Patterns of Smoking Prevalence among the Elderly in Europe

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. European Survey
2.2. Statistical Methods
3. Results

{kind=link}
| N | Current smokers (%; 95% CI) | Ex-smokers (%; 95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Total | Men | Women | Total | Men | Women | ||
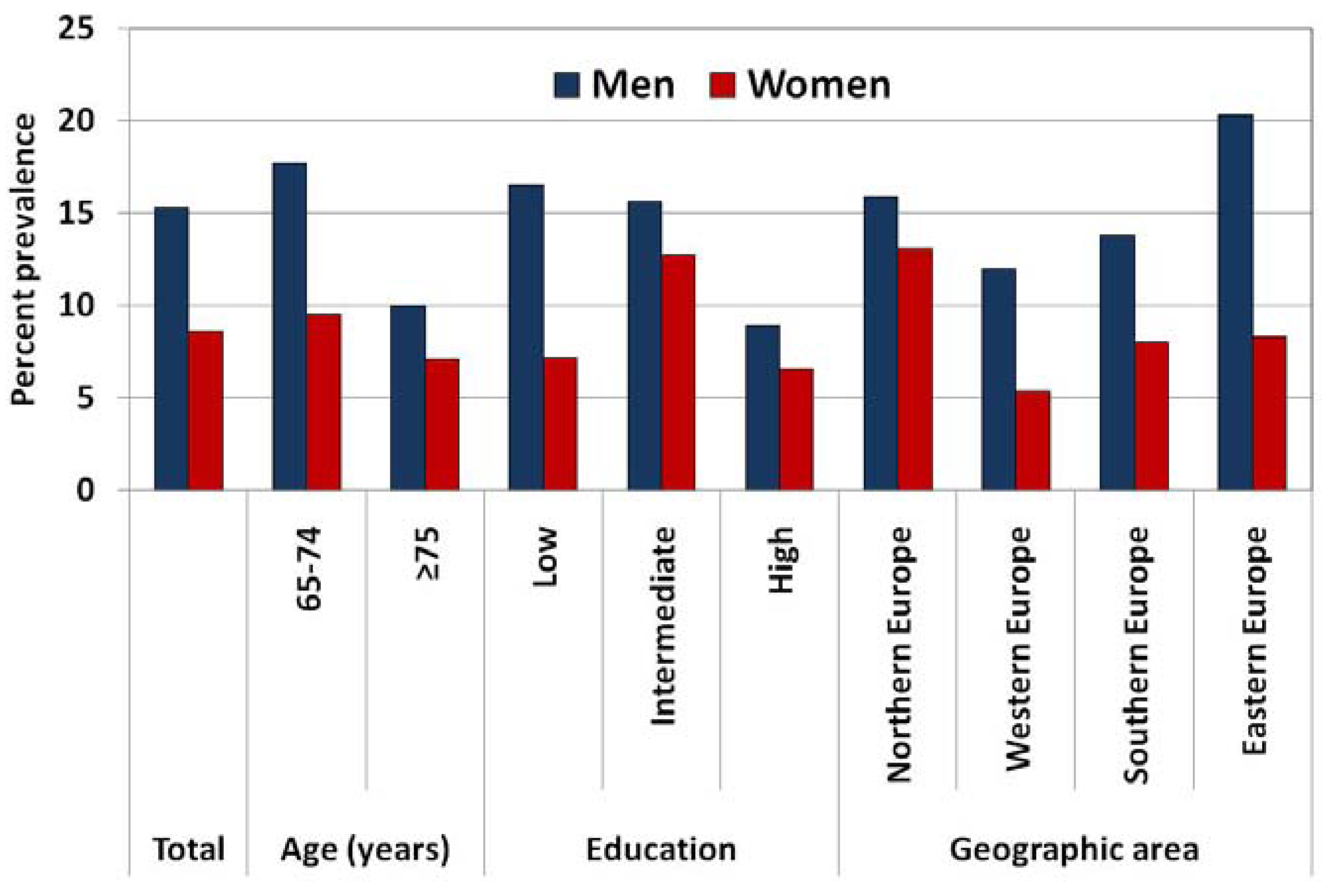
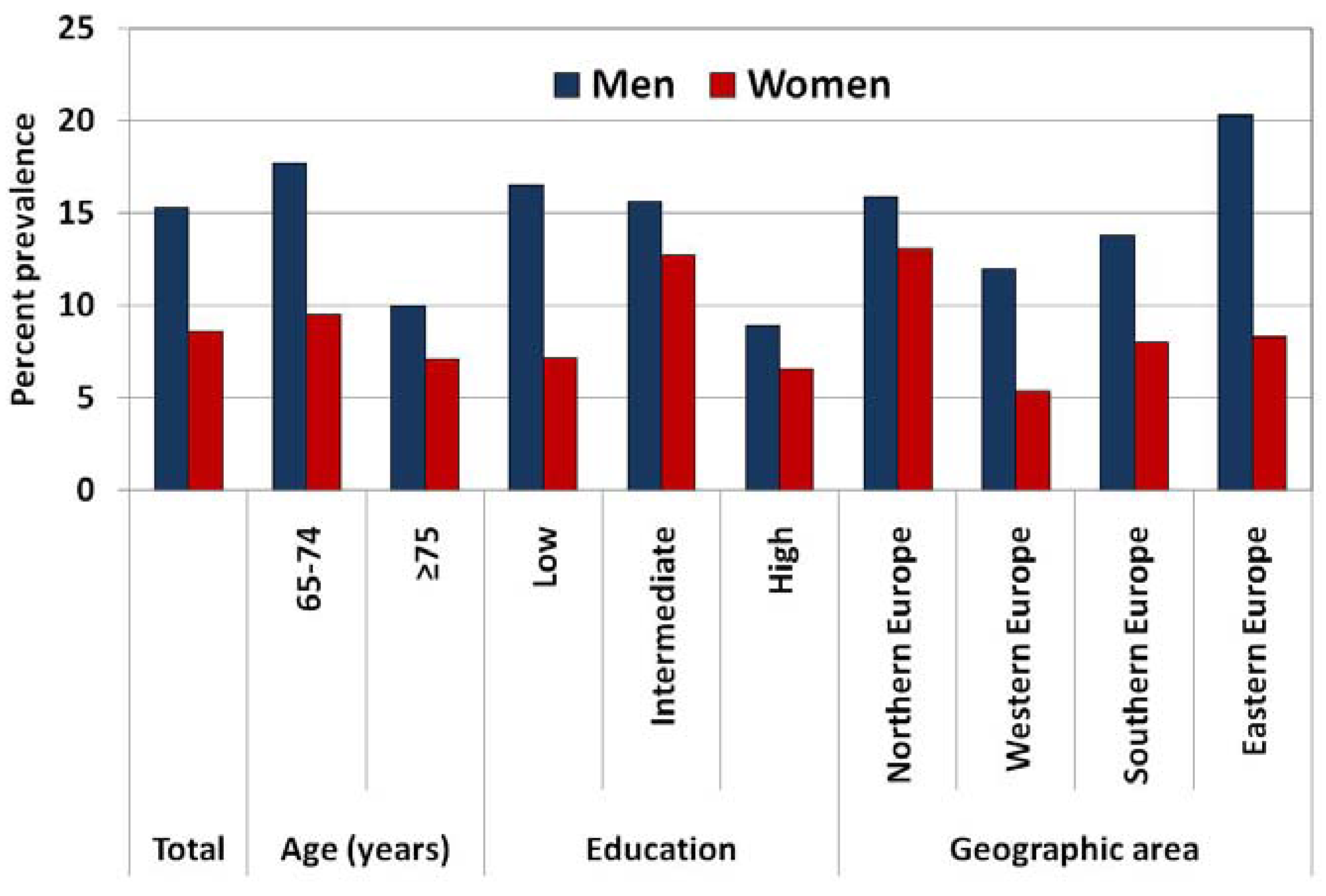
| Total | 3,071 | 11.5 (10.4–12.6) | 15.3 (13.4–17.2) | 8.6 (7.2–10.0) | 23.5 (22.0–25.0) | 33.9 (31.4–36.4) | 15.2 (13.5–16.9) |
| Age | |||||||
| 65–74 | 2,029 | 13.4 (11.9–14.9) | 17.7 (15.3–20.1) | 9.5 (7.7–11.3) | 23.0 (21.2–24.8) | 31.1 (28.2–34.0) | 15.8 (13.6–18.0) |
| ≥75 | 1,042 | 8.2 (6.5–9.9) | 10.0 (7.3–12.7) | 7.1 (5.0–9.2) | 24.4 (21.8–27.0) | 39.9 (35.5–44.3) | 7.1 (5.0–9.2) |
| Education^ | |||||||
| Low | 1,704 | 11.6 (10.1–13.1) | 16.5 (13.9–19.1) | 7.2 (5.5–8.9) | 21.1 (19.2–23.0) | 31.7 (28.5–34.9) | 11.6 (9.5–13.7) |
| Intermediate | 954 | 14.0 (11.8–16.2) | 15.6 (12.1–19.1) | 12.7 (9.9–15.5) | 30.0 (27.1–32.9) | 39.3 (34.6–44.0) | 22.1 (18.6–25.6) |
| High | 412 | 7.7 (5.1–10.3) | 8.9 (5.0–12.8) | 6.6 (3.2–10.0) | 30.0 (25.6–34.4) | 34.5 (28.0–41.0) | 25.4 (19.4–31.4) |
| Geographic area | |||||||
| Northern Europe | 844 | 14.4 (12.0–16.8) | 15.9 (12.3–19.5) | 13.1 (10.0–16.2) | 41.6 (38.3–44.9) | 52.0 (47.1–56.9) | 32.9 (28.6–37.2) |
| Western Europe | 380 | 8.2 (5.4–11.0) | 12.0 (7.1–16.9) | 5.4 (2.4–8.4) | 27.2 (22.7–31.7) | 47.2 (39.6–54.8) | 12.8 (8.3–17.3) |
| Southern Europe | 577 | 10.6 (8.1–13.1) | 13.8 (9.7–17.9) | 8.0 (5.0–11.0) | 14.8 (11.9–17.7) | 21.9 (16.9–26.9) | 9.1 (5.9–12.3) |
| Eastern and central Europe | 1,270 | 13.8 (11.9–15.7) | 20.3 (17.1–23.5) | 8.3 (6.2–10.4) | 16.6 (14.6–18.6) | 23.8 (20.4–27.2) | 10.6 (8.3–12.9) |
| Tobacco Control Scale (TCS) # | |||||||
| <45 | 1,103 | 14.9 (12.8–17.0) | 20.6 (17.0–24.2) | 10.3 (7.9–12.7) | 19.1 (16.8–21.4) | 24.3 (20.5–28.1) | 14.9 (12.1–17.7) |
| ≥45 | 1,712 | 10.8 (9.3–12.3) | 14.0 (11.6–16.4) | 8.2 (6.4–10.0) | 24.7 (22.7–26.7) | 36.2 (32.9–39.5) | 15.6 (13.2–18.0) |
4. Discussion
| N ex smokers aged ≥65 | Reason to quit (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Illness (any medical condition) | Knowledge of the harmful effects of smoking | Physician’s advice | Economic reasons (cigarettes too expensive) | Pressure to quit by partner/ relatives | Pregnancy/birth of a child | Smoke-free legislation | Employer reluctance to hire smokers | Other reasons | |||
| Total | 693 | 39.8 | 19.5 | 9.6 | 5.3 | 4.0 | 2.4 | 0.3 | 0.1 | 19.1 | |
| Sex | |||||||||||
| Men | 465 | 42.1 | 19.7 | 10.2 | 4.2 | 2.7 | 1.6 | 0.4 | 0.1 | 19.0 | |
| Women | 228 | 35.7 | 19.2 | 8.5 | 7.5 | 6.3 | 3.7 | 0.0 | 0.0 | 19.3 | |
| Age (years) | |||||||||||
| 65–74 | 453 | 40.6 | 23.0 | 9.1 | 5.3 | 2.9 | 1.8 | 0.4 | 0.1 | 16.8 | |
| ≥75 | 240 | 38.3 | 13.6 | 10.4 | 5.4 | 5.8 | 3.9 | 0.0 | 0.2 | 23.0 | |
| Education^ | |||||||||||
| Low | 339 | 45.0 | 15.8 | 10.6 | 4.8 | 2.6 | 3.0 | 0.0 | 0.1 | 18.1 | |
| Intermediate | 236 | 33.3 | 21.8 | 9.9 | 7.4 | 5.6 | 1.5 | 0.9 | 0.0 | 19.6 | |
| High | 117 | 31.7 | 29.3 | 4.2 | 2.9 | 7.0 | 1.6 | 0.1 | 0.3 | 22.9 | |
| Geographic area | |||||||||||
| Northern Europe | 291 | 32.3 | 20.9 | 8.5 | 8.9 | 4.0 | 1.5 | 0.0 | 0.1 | 23.8 | |
| Western Europe | 99 | 39.6 | 12.8 | 7.6 | 1.6 | 0.4 | 4.3 | 0.0 | 0.0 | 33.7 | |
| Southern Europe | 93 | 52.4 | 27.1 | 7.4 | 1.1 | 8.8 | 1.9 | 1.1 | 0.3 | 0.0 | |
| Eastern and central Europe | 210 | 38.9 | 14.3 | 19.3 | 9.2 | 2.3 | 2.3 | 0.0 | 0.0 | 13.6 | |
| Tobacco Control Scale (TCS) # | |||||||||||
| <45 | 212 | 28.7 | 14.6 | 27.9 | 9.4 | 5.1 | 6.1 | 0.0 | 0.4 | 7.9 | |
| ≥45 | 446 | 41.5 | 20.4 | 6.5 | 4.7 | 3.9 | 1.8 | 0.3 | 0.0 | 20.9 | |
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Doll, R.; Peto, R.; Boreham, J.; Sutherland, I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ 2004, 328. [Google Scholar] [CrossRef]
- WHO Report on the Global Tobacco Epidemic, 2011. Warning about the Dangers of Tobacco. Available online: http://whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf (accessed on 13 September 2013).
- WHO Global Report: Mortality Attributable to Tobacco. 2012. Available online: http://whqlibdoc.who.int/publications/2012/9789241564434_eng.pdf (accessed on 13 September 2013).
- Peto, R.; Lopez, A.; Boreham, J.; Thun, M. Mortality from Smoking in Developed Countries 1950−2000; CTSU: Oxford, UK, 2006, 2nd ed. Available online: http://www.ctsu.ox.ac.uk/deathsfromsmoking/ (accessed on 13 September 2013).
- Gellert, C.; Schottker, B.; Brenner, H. Smoking and all-cause mortality in older people: Systematic review and meta-analysis. Arch. Intern. Med. 2012, 172, 837–844. [Google Scholar] [CrossRef]
- Burns, D.M. Cigarette smoking among the elderly: Disease consequences and the benefits of cessation. Am. J. Health Promot. 2000, 14, 357–361. [Google Scholar] [CrossRef]
- Husten, C.G.; Shelton, D.M.; Chrismon, J.H.; Lin, Y.C.; Mowery, P.; Powell, F.A. Cigarette smoking and smoking cessation among older adults: United States, 1965–94. Tob. Control 1997, 6, 175–180. [Google Scholar] [CrossRef]
- Lam, T.H.; Li, Z.B.; Ho, S.Y.; Chan, W.M.; Ho, K.S.; Tham, M.K.; Cowling, B.J.; Schooling, C.M.; Leung, G.M. Smoking, quitting and mortality in an elderly cohort of 56,000 Hong Kong Chinese. Tob. Control 2007, 16, 182–189. [Google Scholar] [CrossRef]
- Ferketich, A.K.; Gallus, S.; Colombo, P.; Pacifici, R.; Zuccaro, P.; La Vecchia, C. Hardcore smoking among Italian men and women. Eur. J. Cancer Prev. 2009, 18, 100–105. [Google Scholar] [CrossRef]
- Jarvis, M.J.; Wardle, J.; Waller, J.; Owen, L. Prevalence of hardcore smoking in England, and associated attitudes and beliefs: Cross sectional study. BMJ 2003, 326. [Google Scholar] [CrossRef]
- Lund, M.; Lund, K.E.; Kvaavik, E. Hardcore smokers in Norway 1996–2009. Nicotine Tob. Res. 2011, 13, 1132–1139. [Google Scholar] [CrossRef]
- Finney Rutten, L.J.; Augustson, E.M.; Moser, R.P.; Beckjord, E.B.; Hesse, B.W. Smoking knowledge and behavior in the United States: Sociodemographic, smoking status, and geographic patterns. Nicotine Tob. Res. 2008, 10, 1559–1570. [Google Scholar] [CrossRef]
- Gallus, S.; Muttarak, R.; Franchi, M.; Pacifici, R.; Colombo, P.; Boffetta, P.; Leon, M.E.; La Vecchia, C. Why do smokers quit? Eur. J. Cancer Prev. 2013, 22, 96–101. [Google Scholar] [CrossRef]
- Kim, S.K.; Park, J.H.; Lee, J.J.; Lee, S.B.; Kim, T.H.; Han, J.W.; Youn, J.C.; Jhoo, J.H.; Lee, D.Y.; Kim, K.W. Smoking in elderly Koreans: Prevalence and factors associated with smoking cessation. Arch. Gerontol. Geriatr. 2013, 56, 214–219. [Google Scholar] [CrossRef]
- Marinho, V.; Laks, J.; Coutinho, E.S.; Blay, S.L. Tobacco use among the elderly: A systematic review and meta-analysis. Cad. Saude Publica 2010, 26, 2213–2233. [Google Scholar] [CrossRef]
- Bell, R.A.; Arcury, T.A.; Chen, H.; Anderson, A.M.; Savoca, M.R.; Kohrman, T.; Quandt, S.A. Use of tobacco products among rural older adults: Prevalence of ever use and cumulative lifetime use. Addict. Behav. 2009, 34, 662–667. [Google Scholar] [CrossRef]
- Madruga, C.S.; Ferri, C.P.; Pinsky, I.; Blay, S.L.; Caetano, R.; Laranjeira, R. Tobacco use among the elderly: The first Brazilian National Survey (BNAS). Aging Ment. Health 2010, 14, 720–724. [Google Scholar] [CrossRef]
- Moore, A.A.; Karno, M.P.; Grella, C.E.; Lin, J.C.; Warda, U.; Liao, D.H.; Hu, P. Alcohol, tobacco, and nonmedical drug use in older U.S. Adults: Data from the 2001/02 national epidemiologic survey of alcohol and related conditions. J. Am. Geriatr. Soc. 2009, 57, 2275–2281. [Google Scholar] [CrossRef]
- Zaitune, M.P.; Barros, M.B.; Lima, M.G.; Cesar, C.L.; Carandina, L.; Goldbaum, M.; Alves, M.C. Factors associated with smoking in the elderly: A health survey in Sao Paulo (ISA-SP). Cad. Saude Publica 2012, 28, 583–596. [Google Scholar] [CrossRef]
- Hublet, A.; De Bacquer, D.; Valimaa, R.; Godeau, E.; Schmid, H.; Rahav, G.; Maes, L. Smoking trends among adolescents from 1990 to 2002 in ten European countries and Canada. BMC Public Health 2006, 6. [Google Scholar] [CrossRef]
- Nobile, C.G.; Trani, F.; Di Stasio, S.M.; Angelillo, I.F. Cigarette smoking and alcohol behaviour among adolescents in Italy. Public Health 2006, 120, 942–945. [Google Scholar] [CrossRef]
- Stojiljkovic, D.; Haralanova, M.; Nikogosian, H.; Petrea, I.; Chauvin, J.; Warren, C.W.; Jones, N.R.; Asma, S. Prevalence of tobacco use among students aged 13–15 years in the South-Eastern Europe health network. Am. J. Health. Behav. 2008, 32, 438–445. [Google Scholar]
- Tramacere, I.; Gallus, S.; Pacifici, R.; Zuccaro, P.; Colombo, P.; La Vecchia, C. Smoking in young and adult population, Italy 2009. Tumori 2011, 97, 423–427. [Google Scholar]
- Gallus, S.; La Vecchia, C. Tobacco control: economic aspects of smoking. Prev. Med. 2012, 55, 546–547. [Google Scholar] [CrossRef]
- Gallus, S.; Lugo, A.; La Vecchia, C.; Boffetta, P.; Chaloupka, F.J.; Colombo, P.; Currie, L.; Fernandez, E.; Fischbacher, C.; Gilmore, A.; Godfrey, F.; Joossens, L.; Leon, M.E.; Levy, D.T.; Rosenqvist, G.; Ross, H.; Townsend, J.; Clancy, L. PPACTE, WP2: European Survey on Smoking; PPACTE Consortium: Dublin, Ireland, 2012. [Google Scholar]
- Gallus, S.; Lugo, A.; La Vecchia, C.; Boffetta, P.; Chaloupka, F.J.; Colombo, P.; Currie, L.; Fernandez, E.; Fischbacher, C.; Gilmore, A.; Godfrey, F.; Joossens, L.; Leon, M.E.; Levy, D.T.; Nguyen, L.; Rosenqvist, G.; Ross, H.; Townsend, J.; Clancy, L. Pricing Policies And Control of Tobacco in Europe (PPACTE) project: cross-national comparison of smoking prevalence in 18 European countries. Eur. J. Cancer Prev. 2013, in press. [Google Scholar]
- Perez-Rios, M.; Santiago-Perez, M.I.; Alonso, B.; Malvar, A.; Hervada, X.; de Leon, J. Fagerstrom test for nicotine dependence vs. heavy smoking index in a general population survey. BMC Public Health 2009, 9. [Google Scholar] [CrossRef]
- Joossens, L.; Raw, M. The Tobacco Control Scale 2010 in Europe; Association of the European Cancer Leagues: Brussels, Belgium, 2011. [Google Scholar]
- European Commission; Eurostat. Statistics Database. Available online: http://epp.eurostat.ec.europa.eu/portal/page/portal/statistics/search_database (accessed on 13 September 2013).
- Linardakis, M.; Smpokos, E.; Papadaki, A.; Komninos, I.D.; Tzanakis, N.; Philalithis, A. Prevalence of multiple behavioral risk factors for chronic diseases in adults aged 50+, from eleven European countries - the SHARE study (2004). Prev. Med. 2013, 57, 168–172. [Google Scholar] [CrossRef]
- Lopez, A.; Collishaw, N.; Piha, T. A descriptive model of the cigarette epidemic in developed countries. Tob. Control 1994, 3, 242–247. [Google Scholar]
- Blazer, D.G.; Wu, L.T. Patterns of tobacco use and tobacco-related psychiatric morbidity and substance use among middle-aged and older adults in the United States. Aging Ment. Health 2012, 16, 296–304. [Google Scholar] [CrossRef]
- Manzoli, L.; Di Giovanni, P.; Dragani, V.; Ferrandino, M.G.; Morano, J.P.; Rauti, I.; Schioppa, F.; Romano, F.; Staniscia, T. Smoking behaviour, cessation attempts and the influence of parental smoking in older adult women: A cross-sectional analysis from Italy. Public Health 2005, 119, 670–678. [Google Scholar] [CrossRef]
- Gallus, S.; Schiaffino, A.; La Vecchia, C.; Townsend, J.; Fernandez, E. Price and cigarette consumption in Europe. Tob. Control 2006, 15, 114–119. [Google Scholar] [CrossRef]
- Thun, M.; Peto, R.; Boreham, J.; Lopez, A.D. Stages of the cigarette epidemic on entering its second century. Tob. Control 2012, 21, 96–101. [Google Scholar] [CrossRef]
- Martinez-Sanchez, J.M.; Fernandez, E.; Fu, M.; Gallus, S.; Martinez, C.; Sureda, X.; La Vecchia, C.; Clancy, L. Smoking behaviour, involuntary smoking, attitudes towards smoke-free legislations, and tobacco control activities in the European Union. PLoS One 2010, 5. [Google Scholar] [CrossRef]
- Currie, L.; Gilmore, A.B. Tobacco. In Successes and Failures of Health Policy in Europe: Four Decades of Divergent Trends and Converging Challenges; Mackenbach J., P., McKee, M., Eds.; Open University Press: Maidenhead, Berkshire, UK, 2013; Chapter 2. [Google Scholar]
- Mackenbach, J.P.; Karanikolos, M.; McKee, M. The unequal health of Europeans: successes and failures of policies. Lancet 2013, 381, 1125–1134. [Google Scholar] [CrossRef]
- Breitling, L.P.; Rothenbacher, D.; Stegmaier, C.; Raum, E.; Brenner, H. Older smokers’ motivation and attempts to quit smoking: epidemiological insight into the question of lifestyle versus addiction. Dtsch. Arztebl. Int. 2009, 106, 451–455. [Google Scholar]
- Yong, H.H.; Borland, R.; Siahpush, M. Quitting-related beliefs, intentions, and motivations of older smokers in four countries: findings from the International Tobacco Control Policy Evaluation Survey. Addict. Behav. 2005, 30, 777–788. [Google Scholar] [CrossRef]
- Gallus, S.; La Vecchia, C. A population-based estimate of tobacco dependence. Eur. J. Public Health 2004, 14, 93–94. [Google Scholar] [CrossRef]
- Gallus, S.; Pacifici, R.; Colombo, P.; La Vecchia, C.; Garattini, S.; Apolone, G.; Zuccaro, P. Tobacco dependence in the general population in Italy. Ann. Oncol. 2005, 16, 703–706. [Google Scholar] [CrossRef]
- John, U.; Meyer, C.; Hapke, U.; Rumpf, H.J.; Schumann, A.; Adam, C.; Alte, D.; Ludemann, J. The Fagerstrom test for nicotine dependence in two adult population samples-potential influence of lifetime amount of tobacco smoked on the degree of dependence. Drug Alcohol Depend. 2003, 71, 1–6. [Google Scholar] [CrossRef]
- Jeremias, E.; Chatkin, J.M.; Chatkin, G.; Seibert, J.; Martins, M.; Wagner, M. Smoking cessation in older adults. Int. J. Tuberc. Lung Dis. 2012, 16, 273–278. [Google Scholar] [CrossRef]
- Chabrol, H.; Niezborala, M.; Chastan, E.; de Leon, J. Comparison of the Heavy Smoking Index and of the Fagerstrom Test for Nicotine Dependence in a sample of 749 cigarette smokers. Addict. Behav. 2005, 30, 1474–1477. [Google Scholar] [CrossRef]
- de Leon, J.; Diaz, F.J.; Becona, E.; Gurpegui, M.; Jurado, D.; Gonzalez-Pinto, A. Exploring brief measures of nicotine dependence for epidemiological surveys. Addict. Behav. 2003, 28, 1481–1486. [Google Scholar] [CrossRef]
- Lam, T.H.; He, Y.; Shi, Q.L.; Huang, J.Y.; Zhang, F.; Wan, Z.H.; Sun, C.S.; Li, L.S. Smoking, quitting, and mortality in a Chinese cohort of retired men. Ann. Epidemiol. 2002, 12, 316–320. [Google Scholar] [CrossRef]
- Abdullah, A.S.; Ho, L.M.; Kwan, Y.H.; Cheung, W.L.; McGhee, S.M.; Chan, W.H. Promoting smoking cessation among the elderly: What are the predictors of intention to quit and successful quitting? J. Aging Health 2006, 18, 552–564. [Google Scholar] [CrossRef]
- Chaaya, M.; Mehio-Sibai, A.; El-Chemaly, S. Smoking patterns and predictors of smoking cessation in elderly populations in Lebanon. Int. J. Tuberc. Lung Dis. 2006, 10, 917–923. [Google Scholar]
- Salive, M.E.; Cornoni-Huntley, J.; LaCroix, A.Z.; Ostfeld, A.M.; Wallace, R.B.; Hennekens, C.H. Predictors of smoking cessation and relapse in older adults. Am. J. Public Health 1992, 82, 1268–1271. [Google Scholar] [CrossRef]
- Whitson, H.E.; Heflin, M.T.; Burchett, B.M. Patterns and predictors of smoking cessation in an elderly cohort. J. Am. Geriatr. Soc. 2006, 54, 466–471. [Google Scholar] [CrossRef]
- Ruchlin, H.S. An analysis of smoking patterns among older adults. Med. Care 1999, 37, 615–619. [Google Scholar] [CrossRef]
- Ferketich, A.K.; Gallus, S.; Colombo, P.; Fossati, R.; Apolone, G.; Zuccaro, P.; La Vecchia, C. Physician-delivered advice to quit smoking among Italian smokers. Am. J. Prev. Med. 2008, 35, 60–63. [Google Scholar] [CrossRef]
- Gorin, S.S.; Heck, J.E. Meta-analysis of the efficacy of tobacco counseling by health care providers. Cancer Epidemiol. Biomarkers Prev. 2004, 13, 2012–2022. [Google Scholar]
- Ossip-Klein, D.J.; McIntosh, S.; Utman, C.; Burton, K.; Spada, J.; Guido, J. Smokers ages 50+: Who gets physician advice to quit? Prev. Med. 2000, 31, 364–369. [Google Scholar] [CrossRef]
- Maguire, C.P.; Ryan, J.; Kelly, A.; O’Neill, D.; Coakley, D.; Walsh, J.B. Do patient age and medical condition influence medical advice to stop smoking? Age Ageing 2000, 29, 264–266. [Google Scholar] [CrossRef]
- Tait, R.J.; Hulse, G.K.; Waterreus, A.; Flicker, L.; Lautenschlager, N.T.; Jamrozik, K.; Almeida, O.P. Effectiveness of a smoking cessation intervention in older adults. Addiction 2007, 102, 148–155. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lugo, A.; La Vecchia, C.; Boccia, S.; Murisic, B.; Gallus, S. Patterns of Smoking Prevalence among the Elderly in Europe. Int. J. Environ. Res. Public Health 2013, 10, 4418-4431. https://doi.org/10.3390/ijerph10094418
Lugo A, La Vecchia C, Boccia S, Murisic B, Gallus S. Patterns of Smoking Prevalence among the Elderly in Europe. International Journal of Environmental Research and Public Health. 2013; 10(9):4418-4431. https://doi.org/10.3390/ijerph10094418
Chicago/Turabian StyleLugo, Alessandra, Carlo La Vecchia, Stefania Boccia, Bojana Murisic, and Silvano Gallus. 2013. "Patterns of Smoking Prevalence among the Elderly in Europe" International Journal of Environmental Research and Public Health 10, no. 9: 4418-4431. https://doi.org/10.3390/ijerph10094418
APA StyleLugo, A., La Vecchia, C., Boccia, S., Murisic, B., & Gallus, S. (2013). Patterns of Smoking Prevalence among the Elderly in Europe. International Journal of Environmental Research and Public Health, 10(9), 4418-4431. https://doi.org/10.3390/ijerph10094418