Abstract
Objectives: To quantitatively identify the perception of dentists regarding comprehensiveness and its domains of “patient welcoming”, “bonding” and “quality of care” in primary dental care settings of a large Brazilian city. Methods: A questionnaire was administered to all dentists comprising the primary health care service to Belo Horizonte with tenured jobs and 40 work hours per week, totalling a population of 207 professionals. The response rate was 90.34%. A pilot test was conducted with 44 dentists working in primary care for at least two years and who did not participate in the main study. Descriptive statistical analysis involved calculating proportions. No confidence intervals were calculated because this was a census study. Results: In most items (79.0%), professionals’ perceptions about the comprehensiveness were overwhelmingly positive. When we stratified the analysis by domain and checked those items about which dentists had a less favourable perception, 22.7% were in the patient welcoming domain, 25.0% were in the bonding domain and 12.5% were in quality of care. Conclusions: Comprehensiveness, as an approach in health care practice, needs to be enhanced, and there is evidence that these dentists are aware of its importance.
1. Introduction
Many public health systems around the world are attempting to establish guidelines to improve the performance of health services. To achieve this, they are adopting Primary Health Care (PHC) as a base to focus on prevention and health promotion actions [,,]. PHC is based on a group of aspects that when connected are equally important to structure an efficient healthcare system and reduce health inequalities, considering social, economic and cultural contexts [,,,]. The main aspects, such as universal health access, continuity of care and comprehensiveness, are considered paramount in this structure in order to enhance the quality of care provided [,].
Universal health access calls for making healthcare systems functional and removing supply-side barriers; it is an approach that considers care without obstacles. Continuity of care is the relationship built between the patient and health professional over time, through patient welcoming and bonding with the service, and seeks to respond to the health needs of the population [,,]. Comprehensiveness seeks to take care of people as whole beings in the circumstances in which they live and provide all of the care that people might need; it implies a comprehensive approach to individuals in which the full range of their health needs is recognised. It is a two-dimensional concept, so it also seeks to ensure that more health services at all care levels are interconnected and provided, from prevention to tertiary care [,,].
The focus of our study is on the comprehensiveness approach and its understanding by health professionals, specifically dentists. One meaning of comprehensiveness is related to a way of organising health practices that seeks multidisciplinary and team care. It is necessary that professionals who implement the practices understand and are included in this process because on the basis of comprehensiveness, the health services are organised by making a link between programmed and spontaneous flows of patients, taking advantage of the opportunities generated for the application of diagnostic protocols and identification of risk situations for health, as well as the development of sets of health promotion actions in the community [,].
To understand planning and management in health systems, the contribution of the healthcare workforce is increasingly crucial. The availability of a mix of healthcare occupations across various settings and quantitative, methodical analyses of the stock are essential to motivating better understanding of human resources issues in health care and to identifying problems and solving issues in this area. The necessity to reinforce more studies is overriding, and engaging the healthcare workforce that can potentially produce relevant data that are often underused in health research is very important in this process. Different general data sets can be used as instruments for making assessments of human resources in healthcare, such as sample questionnaires and routine administrative records [,,].
The aim of this study was to quantitatively identify the perception of dentists about comprehensiveness and its domains of “patient welcoming”, i.e., the act of receiving the patient in the clinic and giving a response to their problem; “bonding”, i.e., the link between the patient and the health service; and “quality of care” in dental PHC settings of a large Brazilian city. These concepts are fundamental to exploring the nature of the comprehensiveness approach [,,,]. It is important for the comprehensiveness element to be reinforced in the critical awareness of health professionals and the population to enable the achievement of innovative, integrative and mutual actions in the healthcare system [,,,,,].
2. Methods
This study is part of the second phase of a larger research programme, currently in progress, that proposes to develop an instrument to assess primary care from the dentists’ perspective in domains related to comprehensiveness of care. Parallel studies are examining patient perspectives.
In the first phase, the concept of comprehensiveness was analysed qualitatively through the focus group technique to identify variables and items that should be included in the instrument. In the second phase, the quantitative validation process was carried out, which consists of several steps, one of which was the application of the instrument.
In the initial phase of the research, three key domains in the definition of comprehensiveness of care were discussed: patient welcoming, bonding and quality of care []. Figure 1 illustrates how these domains and their aspects propose a structural link between the concepts of PHC as a way to assess the daily routine of services, professional practices and their relationship with the population [,,,].
The research took place in the city of Belo Horizonte, Brazil. It is the sixth largest city in the country, with approximately 2,450,000 inhabitants and an area of 330 km2. The local health system has a historic tradition in the development of primary care and seeks to structure its system toward the integration of actions, which involves the Medical Specialities Centre and the Centre for Dental Specialities. At the time of the study, the primary health care for dental care consisted of 264 teams divided into 147 health centres in the city [].
A pilot test was conducted with 44 dentists working in primary care for at least two years and who did not participate in the main study. To verify the performance and reliability of the instrument, the test/retest method was employed. The questionnaire was administered twice in the same individuals with an interval of 10–14 days. The weighted Kappa was greater than 0.60.
Data collection was conducted from July to September 2012. The instrument was administered to all dentists in primary health care service in Belo Horizonte with tenured jobs and 40 work hours per week, totalling a population of 207 professionals. The distribution of questionnaires to the 207 dentists took place with the collaboration of the staff from the City Hall. All envelopes were addressed to the healthcare clinics via interoffice mail, and the local managers from each clinic were instructed to remind the participants and to collect the questionnaires in three working days. The response rate was 90.34%.
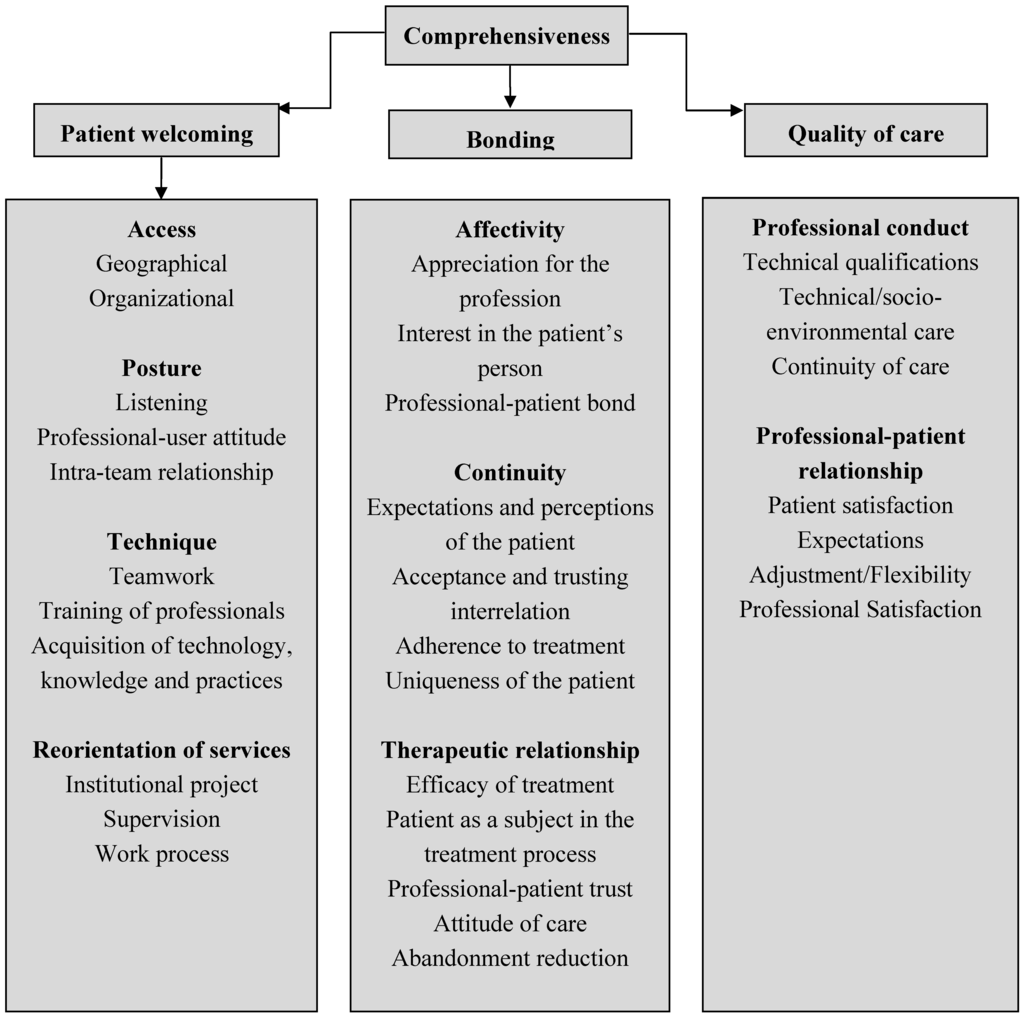
Figure 1.
Domains and aspects related to comprehensiveness to be addressed in the assessment of oral health in PHC.
The database was constructed in the programme EpiData version 3.1 (EpiData Association, Odense M, Denmark). The data were entered twice by different researchers and subsequently validated. This database was exported to SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). At the end of this phase and after execution of the initial stages of the validation process (data not shown), the instrument was constructed with 38 items (Kaiser-Meyer-Olkin measure equal to 0.62 and Cronbach’s alpha equal to 0.76) designed to assess the dentists’ perceptions about dental care in primary care and about comprehensiveness of care in the actions developed in the health service. The questionnaire used an ordinal scale with five response options: always, almost always, sometimes, rarely and never. There were additional options: do not know, refuse to respond and not applicable. The instrument consisted of 38 items (Table 1), with the first 22 about the patient welcoming domain, the following eight relating to bonding and the last eight to the quality of care. Descriptive statistical analysis involved calculating proportions. For each question, the perception was considered positive when more than 50% of the dentists responded with the options “always” and “almost always”. No confidence intervals were calculated because this was a census study. The study was submitted to and approved by the Ethics Committee for Human Research of the Universidade Federal de Minas and the city of Belo Horizonte (protocol number 0437.0.203.410-11A.). Each dentist signed an informed consent after being informed about the objectives of the research.

Table 1.
Items of the instrument and frequency of responses.
| Items | Always | Almost Always | Sometimes | Rarely | Never | Do not Know/Refuse to Respond/Not Applicable |
|---|---|---|---|---|---|---|
| 1—Easy access to dental treatment | 104 | 72 | 11 | – | – | – |
| (55.6%) | (38.5%) | (5.9%) | ||||
| 2—Easy access to emergency dental care | 157 | 28 | 2 | – | – | – |
| (84.0) | (15.0%) | (1.1%) | ||||
| 3—The population have access to oral health care through patient welcoming | 14 | 38 | 7 | – | – | – |
| (75.9%) | (20.3%) | (3.7%) | ||||
| 4—Patient welcoming for oral health care daily | 164 | 12 | 4 | – | 7 | – |
| (87.7%) | (6.4%) | (2.1%) | (3.7%) | |||
| 5—Patient welcoming performed by dentist | 77 | 23 | 54 | 20 | 13 | – |
| (41.2%) | (12.3%) | (28.9%) | (10.7%) | (7.0%) | ||
| 6—Using protocol for the classification of risk and the priority of health care service as part of patient welcoming | 101 | 37 | 19 | 7 | 20 | 3 |
| (54.0%) | (19.8%) | (10.2%) | (3.7%) | (10.7%) | (1.6%) | |
| 7—The population have access to oral health care by appointment | 155 | 28 | 4 | – | – | – |
| (82.9%) | (15.0%) | (2.1%) | ||||
| 8—While waiting, the patient participates in preventive and/or educational activities in oral health care | 28 | 30 | 48 | 46 | 34 | 1 |
| (15.0%) | (16.0%) | (25.7%) | (24.6%) | (18.2%) | (0.5%) | |
| 9—Friendly relationship with patients | 144 | 42 | 1 | – | – | – |
| (77.0%) | (22.5%) | (0.5%) | ||||
| 10—Enough dedicated time to listen to patients’ complaints. | 124 | 59 | 4 | – | – | – |
| (66.3%) | (31.6%) | (2.1%) | ||||
| 11—Clear communication between the dentist and the patient | 125 | 58 | 4 | – | – | – |
| (66.8%) | (31.0%) | (2.1%) | ||||
| 12—Investigations concerning the patient’s life such as work, leisure and housing during the appointment | 36 | 61 | 77 | 11 | – | 2 |
| (19.3%) | (32.6%) | (41.2%) | (5.9%) | (1.1%) | ||
| 13—Knowledge of oral health care team about the oral health problems of the population of the region | 56 | 96 | 31 | 2 | 2 | – |
| (29.9%) | (51.3%) | (16.6%) | (1.1%) | (1.1%) | ||
| 14—Knowledge of other health care professionals about oral health care problems of the population of the region | 13 | 51 | 82 | 28 | 5 | 7 |
| (7.0%) | (27.3%) | (43.9%) | (15.0%) | (2.7%) | (3.7%) | |
| 15—Systematic home visits by the oral health care team | 22 | 44 | 69 | 50 | 2 | – |
| (11.8%) | (23.5%) | (36.9%) | (26.7%) | (1.1%) | ||
| 16—Resolution, at the level of primary care, of the oral health needs of the patient | 122 | 62 | 3 | – | – | – |
| (65.2%) | (33.2%) | (1.6%) | ||||
| 17—Participation of the oral health care team in planning meetings with other professionals from the family health care team | 74 | 62 | 41 | 7 | 3 | – |
| (39.6%) | (33.2%) | (21.9) | (3.7%) | (1.6%) | ||
| 18—Development of activities together by the oral health care team and other professionals on the family health care team | 51 | 62 | 66 | 6 | 2 | – |
| (27.3%) | (33.2%) | (35.3%) | (3.2%) | (1.1%) | ||
| 19—Planning patient care with the aid of other health professionals | 40 | 40 | 76 | 22 | 9 | – |
| (21.4%) | (21.4%) | (40.6%) | (11.8%) | (4.8%) | ||
| 20—Execution of the work supported by the service management | 91 | 57 | 32 | 2 | 1 | 4 |
| (48.7%) | (30.5%) | (17.1%) | (1.1%) | (0.5%) | (2.1%) | |
| 21—Training of auxiliary staff to conduct promotion and prevention actions in oral health by the dentist | 38 | 35 | 74 | 33 | 6 | 1 |
| (20.3%) | (18.7%) | (39.6%) | (17.6%) | (3.2%) | (0.5%) | |
| 22—Providing training course to the dentist that includes family health care | 45 | 50 | 63 | 23 | 5 | 1 |
| (24.1%) | (26.7%) | (33.7%) | (12.3%) | (2.7%) | (0.5%) | |
| 23—Confidence in performing procedures included in primary oral health care | 89 | 87 | 8 | 1 | – | 2 |
| (47.6%) | (46.5%) | (4.6%) | (0.5%) | (1.0%) | ||
| 24—Focus on the oral health of patients | 158 | 21 | 7 | 1 | – | – |
| (84.5%) | (11.2%) | (3.7%) | (0.5%) | |||
| 25—Knowledge of each patient’s medical records | 71 | 89 | 19 | 6 | 1 | 1 |
| (38%) | (47.6%) | (10.2%) | (3.2%) | (0.5%) | (0.5%) | |
| 26—Realisation of referring patients to specialised care | 117 | 8 | 2 | – | – | – |
| (94.7%) | (4.3%) | (1.1%) | ||||
| 27—Transmission of information regarding patient's oral health to the specialist | 114 | 49 | 14 | 7 | 3 | – |
| (61.0%) | (26.2%) | (7.5%) | (3.7%) | (1.6%) | ||
| 28—Return of the patient from specialised care with a written referral prepared by the specialist | 14 | 69 | 77 | 24 | 3 | – |
| (7.5%) | (36.9%) | (41.2%) | (12.8%) | (1.6%) | ||
| 29—Permission for continuity of care in the flow between primary and specialised care | 17 | 71 | 83 | 16 | – | – |
| (9.1%) | (38.0%) | (44.4%) | (8.6%) | |||
| 30—Patient care by the oral health care team at different times of the patient’s life | 72 | 72 | 29 | 2 | – | 12 |
| (38.5%) | (38.5%) | (15.5%) | (1.1%) | (6.4%) | ||
| 31—Cleanliness and organisation of the clinic | 61 | 87 | 31 | 6 | – | 2 |
| (32.6%) | (46.5%) | (16.6%) | (3.2%) | (1.0%) | ||
| 32—Respect for the principles of infection control in dental practice | 105 | 69 | 10 | 1 | – | 2 |
| (56.1%) | (36.9%) | (5.3%) | (0.5%) | (1.0%) | ||
| 33—Supply of inputs and materials for the execution of satisfactory dental care | 18 | 128 | 34 | 5 | – | 2 |
| (9.6%) | (68.4%) | (18.2%) | (2.7%) | (1.0%) | ||
| 34—Using the clinical protocol in the activities of primary care | 127 | 58 | 1 | – | – | 1 |
| (67.9%) | (31%) | (0.5%) | (0.5%) | |||
| 35—Sufficient number of dentists to meet the service demands | 31 | 34 | 30 | 21 | 67 | 3 |
| (16.6%) | (18.2%) | (16.0%) | (11.8%) | (35.8%) | (1.6%) | |
| 36—Knowledge of the major health problems of the community as well as help in resolving them | 48 | 67 | 57 | 8 | 2 | 5 |
| (25.7%) | (35.8%) | (30.5%) | (4.3%) | (1.1%) | (2.7%) | |
| 37—Improvements to care and services provided to the population through courses and training for the oral health care team. | 71 | 65 | 36 | 12 | 1 | 2 |
| (38.0%) | (34.8%) | (19.3%) | (6.4%) | (0.5%) | (1.1%) | |
| 38—Satisfaction with oral health care performance | 54 | 112 | 16 | 2 | – | 3 |
| (28.9%) | (59.9%) | (8.6%) | (1.1%) | (1.6%) |
3. Results
For most items (79.0%), professionals’ perceptions about comprehensiveness were overwhelmingly positive. When we stratified the analysis by the domains that make up the comprehensiveness of care, we found that the perceptions of professionals continued to be largely positive for all three domains: 77.3% for items that make up patient welcoming, 75.0% for the items that make up bonding and 87.5% items which make up quality of care. The five items (22.7%) in the patient welcoming domain about which the perception was less favourable were those about the participation of patients in health promotion activities in the waiting room; knowledge of other health care professionals about oral health care problems of the population of the region; systematic home visits by the oral health care team; planning patient care with the aid of other health professionals; and training of auxiliary team staff by the dentist.
The two items (25.0%) in the bonding domain for which the perception was less favourable were those about the return of the patient from specialised care with a written referral prepared by the specialist and permission for continuity of care in the flow between primary and specialised care. Lastly, the item in the quality of care domain for which the perception was less favourable (12.5%) concerned the sufficiency of the number of dentists to meet the service demands.
4. Discussion
The instrument aimed to assess, in addition to dental care in primary care, the knowledge and attitudes of dentists regarding the comprehensiveness of care and its domains. Dentists’ perception of the concept of comprehensiveness was largely positive. These results may reflect positively on the services because comprehensiveness of care is often used as a quality indicator of PHC [,,], and it is considered an important principle in health systems around the world, such as in the Brazilian and Canadian systems [,]. In PHC, the concept is applied to the mandate to resolve and administer care for the most prevalent health conditions undifferentiated by sex, disease or age, and it has a second meaning that refers to the bio-psycho-social or whole-person approach, which sees the patient within a specific social context [,,,,]. The understanding of this concept is very important for the satisfactory performance of PHC, and these dentists have demonstrated awareness about it for most of the domains.
All of the dentists who made up the study sample were encouraged by the city hall of Belo Horizonte to do a specialisation course in family health care funded by the Brazilian health system. The training policy of the local government for human resources in healthcare may have contributed positively to the findings of the study. The advances in health systems and medical and dental knowledge, as well as the introduction of team-based and holistic, multifaceted patient-centred care, mean that improvements in population health and welfare increasingly depend on the renovation and maintenance of technical capacity among the healthcare workforce [,,].
Stratifying the analysis by the domains that comprise the comprehensiveness of care, most of the issues that were less favourably perceived by the dentists in the patient welcoming domain are related to actions for human resources for health. The less favourable perceptions of the items “knowledge of other health care professionals about oral health care problems of the population of the region” and “planning patient care with the aid of other health professionals” imply a lack of integration between the oral health care team and the other health professionals who work in the same clinic. Historically, oral healthcare has been offered separately from other components integrated into general care []. Nevertheless, the association between systemic health and oral health demonstrates that collaborations among oral health professionals and other health professionals will be necessary for adequately addressing both the oral health care and the general health care of patients receiving healthcare services [,]. According to the literature, some oral diseases such as periodontal disease may be causes or risk factors for several systemic diseases such as diabetes, stroke, cardiovascular disease and atherosclerosis [,]. Because of these issues, collaboration amongst health professionals from both areas is paramount to minimise disparities between care and to ensure that the patient is the focus of an integrated approach to health. [].
The observation of a less favourable perception of “training of auxiliary staff team by the dentist” suggests the need to consider that in team-based work, providing care in accordance with the guidelines set out in a high standard of quality workforce' necessitates engaging in new approaches to and processes in workforce planning []. These dentists seem to have a limited view about this approach. We need to remove the barriers for the development of efficient team-based work and to reinforce the processes of workforce planning; the guidelines that sustain the adequacy and quality of the future workforce can be constructed in line with this view [,,].
In the domain of bonding, the dentists showed less favourable perceptions of items that described the performance and relationship between primary and secondary dental care. Many factors such as lack of a protocol for the construction of referral guidelines between primary and secondary dental care, deficiency in access to/availability of secondary care and lack of co-ordination between primary and secondary dental care may be considered in this context. Possible solutions include coordination to make services complementary and increasing capacity within both levels of care; however, we must note that the issues with the interface between primary and secondary dental care are complex and diverse. Individual measures are therefore likely to be partial and may themselves be complex in execution [,].
In the last domain, quality of care, the participants was concerned about an insufficient number of dentists to meet the service demands. The less favourable perception of this aspect shows that the number of dentists in the study is likely insufficient to care for the high volume of patients who seek health services daily. According to the literature, to obtain satisfactory performance of health services, the dental workforce should be adequate in quantity and skills to address the demand for dental care. Healthcare delivery is shaped by patients, professionals and managers. Adequate working conditions for healthcare stakeholders should be considered in any effort to provide care to a population; otherwise, the quality of care offered will be compromised [,].
Some limitations were faced during the development of the research. Although we used an instrument that has been validated to collect our data, we must consider that the findings for the city of Belo Horizonte do not represent all of Brazil []. We recommend future research with samples from different parts of the country because Brazil is a country of continental dimensions, and the perception of comprehensiveness of care by a professional may differ according to the diverse realities in which s/he operates. Furthermore, it is important to consider that this study is descriptive in nature, and it was not our aim at this time to identify and discuss the causes of the observed perceptions of the concept of comprehensiveness of care and its domains. In future research, we may apply the instrument to other samples in Brazil from different contexts, and further, we may apply the instrument to respondents from other countries, as the items may need to be validated in other languages. The analysis is also important for each group involved in health care delivery, so further research is needed to analyse and compare health services from different perspectives. [,]. On the other hand, a large portion of the Brazilian and world population lives in urban areas and in large cities. Thus, these results could be useful for populations and health systems similar to those in this study.
The descriptive analysis of a scenario or specific situation is a research focus that requires a large amount of effort, but it ultimately enhances the quality of the data collected [,]. In this study, human resources management, the dental workforce and the general population could well benefit from the findings. Most current approaches to assessing the quality of care are based on models developed over fifty years ago. The World Health Organization stated in a report [] that with the growing importance of new experiences, person-focused appraisals should be prioritised over disease-focused appraisals. In this direction, approaches such as comprehensiveness should be studied more and explored more thoroughly so that health systems can benefit from the applicability of its concepts. These key features are increasingly recognised as having an impact on the way health services are delivered, and this study is in line with this statement [,,,,,,,].
5. Conclusions
Identifying and exploring the perceptions of dentists about the characteristics of comprehensiveness are among the main approaches to be considered in the assessment of primary care offered to the population by the Brazilian health system. The results suggest that the dentists in this study are aware of the importance of comprehensiveness for dental practices in primary care, and they also indicate that the concept should be strengthened in some specific areas. Our findings might be useful in further understanding human resources issues in health care and how the perceptions of the dentists can contribute to improvements in primary dental care. In future research, the perceptions of dentists from other parts of Brazil and from different nationalities can be studied to enrich and strengthen the data obtained here.
Acknowledgements
The authors are grateful to the Brazilian funding agency Fundação de Amparo à Pesquisa do Estado de Minas Gerais—FAPEMIG, Coordination of Improvement of Higher Education Personnel—CAPES, Brazil and King’s College London, UK. We also thank the Pró-reitoria de Pesquisa da Universidade Federal de Minas Gerais for financial assistance. Saul M. Paiva and Mauro H.N.G. Abreu are fellows of CNPq.
Author Contributions
Grazielle C. M. Mattos performed the literature review and data collection and statistical analysis. Cleiton G. Sirineu and Bruno R. Teixeira performed the literature review and data collection. Jennifer E. Gallagher, Saul M. Paiva and Mauro H. N. G. Abreu conceived of the study and participated in its design and coordination. All authors helped to draft the manuscript and read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- The World Health Report 2008: Primary Health Care Now More Than Ever; World Health Organization: Geneva, Switzerland, 2009.
- Starfield, B.; Shi, L. Manual for the Primary Care Assessment Tools; Johns Hopkins University: Baltimore, MD, USA, 2009. [Google Scholar]
- Macinko, J.; Montenegro, H.; Nebot, C. Renewing Primary Health Care in the Americas: A Position Paper of the Pan American Health Organization; World Health Organization (PAHO/WHO): Geneva, Switzerland, 2007. [Google Scholar]
- Wallace, B.B.; MacEntee, M.I.; Harrison, R.; Hole, R.; Mitton, C. Community dental clinics: Providers’ perspectives. Community Dent. Oral Epidemiol. 2013, 41, 193–203. [Google Scholar] [CrossRef]
- Aller, M.-B.; Colomé, J.M.; Waibel, S.; Vargas, I.; Vázquez, M.L. A first approach to differences in continuity of care perceived by immigrants and natives in the catalan public healthcare system. Int. J. Environ. Res. Public Health 2013, 10, 1474–1488. [Google Scholar] [CrossRef]
- Dickinson, W.P.; Miller, B.F. Comprehensiveness and continuity of care and the inseparability of mental and behavioral health from the patient-centered medical home. Fam. Syst. Health 2010, 28, 348–355. [Google Scholar] [CrossRef]
- Silva, R.B.D.; Contandriopoulos, A.-P.; Pineault, R.; Tousignant, P. A global approach to evaluation of health services utilization: Concepts and measures. Healthc. Policy. 2011, 6, 106–117. [Google Scholar]
- Mattos, R.A. The Meanings of Comprehensiveness: Some Reflections on Values that Deserve to be Defended. In The Meanings of Comprehensiveness of Care and in Health Care; Pinheiro, R., Mattos, R.A., Eds.; Institute of Social Medicine, State University of Rio de Janeiro/Abrasco: Rio de Janeiro, Brazil, 2001; pp. 39–64. [Google Scholar]
- Haggerty, J.L.; Beaulieu, M.-D.; Pineault, R.; Burge, F.; Lévesque, J.-F.; Santor, D.A.; Bouharaoui, F.; Beaulieu, C. Comprehensiveness of care from the patient perspective: Comparison of primary healthcare evaluation instruments. Healthc. Policy. 2011, 7, 154–166. [Google Scholar]
- Diallo, K.; Zurn, P.; Gupta, N.; Poz, M.D. Monitoring and evaluation of human resources for health: An international perspective. Hum. Resour. Health 2003, 1. [Google Scholar] [CrossRef]
- Gupta, N.; Diallo, K.; Zurn, P.; Poz, M.R.D. Assessing human resources for health: What can be learned from labour force surveys. Hum. Resour. Health 2003, 1, 1–16. [Google Scholar] [CrossRef]
- Rowe, A.K.; de Savigny, D.; Lanata, C.F.; Victora, C.G. How can we achieve and maintain high-quality performance of health workers in low-resource settings? Lancet 2005, 366, 1026–1035. [Google Scholar] [CrossRef]
- Silva Junior, A.G.; Mascarenhas, M.T.M. Basic Healthcare Evaluation from the Perspective of Comprehensiveness: Conceptual and Methodological Aspects. In Care: The Borders of Comprehensiveness; Pinheiro, R., Mattos, R.A., Eds.; Abrasco-Hucitec: Rio de Janeiro, Brazil, 2005; pp. 241–257. [Google Scholar]
- Lewis, S.; Donaldson, C.; Mitton, C.; Currie, G. The future of health care in Canada. BMJ 2001, 323, 926–929. [Google Scholar] [CrossRef]
- Ritchie, J.; Lewis, J. Qualitative Research Practice: A Guide for Social Science Students and Researchers; Sage Pulications: London, UK, 2003. [Google Scholar]
- World Health Organization. Country Cooperation at a Glance: Brazil. Available online: http://apps.who.int/iris/handle/10665/70263 (accessed on 25 January 2014).
- Romanow, R. Building on Values: The Future of Health Care in Canada—–Final Report; Commission of the Future of Health Care: Ottawa, ON, Canada, 2002. [Google Scholar]
- Madore, O. The Canada Health Act.: Overview and Options (Report No.CIR94–4E); Library of Parliament, Parliamentary Information and Research Service: Ottawa, ON, Canada, 2005. [Google Scholar]
- Haggerty, J.; Burge, F.; Lévesque, J.-F.; Gass, D.; Pineault, R.; Beaulieu, M.-D.; Santor, D. Operational definitions of attributes of primary health care: Consensus among Canadian experts. Ann. Fam. Med. 2007, 5, 336–344. [Google Scholar] [CrossRef]
- Gallagher, J.; Wilson, N. The future dental workforce? Brit. Dent. J. 2009, 206, 195–199. [Google Scholar] [CrossRef]
- Mouradian, W.E.; Berg, J.H.; Somerman, M.J. Addressing disparities through dental-medical collaborations, Part 1. The role of cultural competency in health disparities: Training of primary care medical practitioners in children’s oral health. J. Dent. Educ. 2003, 67, 860–868. [Google Scholar]
- Buchan, J.; Poz, M.R.D. Skill mix in the health care workforce: Reviewing the evidence. Bull. WHO 2002, 80, 575–580. [Google Scholar]
- Taylor, G.W. Bidirectional interrelationships between diabetes and periodontal diseases: An epidemiologic perspective. Ann. periodontol. 2001, 6, 99–112. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Bush, R.B.; Paju, S. Associations between periodontal disease and risk for atherosclerosis, cardiovascular disease, and stroke: A systematic review. Ann. periodontol. 2003, 8, 38–53. [Google Scholar] [CrossRef]
- Mitchell, D.A.; Lassiter, S.L. Addressing Health Care Disparities and Increasing Workforce Diversity: The Next Step for the Dental, Medical, and Public Health Professions. Amer. J. Public Health 2006, 96, 2093–2097. [Google Scholar] [CrossRef]
- Grumbach, K.; Bodenheimer, T. Can health care teams improve primary care practice? JAMA 2004, 291, 1246–1251. [Google Scholar] [CrossRef]
- Franzén, C. Boundary work of dentists in everyday work. Community Dent. Oral Epidemiol. 2012, 40, 377–384. [Google Scholar] [CrossRef]
- Morris, A.; Burke, F. Health policy: Primary and secondary dental care: The nature of the interface. Brit. Dent. J. 2001, 191, 660–664. [Google Scholar]
- Morris, A.; Burke, F. Health policy: Primary and secondary dental care: How ideal is the interface? Brit. Dent. J. 2001, 191, 666–670. [Google Scholar]
- Guay, A.H. Access to dental care: Solving the problem for underserved populations. J. Amer. Dent. Assn. 2004, 135, 1599–1605. [Google Scholar] [CrossRef]
- Mosadeghrad, A.M. Healthcare service quality: Towards a broad definition. Int. J. Health Care Qual. Assur. 2013, 26, 203–219. [Google Scholar] [CrossRef]
- Harvey, K.; Catty, J.; Langman, A.; Winfield, H.; Clement, S.; Burns, E.; White, S.; Burns, T. A review of instruments developed to measure outcomes for carers of people with mental health problems. Acta Psychiat. Scand. 2008, 117, 164–176. [Google Scholar] [CrossRef]
- Frencken, J.E.; Souza, A.L.; Sanden, W.J.; Bronkhorst, E.M.; Leal, S.C. The Caries Assessment and Treatment (CAST) instrument. Community Dent. Oral Epidemiol. 2013, 41, 71–77. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).