Prognostic Role of Basal Serum Alpha-Fetoprotein in Patients with Hepatocellular Carcinoma Suitable for Curative Treatment

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. HCC Assessment and Follow-Up
2.3. Outcome Measures
2.4. Study Objectives
- To correlate the different AFP cut-offs with the other outcome measures;
- To correlate the AFP cut-offs with the baseline clinical variables.
2.5. Statistical Analysis
3. Results
3.1. Baseline Features
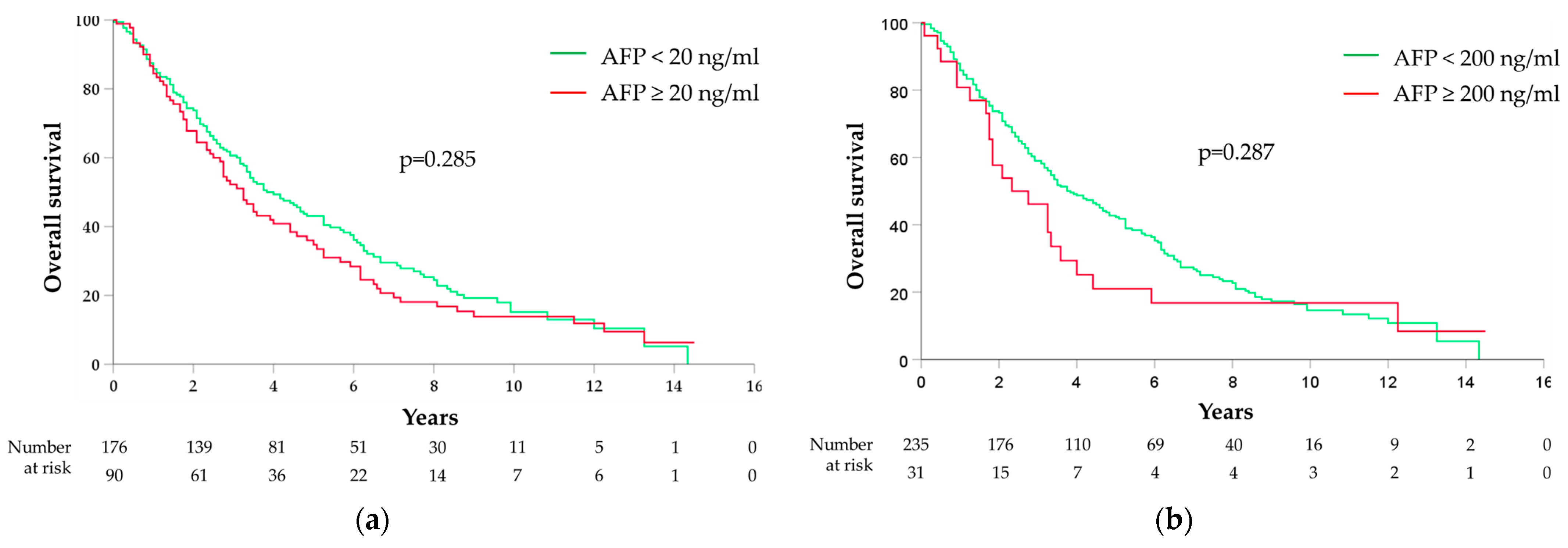
3.2. Correlations between AFP and Survival
3.3. Correlations between AFP and HCC Recurrence
3.4. Correlations between AFP and Baseline Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rumgay, H.; Ferlay, J.; de Martel, C.; Georges, D.; Ibrahim, A.S.; Zheng, R.; Wei, W.; Lemmens, V.; Soerjomataram, I. Global, regional and national burden of primary liver cancer by subtype. Eur. J. Cancer 2022, 161, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, M.J.; Arnold, M.; Bardot, A.; Ferlay, J.; De, P.; Tervonen, H.; Little, A.; Bucher, O.; St Jacques, N.; Gavin, A.; et al. Comparison of liver cancer incidence and survival by subtypes across seven high-income countries. Int. J. Cancer 2021, 149, 2020–2031. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Toh, M.R.; Wong, E.Y.T.; Wong, S.H.; Ng, A.W.T.; Loo, L.H.; Chow, P.K.; Ngeow, J. Global Epidemiology and Genetics of Hepatocellular Carcinoma. Gastroenterology 2023, 164, 766–782. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; El-Serag, H.B.; Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Sandhu, S.; Lai, J.P.; Sandhu, D.S. Hepatocellular carcinoma in non-cirrhotic liver: A comprehensive review. World J. Hepatol. 2019, 11, 1. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Llovet, J.M.; Yarchoan, M.; Mehta, N.; Heimbach, J.K.; Dawson, L.A.; Jou, J.H.; Kulik, L.M.; Agopian, V.G.; Marrero, J.A.; et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology 2023, 78, 1922–1965. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Nolsoe, C.P.; Barr, R.G.; Berzigotti, A.; Burns, P.N.; Cantisani, V.; Chammas, M.C.; Chaubal, N.; Choi, B.I.; Clevert, D.A.; et al. Guidelines and Good Clinical Practice Recommendations for Contrast-Enhanced Ultrasound (CEUS) in the Liver-Update 2020 WFUMB in Cooperation with EFSUMB, AFSUMB, AIUM, and FLAUS. Ultrasound Med. Biol. 2020, 46, 2579–2604. [Google Scholar] [CrossRef]
- Daniele, B.; Mauro Borzio, A.E.B.; Fiore, F.; Daniele, G.; Cabibbo, G.; Casadei Gardini, A.; Gian Grazi, L.; Lorenza Rimassa, L.; Dionisi, F.; ASSOCIAZIONE ITALIANA ONCOLOGIA MEDICA. Linee Guida AIOM Epatocarcinoma. 2020. Available online: https://www.aiom.it/linee-guida-aiom-2020-epatocarcinoma/ (accessed on 1 February 2023).
- Llovet, J.M.; Bru, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Gitlin, D.; Perricelli, A.; Gitlin, G.M. Synthesis of -fetoprotein by liver, yolk sac, and gastrointestinal tract of the human conceptus. Cancer Res. 1972, 32, 979–982. [Google Scholar] [PubMed]
- Ball, D.; Rose, E.; Alpert, E. Alpha-fetoprotein levels in normal adults. Am. J. Med. Sci. 1992, 303, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Masseyeff, R.; Gilli, J.; Krebs, B.; Calluaud, A.; Bonet, C. Evolution of alpha-fetoprotein serum levels throughout life in humans and rats, and during pregnancy in the rat. Ann. N. Y. Acad. Sci. 1975, 259, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.L.; Mo, F.; Johnson, P.J.; Siu, D.Y.; Chan, M.H.; Lau, W.Y.; Lai, P.B.; Lam, C.W.; Yeo, W.; Yu, S.C. Performance of serum alpha-fetoprotein levels in the diagnosis of hepatocellular carcinoma in patients with a hepatic mass. HPB 2014, 16, 366–372. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, K.H. New Blood Biomarkers for the Diagnosis of AFP-Negative Hepatocellular Carcinoma. Front. Oncol. 2020, 10, 1316. [Google Scholar] [CrossRef]
- Carr, B.I.; Akkiz, H.; Uskudar, O.; Yalcin, K.; Guerra, V.; Kuran, S.; Karaogullarindan, U.; Altintas, E.; Ozakyol, A.; Tokmak, S.; et al. HCC with low- and normal-serum alpha-fetoprotein levels. Clin. Pract. 2018, 15, 453–464. [Google Scholar] [CrossRef]
- Schutte, K.; Schulz, C.; Link, A.; Malfertheiner, P. Current biomarkers for hepatocellular carcinoma: Surveillance, diagnosis and prediction of prognosis. World J. Hepatol. 2015, 7, 139–149. [Google Scholar] [CrossRef]
- Liu, L.; Zhao, Y.; Jia, J.; Chen, H.; Bai, W.; Yang, M.; Yin, Z.; He, C.; Zhang, L.; Guo, W.; et al. The Prognostic Value of Alpha-Fetoprotein Response for Advanced-Stage Hepatocellular Carcinoma Treated with Sorafenib Combined with Transarterial Chemoembolization. Sci. Rep. 2016, 6, 19851. [Google Scholar] [CrossRef]
- Agopian, V.G.; Harlander-Locke, M.P.; Markovic, D.; Zarrinpar, A.; Kaldas, F.M.; Cheng, E.Y.; Yersiz, H.; Farmer, D.G.; Hiatt, J.R.; Busuttil, R.W. Evaluation of Patients With Hepatocellular Carcinomas That Do Not Produce alpha-Fetoprotein. JAMA Surg. 2017, 152, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Nomura, F.; Ohnishi, K.; Tanabe, Y. Clinical features and prognosis of hepatocellular carcinoma with reference to serum alpha-fetoprotein levels. Analysis of 606 patients. Cancer 1989, 64, 1700–1707. [Google Scholar] [CrossRef] [PubMed]
- A new prognostic system for hepatocellular carcinoma: A retrospective study of 435 patients: The Cancer of the Liver Italian Program (CLIP) investigators. Hepatology 1998, 28, 751–755. [CrossRef] [PubMed]
- Borzio, M.; Dionigi, E.; Rossini, A.; Marignani, M.; Sacco, R.; De Sio, I.; Bertolini, E.; Francica, G.; Giacomin, A.; Parisi, G.; et al. External validation of the ITA.LI.CA prognostic system for patients with hepatocellular carcinoma: A multicenter cohort study. Hepatology 2018, 67, 2215–2225. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Singal, A.G. Surveillance for Hepatocellular Carcinoma: Current Best Practice and Future Direction. Gastroenterology 2019, 157, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Daniele, B.; Bencivenga, A.; Megna, A.S.; Tinessa, V. Alpha-fetoprotein and ultrasonography screening for hepatocellular carcinoma. Gastroenterology 2004, 127, S108–S112. [Google Scholar] [CrossRef] [PubMed]
- Hakeem, A.R.; Young, R.S.; Marangoni, G.; Lodge, J.P.; Prasad, K.R. Systematic review: The prognostic role of alpha-fetoprotein following liver transplantation for hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2012, 35, 987–999. [Google Scholar] [CrossRef] [PubMed]
- Jearth, V.; Patil, P.S.; Mehta, S.; Sundaram, S.; Seth, V.; Goel, M.; Patkar, S.; Bal, M.; Rao, V. Correlation of Clinicopathological Profile, Prognostic Factors, and Survival Outcomes with Baseline Alfa-Fetoprotein Levels in Patients With Hepatocellular Carcinoma: A Biomarker that is Bruised but Not Broken. J. Clin. Exp. Hepatol. 2022, 12, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Liu, P.H.; Lee, Y.H.; Hsia, C.Y.; Huang, Y.H.; Lin, H.C.; Chiou, Y.Y.; Lee, F.Y.; Huo, T.I. Using serum alpha-fetoprotein for prognostic prediction in patients with hepatocellular carcinoma: What is the most optimal cutoff? PLoS ONE 2015, 10, e0118825. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; Board, W.C.o.T.E. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Associazione Italiana Oncologia Medica (AIOM). I NUMERI DEL CANCRO IN ITALIA 2023. Available online: https://www.aiom.it/i-numeri-del-cancro-in-italia/ (accessed on 1 February 2023).
- Wang, C.Y.; Li, S. Clinical characteristics and prognosis of 2887 patients with hepatocellular carcinoma: A single center 14 years experience from China. Medicine 2019, 98, e14070. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Kang, S.; Lee, J.; Choi, Y.; Kim, H.C.; Chung, J.W. Prognostication and risk factor stratification for survival of patients with hepatocellular carcinoma: A nationwide big data analysis. Sci. Rep. 2023, 13, 10388. [Google Scholar] [CrossRef] [PubMed]
- Biolato, M.; Gallusi, G.; Iavarone, M.; Cabibbo, G.; Racco, S.; De Santis, A.; Corte, C.D.; Maida, M.; Attili, A.F.; Sangiovanni, A.; et al. Prognostic ability of BCLC-B Subclassification in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. Ann. Hepatol. 2018, 17, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.P.; Gorman, R.A.; Berger, N.G.; Tsai, S.; Christians, K.K.; Clarke, C.N.; Mogal, H.; Gamblin, T.C. The prognostic utility of baseline alpha-fetoprotein for hepatocellular carcinoma patients. J. Surg. Oncol. 2017, 116, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.Q.; Fan, Z.Q.; Wang, M.D.; Diao, Y.K.; Chen, T.H.; Zeng, Y.Y.; Chen, Z.; Wang, X.M.; Zhou, Y.H.; Li, J.; et al. Prognostic Value of Serum α-Fetoprotein Level as an Important Characteristic of Tumor Biology for Patients Undergoing Liver Resection of Early-Stage Hepatocellular Carcinoma (BCLC Stage 0/A): A Large Multicenter Analysis. Ann. Surg. Oncol. 2024, 31, 1219–1231. [Google Scholar] [CrossRef] [PubMed]
- Bai, D.S.; Zhang, C.; Chen, P.; Jin, S.J.; Jiang, G.Q. The prognostic correlation of AFP level at diagnosis with pathological grade, progression, and survival of patients with hepatocellular carcinoma. Sci. Rep. 2017, 7, 12870. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Garcia-Tsao, G. Prognostic indicators in hepatocellular carcinoma: A systematic review of 72 studies. Liver Int. 2009, 29, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.Y.; Chen, W.J.; Lai, P.L.; Jeng, Y.M.; Sheu, J.C.; Hsu, H.C. High alpha-fetoprotein level correlates with high stage, early recurrence and poor prognosis of hepatocellular carcinoma: Significance of hepatitis virus infection, age, p53 and beta-catenin mutations. Int. J. Cancer 2004, 112, 44–50. [Google Scholar] [CrossRef]
- Tangkijvanich, P.; Anukulkarnkusol, N.; Suwangool, P.; Lertmaharit, S.; Hanvivatvong, O.; Kullavanijaya, P.; Poovorawan, Y. Clinical characteristics and prognosis of hepatocellular carcinoma: Analysis based on serum alpha-fetoprotein levels. J. Clin. Gastroenterol. 2000, 31, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Sternby Eilard, M.; Holmberg, E.; Naredi, P.; Söderdahl, G.; Rizell, M. Addition of alfa fetoprotein to traditional criteria for hepatocellular carcinoma improves selection accuracy in liver transplantation. Scand. J. Gastroenterol. 2018, 53, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Cheng, A.L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Matsui, O.; Izumi, N.; Iijima, H.; Kadoya, M.; Imai, Y.; Okusaka, T.; Miyayama, S.; Tsuchiya, K.; Ueshima, K.; et al. JSH Consensus-Based Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma: 2014 Update by the Liver Cancer Study Group of Japan. Liver Cancer 2014, 3, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Jiang, L.; Yuan, Y.; Huang, X.; Yang, X.; Hochwald, S.; Liu, J.; Huang, H. A comparison of clinical pathologic characteristics between alpha-fetoprotein negative and positive hepatocellular carcinoma patients from Eastern and Southern China. BMC Gastroenterol. 2022, 22, 202. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Q.; Wang, A.J.; Zhang, T.T.; Chen, S.H. Association of alpha-fetoprotein and metastasis for small hepatocellular carcinoma: A propensity-matched analysis. Sci. Rep. 2022, 12, 15676. [Google Scholar] [CrossRef] [PubMed]
- Katyal, S.; Oliver, J.H.; Peterson, M.S.; Ferris, J.V.; Carr, B.S.; Baron, R.L. Extrahepatic metastases of hepatocellular carcinoma. Radiology 2000, 216, 698–703. [Google Scholar] [CrossRef]
- Yokoo, T.; Patel, A.D.; Lev-Cohain, N.; Singal, A.G.; Yopp, A.C.; Pedrosa, I. Extrahepatic metastasis risk of hepatocellular carcinoma based on α-fetoprotein and tumor staging parameters at cross-sectional imaging. Cancer Manag. Res. 2017, 9, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Shinkawa, H.; Tanaka, S.; Kabata, D.; Takemura, S.; Amano, R.; Kimura, K.; Kinoshita, M.; Kubo, S. The Prognostic Impact of Tumor Differentiation on Recurrence and Survival after Resection of Hepatocellular Carcinoma Is Dependent on Tumor Size. Liver Cancer 2021, 10, 461–472. [Google Scholar] [CrossRef]
- Minagawa, M.; Ikai, I.; Matsuyama, Y.; Yamaoka, Y.; Makuuchi, M. Staging of hepatocellular carcinoma: Assessment of the Japanese TNM and AJCC/UICC TNM systems in a cohort of 13,772 patients in Japan. Ann. Surg. 2007, 245, 909–922. [Google Scholar] [CrossRef]
- Goh, B.K.; Teo, J.Y.; Chan, C.Y.; Lee, S.Y.; Jeyaraj, P.; Cheow, P.C.; Chow, P.K.; Ooi, L.L.; Chung, A.Y. Importance of tumor size as a prognostic factor after partial liver resection for solitary hepatocellular carcinoma: Implications on the current AJCC staging system. J. Surg. Oncol. 2016, 113, 89–93. [Google Scholar] [CrossRef]
- Peng, Y.; Qi, X.; Guo, X. Child-Pugh Versus MELD Score for the Assessment of Prognosis in Liver Cirrhosis: A Systematic Review and Meta-Analysis of Observational Studies. Medicine 2016, 95, e2877. [Google Scholar] [CrossRef] [PubMed]
- Cholongitas, E.; Papatheodoridis, G.V.; Vangeli, M.; Terreni, N.; Patch, D.; Burroughs, A.K. Systematic review: The model for end-stage liver disease--should it replace Child-Pugh’s classification for assessing prognosis in cirrhosis? Aliment. Pharmacol. Ther. 2005, 22, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Durand, F.; Valla, D. Assessment of prognosis of cirrhosis. Semin. Liver Dis. 2008, 28, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Kogo, M.; Kano, A.; Kiuchi, Y.; Mitamura, K.; Yoneyama, K. Prognostic index for survival in patients after treatment for primary hepatocellular carcinoma. Dig. Dis. Sci. 2007, 52, 2444–2451. [Google Scholar] [CrossRef]
- Nam, J.Y.; Lee, Y.B.; Lee, J.H.; Yu, S.J.; Kim, H.C.; Chung, J.W.; Yoon, J.H.; Kim, Y.J. A Prognostic Prediction Model of Transarterial Radioembolization in Hepatocellular Carcinoma: SNAP-HCC. Dig. Dis. Sci. 2022, 67, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Karaoğullarindan, Ü.; Gümürdülü, Y.; Üsküdar, O.; Odabaş, E.; Güler, H.S.; Tozluklu, N.; Bağir, E.; Kuran, S. Prognostic value and morphological findings of overexpression of glypican-3 in hepatocellular carcinoma. Eur. J. Gastroenterol. Hepatol. 2023, 35, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.J.; Li, Y.N.; Shu, C.; Yang, H.Y.; Huang, Z.; Tao, R.; Chen, Y.Y.; Chen, X.P.; Xiao, W. Prognostic value of preoperative circulating tumor cells for hepatocellular carcinoma with portal vein tumor thrombosis: A propensity score analysis. J. Cancer Res. Clin. Oncol. 2023, 149, 8981–8991. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Yu, J.I.; Park, H.C.; Hong, J.Y.; Lim, H.Y.; Goh, M.J.; Paik, Y.H. Nomogram for predicting overall survival in patients with large (>5 cm) hepatocellular carcinoma based on real-world practice. J. Liver Cancer 2023, 23, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Farinati, F.; Marino, D.; De Giorgio, M.; Baldan, A.; Cantarini, M.; Cursaro, C.; Rapaccini, G.; Del Poggio, P.; Di Nolfo, M.A.; Benvegnù, L.; et al. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: Both or neither? Am. J. Gastroenterol. 2006, 101, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Rusie, D.; Mercan Stanciu, A.; Toma, L.; Iliescu, E.L. Correlation Between Serum Alpha-Fetoprotein and Tumour Size in Patients With Hepatocellular Carcinoma Treated With Direct-Acting Antivirals. Cureus 2022, 14, e24506. [Google Scholar] [CrossRef] [PubMed]
- Trevisani, F.; D’Intino, P.E.; Caraceni, P.; Pizzo, M.; Stefanini, G.F.; Mazziotti, A.; Grazi, G.L.; Gozzetti, G.; Gasbarrini, G.; Bernardi, M. Etiologic factors and clinical presentation of hepatocellular carcinoma. Differences between cirrhotic and noncirrhotic Italian patients. Cancer 1995, 75, 2220–2232. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Shen, L.; Wu, Z.; Shi, Y.; Hou, P.; Xue, Z.; Lin, C.; Chen, X.; Group, F.H.-b.S. Trajectories of serum α-fetoprotein and intermediate-stage hepatocellular carcinoma outcomes after transarterial chemoembolization: A longitudinal, retrospective, multicentre, cohort study. EClinicalMedicine 2022, 47, 101391. [Google Scholar] [CrossRef] [PubMed]
- Yen, Y.H.; Kee, K.M.; Li, W.F.; Liu, Y.W.; Wang, C.C.; Hu, T.H.; Tsai, M.C.; Lin, C.Y. Stationary Trend in Elevated Serum Alpha-Fetoprotein Level in Hepatocellular Carcinoma Patients. Cancers 2023, 15, 1222. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, O.; Cacho, B.; Morales-Espinosa, D.; Ruelas-Villavicencio, A.; Flores-Estrada, D.; Hernández-Pedro, N. The progressive elevation of alpha fetoprotein for the diagnosis of hepatocellular carcinoma in patients with liver cirrhosis. BMC Cancer 2007, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L.; Benzi, G.; Santi, V.; Gaiani, S.; Li Bassi, S.L.; Zironi, G.; Mazziotti, A.; Sama, C.; Grigioni, W.; Gozzetti, G. Relationship between alpha-fetoprotein serum levels, tumour volume and growth rate of hepatocellular carcinoma in a western population. Ital. J. Gastroenterol. 1990, 22, 190–194. [Google Scholar] [PubMed]
- Lee, H.S.; Chung, Y.H.; Kim, C.Y. Specificities of serum alpha-fetoprotein in HBsAg+ and HBsAg- patients in the diagnosis of hepatocellular carcinoma. Hepatology 1991, 14, 68–72. [Google Scholar] [CrossRef]
- Carr, B.I.; Guerra, V. Low Alpha-Fetoprotein Levels Are Associated with Improved Survival in Hepatocellular Carcinoma Patients with Portal Vein Thrombosis. Dig. Dis. Sci. 2016, 61, 937–947. [Google Scholar] [CrossRef]
- Siddiqui, M.T.U.; Fareed, G.; Khan, M.R.; Riaz, A.; Hamid, S.S. Portal vein thrombosis in patients with hepatocellular carcinoma and early cirrhosis-prevalence and risk factors. Ecancermedicalscience 2023, 17, 1581. [Google Scholar] [CrossRef] [PubMed]
- Blank, S.; Wang, Q.; Fiel, M.I.; Luan, W.; Kim, K.W.; Kadri, H.; Mandeli, J.; Hiotis, S.P. Assessing prognostic significance of preoperative alpha-fetoprotein in hepatitis B-associated hepatocellular carcinoma: Normal is not the new normal. Ann. Surg. Oncol. 2014, 21, 986–994. [Google Scholar] [CrossRef]
- Sauzay, C.; Petit, A.; Bourgeois, A.M.; Barbare, J.C.; Chauffert, B.; Galmiche, A.; Houessinon, A. Alpha-foetoprotein (AFP): A multi-purpose marker in hepatocellular carcinoma. Clin. Chim. Acta 2016, 463, 39–44. [Google Scholar] [CrossRef]
- Wei, Z.; Zhang, Y.; Lu, H.; Ying, J.; Zhao, H.; Cai, J. Serum alpha-fetoprotein as a predictive biomarker for tissue alpha-fetoprotein status and prognosis in patients with hepatocellular carcinoma. Transl. Cancer Res. 2022, 11, 669–677. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | |
|---|---|
| Parameter | n = 266 |
| Sex (F), n (%) | 85 (32) |
| Age at HCC enrollment, years, median (range) | 73 (45–87) |
| Etiology (viral vs. others), n (%) | |
| Viral | 212 (80) |
| Others | 54 (20) |
| Dimension, mm, median (range) | 26.5 (12–150) |
| Diameter, n (%) | |
| ≥5 cm | 224 (84) |
| <5 cm | 42 (16) |
| Child–Pugh score, n (%) | |
| A | 215 (81) |
| B–C | 51 (19) |
| BCLC stage | |
| 0 (Very early) | 60 (23) |
| A (Early) | 206 (77) |
| HCC Grade 1 (1–2 vs. 3), n (%) | |
| 1–2 | 201 (85) |
| 3 | 36 (15) |
| PVT, n (%) | 42 (16) |
| Malignant PVT, n (%) | 37 (14) |
| Type of curative treatment, n (%) | |
| RFTA | 201 (76) |
| PEI | 48 (18) |
| Resection | 29 (11) |
| TACE/TAE 2 | 39 (15) |
| Type of curative treatment, n (%) | |
| AFP cut-offs | 91 (34) |
| ≥20 ng/mL | 31 (12) |
| ≥200 ng/mL | 21 (8) |
| ≥400 ng/mL | 15 (6) |
| ≥1000 ng/ml | |
| HCC recurrence, n (%) 3 | 116 (44) |
| Local recurrence after treatment | 41 (15) |
| New intrahepatic | 77 (29) |
| Extrahepatic metastases | 28 (11) |
| Dead at f-up end, n (%) | 212 (80) |
| Disease-related death, n (%) | 157 (59) |
| Follow-up time, months, median (range) | 41.5 (1–174) |
| Features | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p Value 1 | HR (95%CI) | p Value 1 | |
| Sex (F vs. M) | 0.96 (0.72–1.28) | 0.764 | ||
| Age at HCC enrollment | 1.29 (0.87–1.92) | 0.038 | 1.02 (1.00–1.04) | 0.120 |
| Etiology (viral vs. others) | 1.19 (0.85–1.69) | 0.314 | ||
| Diameter (≥5 cm vs. <5 cm) | 1.79 (1.26–2.55) | 0.001 | 1.50 (1.03–2.18) | 0.034 |
| Child-Pugh score (B–C vs. A) | 1.63 (1.17–2.27) | 0.004 | 1.41 (0.99–2.01) | 0.042 |
| BCLC stage (A vs. 0) | 2.07 (1.46–2.95) | <0.001 | 1.79 (1.22–2.62) | 0.003 |
| HCC Grade (3 vs. 1–2) | 1.43 (0.98–2.09) | 0.061 | ||
| PVT (yes vs. no) | 1.84 (1.29–2.63) | 0.001 | 1.03 (0.56–1.89) | 0.918 |
| Malignant PVT (yes vs. no) | 2.20 (1.51–3.21) | <0.001 | 2.34 (1.24–4.44) | 0.009 |
| Type of treatment (locoregional vs. surgical) | 1.29 (0.84–2.00) | 0.247 | ||
| AFP ≥ 20 ng/mL (vs. < 20 ng/mL) | 1.17 (0.88–1.55) | 0.285 | ||
| AFP ≥ 200 ng/mL (vs. < 200 ng/mL) | 1.27 (0.82–1.99) | 0.287 | ||
| AFP ≥ 400 ng/mL (vs. < 400 ng/mL) | 1.11 (0.67–1.83) | 0.688 | ||
| AFP ≥ 1000 ng/mL (vs. < 1000 ng/mL) | 2.29 (1.35–3.89) | 0.002 | 2.20 (1.28–3.78) | 0.004 |
| Features | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p Value 1 | HR (95%CI) | p Value 1 | |
| Sex (F vs. M) | 0.69 (0.46–1.05) | 0.091 | ||
| Age at HCC enrollment | 1.01 (0.99–1.04) | 0.207 | ||
| Etiology (viral vs. others) | 0.88 (0.57–1.35) | 0.560 | ||
| Diameter (≥5 cm vs. <5 cm) | 2.60 (1.67–4.07) | <0.001 | 2.36 (1.45–3.83) | 0.001 |
| Child-Pugh score (B–C vs. A) | 1.47 (0.94–2.29) | 0.092 | ||
| BCLC stage (A vs. 0) | 2.21 (1.24–3.96) | 0.008 | 2.41 (1.22–4.75) | 0.011 |
| HCC Grade (3 vs. 1–2) | 1.41 (0.84–2.38) | 0.032 | 1.65 (1.04–4.67) | 0.003 |
| PVT (yes vs. no) | 2.39 (1.54–3.71) | <0.001 | 1.55 (0.60–4.01) | 0.363 |
| Malignant PVT (yes vs. no) | 2.40 (1.48–3.88) | <0.001 | 1.69 (0.62–4.61) | 0.304 |
| Type of treatment (locoregional vs. surgical) | 1.41 (0.81–2.48) | 0.229 | ||
| AFP ≥ 20 ng/mL (vs. < 20 ng/mL) | 1.23 (0.84–1.79) | 0.283 | ||
| AFP ≥ 200 ng/mL (vs. < 200 ng/mL) | 1.04 (0.54–1.99) | 0.412 | ||
| AFP ≥ 400 ng/mL (vs. < 400 ng/mL) | 1.97 (1.03–2.17) | 0.104 | ||
| AFP ≥ 1000 ng/mL (vs. < 1000 ng/mL) | 1.82 (1.20–4.13) | 0.021 | 1.95 (1.04–3.68) | 0.038 |
| AFP Cut-Offs | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 20 ng/mL | 200 ng/mL | 400 ng/mL | 1000 ng/mL | |||||||||
| Parameter | < | ≥ | p 2 | < | ≥ | p 2 | < | ≥ | p 2 | < | ≥ | p 2 |
| Sex (F), % | 30 | 32 | 0.368 | 31 | 39 | 0.102 | 30 | 50 | 0.045 | 31 | 47 | 0.020 |
| Age at HCC enrollment, years, median | 73 | 72 | 0.672 | 73 | 72 | 0.753 | 73 | 72 | 0.903 | 73 | 73 | 0.669 |
| Viral etiology, % | 76 | 87 | 0.073 | 79 | 89 | 0.242 | 79 | 91 | 0.201 | 79 | 87 | 0.743 |
| Diameter ≥ 5 cm, % | 11 | 24 | 0.006 | 14 | 30 | 0.027 | 15 | 29 | 0.032 | 15 | 33 | 0.045 |
| Child-Pugh score A, % | 82 | 79 | 0.566 | 83 | 63 | 0.061 | 82 | 62 | 0.022 | 83 | 53 | 0.012 |
| BCLC A, % | 75 | 81 | 0.354 | 76 | 89 | 0.153 | 77 | 86 | 0.426 | 77 | 87 | 0.532 |
| HCC Grade 1 1–2, % | 84 | 69 | <0.001 | 88 | 52 | <0.001 | 87 | 53 | <0.001 | 88 | 36 | <0.001 |
| PVT, % | 13 | 20 | 0.178 | 16 | 19 | 0.612 | 15 | 19 | 0.670 | 16 | 20 | 0.713 |
| Malignant PVT, % | 12 | 18 | 0.192 | 14 | 11 | 0.713 | 14 | 9 | 0.748 | 14 | 13 | 0.947 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazza, S.; Frigerio, C.; Alfieri, D.; Mauro, A.; Torello Viera, F.; Scalvini, D.; Barteselli, C.; Sgarlata, C.; Veronese, L.; Bardone, M.; et al. Prognostic Role of Basal Serum Alpha-Fetoprotein in Patients with Hepatocellular Carcinoma Suitable for Curative Treatment. Medicina 2024, 60, 692. https://doi.org/10.3390/medicina60050692
Mazza S, Frigerio C, Alfieri D, Mauro A, Torello Viera F, Scalvini D, Barteselli C, Sgarlata C, Veronese L, Bardone M, et al. Prognostic Role of Basal Serum Alpha-Fetoprotein in Patients with Hepatocellular Carcinoma Suitable for Curative Treatment. Medicina. 2024; 60(5):692. https://doi.org/10.3390/medicina60050692
Chicago/Turabian StyleMazza, Stefano, Chiara Frigerio, Daniele Alfieri, Aurelio Mauro, Francesca Torello Viera, Davide Scalvini, Chiara Barteselli, Carmelo Sgarlata, Letizia Veronese, Marco Bardone, and et al. 2024. "Prognostic Role of Basal Serum Alpha-Fetoprotein in Patients with Hepatocellular Carcinoma Suitable for Curative Treatment" Medicina 60, no. 5: 692. https://doi.org/10.3390/medicina60050692