
Retrospective Evaluation of the Effect of Lumbar Sympathetic Blockade on Pain Scores, Fontaine Classification, and Collateral Perfusion Status in Patients with Lower Extremity Peripheral Arterial Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics, Consent, and Permissions
2.2. Patient Selection
- To have a diagnosis of PAD in lower extremities that could not be treated with conservative treatment (painkillers or vasodilator drugs and regular walking exercise) or revascularization procedures,
- To have received an LSB procedure with a combination of local anesthetics and steroids,
- To be a Stage III and/or IV according to the Fontaine Classification,
- To have been evaluated by Fontaine Classification, the Numeric Rating Scale (NRS), and the Pain Detect Questionnaire (PDQ) score before the procedure and at the first, third, and sixth month after the procedure,
- To have the treated lower extremities examined with arterial Doppler US at and before the first, third, and sixth month after the procedure.
2.3. Assessment before the Lumbar Sympathetic Block
2.4. Procedure of Lumbar Sympathetic Block
2.5. Follow-Up and Evaluation after Lumbar Sympathetic Block
2.6. Power and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Criqui, M.H.; Matsushita, K.; Aboyans, V.; Hess, C.N.; Hicks, C.W.; Kwan, T.W.; McDermott, M.M.; Misra, S.; Ujueta, F.; on behalf of the American Heart Association Council on Epidemiology and Prevention; et al. Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement from the American Heart Association. Circulation 2021, 144, 171–191. [Google Scholar] [CrossRef]
- Signorelli, S.S.; Vanella, L.; Abraham, N.G.; Scuto, S.; Marino, E.; Rocic, P. Pathophysiology of chronic peripheral ischemia: New perspectives. Ther. Adv. Chronic Dis. 2020, 11, 2040622319894466. [Google Scholar] [CrossRef]
- Shu, J.; Santulli, G. Update on peripheral artery disease: Epidemiology and evidence-based facts. Atherosclerosis 2018, 275, 379–381. [Google Scholar] [CrossRef]
- Gardner, A.W.; Afaq, A. Management of lower extremity peripheral arterial disease. J. Cardiopulm. Rehabil. Prev. 2008, 28, 349–357. [Google Scholar] [CrossRef]
- Muller, M.D.; Reed, A.B.; Leuenberger, U.A.; Sinoway, L.I. Physiology in medicine: Peripheral arterial disease. J. Appl. Physiol. 2013, 115, 1219–1226. [Google Scholar] [CrossRef]
- Kulkarni, K.; Kulkarni, R. Chemical Neurolysis and Radiofrequency Ablation of Lumbar Sympathetic Ganglion in Peripheral Vascular Diseases of the Lower Limbs. In Novel Approaches in Regional Anesthesia & Pain Management; Open Access eBooks: Las Vegas, NV, USA, 2021; pp. 1–16. [Google Scholar]
- Cerqueira, L.O.; Duarte, E.G.; Barros, A.L.S.; Cerqueira, J.R.; de Araújo, W.J.B. WIfI classification: The Society for Vascular Surgery lower extremity threatened limb classification system, a literature review. J. Vasc. Bras. 2020, 19, 20190070. [Google Scholar] [CrossRef]
- Cruccu, G.; Sommer, C.; Anand, P.; Attal, N.; Baron, R.; Garcia-Larrea, L.; Haanpaa, M.; Jensen, T.S.; Serra, J.; Treede, R. EFNS guidelines on neuropathic pain assessment: Revised 2009. Eur. J. Neurol. 2010, 17, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Martin, B.; Marianne, B.; Tina, C.; Jean-Philippe, C.; Martin, C.; Marco, D.C.; Sebastian, D.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: The European Stroke Organization (ESO) The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [PubMed]
- Joo, E.Y.; Kong, Y.G.; Lee, J.; Cho, H.S.; Kim, S.H.; Suh, J.H. Change in pulse transit time in the lower extremity after lumbar sympathetic ganglion block: An early indicator of successful block. J. Int. Med. Res. 2017, 45, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Nahm, F.S.; Kim, Y.C.; Lee, S.C.; Sim, S.E.; Lee, S.J. The cut-off rate of skin temperature changes to confirm successful lumbar sympathetic block. J. Int. Med. Res. 2010, 38, 266–275. [Google Scholar] [CrossRef]
- Day, M. Sympathetic blocks: The evidence. Pain. Pract. 2008, 8, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Cahana, A.; Van Zundert, J.; Macrea, L.; van Kleef, M.; Sluijter, M. Pulsed radiofrequency: Current clinical and biological literature available. Pain Med. 2006, 7, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef] [PubMed]
- Gunduz, O.H.; Kenis-Coskun, O. Ganglion blocks as a treatment of pain: Current perspectives. J. Pain Res. 2017, 10, 2815–2826. [Google Scholar] [CrossRef] [PubMed]
- Punj, J.; Marada, S. Ultrasound lumbar sympathetic block: Out of plane approach with insulated stimulation needle-Case series of three patients. Indian J. Anaesth. 2020, 64, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Marada, S.; Punj, J.; Dhar, A.; Bhoi, D.; Mohan, V.; Trikha, A.; Pandey, R.K.; Darlong, V. To Assess Technical Feasibility of Ultrasound Lumbar Sympathetic Block with Electrical Stimulation Needle in Out of Plane Needle Orientation: A Prospective Interventional Study. Pain Med. 2021, 23, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Chahal, A.; Malla, S.; Sharma, S.; Chumber, S.; Madhusudhan, K.S. CT-Guided Lumbar Sympathectomy as a Last Option for Chronic Limb-Threatening Ischemia of the Lower Limbs: Evaluation of Technical Factors and Long-Term Outcomes. AJR Am. J. Roentgenol. 2021, 216, 1273–1282. [Google Scholar] [CrossRef] [PubMed]
- Dominkus, M.; Bauer, R.; Kepplinger, B.; Malikpur, G. Percutaneous radio-frequency sympathetic block in peripheral circulatory disorders. Vasa Suppl. 1990, 30, 152–156. [Google Scholar]
- Singh, R.; Kulkarni, R.; Kulkarni, K.; Chavannavar, K. Evaluation of The Radiofrequency Ablation of Lumbar Sympathetic Ganglia In Lower Limb Ischemic Ulcers In Indian Population: Radiofrequency Ablation and Lower Limb Ischemic Ulcers. Int. J. Med. Surg. Sci. 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Gleim, M.; Maier, C.; Melchert, U. Lumbar neurolytic sympathetic blockades provide immediate and long-lasting improvement of painless walking distance and muscle metabolism in patients with severe peripheral vascular disease. J. Pain Symptom Manag. 1995, 10, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Yeo, J.S.; Kim, S.O.; Park, Y.H. Sympathetic block for treating primary erythromelalgia. Korean J. Pain 2010, 23, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Kirksey, M.A.; Haskins, S.C.; Cheng, J.; Liu, S.S. Local Anesthetic Peripheral Nerve Block Adjuvants for Prolongation of Analgesia: A Systematic Qualitative Review. PLoS ONE 2015, 10, 0137312. [Google Scholar] [CrossRef]
- Spiegel, M.A.; Hingula, L.; Chen, G.H.; Legler, A.; Puttanniah, V.; Gulati, A. The Use of L2 and L3 Lumbar Sympathetic Blockade for Cancer-Related Pain, an Experience and Recommendation in the Oncologic Population. Pain Med. 2020, 21, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; He, M.; Pang, J.; Guo, X.; Huo, Y.; Ma, J. Continuous Lumbar Sympathetic Blockade Enhances the Effect of Lumbar Sympatholysis on Refractory Diabetic Neuropathy: A Randomized Controlled Trial. Diabetes Ther. 2020, 11, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, E.C.; Sencan, S.; Gunduz, O.H. Lumbar Sympathetic Block for Intractable Lower-Limb Postherpetic Neuralgia: Report of Two Cases. Pain Pract. 2021, 21, 353–356. [Google Scholar] [CrossRef]
- Kalka, C.; Baumgartner, I. Gene and stem cell therapy in peripheral arterial occlusive disease. Vasc. Med. 2008, 13, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.M.; Zurakowski, D.; Berde, C.B.; Sethna, N.F. Lumbar sympathetic blockade in children with complex regional pain syndromes: A double blind placebo-controlled crossover trial. Anesthesiology 2009, 111, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Baek, H.J.; Park, K.S.; Kim, Y.C. Photoplethysmographic signals to predict the success of lumbar sympathetic blockade for lower extremity pain. J. Int. Med. Res. 2014, 42, 938–948. [Google Scholar] [CrossRef]
- Kanao-Kanda, M.; Kanda, H.; Iida, T.; Kikuchi, S.; Azuma, N. Clinical Application of Laser Speckle Flowgraphy to Assess Changes in Blood Flow to the Foot After a Lumbar Sympathetic Ganglion Block: A Case Report. J. Pain Res. 2021, 14, 1451–1456. [Google Scholar] [CrossRef]
- Biscetti, F.; Pecorini, G.; Straface, G.; Arena, V.; Stigliano, E.; Rutella, S.; Locatelli, F.; Angelini, F.; Ghirlanda, G.; Flex, A. Cilostazol promotes angiogenesis after peripheral ischemia through a VEGF-dependent mechanism. Int. J. Cardiol. 2013, 167, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.E.; De Jesus, O.; Varacallo, M. Lumbar Sympathetic Block. 1 May 2022. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | n = 21 |
|---|---|
| Age a | 60.2 ± 11.2 61.0 (41.0–86.0) |
| Gender b | |
| Male | 17 (81.0) |
| Female | 4 (19.0) |
| Height (cm) a | 170.4 ± 8.1 170.0 (156.0–185.0) |
| Weight (kg) a | 79.0 ± 12.2 81.0 (57.0–98.0) |
| Body mass index a | 27.1 ± 3.5 27.1 (19.7–32.8) |
| Symptomatic period (year) a | 4.7 ± 5.1 2.0 (1.0–20.0) |
| Before the Procedure | First Month | Third Month | Sixth Month | p Value | |
|---|---|---|---|---|---|
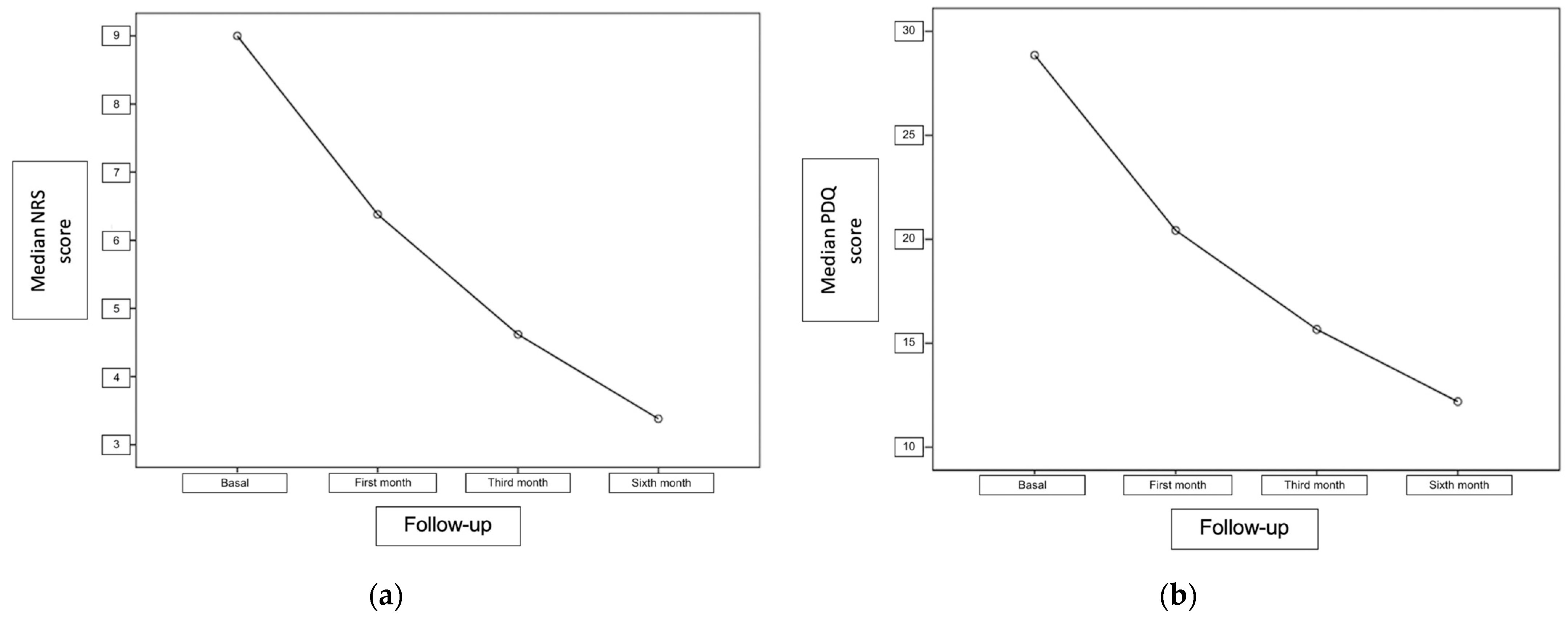
| NRS | 9.0 ± 1.1 9.0 (6.0–10) | 6.3 ± 1.3 6.0 (4.0–9.0) | 4.6 ± 1.5 5.0(2.0–7.0) | 3.3 ± 1.9 3.0 (0.0–7.0) | <0.001 |
| PDQ | 28.8 ± 6.1 30 (14–37) | 20.4 ± 5.1 21 (10–28) | 15.6 ± 5.3 15 (6–28) | 12.1 ± 4.8 11 (2–24) | <0.001 |
| Before the Procedure | First Month | Third Month | Sixth Month | p Value | |
|---|---|---|---|---|---|
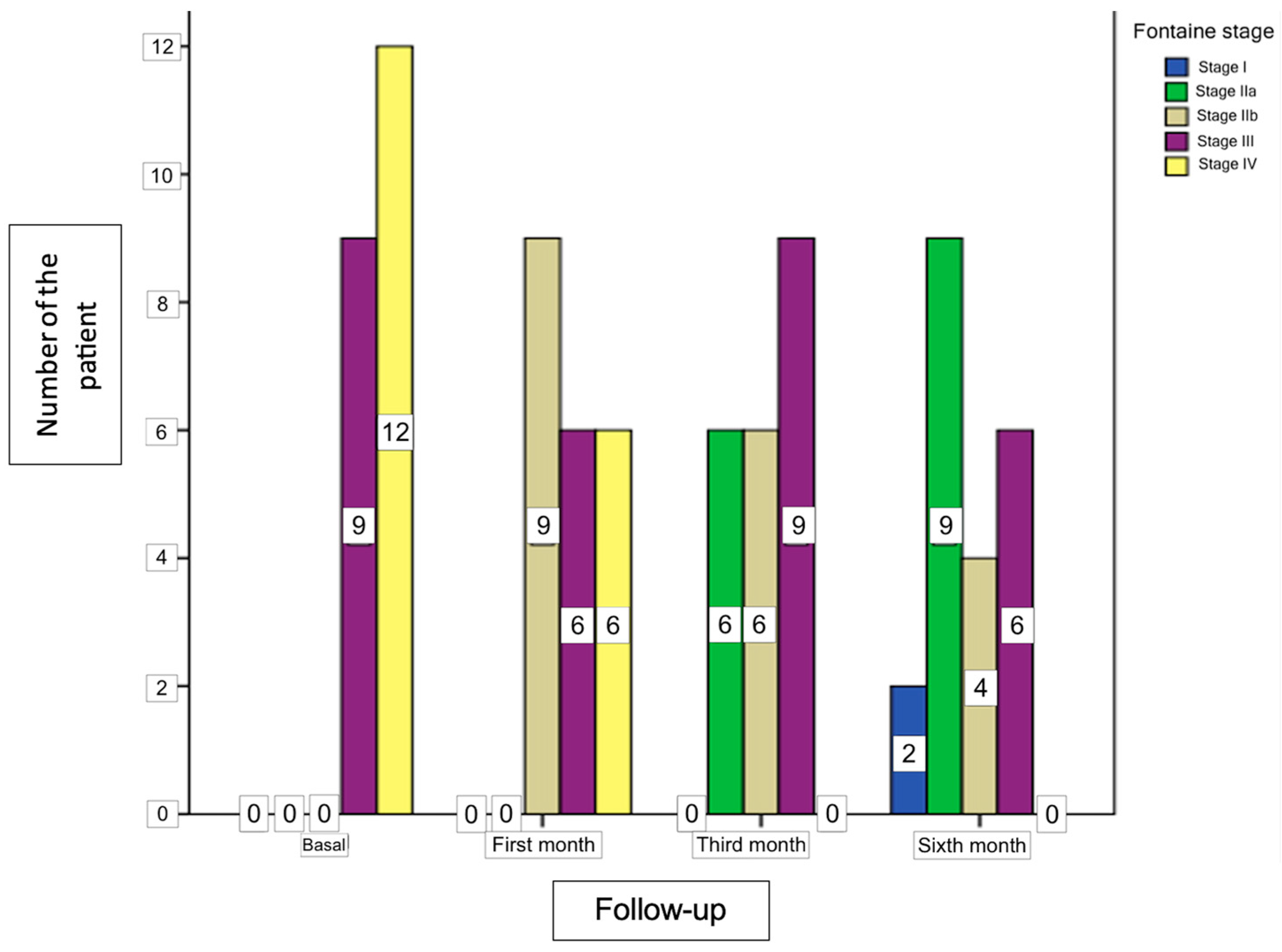
| Fontaine Stages | <0.001 | ||||
| Stage I | - | - | - | 2 (9.5%) | |
| Stage IIa | - | - | 6 (28.6%) | 9 (42.9%) | |
| Stage IIb | - | 9 (42.9%) | 6 (28.6%) | 4 (19.0%) | |
| Stage III | 9 (42.9%) | 6 (28.6%) | 9 (42.9%) | 6 (28.6%) | |
| Stage IV | 12 (57.1%) | 6 (28.6%) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keser-Pehlivan, C.; Kucukbingoz, C.; Pehlivan, U.A.; Balli, H.T.; Unlugenc, H.; Ozbek, H.T. Retrospective Evaluation of the Effect of Lumbar Sympathetic Blockade on Pain Scores, Fontaine Classification, and Collateral Perfusion Status in Patients with Lower Extremity Peripheral Arterial Disease. Medicina 2024, 60, 682. https://doi.org/10.3390/medicina60050682
Keser-Pehlivan C, Kucukbingoz C, Pehlivan UA, Balli HT, Unlugenc H, Ozbek HT. Retrospective Evaluation of the Effect of Lumbar Sympathetic Blockade on Pain Scores, Fontaine Classification, and Collateral Perfusion Status in Patients with Lower Extremity Peripheral Arterial Disease. Medicina. 2024; 60(5):682. https://doi.org/10.3390/medicina60050682
Chicago/Turabian StyleKeser-Pehlivan, Celalet, Cagatay Kucukbingoz, Umur Anil Pehlivan, Huseyin Tugsan Balli, Hakki Unlugenc, and Hayri Tevfik Ozbek. 2024. "Retrospective Evaluation of the Effect of Lumbar Sympathetic Blockade on Pain Scores, Fontaine Classification, and Collateral Perfusion Status in Patients with Lower Extremity Peripheral Arterial Disease" Medicina 60, no. 5: 682. https://doi.org/10.3390/medicina60050682