Distal and Proximal Factors of Health Behaviors and Their Associations with Health in Children and Adolescents


Abstract
:1. Introduction
1.1. Relevance of Biopsychosocial Approaches
1.2. Objectives of the Present Study
2. Method Section
2.1. Participant Characteristics
2.2. Sampling Procedures
2.3. Sample Size
2.4. Measures
2.4.1. Immigration Background
2.4.2. SES
2.4.3. Rural-Urban Differences
2.4.4. Intrinsic Motivation
2.4.5. QOL
2.4.6. Psychopathological Problems
2.4.7. PA (of Relatives and Peers)
2.4.8. Eating Patterns
2.4.9. SB
2.4.10. PF
2.4.11. Objective Health Parameters
2.4.12. Subjective Health and Health Complaints
2.5. Research Design
2.6. Data Analysis
3. Results
3.1. Bivariate Path Correlations and Model Fit

{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | R2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| a | r | a | r | a | r | a | r | a | r | a | r | ||
| 1 Socio-economic status | - | ||||||||||||
| 2 Rural-urban differences | - | 0.03 1 | |||||||||||
| 3 Immigration background | - | −0.25 3 | - | 0.18 3 | |||||||||
| 4 Intrinsic motivation | −0.09 3 | −0.06 3 | −0.02 | −0.02 | −0.01 | −0.01 | 2.3 | ||||||
| 5 Physical activity of relatives and peers | 0.24 3 | 0.25 3 | −0.02 | −0.01 | −0.03 | −0.09 3 | 0.14 3 | 0.12 3 | 6.3 | ||||
| 6 Quality of life | 0.04 | 0.06 2 | −0.01 | −0.02 | −0.10 3 | −00.10 3 | 0.20 3 | 0.23 3 | - | - | 1.2 | ||
| 7 Psychopathological problems | −0.14 3 | −0.15 3 | 0.02 | 0.03 | 0.04 1 | 0.08 3 | −0.08 3 | −0.09 3 | - | - | −0.59 3 | −0.60 3 | 2.6 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | R2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| a | r | a | r | a | r | a | r | a | r | a | r | a | r | a | r | a | r | ||
| 8 Eating pattern | −0.12 3 | −0.14 3 | −0.05 3 | −0.05 3 | 0.04 1 | 0.06 3 | - | - | - | - | 0.06 2 | 2.5 | |||||||
| 9 Physical activity | 0.05 3 | 0.12 3 | −0.01 | −0.02 | −0.03 | −0.08 3 | 0.17 3 | 0.22 3 | 0.25 3 | 0.30 3 | 0.09 3 | 0.14 3 | 0.03 | −0.07 2 | 0.05 1 | 0.03 1 | 12.6 | ||
| 10 Sedentary behavior | −0.14 3 | −0.22 3 | 0.05 2 | 0.05 2 | 0.05 1 | 0.12 3 | - | - | −0.10 3 | −0.14 3 | −0.06 | −0.05 | −0.04 | 0.02 | 0.15 3 | 0.15 3 | −0.02 | 0.08 3 | 6.6 |
| 8 | 9 | 10 | 11 | 12 | 13 | R2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| a | r | a | r | a | r | a | r | a | r | a | r | |||
| 11 Physical fitness | 0.09 3 | 0.10 3 | 0.24 3 | 0.25 3 | −0.10 3 | −0.10 3 | 8.0 | |||||||
| 12 Objective health | −0.103 | −0.10 3 | −0.01 | −0.09 3 | 0.08 3 | 0.09 3 | −0.29 3 | −0.31 3 | 11.0 | |||||
| 13 Subjective health | - | - | - | - | - | - | −0.153 | −0.17 3 | 0.06 1 | 0.11 3 | 3.1 | |||
| 14 Psychosomatic complaints | - | - | - | - | - | - | −0.113 | −0.11 3 | 0.01 | 0.05 1 | 0.21 3 | 0.26 3 | 1.2 | |
| 15 Pains with regard to the locomotor system | - | - | - | - | - | - | −0.02 | 0.00 | −0.02 | −0.03 | 0.07 2 | 0.13 3 | 0.2 | |
| 16 Earache, eyestrain, and sore throat | - | - | - | - | - | - | 0.04 | 0.03 | 0.02 | 0.00 | −0.07 1 | −0.17 3 | 0.1 | |
3.2. Loadings
3.2.1. Level 1: Immigration Background, Rural-Urban Differences, and SES
3.2.2. Level 2: Psychopathological Problems, QOL, Intrinsic Motivation, and Physical Activity of Relatives and Peers
3.2.3. Level 3: SB, PA, and Eating Patterns
3.2.4. Level 4: Objective Health and PF
3.2.5. Level 5: Subjective Health and Health Complaints
4. Discussion
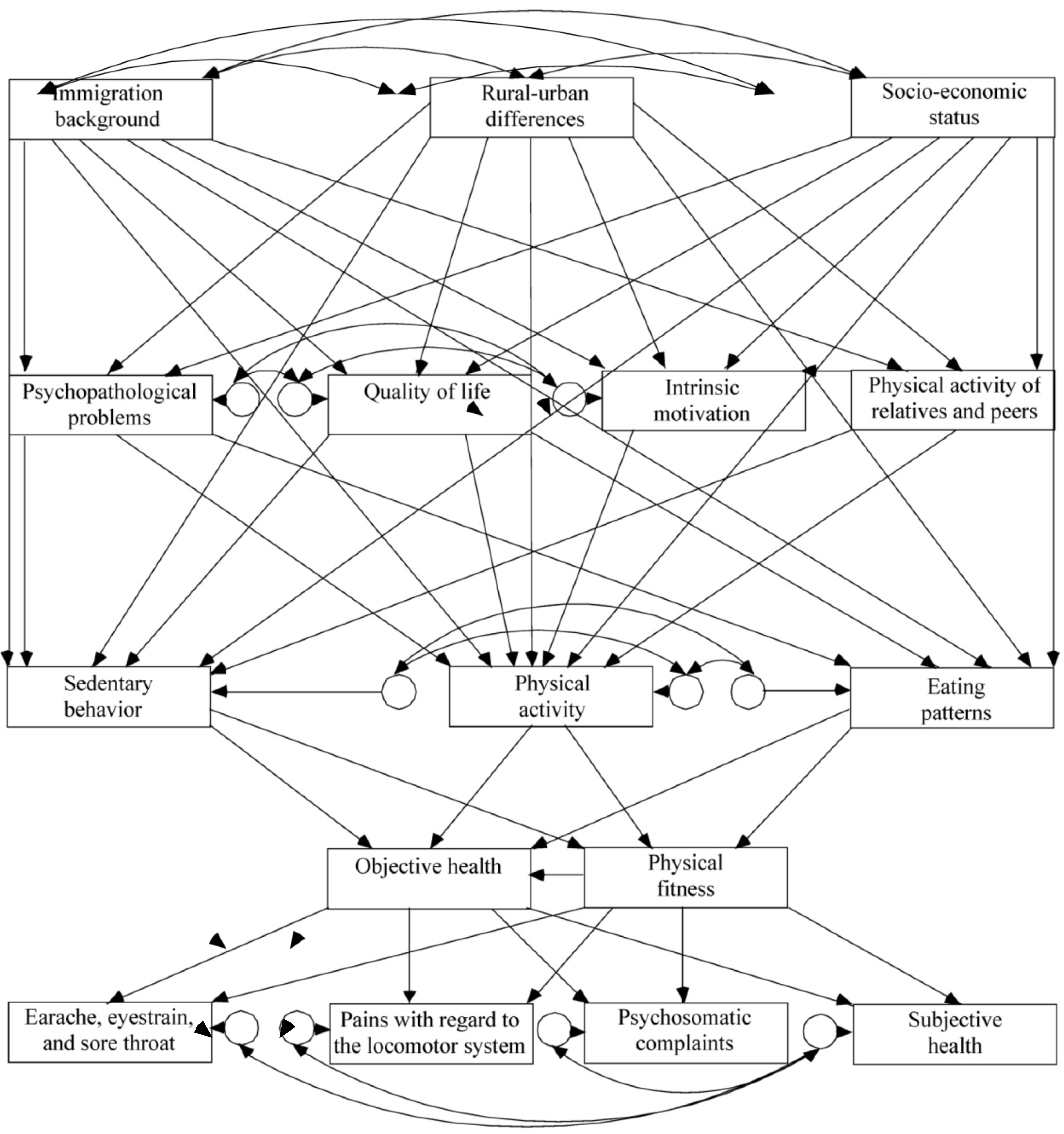
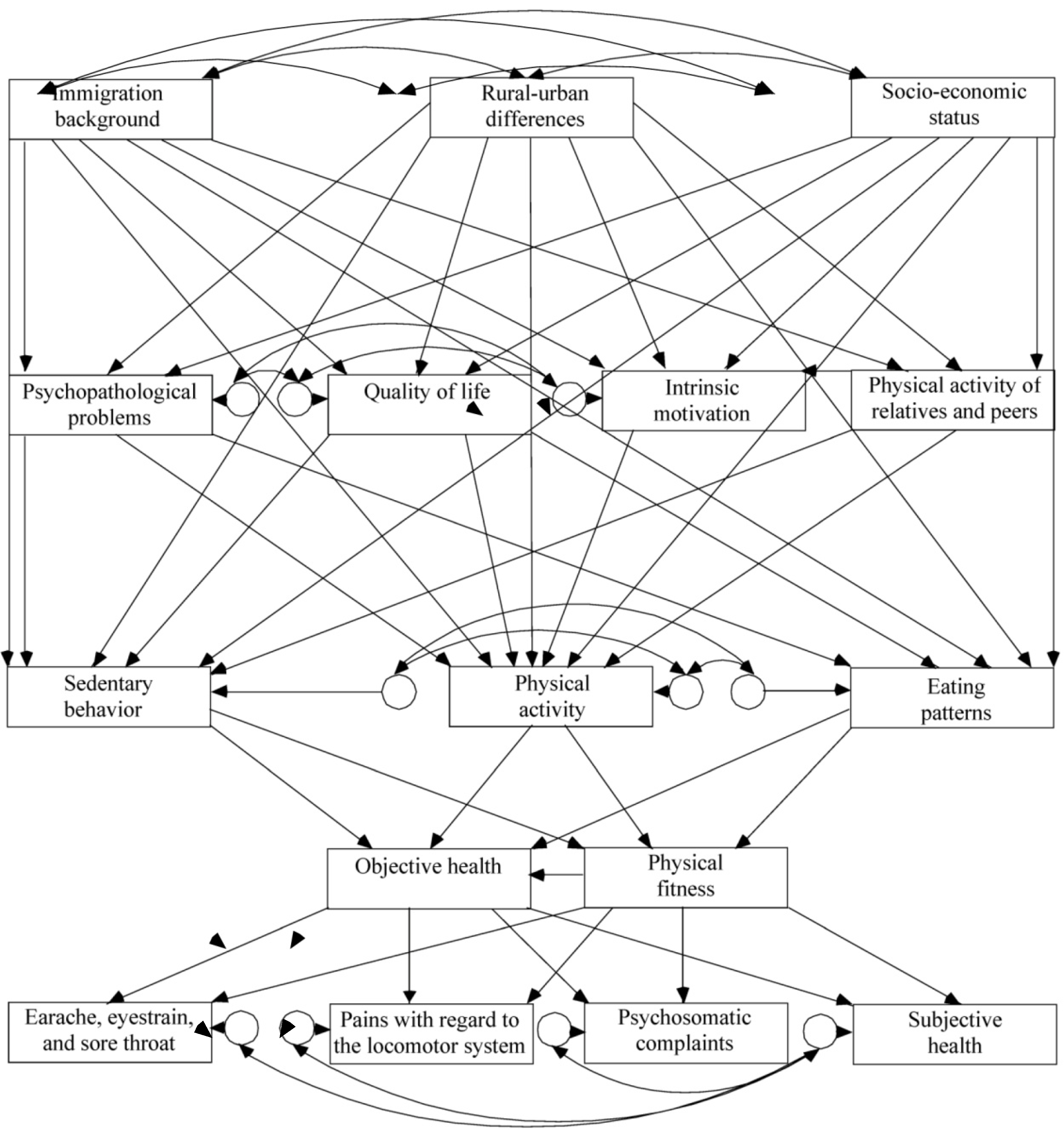
4.1. Key Findings of the Model Paths
4.1.1. Level 1: SES
| Paths | Previous research | Findings of the present study | |||
|---|---|---|---|---|---|
| Authors | Main results | Path model | Comparison of bivariate and path model findings 1 | ||
| Socio-economic status, rural-urban differences | Ferriss (2006) [ 49] | Interplays of socio-economic status, rural-urban differences, immigration status | Lower socioeconomic status was associated with immigration background and urban-dwelling children, and adolescents. Children and adolescents with parents with migration background live in urban areas more frequently. | ||
| Health | Islam
et al. (2008) [50] Steffen et al. (2006) [51] | Connection to health outcomes | Indirect effects on health outcomes | ||
| Socio-economic status & | Physical activity (of relatives and peers ) | Hanson
et al. (2007) [17] Kamphuis et al. (2007) [45] | Less participation in physical activity for lower socioeconomic status | In accordance | |
| Intrinsic motivation | Public authorities for social affairs, the family, and consumer protection (2006)
[52] | A higher intrinsic motivation to be physically active for lower socio-economic status | In accordance | ||
| Quality of life | Ravens-Sieberer et al. (2008) [16] | Negative impact of lower
socio-economic status on quality of life | No differences in quality of life by socio-economic status | Probably effects of common variance for intrinsic motivation & psychopathological problems | |
| Psychopathological problems | Sellstrom & Bremberg,
(2006) [46] | Children living in deprived areas display psychopathological problems more frequently | In accordance | ||
| Eating patterns | Morland
et al. (2002) [18] Eikenberry & Smith, (2004) [47] | Poorer eating patterns for lower socio-economic status | In accordance | ||
| Sedentary behavior | Whitt-Glover et al. (2009) [48] | Some evidence for lower sedentary behavior with a higher socio-economic status | Lower sedentary behavior for a higher socio-economic status | ||
| Hanson & Chen, (2007) [ 17] | Inconsistent findings; more recent research has suggested lower levels of physical activity for lower socio-economic status | Lower levels of physical activity for lower socio-economic status | |||
| Rural-urban differences & | Physical activity (of relatives and peers ) | Trost et al. (2002) [53] | Higher levels of leisure time physical activity among adults living in rural areas than for adults living in urban areas | No differences | |
| Intrinsic motivation | Monge-Rojas et al. (2009) [54] | Scant information available; similar emergent themes of barriers and motivators for achieving an active lifestyle for rural and urban Costa Rican adolescents | No differences | ||
| Quality of life | Collier
et al. (2000) [55] Camfield & Ruta (2007) [56] | Scant information available; no rural-urban differences in quality of life in a developed country; but seen in developing countries | No differences | ||
| Psychopathological problems | Roussos
et al. (2001) [57] Heyerdal et al. (2004) [58] Nie et al. (2008) [59] | Inconsistent findings on rural-urban differences and psychopathological problems may be due to culture as well as to different operationalizations | No differences | ||
| Eating patterns | Adair & Popkin (2005) [ 60] | Scant information available; in China, Russia, Cebu, the Philippines, and the United States, higher percentages of snacking and of calories were found for children and adolescents living in urban environments | Poorer eating patterns for rural children and adolescents | ||
| Sedentary behavior | Biddle (2007) [
61] Li et al. (2007) [62] Shi et al. (2006) [63] Springer et al. (2006) [64] | Scant and inconsistent information available on differences in sedentary behavior caused by rural-urban differences | Children and adolescents living in urban environments revealed more sedentary behavior | ||
| Physical activity | Sjolie & Thuen (2002) [
65] Nelson, Gordon-Larsen, Song, & Popkin (2006) [66] Yamamoto-Kimura et al. (2006) [67] | Inconsistent findings on rural-urban differences and physical activity with regard to nationality, age, and measurement method | No differences | ||
| Immigration background & | Physical activity (of relatives and peers ) | Dotevall
et al. (2000) [68] Lindström & Sundquist (2001) [69] Green et al. (2003) [70] | Higher prevalence of physical inactivity for certain groups of children and adolescents with parents with migration background , also associated with socioeconomic differences; research on of children and adolescents with parents with migration background and physical activity levels has been rare | No differences | Rural-urban differences was shown to be a moderator, indicating common variance in the association of immigration background on physical activity of relatives and peers; quality of life, and physical activity of relatives and peers were found to be mediators; common variance with sedentary behavior and eating patterns could not be excluded |
| Intrinsic motivation | Hosper et al. (2008) [71] | Scant Information on the correlation of immigration background and intrinsic motivation to be physically active | No correlation | ||
| Quality of life | Pantzer et al. (2006) [72] | Effects on quality of life of children’s immigration experience have been examined only marginally; most of these studies have focused on specific aspects such as psychological well-being, mental health, and self-esteem | Children and adolescents with parents with migration background showed a lower quality of life compared to native children and adolescents | ||
| Psychopathological problems | Fazel & Stein (2003) [
73] Leavy et al. (2004) [74] | Studies with children with parents with migration background have revealed more psychopathological problems compared to ethnic minority children | In accordance, children and adolescents with parents with migration background revealed more psychopathological problems | A moderation effect was shown for socio-economic status; assumption of common variance for quality of life and intrinsic motivation to be physically active | |
| Eating patterns | Kumar & Wandel (2006) [ 75] | Immigrants are confronted with nutritional problems | In accordance, poorer eating patterns were observed for children and adolescents with parents with migration background than for native children and adolescents | There seemed to be common variance effects for physical activity and sedentary behavior | |
| Sedentary behavior | Singh
et al. (2008) [76] Allen et al. (2007) [77] | Inconsistent findings on the relationship between immigration background and sedentary behavior | Sedentary behavior in the present study was more widespread in children and adolescents with parents with migration background | Socio-economic status, rural-urban differences, psychopathological problems, and quality of life were moderators of the relationship between immigration background and sedentary behavior | |
| Physical activity (of relatives and peers ) & | Intrinsic motivation | Lämmle et al. (2011) [78] | Positive relationship between the physical activity of relatives and peers and intrinsic motivation | In accordance | |
| Physical activity | Lämmle et al. (2011) [78] | Higher levels of activity of relatives and peers were associated with higher levels of activity for children and adolescents | In accordance | ||
| Sedentary behavior | Saelens & Kerr (2008) [ 79] | The parents’ sedentary behavior was previously shown to be positively associated with their children’s sedentary behavior; research gap on hypothesis as to whether or not a physically active environment also positively affects the sedentary behavior of children and adolescents in the direction of less sedentary behavior | Sedentary behavior was lower for higher levels of activity of relatives and peers | ||
| Intrinsic motivation & | Quality of life, psychopathological problems | Weiner (1986) [
80] Lustyk et al. (2004) [81] | Referring to attribution theory, it can be assumed that intrinsic motivation as a reason for engaging in PA could affect psychological outcomes such as quality of life and psychopathological problems; associations between exercise motivation and quality of life | In accordance; results revealed fewer psychopathological problems and higher quality of life for a higher intrinsic motivation to be physically active | |
| PA | Woods et al. (2007) [82] | Intrinsic motivation was shown to be predictive of PA in children and adolescents | In accordance | ||
| Psychopathological problems | Ravens-Sieberer et al. (2008) [15] | Higher quality of life rates in children and adolescents in 21 European countries (among them Germany) were associated with more psychopathological problems | In accordance | ||
| Sedentary behavior | Lee et al. (2009) [83] | Initial findings with quality of life factors have suggested that parental limits and family conflict are predictive of sedentary behavior; it was hypothesized that a higher quality of life would lead to a reduced sedentary behavior pattern | No correlation | ||
| Physical activity | Sánchez-López et al. (2009) [84] | Scant information on the relationship of quality of life and physical activity; higher levels of physical activity have been associated with higher quality of life | In accordance | ||
| Eating patterns | Wang
et al. (2008) [10] Chen et al. (2005) [85] | Scant information on the relationship of quality of life and eating patterns in childhood and adolescence; unhealthy eating patterns are a risk factor for poor quality of life | No correlation | ||
| Psychopathological problems & | Sedentary behavior | Griffith
et al. (2007) [86] Hamer et al. (2009) [87] | Inconsistent findings on the association between psychopathological problems and sedentary behavior | The assumption that more psychopathological problems would lead to more sedentary behavior was not confirmed. | |
| Physical activity | Wiles et al. (2008) [88] | Reduced psychopathological problems when a physically active lifestyle is maintained | No correlation | Mediation effect was observed for intrinsic motivation to be physically active; common variance effects for eating patterns and sedentary behavior could not be excluded | |
| Eating patterns | Mamun et al. (2009) [89] | Eating patterns are often seen as being confounded or as mediating factors for the association between psychopathological problems and obesity (or being overweight) in children and adolescents | No correlation | There could be common variance between physical activity and sedentary behavior. | |
| Eating patterns & | Physical activity, sedentary behavior | Anderson & Butcher (2006); [
90] Sallis et al. (2009) [19] | Eating patterns, physical activity, and sedentary behavior have been viewed as the primary modifiable behaviors of energy imbalance. Higher physical activity levels have been shown to be related to a healthy diet. | Unhealthy dietary patterns were associated with higher levels of physical activity and physical fitness as well as with better health | |
| Sedentary behavior | Kutchman
et al. (2009) [91] Kremers et al. (2007) [92] | Sedentary behavior is positively associated with the consumption of energy-dense snacks and sugar-containing drinks | In accordance; unhealthier food intake occurred more when sedentary behavior was higher | ||
| Physical fitness | Brunet et al. (2007) [93] | As two other well-known correlates of eating patterns, obesity and being overweight are associated with lower physical fitness levels | |||
| Health | Lindadakis et al. (2008) [94] | Inverse associations of physical fitness and eating patterns with metabolic syndrome risk factors. Unhealthier eating patterns are associated with obesity, being overweight | |||
| Physical activity & | Sedentary behavior | Sallis et al. (2009) [19] | Weak association between physical activity and sedentary behavior; | ||
| Hills et al. (2007) [2] | physically active children and adolescents have exhibited sedentary behavior, even on the same day | In accordance | Common variance was present for socioeconomic status, rural-urban differences, immigration background, physical activity of relatives and peers, quality of life, psychopathological problems, and eating patterns | ||
| Physical fitness | Castelli & Valley (2007) [ 95] | Regular engagement in physical activity has been shown to be associated with the attainment of standards addressing physical fitness | In accordance; higher levels of physical activity had an enhancing effect on physical fitness | ||
| Health | Sallis et al. (2009) [19] | Higher levels of physical activity were associated with better health | No correlation | Mediation effect of physical fitness; common variance of sedentary behavior and eating patterns cannot be excluded; | |
| Sedentary behavior & | Physical fitness | Kerner (2005) [ 96] | The relationship between sedentary behavior and physical fitness has been hypothesized more than it has been explored | Our underlying assumption that less sedentary behavior would be associated with higher levels of physical fitness was confirmed | |
| Health | Sallis et al. (2009) [19] | Sedentary behavior is contributing to obesity since it is characterized by low energy expenditure | In accordance; we found a negative association of sedentary behavior with health | ||
| Physical fitness & | Health, subjective health, psychosomatic complaints, pains with regard to the locomotor system, earache, eyestrain, and sore throat | Eiberg et al. (2005) [97] | There has been some evidence that PF is related to health and subjective health in children | Better health, better subjective health, and fewer psychosomatic complaints revealed for higher physical fitness levels. No significance emerged for pains with regard to the locomotor system and earache, eyestrain, and sore throat. | |
| Health & | Subjective health, psychosomatic complaints, pains with regard to the locomotor system, earache, eyestrain, and sore throat | Janssen et al. (2004) [20] | Health-relevant parameters have been shown to be associated with physical and psychological health complaints | Health was associated with subjective health, but not with pains with regard to the locomotor system, psychosomatic complaints and earache, eyestrain, and sore throat | The diminishing effect of health on psychosomatic complaints within the biopsychosocial process model seemed to be due to collinearity with physical fitness |
| Subjective health & | Psychosomatic complaints, pains with regard to the locomotor system, earache, eyestrain, and sore throat | Vetter (2007) [ 98] | Self-reported occurrence of pain and/or illness influenced the general perception of subjective health | Poorer subjective health was associated with fewer psychosomatic complaints and lower, pains with regard to the locomotor system, but higher earache, eyestrain, and sore throat | For the relationships between subjective health and pains with regard to the locomotor system and between subjective health and earache, eyestrain, and sore throat common variance shared with physical fitness and health emerged |
4.1.2. Level 1: Rural-Urban Differences
4.1.3. Level 1: Immigration Background
4.1.4. Level 2: PA of Relatives and Peers
4.1.5. Level 2: Intrinsic Motivation to be Physically Active
4.1.6. Level 2: QOL
4.1.7. Level 2: Psychopathological Problems
4.1.8. Level 3: Eating Patterns
4.1.9. Level 3: PA and SB
4.1.10. Level 4: PF and Objective Health
4.1.11. Level 5: Subjective Health and Health Complaints
4.2. Limitations
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Hallal, P.C.; Victora, C.G.; Azevedo, M.R.; Wells, J.C.K. Adolescent physical activity and health. Sports Med. 2006, 36, 1019–1030. [Google Scholar] [CrossRef]
- Hills, A.P.; King, N.A.; Armstrong, T.P. The contribution of physical activity and sedentary behaviors to the growth and development of children and adolescents: Implications for overweight and obesity. Sports Med. 2007, 37, 533–545. [Google Scholar] [CrossRef]
- Spear, B.A.; Barlow, S.E.; Ervin, C.; Ludwig, D.S.; Saelens, B.E.; Schetzina, K.E.; Taveras, E.M. Recommendations for treatment of child and adolescent overweight and obesity. Pediatrics 2007, 120, 254–288. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Keller, K.L.; Heymsfield, S.B. Changes in childhood food consumption patterns: A cause for concern in light of increasing body weights. Am. J. Clin. Nutr. 2003, 78, 1068–1073. [Google Scholar]
- Whitaker, R.C.; Wright, J.A.; Pepe, M.S.; Seidel, K.D.; Dietz, W.H. Predicting obesity in young adulthood from childhood and parental obesity. N. Engl. J. Med. 1997, 337, 869–873. [Google Scholar] [CrossRef]
- Friedman, H.S.; Martin, L.R.; Tucker, J.S.; Criqui, M.H.; Kern, M.L.; Reynolds, C.A. Stability of physical activity across the lifespan. J. Health Psychol. 2008, 13, 1092–1104. [Google Scholar] [CrossRef]
- Boreham, C.; Riddoch, C. Physical activity, physical fitness and children’s health: Current concepts. In Paediatric Exercise Science and Medicine; Amstrong, N., Mechelen, W., Eds.; University Press: Ofxford, UK, 2001; pp. 244–250. [Google Scholar]
- Taylor, D.O.; Horner, S.D. Collaborating with low-income families and their overweight children to improve weight related behaviors: An intervention process evaluation. J. Spec. Pediatr. Nurs. 2008, 13, 263–274. [Google Scholar] [CrossRef]
- Dehghan, M.; Akhtar-Danesh, N.; Merchant, A.T. Childhood obesity, prevalence and prevention. Nutr. J. 2005, 4, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Sekine, M.; Chen, X.; Yamagami, T.; Kagamimori, S. Lifestyle at 3 years of age and quality of life (QOL) in first-year junior high school students in Japan: Results of the Toyama birth cohort study. Q. Life Res. 2008, 17, 257–265. [Google Scholar] [CrossRef]
- Flay, B.R.; Petraitis, J. The theory of triadic influence: A new theory of health behaviour with implications for preventive interventions. In Advances in Medical Sociology; Albrecht, G.L., Ed.; JAI Press: Greenwich, CT, USA, 1994; Volume 4, pp. 19–44. [Google Scholar]
- Jessor, R. New Perspectives on Adolescent Risk Behavior; University Press: New York, NY, USA, 1998. [Google Scholar]
- Fishbein, M.; Triandis, H.C.; Kanfer, F.H.; Becker, M.; Middlestadt, S.E.; Eichler, A. Factors influencing behavior and behavior change. In Handbook of Health Psychology; Baum, A., Revenson, T.A., Singer, J.E., Eds.; Erlbaum: Mahwah, NJ, USA, 2001; pp. 3–17. [Google Scholar]
- De Vries, H.; Mesters, I.; van de Steeg, H.; Honing, C. The general public’s information needs and perceptions regarding hereditary cancer: An application of the integrated change model. Patient Educ. Couns. 2005, 56, 154–165. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Erhart, M.; Gosch, A.; Wille, N. The European KIDSCREEN group. Mental health of children and adolescents in 12 European countries—Results from the European KIDSCREEN study. Clin. Psychol. Psychother. 2008, 15, 154–163. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Gosch, A.; Rajmil, L.; Erhart, M.; Bruil, J.; Power, M; The European KIDSCREEN Group. The KIDSCREEN-52 quality of life measure for children and adolescents: Psychometric results from a cross-cultural survey in 13 European countries. Value Health 2008, 11, 645–658. [Google Scholar] [CrossRef]
- Hanson, M.D.; Chen, E. Socioeconomic status and health behaviours in adolescence: A review of the literature. J. Behav. Med. 2007, 25, 425–438. [Google Scholar]
- Morland, K.; Wing, S.; Diez Roux, A. The contextual effect of the local food environment on residents’ diets: The atherosclerosis risk in communities study. Am. J. Public Health 2002, 92, 1761–1767. [Google Scholar] [CrossRef]
- Sallis, J.F.; Rosenberg, D.; Kerr, J. Early physical activity, sedentary behavior, and dietary patterns. In Obesity in youth: Causes, Consequences, and Cures; Heinberg, L.J., Thompson, K.J., Eds.; American Psychology Association: Washington, DC, USA, 2009; pp. 37–57. [Google Scholar]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Pickett, W. The independent influence of physical inactivity and obesity on health complaints in 6th to 10th grade Canadian youth. J. Phys. Act. Health 2004, 1, 331–343. [Google Scholar]
- Kinmonth, A.L.; Wareham, N.J.; Hardeman, W.; Sutton, S.; Prevost, A.T.; Fanshawe, T.; Williams, K.M.; Elkelund, U.; Spiegelhalter, D.; Griffin, S.J. Efficacy of a theory-based behavioural intervention to increase physical activity in an at-risk group in primary care (ProActive UK): A randomised trial. Lancet 2008, 371, 41–48. [Google Scholar] [CrossRef]
- Kurth, B. The german health interview and examination survey for children and adolescents (KiGGS): An overview of its planning, implementation and results taking into account aspects of quality management. (in German). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 533–546. [Google Scholar] [CrossRef]
- Bös, K.; Worth, A.; Opper, E.; Oberger, J.; Romahn, N.; Wagner, M.; Woll, A. The Motoric-Module: Motor Performance Ability and Physical Activity of Children and Adolescents in Germany; Nomos Verlag: Baden-Baden, Germany, 2009. [Google Scholar]
- Cox, L.H. A constructive procedure for unbiased controlled rounding. J. Am. Stat. Assoc. 1987, 82, 520–524. [Google Scholar] [CrossRef]
- Kamtsiuris, P.; Lange, M.; Schaffrath Rosario, A. The german health interview and examination survey for children and adolescents (KiGGS): Sample design, response and nonresponse analysis. (in German). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 547–556. [Google Scholar] [CrossRef]
- Hölling, H.; Kamtsiuris, P.; Lange, M.; Thierfelder, W.; Thamm, M.; Schlack, R. Der Kinder und jugendgesundheitssurvey (KiGGS): Studienmanagement und durchführung der feldarbeit. (in German). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 557–566. [Google Scholar] [CrossRef]
- Lange, M.; Kamtsiuris, P.; Lange, C.; Schaffrath, R.A.; Stolzenberg, H.; Lampert, T. The german health interview and examination survey for children and adolescents (KiGGS): Assessment of socio-demographic factors in the survey for children and adolescents and their meanings on the example of self-evaluation of general health. (in German). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 578–589. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behaviour; Prentice-Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Biddle, S. Sport and exercise motivation: A brief review of antecedent factors and psychological outcomes of participation. In Physical Education: A Reader; Green, K., Hardman, K., Eds.; Meyer & Meyer: Aachen, Germany, 1998; pp. 154–183. [Google Scholar]
- Bullinger, M.; Brütt, A.L.; Erhart, M.; Ravens-Sieberer, U.; The BELLA Study Group. Psychometric properties of the KINDL-R questionnaire: Results of the BELLA study. Eur. Child Adolesc. Psychiatry 2008, 17, 25–132. [Google Scholar]
- Hölling, H.; Erhart, M.; Ravens-Sieberer, U.; Schlack, R. Verhaltensauffälligkeiten bei Kindern und Jugendlichen. (in German). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 784–793. [Google Scholar] [CrossRef]
- Treuth, M.S.; Hou, N.; Young, D.R.; Mayland, L.M. Validity and reliability of the fels physical activity questionnaire for children. Med. Sci. Sports Exer. 2005, 37, 448–495. [Google Scholar]
- Presidents Council on Physical Fitness and Sports, 2008 Physical Activity Guidelines for Americans; U.S. Department of Health and Human Services: Washington, DC, USA, 2008.
- World Health Organization, Global Recommendations on Physical Activity for Health; WHO Library Cataloguing-in-Publication Data: Geneva, Switzerland, 2004.
- Sallis, J.F.; Owen, N. Physical Activity and Behavioural Medicine; Sage: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Truthmann, J.; Mensink, G.B.M.; Richter, A. Relative validation of the KiGGS food frequency questionnaire among adolescents in Germany. Nutr. J. 2011, 10, 133. [Google Scholar] [CrossRef]
- Subar, A.F.; Thompson, F.E.; Kipnis, V.; Midthune, D.; Hurwitz, P.; McNutt, S.; McIntosh, A.; Rosenfeld, S. Comparative validation of the Block, Willett, and National Cancer Institute food frequency questionnaires—The Eating at America’s table study. Am. J. Epidemiol. 2001, 154, 1089–1099. [Google Scholar] [CrossRef]
- McClain, A.D.; Chappuis, C.; Nguyen-Rodriguez, S.T.; Yaroch, A.L.; Spruijt-Metz, D. Psychosocial correlates of eating behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act 2009, 6, 54. [Google Scholar] [CrossRef]
- Lämmle, L.; Tittlbach, S. A two-level model of motor performance ability. J. Exerc. Sci. Fitness 2010, 8, 41–49. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cut off criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Beauducel, A.; Wittmann, W. Simulation study on fit indexes in CFA based on data with slightly distorted simple structure. Struct. Equ. Model. 2005, 12, 41–75. [Google Scholar] [CrossRef]
- Arbuckle, J.L. Full information estimation in the presence of incomplete data. In Advanced Structural Equation Modeling; Marcoulides, G.A., Schumacker, R.E., Eds.; Lawrence Erlbaum: Mahwah, NJ, USA, 1996; pp. 243–277. [Google Scholar]
- Enders, C.K.; Bandalos, D.L. The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Struct. Equ. Model. 2001, 8, 430–457. [Google Scholar] [CrossRef]
- Office of Disease Prevention and Health Promotion, Healthy People 2010; US Department of Health and Human Services: Washington, DC, USA, 2009.
- Kamphuis, C.B.; van Lenthe, F.J.; Giskes, K.; Brug, J.; Mackenbach, J.P. Perceived environmental determinants of physical activity and fruit and vegetable consumption among high and low socioeconomic groups in the Netherlands. Health Place 2007, 13, 493–503. [Google Scholar] [CrossRef]
- Sellstrom, E.; Bremberg, S. The significance of neighbourhood context to child and adolescent health and well-being: A systematic review of multilevel studies. Scand. J. Public Health 2006, 34, 544–554. [Google Scholar] [CrossRef]
- Eikenberry, N.; Smith, C. Healthful eating: Perceptions, motivations, barriers, and promoters in low-income Minnesota communities. J. Am. Diet. Assoc. 2004, 104, 1158–1161. [Google Scholar] [CrossRef]
- Whitt-Glover, M.C.; Brand, D.J.; Turner, M.E.; Ward, S.A.; Jackson, E.M. Increasing physical activity among African-American women and girls. Curr. Sports Med. Rep. 2009, 8, 318–324. [Google Scholar]
- Ferriss, A.L. Social structure and child poverty. Soc. Indic. Res. 2006, 78, 453–472. [Google Scholar] [CrossRef]
- Islam, M.M.; Azad, K.M.A.K. Rural-urban migration and child survival in urban Bangladesh: Are the urban migrants and poor disadvantaged? J. Biosoc. Sci. 2008, 40, 83–96. [Google Scholar]
- Steffen, P.R.; Smith, T.B.; Larson, M.; Butler, L. Acculturation to western society as a risk factor for high blood pressure: A meta-analytic review. Psychosom. Med. 2006, 68, 386–397. [Google Scholar] [CrossRef]
- Public authorities for social affairs, the family and consumer protection (2006), Children in Hamburg in Motion; Creativepool: Hamburg, Germany, 2006.
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sport. Exerc. 2002, 12, 1996–2001. [Google Scholar]
- Monge-Rojas, R.; Garita-Arce, C.; Sánchez-López, M.; Colón-Ramos, U. Barriers to and suggestions for a healthful, active lifestyle as perceived by rural and urban Costa Rican adolescents. J. Nutr. Educ. Behav. 2009, 41, 152–160. [Google Scholar] [CrossRef]
- Collier, J.; MacKinlay, D.; Phillips, D. Norm values for the generic children’s quality of life measure (GCQ) from a large school-based sample. Qual. Life Res. 2000, 9, 617–623. [Google Scholar] [CrossRef]
- Camfield, L.; Ruta, D. “Translation is not enough”: Using the global person generated index (GPGI) to assess individual quality of life in Bangladesh, Thailand, and Ethiopia. Qual. Life Res. 2007, 16, 1039–1051. [Google Scholar] [CrossRef]
- Roussos, A.; Francis, K.; Zoubou, V.; Kiprianis, S.; Prokopiou, A.; Richardson, C. The standardization of Achenbach’s youth self-report in Greece in a national sample of high school students. Euro. Child Adolesc. Psychiatr. 2001, 10, 47–53. [Google Scholar] [CrossRef]
- Heyerdal, S.; Kvemmo, S.; Wichstrom, L. Self-reported behavioural/emotional problems in Norwegian adolescents from multiethnic areas. Euro. Child Adolesc. Psychiatr. 2004, 13, 64–72. [Google Scholar] [CrossRef]
- Nie, Y.G.; Lin, C.D.; Pang, Y.S.; Ding, L.; Gan, X.Y. The development characteristic of adolescents’ social adaptive behavior. Acta Psycholo. Sinica 2008, 40, 1013–1020. [Google Scholar] [CrossRef]
- Adair, L.S.; Popkin, B.M. Are child eating patterns being transformed globally. Obes. Res. 2005, 13, 1281–1299. [Google Scholar] [CrossRef]
- Biddle, S.J.H. Sedentary behavior. Am. J. Prev. Med. 2007, 33, 502–504. [Google Scholar] [CrossRef]
- Li, M.; Dibley, M.J.; Sibbritt, D.W.; Zhou, X.; Hong, Y. Physical activity and sedentary behavior in adolescents in Xi’an City, China. J. Adolesc. Health 2007, 41, 99–101. [Google Scholar] [CrossRef]
- Shi, Z.; Lien, N.; Kumar, B.N.; Holmboe-Ottesen, G. Physical activity and associated socio-demographic factors among school adolescents in Jiangsu province, China. Prev. Med. 2006, 43, 218–221. [Google Scholar] [CrossRef]
- Springer, A.E.; Hoelscher, D.M.; Kelder, S.H. Prevalence of physical activity and sedentary behaviors in US high school students by metropolitan status and geographic region. J. Phys. Act. Health 2006, 3, 365–380. [Google Scholar]
- Sjolie, A.N.; Thuen, F. School journeys and leisure activities in rural and urban adolescents in Norway. Health Promot. Int. 2002, 17, 21–30. [Google Scholar] [CrossRef]
- Nelson, M.C.; Gordon-Larsen, P.; Song, Y.; Popkin, B.M. Built and social environments, associations with adolescent overweight and activity. Am. J. Prevent. Med. 2006, 31, 109–117. [Google Scholar] [CrossRef]
- Yamamoto-Kimura, L.; Posadas-Romero, C.; Posadas-Sánchez, R.; Zamora-González, J.; Cardoso-Saldaña, G.; Méndez Ramírez, I. Prevalence and interrelations of cardiovascular risk factors in urban and rural Mexican adolescents. J. Adolesc. Health 2006, 38, 591–598. [Google Scholar] [CrossRef]
- Dotevall, A.; Rosengren, A.; Lappas, G.; Wilhelmsen, L. Does immigration contribute to decreasing CAD incidence? J. Int. Med. 2000, 247, 331–339. [Google Scholar] [CrossRef]
- Lindström, M.; Sundquist, J. Immigration and leisure-time physical inactivity: A population-based study. Ethnic. Health 2001, 6, 77–85. [Google Scholar] [CrossRef]
- Green, J.; Waters, E.; Haikerwal, A.; O’Neill, C.; Raman, S.; Booth, M.L.; Gibbons, K. Social, cultural and environmental influences on child activity and eating in Australian migrant communities. Care Health Dev. 2003, 29, 441–448. [Google Scholar] [CrossRef]
- Hosper, K.; Nierkens, V.; van Valkengoed, I.; Stronks, K. Motivational factors mediating the association between acculturation and participation in sport among young Turkish and Moroccan women in the Netherlands. Prev. Med. 2008, 47, 95–100. [Google Scholar] [CrossRef]
- Pantzer, K.; Rajmil, L.; Tebé, C.; Codina, F.; Serra-Sutton, V.; Ferrer, M.; Ravens-Sieberer, U.; Simeoni, M.; Alonso, J. Health related quality of life in immigrants and native school aged adolescents in Spain. J. Epidemiol. Community Health 2006, 60, 694–698. [Google Scholar] [CrossRef]
- Fazel, M.; Stein, A. Mental health of refugee children: Comparative study. Br. Med. J. 2003, 327, 134. [Google Scholar] [CrossRef]
- Leavy, G.; Hollins, K.; King, M.; Barnes, J.; Papadopoulos, C.; Grayson, K. Psychological disorders amongst refugee and migrant schoolchildren in London. Soc. Psychiatr. Psychiatr. Epidemiol. 2004, 39, 191–195. [Google Scholar] [CrossRef]
- Kumar, B.; Wandel, M. Nutritional challenges among immigrant children and youth in Norway. In Global Migration and Education: Schools, Children, and Families; Adams, L.D., Kirova, A., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2006; pp. 67–81. [Google Scholar]
- Singh, G.K.; Yu, S.M.; Siahpush, M.; Kogan, M.D. High levels of physical inactivity and sedentary behaviors among US immigrant children and adolescents. Arch. Pediatr. Adolesc. Med. 2008, 162, 756–763. [Google Scholar] [CrossRef]
- Allen, M.L.; Elliott, M.N.; Morales, L.S.; Diamant, A.L.; Hambarsoomian, K.; Schuster, M.A. Adolescent participation in preventive health behaviours, physical activity, and nutrition: Differences across immigrant generations for Asians and Latinos compared with whites. Am. J. Public Health 2007, 97, 337–343. [Google Scholar] [CrossRef]
- Lämmle, L.; Worth, A.; Bös, K. A biopsychosocial process model of health and complaints in children and adolescents. J. Health Psychol. 2011, 16, 226–235. [Google Scholar] [CrossRef]
- Saelens, B.E.; Kerr, J. The family. In Youth Physical Activity and Sedentary Behaviour. Challenges and Solutions; Smith, A.L., Biddle, S.J.H., Eds.; Human Kinetics: Champaign, IL, USA, 2008; pp. 267–294. [Google Scholar]
- Weiner, B. An Attributional Theor of Emotion and Motivationy; Springer-Verlag: New York, NY, USA, 1986. [Google Scholar]
- Lustyk, M.K.B.; Widman, L.; Paschane, A.A.E.; Olson, K.C. Physical activity and quality of life: Assessing the influence of activity frequency, intensity, volume, and motives. J. Behav. Med. 2004, 30, 124–132. [Google Scholar] [CrossRef]
- Woods, A.M.; Bolton, K.; Graber, K.C.; Crull, G.S. Influence of perceived motor competence and motives on children’s physical activity. J. Teach. Phys. Educ. 2007, 26, 390–403. [Google Scholar]
- Lee, S.J.; Bartolic, S.; Vandewater, E.A. Predicting children’s media use in the USA: Differences in cross-sectional and longitudinal analysis. Br. J. Dev. Psychol. 2009, 27, 123–143. [Google Scholar] [CrossRef]
- Sánchez-López, M.; Salcado-Aguilar, F.; Solera-Martinez, M.; Moya-Martinez, P.; Notario-Pacheco, B.; Martinez-Vizcaino, V. Physical activity and quality of life in schoolchildren aged 11–13 years of Cuenca, Spain. Scand. J. Med. Sci. Sports 2009, 19, 879–884. [Google Scholar] [CrossRef]
- Chen, X.; Sekine, M.; Hamanishi, S.; Yamagami, T.; Kagamimori, S. Associations of lifestyle factors with quality of life (QOL) in Japanese children: A 3-year follow-up of the Toyama birth cohort study. Child Care Health Dev. 2005, 31, 433–439. [Google Scholar] [CrossRef]
- Griffith, N.M.; Szaflarski, J.P.; Schefft, B.K.; Isaradisaikul, D.; Meckler, J.M.; McNally, K.A.; Privitera, M.D. Relationship between semiology of psychogenic nonepileptic seizures and minnesota multiphasic personality inventory profile. Epilep. Behav. 2009, 11, 105–111. [Google Scholar]
- Hamer, M.; Stamatakis, E.; Mishra, G. Psychological distress, television viewing, and physical activity in children aged 4 to 12 years. Pediatrics 2009, 123, 1263–1268. [Google Scholar] [CrossRef]
- Wiles, N.J.; Jones, G.T.; Haase, A.M.; Lawlor, D.A.; Macfarlane, G.J.; Lewis, G. Physical activity and emotional problems amongst adolescents. Soc. Psychiatr. Psychiatr. Epidemiol. 2008, 43, 765–772. [Google Scholar] [CrossRef]
- Mamun, A.A.; O’Callaghan, M.J.; Cramb, S.M.; Najman, J.M.; Williams, G.M.; Bor, W. Childhood behavioural problems predict young adults’ BMI and obesity: Evidence from a birth cohort study. Obesity 2009, 17, 761–766. [Google Scholar] [CrossRef]
- Anderson, P.M.; Butcher, K.F. Child obesity: Trends and potential causes. Future Child. 2006, 16, 19–45. [Google Scholar] [CrossRef]
- Kutchman, E.; Lawhun, S.; Laheta, J.; Heinberg, L. Proximal causes and behavior associated with pediatric obesity. In Body Image, Eating Disorders, and Obesity in Youth: Assessment, Prevention, and Treatment; Smolak, L., Thompson, J.K., Eds.; American Psychological Association: Washington, DC, USA, 2009; pp. 157–173. [Google Scholar]
- Kremers, S.P.J.; van der Horst, K.; Brug, J. Adolescent screen-viewing behavior isassociated with consumption of sugar-sweetened beverages: The role of habit strength and perceived parental norms. Appetite 2007, 48, 345–350. [Google Scholar] [CrossRef]
- Brunet, M.; Chaput, J.P.; Tremblay, A. The association between low physical fitness and high body mass index or waist circumference is increasing with age in children: The “Québec en Forme” Project. Int. J. Obes. 2007, 31, 637–643. [Google Scholar]
- Lindadakis, M.; Bertsias, G.; Sarri, S.; Papadaki, A.; Kafatos, A. Metabolic syndrome in children and adolescents in Crete, Greece, and association with diet quality and physical fitness. J. Public Health 2008, 16, 421–428. [Google Scholar] [CrossRef]
- Castelli, D.M.; Valley, J.A. Chapter 3: The relationship of physical fitness and motor competence to physical activity. J. Teach. Phys. Educ. 2007, 26, 358–374. [Google Scholar]
- Kerner, M. Leisure-time physical activity, sedentary behavior, and physical fitness among adolescents: Varying definitions yield differing results in fitness research. J. Phys. Educ. Recreat. Dance 2005, 76, 26–31. [Google Scholar] [CrossRef]
- Eiberg, S.; Hasselstrom, H.; Gronfeldt, V.; Froberg, K.; Cooper, A.; Andersen, L.B. Physical fitness as a predictor of cardiovascular disease risk factors in 6- to 7-year-old Danish children: The Copenhagen school-child intervention study. Paediatr. Exerc. Sci. 2005, 17, 161–170. [Google Scholar]
- Vetter, T.R. A primer on health-related quality of life in chronic pain medicine. J. Int. Anesth. Res. Soc. 2007, 104, 703–718. [Google Scholar]
- Wang, L.Y.; Gutin, B.; Barbeau, P.; Moore, J.B.; Hanes, J.; Johnson, M.H.; Cavnar, M.; Thornburg, J.; Yin, Z. Cost-effectiveness of a school-based obesity prevention program. J. Sch. Health 2008, 78, 619–624. [Google Scholar] [CrossRef]
- Griffith, L.J.; Dowda, M.; Dezateux, C.; Pate, R. Associations between sport and screen-entertainment with mental health problems in 5-year-old children. Int. J. Behav. Nutr. Phys. Acta 2010, 7, 30. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social relationships and mortality risk: A meta-analytic review. PLoS Med. 2010, 7, 1–20. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lämmle, L.; Woll, A.; Mensink, G.B.M.; Bös, K. Distal and Proximal Factors of Health Behaviors and Their Associations with Health in Children and Adolescents. Int. J. Environ. Res. Public Health 2013, 10, 2944-2978. https://doi.org/10.3390/ijerph10072944
Lämmle L, Woll A, Mensink GBM, Bös K. Distal and Proximal Factors of Health Behaviors and Their Associations with Health in Children and Adolescents. International Journal of Environmental Research and Public Health. 2013; 10(7):2944-2978. https://doi.org/10.3390/ijerph10072944
Chicago/Turabian StyleLämmle, Lena, Alexander Woll, Gert B. M. Mensink, and Klaus Bös. 2013. "Distal and Proximal Factors of Health Behaviors and Their Associations with Health in Children and Adolescents" International Journal of Environmental Research and Public Health 10, no. 7: 2944-2978. https://doi.org/10.3390/ijerph10072944