
Arsenic and Other Metals’ Presence in Biomarkers of Cambodians in Arsenic Contaminated Areas

Abstract
:1. Introduction
2. Materials and Methods
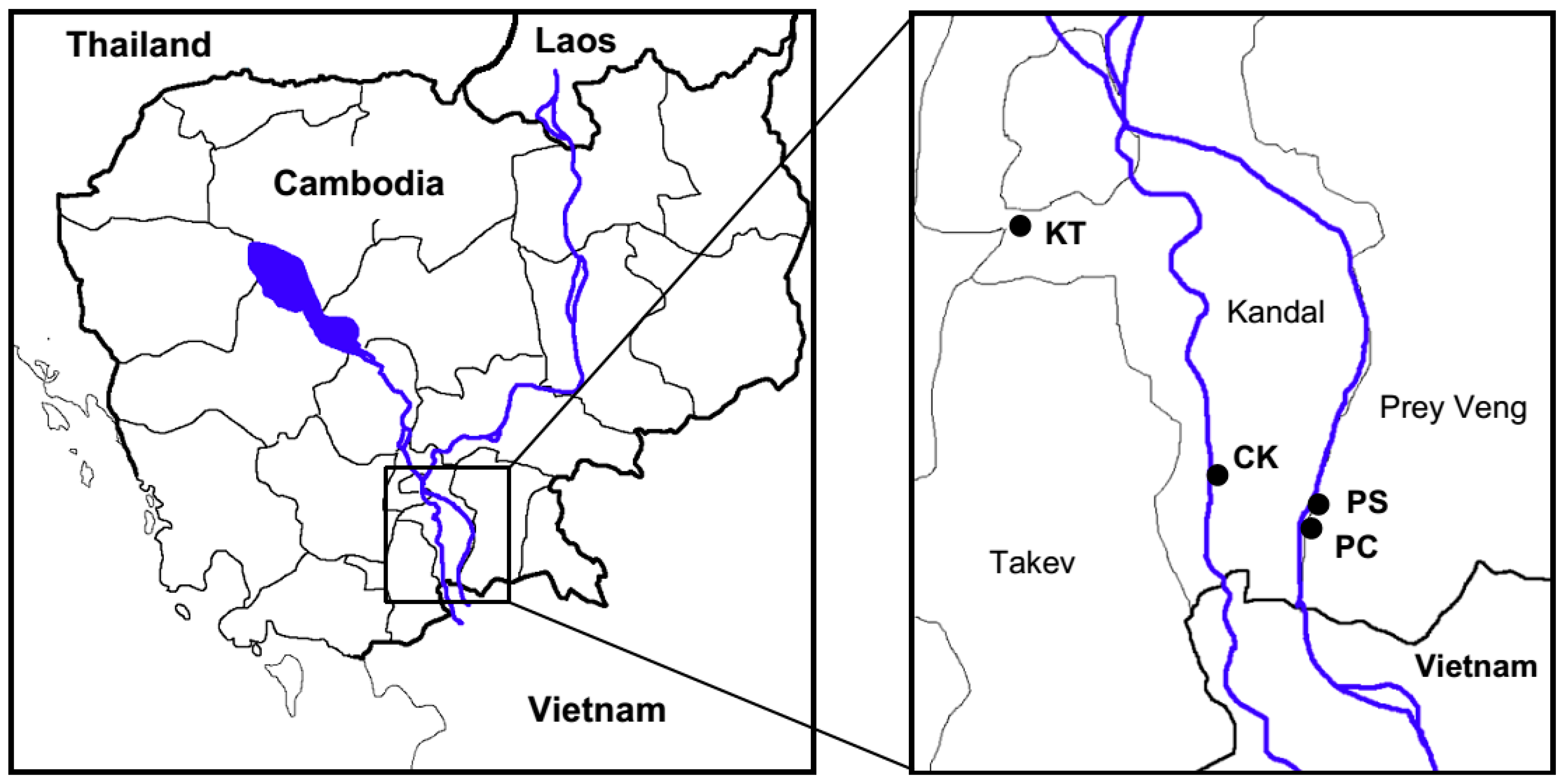
2.1. Study Areas

2.2. Collection of Human Biomarkers
2.3. Collection of Groundwater
2.4. Sample Pre-treatment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Element | Limit of Detection | ||
|---|---|---|---|
| Groundwater (μg·L−1) | Hair and Nails (mg·kg−1) | Urine (ng·mg−1 Creatinine) | |
| Cr | 0.38 | 0.10 | 0.10 |
| Mn | 1.20 | 0.33 | 0.07 |
| Fe | 2.78 | 2.93 | 0.09 |
| Co | 0.32 | 0.01 | 0.04 |
| Ni | 0.34 | 0.02 | 0.01 |
| Cu | 0.29 | 0.12 | 0.04 |
| Zn | 0.33 | 0.14 | 0.09 |
| As | 0.55 | 0.03 | 0.02 |
| Mo | 0.35 | 0.02 | 0.09 |
| Ba | 1.36 | 0.79 | 0.02 |
| Pb | 0.33 | 0.01 | 0.02 |
2.5. Sample Analyses
2.6. Data Analyses
3. Results and Discussion
3.1. Metals Concentrations in Groundwater
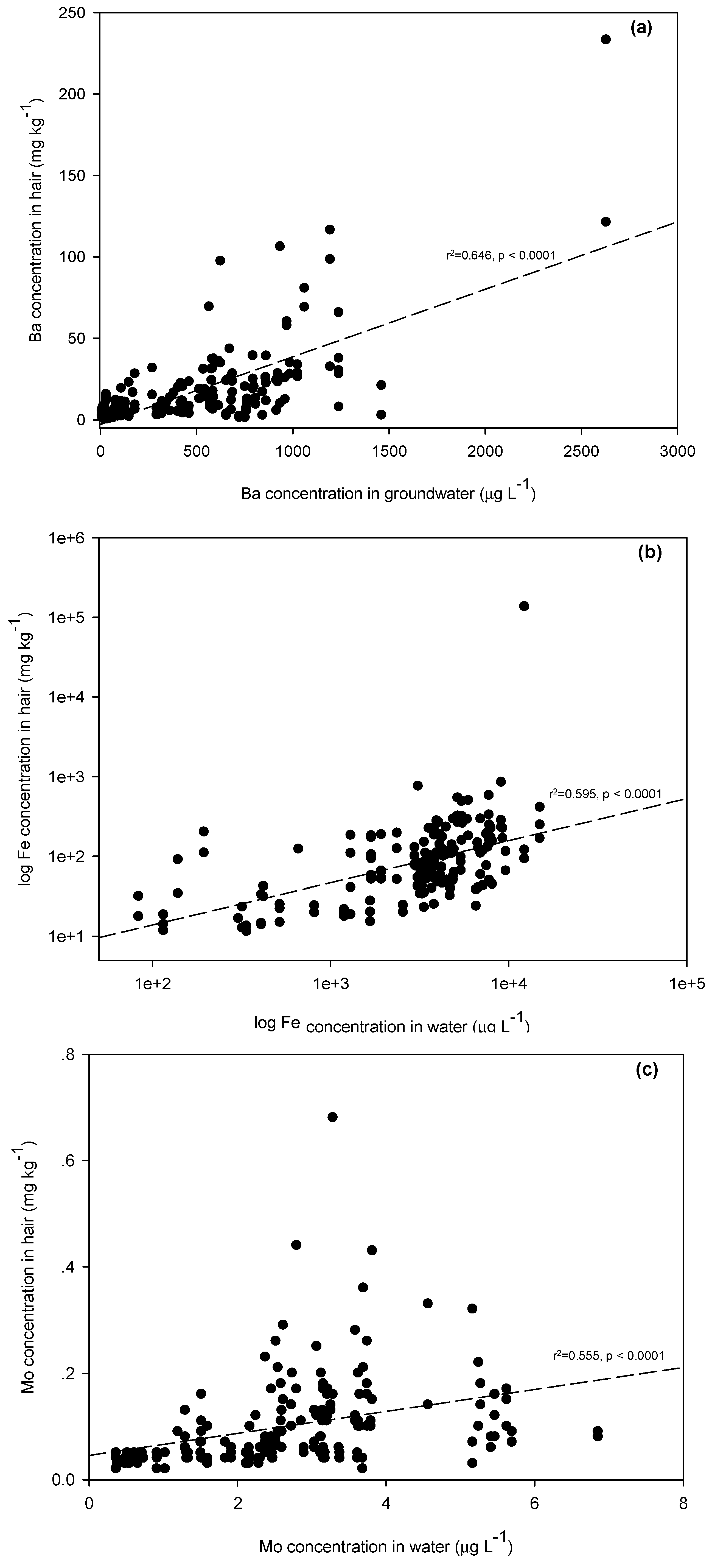
3.2. Metal Concentrations in Hair
| Statistics | Population | Study Area | |||
|---|---|---|---|---|---|
| KT | CK | PC | PS | ||
| Groundwater (μg·L−1) | |||||
| No. of samples | 76 | 12 | 24 | 22 | 18 |
| Min | <LOQ | <LOQ | 402 | 57.93 | 16.02 |
| Max | 997 | 8.36 | 923 | 997 | 959 |
| Mean | 512 | 2.56 | 686 | 587 | 567 |
| Median | 591 | 1.24 | 700 | 650 | 616 |
| SE | 22.13 | 0.44 | 19.23 | 32.68 | 32.04 |
| Hair (mg·kg−1) | |||||
| No. of samples | 180 | 30 | 50 | 50 | 50 |
| Min | 0.03 | 0.03 | 0.65 | 0.27 | 0.23 |
| Max | 56.75 | 0.41 | 56.75 | 22.69 | 12.94 |
| Mean | 5.93 | 0.17 | 9.69 | 7.37 | 4.19 |
| Median | 4.18 | 0.16 | 6.37 | 6.78 | 4.12 |
| SE | 0.52 | 0.02 | 1.44 | 0.79 | 0.36 |
| Nails (mg·kg−1) | |||||
| No. of samples | 176 | 27 | 49 | 50 | 50 |
| Min | 0.11 | 0.11 | 0.77 | 1.14 | 0.55 |
| Max | 23.24 | 0.88 | 23.24 | 18.48 | 14.41 |
| Mean | 4.14 | 0.37 | 5.47 | 4.72 | 4.29 |
| Median | 3.04 | 0.31 | 3.84 | 3.40 | 3.61 |
| SE | 0.30 | 0.04 | 0.72 | 0.49 | 0.45 |
| Urine (ng·mg−1 creatinine) | |||||
| No. of samples | 180 | 30 | 50 | 50 | 5 |
| Min | 22.26 | 30.22 | 22.26 | 52.51 | 46.76 |
| Max | 995 | 995 | 448 | 689 | 407 |
| Mean | 124 | 107 | 81.07 | 199 | 103 |
| Median | 86.77 | 60.04 | 64.40 | 159 | 84.02 |
| SE | 9.21 | 32.32 | 8.64 | 20.63 | 8.97 |


3.3. Metal Concentrations in Nails
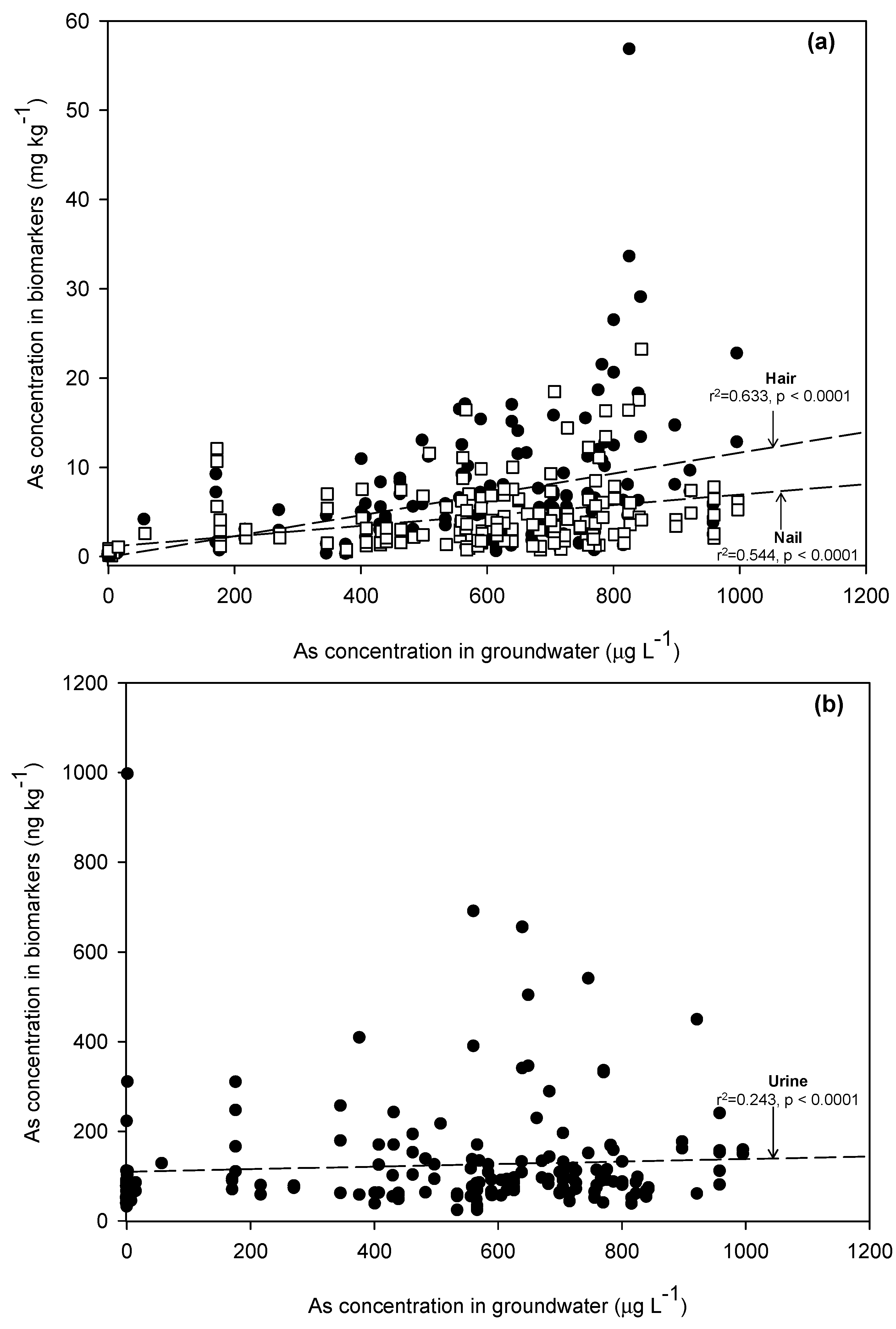
3.4. Arsenic Concentrations in Urine
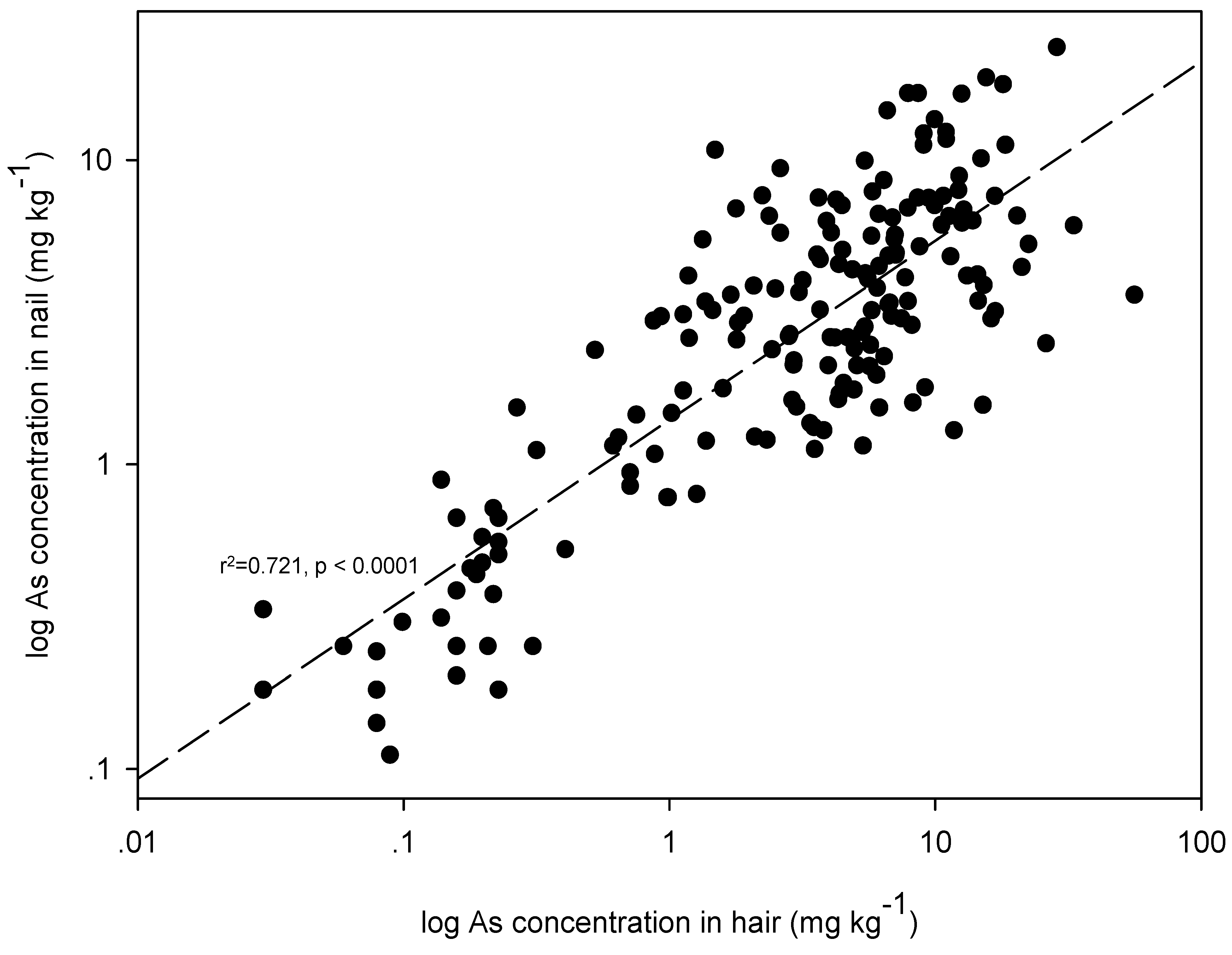
3.5. Comparison of Metal Concentrations in Biomarkers and Agreement among Different Biomarkers
| Biomarker | As | Ba | Cr | Mn | Fe | Co | Ni | Cu | Zn | Mo | Pb |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hair | 0.633 ** | 0.646 ** | −0.388 ** | 0.234 ** | 0.595 ** | 0.149 | −0.287 ** | −0.017 | 0.132 | 0.555 ** | 0.027 |
| Nail | 0.544 ** | 0.306 ** | −0.111 | −0.073 | 0.296 ** | −0.176 ** | −0.202 ** | −0.076 | 0.008 | 0.082 | −0.004 |
| Urine | 0.243 ** | −0.104 | 0.018 | 0.008 | 0.033 | 0.112 | −0.014 | −0.103 | −0.014 | 0.122 | 0.031 |
| Metal | Statistical Analyses for Comparisons Of Metal Concentrations in Each Pair of Biomarkers (Z− and p−Values) | Order of Biomarkers by Concentration of Each Metal | ||
|---|---|---|---|---|
| Hair−Nail | Hair-Urine | Nail-Urine | ||
| Cr | −10.459; <0.0001 | −10.596; <0.0001 | −2.215; 0.027 | Hair < Nail < Urine |
| Mn | −1.970; 0.049 | −10.738; <0.0001 | −10.617; <0.0001 | Urine < Hair < Nail |
| Fe | −11.096; <0.0001 | −4.868; <0.0001 | −11.237; <0.0001 | Urine < Hair < Nail |
| Co | −10.992; <0.0001 | −11.557; <0.0001 | −1.337; <0.0001 | Hair < Nail < Urine |
| Ni | −6.158; <0.0001 | −11.456; <0.0001 | −11.078; <0.0001 | Hair < Nail < Urine |
| Cu | −10.565; <0.0001 | −2.247; 0.025 | −9.728; <0.0001 | Urine < Hair < Nail |
| Zn | −10.954; <0.0001 | −3.560; <0.0001 | −11.272; <0.0001 | Nail < Hair < Urine |
| As | −3.427; <0.0001 | −11.635; <0.0001 | −11.505; <0.0001 | Nail < Hair < Urine |
| Mo | −7.434; <0.0001 | −11.635; <0.0001 | −11.505; <0.0001 | Nail < Hair < Urine |
| Ba | −1.848; 0.065 | −0.895; 0.371 | −2.649; 0.008 | Nail < Hair < Urine |
| Pb | −7.837; <0.0001 | −2.103; 0.035 | −6.093; <0.0001 | Urine < Hair < Nail |
| Biomarker | As | Ba | Cr | Mn | Fe | Co | Ni | Cu | Zn | Mo | Pb |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hair-Nail | 0.721 ** | 0.341 ** | 0.067 | 0.315 ** | 0.358 ** | 0.203 ** | 0.079 | 0.102 | −0.019 | 0.079 | 0.276 ** |
| Hair-Urine | 0.275 ** | −0.069 | 0.023 | 0.057 | 0.099 | 0.038 | −0.034 | −0.018 | −0.079 | 0.069 | −0.026 |
| Nail-Urine | 0.297 ** | −0.112 | −0.077 | −0.096 | −0.030 | −0.084 | 0.033 | −0.082 | 0.078 | 0.006 | −0.134 |

4. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Briggs, D. Environmental pollution and the global burden of disease. Brit. Med. Bull. 2003, 68, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Schmoll, O.; Howard, G.; Chilton, G.; Chorus, I. Protecting Groundwater for Health: Managing the Quality of Drinking-water Resources; World Health Organization: London, UK, 2006. [Google Scholar]
- Polya, D.A.; Gault, A.G.; Diebe, N.; Feldman, P.; Rosenboom, J.W.; Gilligan, E.; Fredericks, D.; Milton, A.H.; Sampson, M.; Rowland, H.A.L.; et al. Arsenic hazard in shallow Cambodian groundwaters. Mineral. Mag. 2005, 695, 807–823. [Google Scholar] [CrossRef]
- Berg, M.; Stengel, C.; Pham, T.K.; Pham, H.V.; Sampson, M.L.; Leng, M.; Semreth, S.; Fredericks, D. Magnitude of Arsenic Pollution in the Mekong and Red River Deltas-Cambodia and Vietnam. Sci. Total Environ. 2007, 372, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Buschmann, J.; Berg, M.; Stengel, C.; Winkel, L.; Sampson, M.L.; Trang, P.T.; Viet, P.H. Contamination of drinking water resources in the Mekong delta floodplains: Arsenic and other trace metals pose serious health risks to population. Environ. Int. 2008, 346, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Sthiannopkao, S.; Kim, K.W.; Sotham, S.; Choup, S. Arsenic and manganese in tube well waters of Prey Veng and Kandal Provinces, Cambodia. Appl. Geochem. 2008, 235, 1086–1093. [Google Scholar] [CrossRef]
- Luu, T.T.; Sthiannopkao, S.; Kim, K.W. Arsenic and other trace elements contamination in groundwater and a health risk assessment study for the residents in the Kandal Province of Cambodia. Environ. Int. 2009, 35, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Sthiannopkao, S.; Kim, K.W.; Wong, M.H.; Sao, V.; Hashim, J.H.; Mohamed, Y.M.S.; Aljunid, S.M. Health risk assessment of inorganic arsenic intake of Cambodia residents through groundwater drinking pathway. Water Res. 2010, 44, 5777–5788. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.W.; Chanpiwat, P.; Hanh, H.T.; Phan, K.; Sthiannopkao, S. Arsenic geochemistry of groundwater in Southeast Asia. Front. Med. 2011, 54, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Adriano, D.C. Trace Elements in Terrestrial Environments: Biogeochemistry, Bioavailability, and Risks of Metals, 2nd ed.; Springer-Verlag: New York, NY, USA, 2001. [Google Scholar]
- Issue Paper on the Human Health Effects of Metals. Available online: http://www2.epa.gov/osa/issue-paper-human-health-effects-metals (accessed on 1 September 2015).
- Gil, F.; Pla, A. Biomarkers as biological indicators of xenobiotics exposure. J. Appl. Toxicol. 2001, 21, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Angerer, J.; Ewers, U.; Wilhelm, M. Human biomonitoring: State of the art. Int. J. Hgy. Environ. Health 2007, 210, 201–228. [Google Scholar] [CrossRef] [PubMed]
- Esteban, M.; Castano, A. Non-invasive matrices in human biomonitoring: A review. Environ. Int. 2009, 35, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Clewell, H.J.; Tan, Y.M.; Campbell, J.L.; Andersen, M.E. Quantitative interpretation of human biomonitoring data. Int. J. Hgy. Environ. Health 2008, 231, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Smolders, R.; Schramm, K.W.; Nickmilder, M.; Schoeters, G. Applicability of non-invasively matrices for human biomonitoring. Environ. Health 2009, 8. [Google Scholar] [CrossRef] [PubMed]
- Marchiset-Ferlay, M.; Savanovitch, C.; Sauvant-Rochat, M.P. What is the best biomarker to assess arsenic exposure via drinking water. Environ. Int. 2012, 35, 150–171. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Kim, K.W.; Hashim, J.H. Environmental arsenic epidemiology in the Mekong river basin of Cambodia. Environ. Res. 2014, 135, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Kim, K.W.; Huoy, L.; Phan, S.; Se, S.; Capon, A.G.; Hashim, J.H. Current status of arsenic exposure and social implication in the Mekong River basin of Cambodia. Environ. Geochem. Health 2015, 8. [Google Scholar] [CrossRef] [PubMed]
- Samanta, G.; Sharma, R.; Roychowdhury, T.; Chakraborti, D. Arsenic and other elements in hair, nails, and skin-scales of arsenic victims in West Bengal, India. Sci. Total Environ. 2004, 326, 33–47. [Google Scholar] [CrossRef] [PubMed]
- Gault, A.G.; Rowland, H.A.L.; Charnock, J.M.; Wogelius, R.A.; Gomez-Morilla, I.; Vong, S.; Leng, M.; Samreth, S.; Sampson, M.L.; Polya, D.A. Arsenic in hair and nails of individuals exposed to arsenic-rich groundwaters in Kandal province, Cambodia. Sci. Total Environ. 2008, 393, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.L.; Amarasiriwardena, C.J.; Christiani, D.C. Determination of total arsenic concentrations in nails by inductively coupled plasma mass spectrometry. Biol. Trace Elem. Res. 1999, 67, 109–125. [Google Scholar] [CrossRef] [PubMed]
- Hossain, E.; Islam, K.; Yeasmin, F.; Karim, M.R.; Rahman, M.; Agarwal, S.; Hossain, S.; Aziz, A.; Mamun, A.A.; Sheikh, A.; et al. Elevated levels of plasma Big endothelin-1 and its relation to hypertension and skin lesions in individuals exposed to arsenic. Toxicol. Appl. Pharm. 2012, 259, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Drinking-Water Quality. Available online: http://www.who.int/water_sanitation_health/publications/2011/dwq_guidelines/en/ (accessed on 1 September 2015).
- Phan, K.; Phan, S.; Heng, S.; Huoy, L.; Kim, K.W. Assessing arsenic intake from groundwater and rice by residents in Prey Veng province, Cambodia. Environ. Pollut. 2014, 185, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Phan, S.; Huoy, L.; Suy, B.; Wong, M.H.; Hashim, J.H.; Yasin, M.S.M.; Aljunid, S.M.; Sthiannopkao, S.; Kim, K.W. Assessing mixed trace elements in groundwater and their health risk of residents living in the Mekong River basin of Cambodia. Environ. Pollut. 2013, 182, 111–119. [Google Scholar] [CrossRef] [PubMed]
- ATSDR. ToxGuide™ for Arsenic. Available online http://www.atsdr.cdc.gov/toxguides/toxguide-2.pdf (accessed on 1 September 2015).
- Sthiannopkao, S.; Kim, K.W.; Cho, K.H.; Wantala, K.; Sotham, S.; Sokuntheara, C.; Kim, J.H. Arsenic levels in human hair, Kandal province, Cambodia: The influences of groundwater arsenic, consumption period, age and gender. Appl. Geochem. 2010, 25, 81–90. [Google Scholar] [CrossRef]
- Sampson, M.L.; Bostick, B.; Chiew, H.; Hagan, J.M.; Shantz, A. Arsenicosis in Cambodia: Case studies and policy response. Appl. Geochem. 2008, 23, 2977–2986. [Google Scholar] [CrossRef]
- Hughes, M.F. Biomarkers of exposure: A case study with inorganic arsenic. Environ. Health Perspect. 2006, 114, 1790–1796. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.; Costa, S.; Silva, S.; Walter, A.; Ranville, J.; Sousa, A.C.A.; Costa, C.; Coelho, M.; Garcia-Leston, J.; Pastorinho, M.R.; et al. Metal(Loid) levels in biological matrices from human populations exposed to mining contamination—Panasqueira Mine (Portugal). J. Toxicol. Environ. Health A 2012, 75, 893–908. [Google Scholar] [CrossRef] [PubMed]
- Looney, S.W. Statistical methods for assessing biomarkers. Methods Mol. Biol. 2002, 184, 81–109. [Google Scholar] [PubMed]
- Phan, K.; Sthiannopkao, S.; Kim, K.W. Surveillance on chronic arsenic exposure in the Mekong River basin of Cambodia using different biomarkers. Int. J. Hyg. Environ. Health 2011, 215, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.S.; Sthiannopkao, S.; Chen, Z.J.; Man, Y.B.; Du, J.; Xing, G.H.; Kim, K.W.; Mohammad, Y.M.S.; Hashim, J.H.; Wong, M.H. Arsenic concentrations in rice fish, and meat and vegetables in Cambodia: A study risk assessment. Environ. Geochem. Health 2013, 35, 745–755. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chanpiwat, P.; Himeno, S.; Sthiannopkao, S. Arsenic and Other Metals’ Presence in Biomarkers of Cambodians in Arsenic Contaminated Areas. Int. J. Environ. Res. Public Health 2015, 12, 14285-14300. https://doi.org/10.3390/ijerph121114285
Chanpiwat P, Himeno S, Sthiannopkao S. Arsenic and Other Metals’ Presence in Biomarkers of Cambodians in Arsenic Contaminated Areas. International Journal of Environmental Research and Public Health. 2015; 12(11):14285-14300. https://doi.org/10.3390/ijerph121114285
Chicago/Turabian StyleChanpiwat, Penradee, Seiichiro Himeno, and Suthipong Sthiannopkao. 2015. "Arsenic and Other Metals’ Presence in Biomarkers of Cambodians in Arsenic Contaminated Areas" International Journal of Environmental Research and Public Health 12, no. 11: 14285-14300. https://doi.org/10.3390/ijerph121114285