Estimated Fluoride Doses from Toothpastes Should be Based on Total Soluble Fluoride

Abstract
:1. Introduction
2. Experimental Section
2.1. Ethical Considerations and Sampling
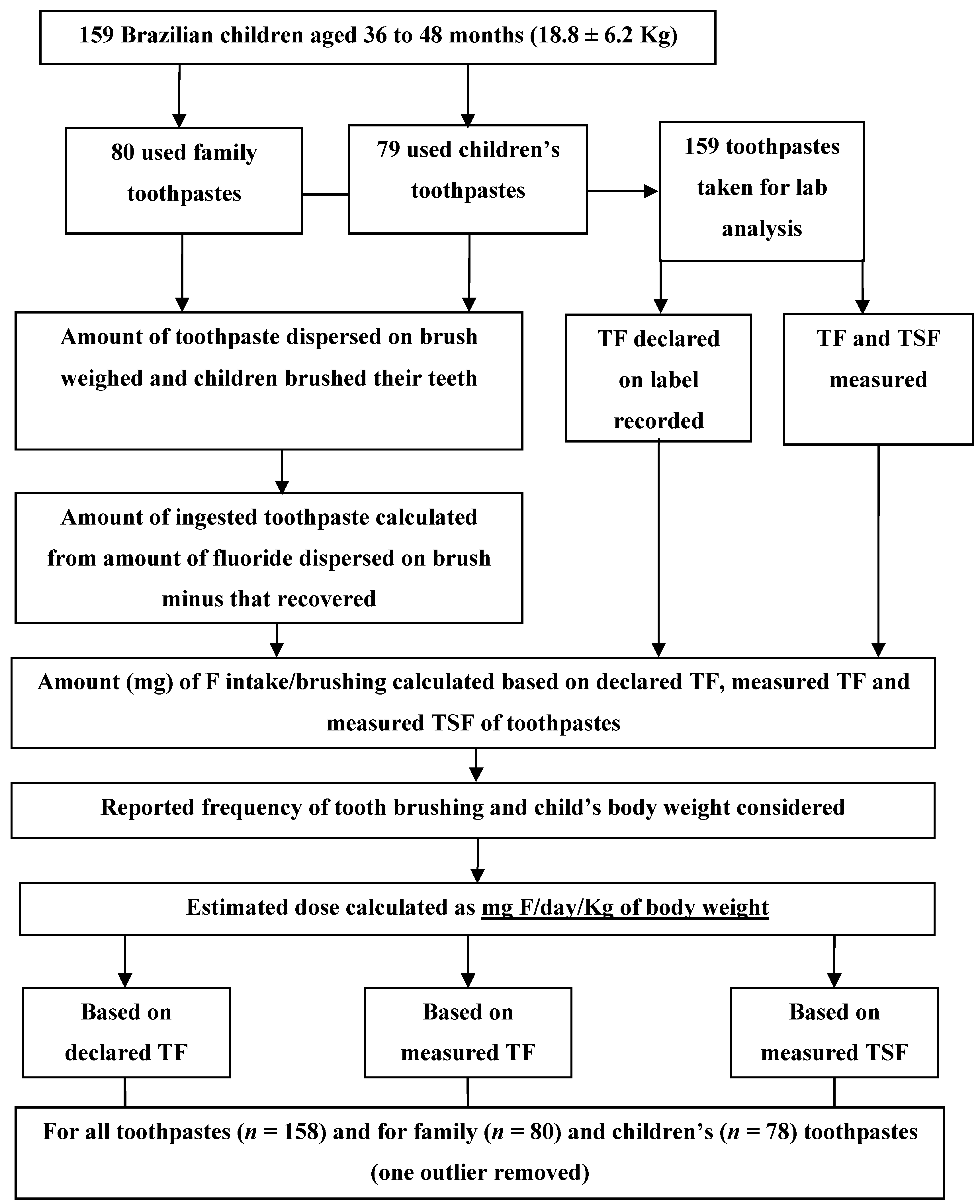
2.2. Experimental Design
2.3. Toothpastes Used

{kind=link}
| Toothpaste | F concentration (ppm F) | ||
|---|---|---|---|
| Declared TF | Measured TF | Measured TSF | |
| Family * (n = 80) | 1,424.3 ± 12.0 | 1,434.0 ± 16.2 | 971.6 ± 23.4 |
| Children’s ** (n = 79) | 1,074.9 ± 13.1 | 1,062.3 ± 12.4 | 1,070.7 ± 24.5 |
| All (n = 159) | 1,251.8 ± 14.6 | 1,250.5 ± 18.0 | 1,020.0 ± 17.3 |
2.4. Determination of Fluoride Intake
2.5. Fluoride Analysis
2.6. Statistical Analysis
3. Results
| Toothpaste | Dose (mg F/day/Kg bw) | ||
|---|---|---|---|
| Based on declared TF | Based on measured TF | Based on measured TSF | |
| Family * (n = 80) | 0.074 ± 0.007 A,a | 0.074 ± 0.007 A,a | 0.039 ± 0.005 A,b |
| Children’s ** (n = 78) | 0.040 ± 0.007 B,a | 0.039 ± 0.003 B,a | 0.039 ± 0.005 A,a |
| All (n = 158) | 0.057 ± 0.004 a | 0.057 ± 0.004a | 0.039 ± 0.003 b |
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Bratthall, D.; Hansel-Petersson, G.; Sundberg, H. Reasons for the caries decline: What do the experts believe? Eur. J. Oral Sci. 1996, 104, 416–422. [Google Scholar] [CrossRef]
- Cury, J.A.; Tenuta, L.M.; Ribeiro, C.C.; Paes Leme, A.F. The importance of fluoride dentifrices to the current dental caries prevalence in Brazil. Braz. Dent. J. 2004, 15, 167–174. [Google Scholar]
- Marinho, V.C.; Higgins, J.P.; Logan, S.; Sheiham, A. Topical fluoride (toothpastes, mouthrinses, gels or varnishes) for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2003, 4. [Google Scholar] [CrossRef]
- Wong, M.C.; Glenny, A.M.; Tsang, B.W.; Lo, E.C.; Worthington, H.V.; Marinho, V.C. Topical fluoride as a cause of dental fluorosis in children. Cochrane Database Syst. Rev. 2010, 1. [Google Scholar] [CrossRef]
- Fejerskov, O.; Manji, F.; Baelum, V. The nature and mechanisms of dental fluorosis in man. J. Dent. Res. 1990, 69, 692–700. [Google Scholar]
- Burt, B.A. The changing patterns of systemic fluoride intake. J. Dent. Res. 1992, 71, 1228–1237. [Google Scholar] [CrossRef]
- Martins, C.C.; Paiva, S.M.; Lima-Arsati, Y.B.; Ramos-Jorge, M.L.; Cury, J.A. Prospective study of the association between fluoride intake and dental fluorosis in permanent teeth. Caries Res. 2008, 42, 125–133. [Google Scholar] [CrossRef]
- Warren, J.J.; Levy, S.M.; Broffitt, B.; Cavanaugh, J.E.; Kanellis, M.J.; Weber-Gasparoni, K. Considerations on optimal fluoride intake using dental fluorosis and dental caries outcomes—A longitudinal study. J. Public Health Dent. 2009, 69, 111–115. [Google Scholar] [CrossRef]
- Forsman, B.; Ericsson, Y. Fluoride absoption from swallowed fluoride toothpaste. Commun. Dent. Oral Epidemiol. 1973, 1, 115–120. [Google Scholar] [CrossRef]
- Roldi, C.R.; Cury, J.A. Flluoride metabolism after ingestion of dentifrice. Rev. Gaúcha Odontol. 1986, 34, 425–427. (In Portuguese) [Google Scholar]
- Drummond, B.K.; Curzon, M.E.; Strong, M. Estimation of fluoride absoption from swallowed fluoride toothpastes. Caries Res. 1990, 24, 211–215. [Google Scholar] [CrossRef]
- Falcão, A.; Tenuta, L.M.; Cury, J.A. Fluoride gastrointestinal absorption from Na2FPO3/CaCO3- and NaF/SiO2-based toothpastes. Caries Res. 2013, 47, 226–233. [Google Scholar] [CrossRef]
- Giacaman, R.A.; Carrera, C.A.; Munoz-Sandoval, C.; Fernandez, C.; Cury, J.A. Fluoride content in toothpastes commercialized for children in Chile and discussion on professional recommendations of use. Int. J. Paediatr. Dent. 2013, 23, 77–83. [Google Scholar] [CrossRef]
- Cury, J.A.; Oliveira, M.J.; Martins, C.C.; Tenuta, L.M.; Paiva, S.M. Available fluoride in toothpastes used by Brazilian children. Braz. Dent. J. 2010, 21, 396–400. [Google Scholar]
- Carrera, C.A.; Giacaman, R.A.; Munoz-Sandoval, C.; Cury, J.A. Total and soluble fluoride content in commercial dentifrices in Chile. Acta Odontol. Scand. 2012, 70, 583–588. [Google Scholar] [CrossRef]
- Cury, J.A.; Tenuta, L.M. How to maintain a cariostatic fluoride concentration in the oral environment. Adv. Dent. Res. 2008, 20, 13–16. [Google Scholar] [CrossRef]
- Ekstrand, J.; Ehrnebo, M. Absoption of fluoride from fluoride dentifrices. Caries Res. 1980, 14, 96–102. [Google Scholar] [CrossRef]
- Borremans, M.; van Loco, J.; van den Meerssche, P.; Meunier, J.; Vrindts, E.; Goeyens, L. Analysis of fluoride in toothpastes on the Belgian market. Int. J. Cosmet. Sci. 2008, 30, 145–152. [Google Scholar] [CrossRef]
- Van Loveren, C.; Moorer, W.R.; Buijs, M.J.; van Palenstein Helderman, W.H. Total and free fluoride in toothpastes from some non-established market economy countries. Caries Res. 2005, 39, 224–230. [Google Scholar] [CrossRef]
- Ricomini Filho, A.P.; Tenuta, L.M.; Fernandes, F.S.; Calvo, A.F.; Kusano, S.C.; Cury, J.A. Fluoride concentration in the top-selling Brazilian toothpastes purchased at different regions. Braz. Dent. J. 2012, 23, 45–48. [Google Scholar] [CrossRef]
- Martins, C.C.; Oliveira, M.J.; Pordeus, I.A.; Cury, J.A.; Paiva, S.M. Association between socioeconomic factors and the choice of dentifrice and fluoride intake by children. Int. J. Environ. Res. Public Health 2011, 8, 4284–4299. [Google Scholar] [CrossRef]
- Puppin Rontani, R.M.; Correa Kassawara, A.B.; Delgado Rodrigues, C.R. Influence of socioeconomic level and dentifrice brand on the oral hygiene habits and the fluoride dentifrice ingestion. J. Clin. Pediatr. Dent. 2002, 26, 319–325. [Google Scholar]
- Omena, L.M.; Silva, M.F.; Pinheiro, C.C.; Cavalcante, J.C.; Sampaio, F.C. Fluoride intake from drinking water and dentifrice by children living in a tropical area of Brazil. J. Appl. Oral Sci. 2006, 14, 382–387. [Google Scholar] [CrossRef]
- Moraes, S.M.; Pessan, J.P.; Ramires, I.; Buzalaf, M.A. Fluoride intake from regular and low fluoride dentifrices by 2–3-year-old children: Influence of the dentifrice flavor. Braz. Oral Res. 2007, 21, 234–240. [Google Scholar] [CrossRef]
- Oliveira, M.J.; Paiva, S.M.; Martins, L.H.; Ramos-Jorge, M.L.; Lima, Y.B.; Cury, J.A. Fluoride intake by children at risk for the development of dental fluorosis: Comparison of regular dentifrices and flavoured dentifrices for children. Caries Res. 2007, 41, 460–466. [Google Scholar] [CrossRef]
- Kobayashi, C.A.; Belini, M.R.; Italiani, F.M.; Pauleto, A.R.; Araújo, J.J.; Tessarolli, V.; Grizzo, L.T.; Pessan, J.P.; Machado, M.A.; Buzalaf, M.A. Factors influencing fluoride ingestion from dentifrice by children. Commun. Dent. Oral Epidemiol. 2011, 39, 426–432. [Google Scholar] [CrossRef]
- Guha-Chowdhury, N.; Drummond, B.K.; Smillie, A.C. Total fluoride intake in children aged 3 to 4 years—A longitudinal study. J. Dent. Res. 1996, 75, 1451–1457. [Google Scholar] [CrossRef]
- Szpunar, S.M.; Burt, B.A. Trends in the prevalence of dental fluorosis in the United States: A review. J. Public Health Dent. 1987, 47, 71–79. [Google Scholar] [CrossRef]
- Ekstrand, J.; Spak, C.J.; Vogel, G. Pharmacokinetics of fluoride in man and its clinical relevance. J. Dent. Res. 1990, 69, 550–555. [Google Scholar]
- Cury, J.A.; del Fiol, F.S.; Tenuta, L.M.; Rosalen, P.L. Low-fluoride dentifrice and gastrointestinal fluoride absorption after meals. J. Dent. Res. 2005, 84, 1133–1137. [Google Scholar] [CrossRef]
- Spak, C.J.; Ekstrand, J.; Zylberstein, D. Bioavailability of fluoride added by baby formula and milk. Caries Res. 1982, 16, 249–256. [Google Scholar] [CrossRef]
- Petersen, P.E.; Lennon, M.A. Effective use of fluorides for the prevention of dental caries in the 21st century: The WHO approach. Commun. Dent. Oral Epidemiol. 2004, 32, 319–321. [Google Scholar] [CrossRef]
- Levy, S.M.; Warren, J.J.; Broffitt, B. Patterns of fluoride intake from 36 to 72 months of age. J. Public Health Dent. 2003, 63, 211–220. [Google Scholar] [CrossRef]
- De Almeida, B.S.; da Silva Cardoso, V.E.; Buzalaf, M.A. Fluoride ingestion from toothpaste and diet in 1- to 3-year-old Brazilian children. Commun. Dent. Oral Epidemiol. 2007, 35, 53–63. [Google Scholar] [CrossRef]
- Hashizume, L.N.; Lima, Y.B.; Kawaguchi, Y.; Cury, J.A. Fluoride availability and stability of Japanese dentifrices. J. Oral Sci. 2003, 45, 193–199. [Google Scholar] [CrossRef]
- Martins, C.C.; Paiva, S.M.; Cury, J.A. Effect of discontinuation of fluoride intake from water and toothpaste on urinary excretion in young children. Int. J. Environ. Res. Public Health 2011, 8, 2132–2141. [Google Scholar] [CrossRef]
- Zohoori, F.V.; Duckworth, R.M.; Omid, N.; O’Hare, W.T.; Maguire, A. Fluoridated toothpaste: Usage and ingestion of fluoride by 4- to 6-yr-old children in England. Eur. J. Oral Sci. 2012, 120, 415–421. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Oliveira, M.J.L.; Martins, C.C.; Paiva, S.M.; Tenuta, L.M.A.; Cury, J.A. Estimated Fluoride Doses from Toothpastes Should be Based on Total Soluble Fluoride. Int. J. Environ. Res. Public Health 2013, 10, 5726-5736. https://doi.org/10.3390/ijerph10115726
Oliveira MJL, Martins CC, Paiva SM, Tenuta LMA, Cury JA. Estimated Fluoride Doses from Toothpastes Should be Based on Total Soluble Fluoride. International Journal of Environmental Research and Public Health. 2013; 10(11):5726-5736. https://doi.org/10.3390/ijerph10115726
Chicago/Turabian StyleOliveira, Maria José L., Carolina C. Martins, Saul M. Paiva, Livia M. A. Tenuta, and Jaime A. Cury. 2013. "Estimated Fluoride Doses from Toothpastes Should be Based on Total Soluble Fluoride" International Journal of Environmental Research and Public Health 10, no. 11: 5726-5736. https://doi.org/10.3390/ijerph10115726