracic Echocardiogram Delays Time to Surgery for Geriatric Hip Fractures. J. Orthop. Trauma 2021, 35, 205–210. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modified Baumgaertner Criteria | ||
|---|---|---|
| 1. Alignment | 2. Displacement of Fragments | Reduction Quality |
| (a) Anteroposterior view: Normal or slight valgus neck–shaft angle (b) Lateral view: Less than 20° of angulation | (a) >80% overlap (b) <5 mm shortening | Good: Both criteria met Acceptable: Only one criterion met Poor: Neither criterion met |
| N | Mean ± SD | Median | Min-Max | ||
|---|---|---|---|---|---|
| Age | 170 | 77.8 ± 8.8 | 79 | 65–99 | |
| ASA score | 170 | 2.8 ± 0.7 | 3 | 1–4 | |
| Time between fracture and surgery (days) | 170 | 3.1 ± 2.3 | 2 | 1–10 | |
| Duration of surgery (minutes) | 170 | 110.6 ± 45.2 | 105 | 35–285 | |
| Duration of intensive care unit stay (days) | 170 | 2.4 ± 3.8 | 2 | 0–30 | |
| Duration of hospital stay (days) | 170 | 8.3 ± 4.5 | 7 | 0–31 | |
| Collodiaphyseal angle | 170 | 129.3 ± 6.7 | 130 | 110–146 | |
| TAD (mm) | 170 | 21.9 ± 9.1 | 20 | 9–74 | |
| Cut-out (days) | 11 | 39.5 ± 27.3 | 30 | 25–120 | |
| Gender | Male | 72(42.4%) | |||
| Female | 98(57.6%) | ||||
| Groups | Lateral decubitus | 45(26.5%) | |||
| Supine hemilithotomy | 46(27.1%) | ||||
| Traction table | 79(46.5%) | ||||
| AO Stable | 31A1.2 | 22(12.9%) | |||
| 31A1.3 | 34(20.5%) | ||||
| AO Unstable | 31A2.1 | 50(29.4%) | |||
| 31A2.2 | 14(8.2%) | ||||
| 31A2.3 | 37(21.7%) | ||||
| 31A3.1 | 7(4.1%) | ||||
| 31A3.3 | 5(2.9%) | ||||
| Variables | Category | Lateral Decubitus | Supine Hemilithotomy | Traction Table | p | |||
|---|---|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||||||
| Gender | Male | 26 (57.8) | 20 (43.5) | 26 (32.9) | 0.026 * | |||
| Female | 19 (42.2) | 26 (56.5) | 53 (67.1) | |||||
| Comorbidities | No | 18 (40) | 7 (15.2) | 4 (5.1) | <0.001 * | |||
| Yes | 27 (60) | 39 (84.8) | 75 (94.9) | |||||
| Number of comorbidities | 1 comorbidity | 8 (29.6) | 15 (38.5) | 24 (32) | 0.709 | |||
| 2 and more comorbidities | 19 (70.4) | 24 (61.5) | 51 (68) | |||||
| Modified Baumgaertner | Good | 18 (40) | 30 (65.2) | 46 (58.2) | 0.054 | |||
| Acceptable | 17 (37.8) | 14 (30.4) | 21 (26.6) | |||||
| Poor | 10 (22.2) | 2 (4.3) | 12 (15.2) | |||||
| Cut-out | No | 41 (91.1) | 42 (91.3) | 76 (96.2) | 0.418 | |||
| Yes | 4 (8.9) | 4 (8.7) | 3 (3.8) | |||||
| Complications | No | 34 | 75.6 | 42 | 91.3 | 79 | 100 | <0.001 * |
| Yes | 11 | 24.4 | 4 | 8.7 | 0 | 0 | ||
| Traction Table (N = 79) | Supine Hemilithotomy (N = 46) | Lateral Decubitus (N = 45) | p | pTT&SH | pTT&LD | pSH&LD | |
|---|---|---|---|---|---|---|---|
| Age | 78.5 ± 8.4 | 75.6 ± 8.2 | 76.9 ± 9.4 | 0.059 | - | - | |
| ASA score | 2.7 ± 0.6 | 3.1 ± 0.8 | 2.7 ± 0.6 | 0.006 | 0.002 | 0.392 | 0.022 |
| Time between fracture and surgery (days) | 4 (1–10) | 2 (0–5) | 1 (1–9) | 0.0001 | 0.0001 | 0.0001 | 0.935 |
| Duration of surgery (minutes) | 135 (45–285) | 95 (40–155) | 70 (35–180) | 0.0001 | 0.0001 | 0.0001 | 0.0001 |
| Duration of intensive care unit stay (days) | 0 (0–8) | 3 (0–30) | 2 (0–23) | 0.0001 | 0.0001 | 0.0001 | 0.803 |
| Duration of hospital stay (days) | 8 (3–24) | 7 (7–31) | 6 (3–26) | 0.680 | - | - | - |
| Collodiaphyseal angle | 129.5 ± 4.9 | 126.6 ± 5.7 | 133 (111–146) | 0.001 | 0.001 | 0.012 | 0.001 |
| TAD (mm) | 17 (9–30) | 26 (16–74) | 18.3 (9.5–49.1) | 0.0001 | 0.0001 | 0.322 | 0.0001 |
| AO Stable (n = 56) | AO Unstable (n = 114) | p | |
|---|---|---|---|
| Collodiaphyseal angle | 131.2 ± 5.2 | 128.4 ± 7.2 | 0.010 |
| TAD | 17.4 ± 5.4 | 24.1 ± 9.7 | 0.0001 |
| Cut-out | 4 (7.1) | 7 (6.1) | 0.753 |
| Modified Baumgaertner | |||
| Good | 36 (64.3) | 58 (50.9) | 0.239 |
| Poor | 7 (12.5) | 17 (14.9) | |
| Acceptable | 13 (23.2) | 39 (34.2) |
| Beta | SE of Beta | Odds Ratio | 95% CA | p | ||
|---|---|---|---|---|---|---|
| Age | −0.020 | 0.036 | 0.980 | 0.914–1.052 | 0.582 | |
| Gender | −1.264 | 0.798 | 0.283 | 0.059–1.350 | 0.113 | |
| ASA score | 0.425 | 0.466 | 1.530 | 0.613–3.816 | 0.362 | |
| Comorbidities (Yes/No) | 0.083 | 0.810 | 1.086 | 0.222–5.312 | 0.918 | |
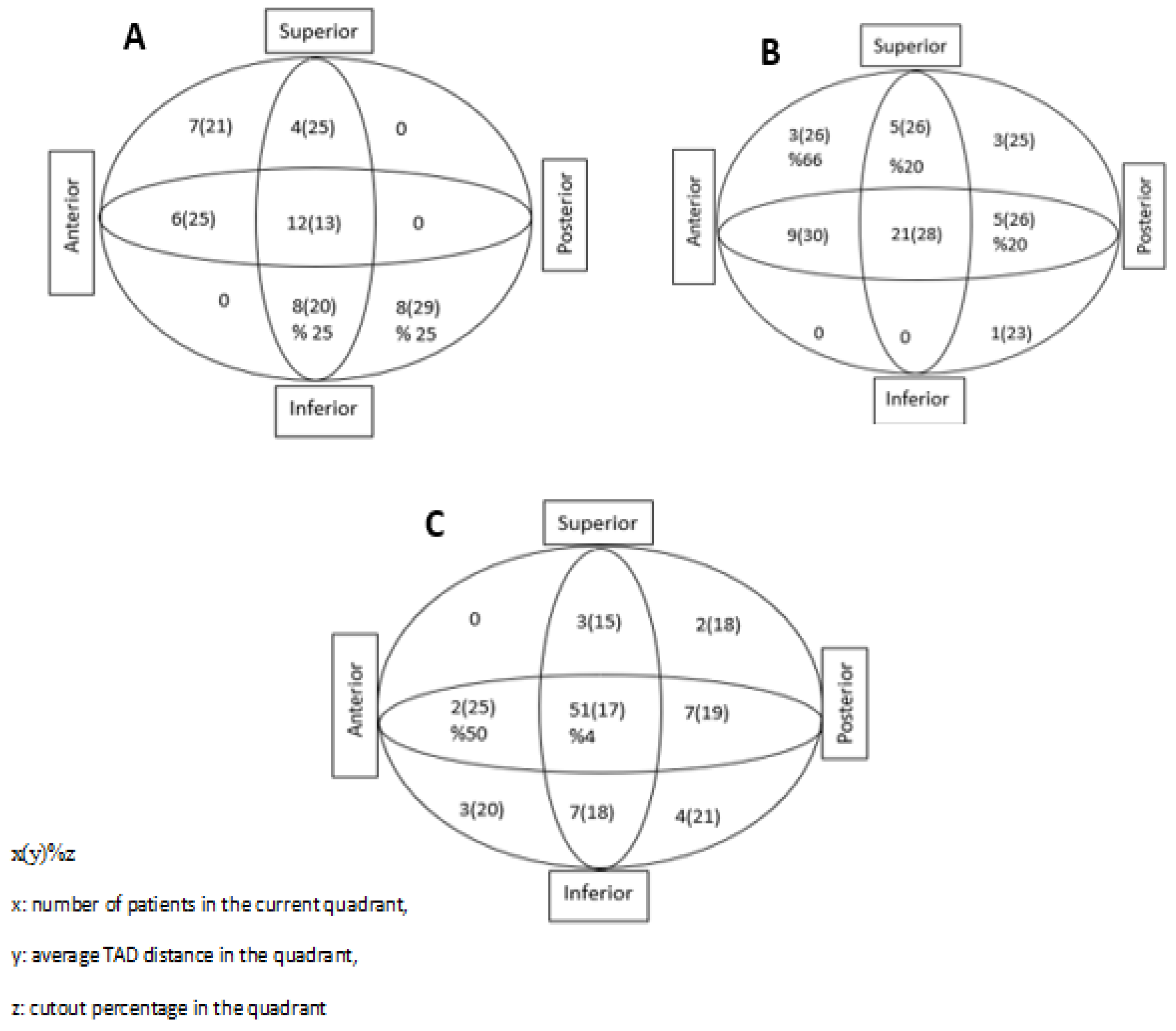
| Cleveland–Bosworth quadrant | 0.048 | 0.156 | 1.049 | 0.773–1.425 | 0.759 | |
| Modified Baumgaertner | Ref: Good | 0.003 * | ||||
| Acceptable | 0.193 | 0.930 | 1.213 | 0.196–7.505 | 0.835 | |
| Poor | 2.314 | 0.753 | 10.111 | 2.313–44.207 | 0.002 | |
| Collodiaphyseal angle | 0.085 | 0.049 | 1.089 | 0.988–1.199 | 0.085 | |
| Tip–apex distance | 0.022 | 0.030 | 1.022 | 0.964–1.083 | 0.470 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaya, O.; Kundakçı, B.; Önder, C.; Kurt, V.; Atmaca, E.; Tunç, F. The Effect of Intraoperative Patient Positioning on the Success of Intertrochanteric Fracture Surgery in Older Patients. Medicina 2024, 60, 646. https://doi.org/10.3390/medicina60040646
Kaya O, Kundakçı B, Önder C, Kurt V, Atmaca E, Tunç F. The Effect of Intraoperative Patient Positioning on the Success of Intertrochanteric Fracture Surgery in Older Patients. Medicina. 2024; 60(4):646. https://doi.org/10.3390/medicina60040646
Chicago/Turabian StyleKaya, Onur, Buğra Kundakçı, Cem Önder, Vahap Kurt, Emre Atmaca, and Fatih Tunç. 2024. "The Effect of Intraoperative Patient Positioning on the Success of Intertrochanteric Fracture Surgery in Older Patients" Medicina 60, no. 4: 646. https://doi.org/10.3390/medicina60040646