
Arsenic in Drinking Water, Transition Cell Cancer and Chronic Cystitis in Rural Bangladesh


Abstract
:1. Introduction
2. Methods
2.1. Arsenic Concentrations in Well Water
2.2. Confounding
2.3. Statistical Methods
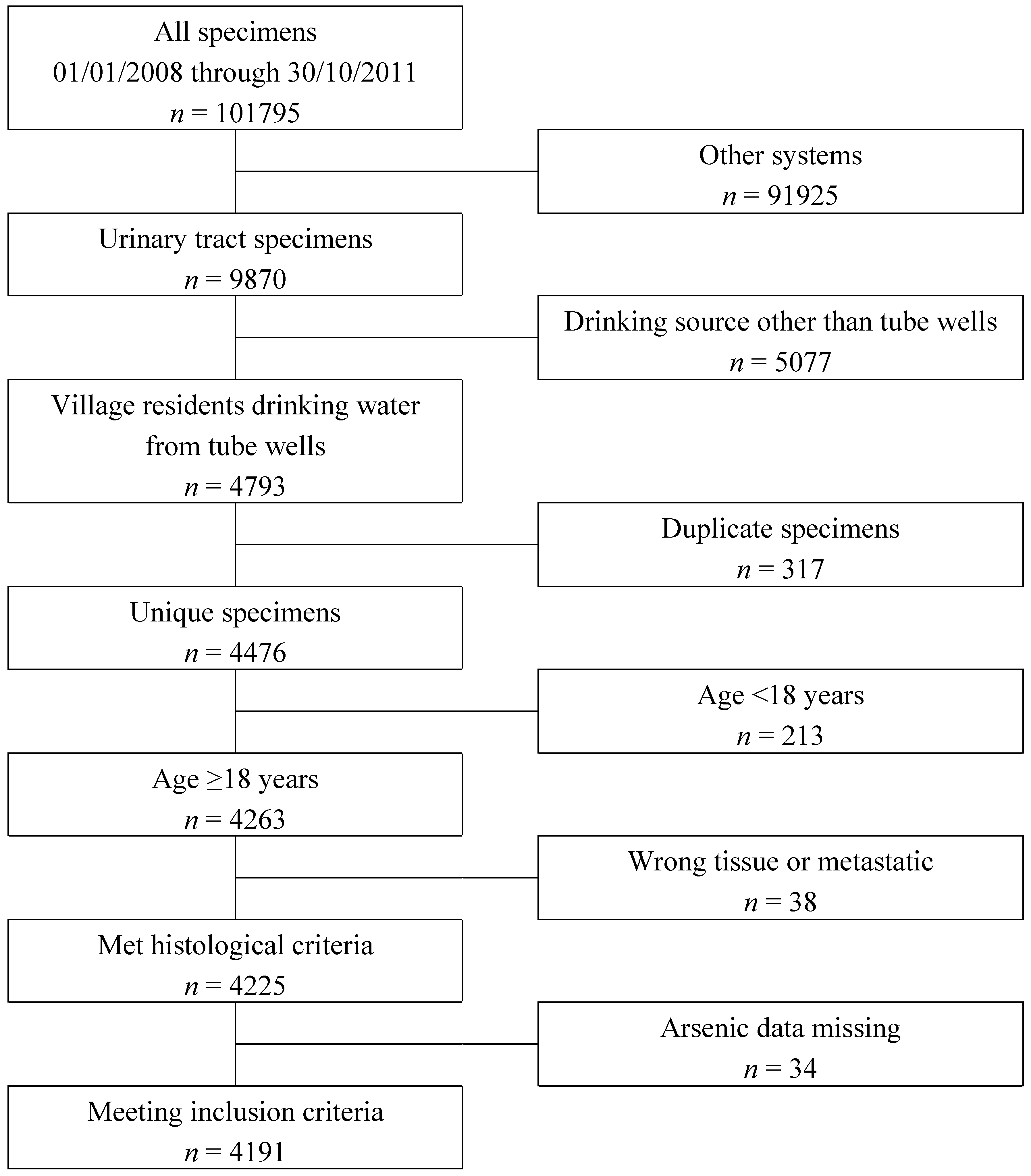
3. Results and Discussion
3.1. Results


{kind=link}
| Histological Diagnoses | Kidney | Ureter | Bladder | Urethra | All | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Both | Male | Female | Both | Male | Female | Both | Male | Female | Both | Male | Female | Both | |
| Benign | |||||||||||||||
| n | 281 | 222 | 503 | 101 | 72 | 173 | 513 | 280 | 793 | 48 | 64 | 112 | 943 | 638 | 1581 |
| % | 27.5 | 44.3 | 33.0 | 68.7 | 80.9 | 73.3 | 29.0 | 53.5 | 34.6 | 72.7 | 86.5 | 80.0 | 31.4 | 53.7 | 37.7 |
| Transitional cell carcinoma | |||||||||||||||
| n | 61 | 29 | 90 | 40 | 14 | 54 | 1171 | 212 | 1383 | 2 | 7 | 9 | 1274 | 262 | 1536 |
| % | 6.0 | 5.8 | 5.9 | 27.2 | 15.7 | 22.9 | 66.2 | 40.5 | 60.3 | 3.0 | 9.5 | 6.4 | 42.4 | 22.1 | 36.6 |
| Renal cell carcinoma | |||||||||||||||
| n | 657 | 239 | 896 | - | - | - | - | - | - | - | - | - | 657 | 239 | 896 |
| % | 64.3 | 47.7 | 58.9 | - | - | - | - | - | - | - | - | - | 21.9 | 20.1 | 21.4 |
| Other malignant | |||||||||||||||
| n | 22 | 11 | 33 | 6 | 3 | 9 | 86 | 31 | 117 | 16 | 3 | 19 | 130 | 48 | 178 |
| % | 2.2 | 2.2 | 2.2 | 4.1 | 3.4 | 3.8 | 4.9 | 5.9 | 5.1 | 24.2 | 4.1 | 13.6 | 4.3 | 4.0 | 4.2 |
| All | |||||||||||||||
| n | 1021 | 501 | 1522 | 147 | 89 | 236 | 1770 | 523 | 2293 | 66 | 74 | 140 | 3004 | 1187 | 4191 |
| % | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| Arsenic Concentration µg/L | Men | Women | Both | All | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TCC | Benign | TCC | Benign | TCC | Benign | |||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| ≤10 | 211 | 17.4 | 126 | 19.0 | 27 | 11.6 | 80 | 19.2 | 238 | 16.5 | 206 | 19.1 | 444 | 17.6 |
| 10 < 50 | 278 | 22.9 | 101 | 15.3 | 41 | 17.6 | 89 | 21.4 | 319 | 22.1 | 190 | 17.6 | 509 | 20.2 |
| 50 < 100 | 177 | 14.6 | 91 | 13.7 | 27 | 11.6 | 54 | 13.0 | 204 | 14.1 | 145 | 13.5 | 349 | 13.8 |
| 100 < 200 | 219 | 18.1 | 154 | 23.3 | 59 | 25.3 | 90 | 21.6 | 278 | 19.2 | 244 | 22.6 | 522 | 20.7 |
| 200 < 300 | 207 | 17.1 | 95 | 14.4 | 44 | 18.9 | 48 | 11.5 | 251 | 17.4 | 143 | 13.3 | 394 | 15.6 |
| 300 or more | 121 | 10.0 | 95 | 14.4 | 35 | 15.0 | 55 | 13.2 | 156 | 10.8 | 150 | 13.9 | 306 | 12.1 |
| Total | 1213 | 100.0 | 662 | 100.0 | 233 | 100.0 | 416 | 100.0 | 1446 | 100.0 | 1078 | 100.0 | 2524 | 100.0 |
| X2 (df = 5) | 28.2 | 13.5 | 23.7 | - | ||||||||||
| tabl | p < 0.001 | p < 0.019 | p < 0.001 | - | ||||||||||
| Men | Women | Both | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Smoking | Non-Smoking | Both | ||||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Arsenic µg/L | ||||||||||
| <10 | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| 10 < 50 | 1.70 | 1.01–2.86 | 1.67 | 0.97–2.89 | 1.68 | 1.14–2.48 | 1.41 | 0.71–2.81 | 1.52 | 1.08–2.14 |
| 50 < 100 | 1.06 | 0.61–1.83 | 1.10 | 0.61–1.97 | 1.05 | 0.68–1.60 | 1.41 | 0.65–3.06 | 1.07 | 0.73–1.57 |
| 100 < 200 | 0.68 | 0.40–1.13 | 0.99 | 0.58–1.69 | 0.80 | 0.54–1.12 | 1.90 | 0.95–3.81 | 0.99 | 0.69–1.41 |
| 200 < 300 | 0.90 | 0.49–1.63 | 2.19 | 1.20–4.01 | 1.29 | 0.81–2.07 | 3.38 | 1.54–7.44 | 1.63 | 1.08–2.46 |
| 300 or more | 0.65 | 0.34–1.25 | 0.65 | 0.34–1.26 | 0.66 | 0.39–1.11 | 2.06 | 0.89–4.78 | 0.89 | 0.55–1.43 |
| Smoking | ||||||||||
| Never | – | – | – | – | 1 | – | – | – | 1 | – |
| Ever | – | – | – | – | 2.47 | 2.00–3.05 | – | – | 2.71 | 2.20–3.33 |
| Sex | ||||||||||
| Female | – | – | – | – | – | – | – | – | 1 | – |
| Male | – | – | – | – | – | – | – | – | 1.46 | 1.16–1.85 |
| Age (years) | 1.03 | 1.02–1.04 | 1.04 | 1.03–1.05 | 1.04 | 1.03–1.04 | 1.05 | 1.04–1.06 | 1.04 | 1.03–1.05 |
| Histological Diagnosis | Origin of Tissue Sample | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kidney | Ureter | Bladder | Urethra | All | |||||||||||
| Mean | SD | n | Mean | SD | n | Mean | SD | n | Mean | SD | n | Mean | SD | n | |
| Benign | |||||||||||||||
| Chronic cystitis | - | - | - | 98.3 | 89.3 | 125 | 153.8 | 137.3 | 726 | 81.5 | 98.1 | 33 | 143.3 | 132.2 | 884 |
| Other | 81.0 | 111.0 | 503 | 65.4 | 102.1 | 48 | 133.4 | 147.5 | 67 | 70.4 | 102.1 | 79 | 83.8 | 114.5 | 697 |
| Transitional cell cancer (TCC) | 158.6 | 137.4 | 90 | 177.9 | 133.8 | 54 | 130.6 | 127.2 | 1383 | 35.9 | 46.7 | 9 | 133.4 | 128.3 | 1536 |
| Renal cell cancer (RCC) | 146.7 | 140.6 | 896 | - | - | - | - | - | - | - | - | - | 146.7 | 140.6 | 896 |
| Other malignant | 86.6 | 116.0 | 33 | 149.4 | 179.7 | 9 | 99.6 | 110.8 | 117 | 83.3 | 105.7 | 19 | 97.9 | 115.1 | 178 |
| All | 124.4 | 134.5 | 1522 | 111.8 | 114.1 | 236 | 136.5 | 131.0 | 2293 | 72.6 | 98.8 | 140 | 128.6 | 131.0 | 4191 |
| Women | Men | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Never Smoker | Ever Smoker | All | |||||||
| Arsenic concentration | n | OR * | 95% CI | OR * | 95% CI | OR * | 95% CI | OR ** | 95% CI |
| <10 µg/L | 206 | 1 | - | 1 | - | 1 | - | 1 | - |
| <50 µg/L | 190 | 0.95 | 0.38–2.41 | 1.28 | 0.47–3.52 | 2.27 | 0.64–8.06 | 1.72 | 0.75–4.00 |
| 50 < 100 µg/L | 145 | 1.24 | 0.41–3.81 | 0.72 | 0.27–1.88 | 1.69 | 0.47–6.10 | 0.96 | 0.42–2.18 |
| ≥100 µg/L | 537 | 2.46 | 1.01–5.97 | 1.73 | 0.73–4.10 | 4.01 | 1.47–10.91 | 2.44 | 1.20–4.94 |
3.2. Discussion
4. Conclusions
Supplementary Files
Supplementary File 1Ethics Statement
Author Contributions
Conflicts of Interest
References
- Mostafa, M.G.; Cherry, N.M. Arsenic in drinking water and renal cancers in rural Bangladesh. Occup. Environ. Med. 2013, 70, 768–773. [Google Scholar] [PubMed]
- IARC. Some Drinking Water Disinfectants and Contaminants, Including Arsenic. In Monographs on the Evaluation of Carcinogenic Risk to Humans; IARC Monographs, IARC: Lyon, France, 2004; Volume 84. [Google Scholar]
- IARC. A Review of Human Carcinogens (Part C): Arsenic, Metals, Fibres, and Dusts. In IARC Working Group on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2009. [Google Scholar]
- Tsuji, J.S.; Alexander, D.D.; Perez, V.; Mink, P.J. Arsenic exposure and bladder cancer: Quantitative assessment of studies in human populations to detect risks at low doses. Toxicology 2014, 317, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Christoforidou, E.P.; Riza, E.; Kales, S.N.; Hadjistavrou, K.; Stoltidi, M.; Kastania, A.N.; Linos, A. Bladder cancer and arsenic through drinking water: A systematic review of epidemiologic evidence. J. Environ. Sci. Health Part A Toxic/Hazard. Subst. Environ. Eng. 2013, 48, 1764–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, H.A.; Crawford-Brown, D.J. Inorganic arsenic in drinking water and bladder cancer: A meta-analysis for dose-response assessment. Int. J. Environ. Res. Public Health 2006, 3, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Burger, M.; Catto, J.W.F.; Dalbangni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; la Vecchia, C.; Shariat, S.; et al. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Kiriluk, K.J.; Prasad, S.M.; Patel, A.R.; Steinberg, G.D.; Smith, N.D. Bladder cancer risk from occupational and environmental exposures. Urol. Oncol. Semin. Orig. Investig. 2012, 30, 199–211. [Google Scholar] [CrossRef] [PubMed]
- Bladder Cancer Incidence Statistics. Available online: http://www.cancerresearchuk.org/cancer-info/cancerstats/types/bladder/incidence (accessed on 15 July 2015).
- Zeegers, M.P.A.; Tan, F.E.S.; Dorant, E.; van Den Brandt, P.A. The impact of characteristics of cigarette smoking on urinary tract cancer Risk: A meta-analysis of epidemiologic studies. Cancer 2000, 89, 630–639. [Google Scholar] [CrossRef]
- Bladder Cancer Statistics. Available online: http://www.wcrf.org/int/cancer-facts-figures/data-specific-cancers/bladder-cancer-statistics (accessed on 15 July 2015).
- Using the on-line ANalysis Function for INcidence Tables by Population. Available online: http://globocan.iarc.fr (accessed on 15 July 2015).
- Zaghloul, M.S. Bladder cancer and schistosomiasis. J. Egypt. Natl. Cancer Inst. 2012, 24, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Kinniburgh, D.G.; Smedley, P.L. Arsenic Contamination of Groundwater in Bangladesh; BGS Technical Report WC/00/19; British Geological Survey: Keyworth, Nottingham, UK, 2001. [Google Scholar]
- World Health Organisation. Arsenic in Drinking-Water. In Background Document for Development of WHO Guidelines for Drinking-Water Quality; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Mostafa, M.G.; McDonald, J.C.; Cherry, N.M. Lung cancer and exposure to arsenic in rural Bangladesh. Occup. Environ. Med. 2008, 65, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Shacter, E.; Weizman, S.A. Chronic inflammation and cancer. Oncology 2002, 16, 217–226. [Google Scholar] [PubMed]
- Michaud, D.S. Chronic inflammation and bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2007, 25, 260–268. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mostafa, M.G.; Cherry, N. Arsenic in Drinking Water, Transition Cell Cancer and Chronic Cystitis in Rural Bangladesh. Int. J. Environ. Res. Public Health 2015, 12, 13739-13749. https://doi.org/10.3390/ijerph121113739
Mostafa MG, Cherry N. Arsenic in Drinking Water, Transition Cell Cancer and Chronic Cystitis in Rural Bangladesh. International Journal of Environmental Research and Public Health. 2015; 12(11):13739-13749. https://doi.org/10.3390/ijerph121113739
Chicago/Turabian StyleMostafa, Mohammad Golam, and Nicola Cherry. 2015. "Arsenic in Drinking Water, Transition Cell Cancer and Chronic Cystitis in Rural Bangladesh" International Journal of Environmental Research and Public Health 12, no. 11: 13739-13749. https://doi.org/10.3390/ijerph121113739