
Community, State, and Federal Approaches to Cumulative Risk Assessment: Challenges and Opportunities for Integration

Abstract
:1. Introduction
2. Background
2.1. Cumulative versus Conventional Risk Assessment

2.2. Multiple-Risk Quantification and Decision Analysis
2.3. Environmental Justice
3. Methods
3.1. Community
3.1.1. Stressor Quantification

{kind=link}
| Study & Topics | Purpose or Problem | Study Design | Primary Findings |
|---|---|---|---|
| Sadd et al., (2011) [3] Air and Social Environment | Development of the Environmental Justice Screening Method (EJSM) to Examined the relative rank of cumulative impacts and social vulnerability within metropolitan regions. | EJSM uses 23 health, environmental and social vulnerability measures organized along three categories: (1) hazard proximity and land use; (2) estimated air pollution exposure and health risk; and (3) social and health vulnerability in the Los Angeles area. | Areas with high hazard proximity and sensitive land use scores correspond to Areas with high hazard proximity and sensitive land use scores corresponded with dense populations and major industrial centers or transportation corridors. Health risk and exposure scores had little fine-scale variation and broad areas with a single score. Cumulative impact (CI) scores were normally distributed, with highest scores corresponding to communities near ports and airports. |
| Clougherty et al., (2007) [19] Air, Social Environment, and Health Impacts | Examined the role of exposure to violence (ETV), a chronic stressor, in altering susceptibility to traffic-related air pollution in asthma etiology. | GIS-based models estimated residential exposures to traffic-related pollution for 413 children in East Boston, MA, between 1987 and 1993, using monthly NO2 measurements for 13 sites over 18 years. Pollution estimates were merged with questionnaire data on lifetime exposure to violence, and effects of both on childhood asthma etiology were examined. | Found elevated risk of asthma with a one standard deviation (4.3 ppb) increase in NO2 exposure among children with above-median ETV (odds ratio = 1.63; 95% confidence interval = 1.14–2.33). Demonstrated an association between traffic-related air pollution and asthma solely among urban children exposed to violence. |
| Clougherty and Kubzansky (2009) [20] Health Impacts and Social Environment | Synthesized relevant research from social and environmental epidemiology, toxicology, immunology, and exposure assessment to provide a framework for environmental health researchers aiming to investigate health effects of environmental pollution combined with social or psychological factors. | Reviewed existing epidemiologic and toxicological evidence on synergistic effects of stress and pollution. | Described Physiologic effects of stress. Addressed key issues related to measuring and evaluating stress as it relates to physical environmental exposures and susceptibility. |
| Brody et al., (2009) [21] Air and Health Impacts | Tested for chemical markers of oil refinery emissions in homes; characterized cumulative effects of emissions in an EJ community by measuring a large and diverse set of pollutants from outdoor and indoor sources; assessed geographic and sociodemographic differences in endocrine disrupting compound (EDC) exposures. | The investigators analyzed indoor and outdoor air from 40 homes in industrial Richmond, CA, and 10 in rural Bolinas, CA, for 153 compounds, including particulates and endocrine disruptors. | Detected eighty outdoor compounds in Richmond and 60 in Bolinas; Richmond concentrations were generally higher, due to heavy oil combustion from oil refining and shipping. Paired outdoor-indoor measurements were correlated to industry- and traffic-related pollutants. Indoor air quality is an important indicator of the cumulative impact of outdoor emissions in fence-line communities. |
| Morello-Frosch and Shenassa (2006) [22] Psychosocial Stressors and Environmental Hazards | Presented evidence that individual-level and place-based psychosocial stressors may combine with environmental pollutants and have adverse health effects, explaining maternal and child health (MCH) disparities. | Proposed a conceptual framework for holistic approaches to future MCH research that elucidates the interplay of psychosocial stressors and environmental hazards to better explain drivers of MCH disparities. | Suggested that a holistic approach to future MCH research that seeks to untangle the double jeopardy of chronic stressors and environmental hazard exposures could help elucidate how the interplay of these factors shapes persistent racial and economic disparities in MCH. |
| Su et al., (2009) [23] Air and Social Environment | Proposes an index to assess cumulative environmental hazard inequalities in socially disadvantaged groups and neighborhoods in the Los Angeles region of California. | Extended the concentration index to summarize inequality in the distribution of multiple pollutants across socioeconomic and racial/ethnic groups. Index used population ranked by area-based racial, ethnic or socioeconomic composition, and the cumulative environmental hazard, aggregated with various weighting functions. | Analyzed single and cumulative environmental inequalities in exposure to NO2, PM2.5 and diesel PM; cancer risk; poverty measures; and racial/ethnic population composition. Environmental inequality curves were significantly different from the equality line. Demonstrated that environmental inequalities exist for non-white populations as well as for poorer populations in Los Angeles. |
| Fox et al., (2002) [24] Health Impacts | Advanced CRA methods and tested their application in a community case study. Cumulative risk and health assessments were compared for south and southwest Philadelphia communities. | Obtained mortality data by from the city of Philadelphia, using deaths for 1990 ( n = 3151) and for 1988–1992 (n = 16,168). Used air pollutant data for all census tracts as a proxy for human exposure. Conducted cumulative risk scoring using two toxicological databases, a multi-end point toxicological database and the EPA Cumulative Exposure Toxicity Database (CETDB). | Analysis found correlations between cumulative risk and mortality measurements for whites and non-whites when risk when using the multi-end point toxicological database. Statistically significant increases in total and respiratory mortality were associated with increases in cumulative risk scores. Regression analyses that controlled for percent non-white population and per capita income indicated that environmental effects on health were independent of race and income. |
| Krieg and Faber (2004) [25] Toxic Sites | The EJ literature is characterized by a failure to measure overall impact from an extensive range of ecological hazards effectively. Limitations on available data make this a serious problem for present and future studies. | Developed and implemented a cumulative measure of negative environmental impacts by controlling for the density and severity of ecological hazardous sites and facilities within every community in the state. | Found that exposure patterns take a generally linear distribution when analyzed by race and class. Findings suggest that environmental injustice existed on a consistent continuum for nearly all communities. |
3.1.2. Stakeholder Engagement
3.2. State
3.2.1. Policies and Regulations
3.2.2. Analytical Methods and Decision-Making
3.3. Federal
3.3.1. Federal Insecticide, Fungicide, and Rodenticide Act/Pesticides
3.3.2. Clean Water Act
3.3.3. Safe Drinking Water Act
3.3.4. Comprehensive Environmental Response, Compensation, and Liability Act (Superfund)
3.3.5. Clean Air Act
3.3.6. National Environmental Policy Act
4. Results
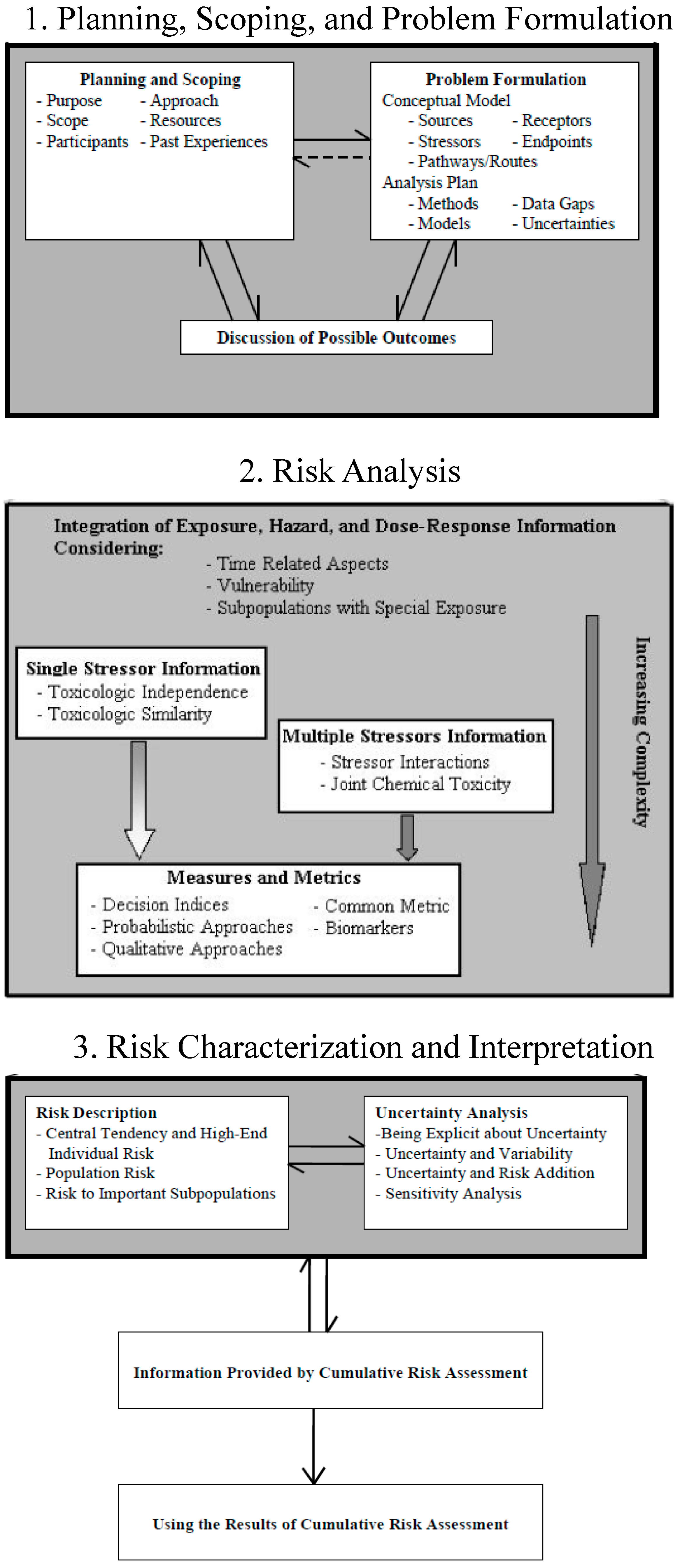
4.1. CRA Planning, Scoping, and Problem Formulation
4.2. CRA Risk Analysis
4.3. CRA Risk Characterization, Interpretation, and Management
| Planning, Scoping, Problem Formulation Elements | Community | State | Federal |
|---|---|---|---|
| Planning and Scoping | |||
| Purpose | Improve community health | Allocate/distribute resources to protect residents from environmental harm | Maximal protection of population as a whole; improve conditions at local levels |
| Scope | Neighborhood area(s); current conditions; historical exposures; future projections; population-based; precautionary | Geo-political boundaries; community scales; urban, suburban, and rural scales; pollution regulation; land maintenance; infrastructure; transportation; social, environmental, and economic considerations (i.e., sustainability) for planning | Sector and chemical-driven protection; cost-effective solutions (e.g., CAA); principally reactive in origin (e.g., CERCLA); predictive as well (e.g., MOA grouping in FIFRA); agencies adopting local-scale principals (e.g., Superfund RAGS) |
| Participants | Local residents (e.g., Chester, PA); agencies (e.g., South Baltimore); academics and health departments (e.g., Spartanburg, SC) | Representative councils (e.g., EJAC); stakeholder input (e.g., EJSM) Locally-driven initiatives (e.g., BAAQMD) | Expert solicitation (e.g., SDWA); local considerations (e.g., NEPA) Multi-stakeholder involvement (e.g., SARA) |
| Approach | Participatory | Interactive | Reflective |
| Resources | Human; financial; technical; political | Policy-driven allocation | Distributed across agencies |
| Past Experiences | Anecdotal; perceived risk; historical perspectives on exposure; local knowledge of health and environment | Multi-faceted (social, environmental, economic) perspective on impacts and decision-making | Historical records and lessons learned domestically and abroad |
| Problem Formulation | |||
| Conceptual Model Sources Stressors Pathways/Routes Receptors Endpoints | Network of partners and collaborators; linkages between stressors and solutions | Environmental and health predictions with sustainability considerations | Establish baseline and modifications to exposure/response due to multiple stressors |
| Analysis Plan Methods Models Data Gaps Uncertainties | Data informs decision-making and defense of risk analysis, characterization, and management options | Data identifies populations of interest and informs allocation of resources | Quantitative approaches with modes of action (MOAs) and maximum contaminant level goals (MCLGs) inform standards |
| Discussion of Possible Outcomes | Develop and adopt local initiatives/policies implemented by residents or government; work with intentionality | Achieve sustainable use of available social, environmental, and economic resources | Protect human health and environment across country, while maintaining global perspective |
| Risk Analysis Elements | Community | State | Federal |
|---|---|---|---|
| Integration of Exposure, Hazard, and Dose-Response Information Considering: | |||
| Time Related Aspects Vulnerability Subpopulations with Special Features | Analytic-deliberative methods linking decision analysis and risk assessment | Indexes of cumulate risk (e.g., EJSM); indicators and surrogates as proxies for exposure and risk | Providing protective standards for human health based on best available toxicity and exposure relationships |
| Single Stressor Information | |||
| Toxicological Independence Toxicological Similarity | Chemical mixtures from multiple sources; non-chemical stressors and other exposure/response modifiers | Implement regulations with permitting, oversight, management, and public initiatives or programs | Regulations and mixtures limited to chemically similar stressors (e.g., pesticides); also site- or source-specific (e.g., Superfund, CAA) |
| Multiple Stressor Information | |||
| Stressor Interactions Joint Chemical Toxicity | Relative risk of stressors for prioritization of actions; determination of environmental impacts on health | Consideration of social determinants of health | Determination of environmental impacts on health |
| Measures and Metrics | |||
| Decision Indices Probabilistic Approaches Qualitative Approaches Common Metric Biomarkers | Data collection and consolidation informs decision making and supports local initiatives | Consolidation of multiple aspects of sustainability addresses state-level decisions about resources and priorities | Impact-driven assessments of environmental stressors on human health and ecosystems |
| Risk Characterization and Interpretation Elements | Community | State | Federal |
|---|---|---|---|
| Risk Description | |||
| Central Tendency and High-End Individual Risk Population Risk Risk to Important Subpopulations | Multiroute chemical risk assessments; poverty and race/ethnicity considerations; children and elderly; mortality/morbidity clusters | Sensitive/vulnerable population groups; socioeconomic factors; multiple emissions and discharges; current and future conditions | Standards to protect most sensitive populations (e.g., SDWA); aggregate exposure regulations (e.g. FQPA); reasonably anticipated adverse effects (e.g., CWA Sn. 405); primary standards to protect children, elderly, asthmatics |
| Uncertainty Analysis | |||
| Being Explicit about Uncertainty Uncertainty and Variability Uncertainty and Risk Addition Sensitivity Analysis | GIS-based analyses; local health and emissions records; deviations from baseline or more ideal conditions; proxies for exposure; measurements and sensors increase certainty | Indicators or surrogates of exposure, such as hazard proximity and air pollution exposure estimates; resolution suitable for targeting and implementation of policy | Economic, social, and environmental conditions are interrelated, producing direct, indirect and cumulative effects |
| Information Provided by CRA | Stressor, asset, and resource identification; absolute or relative ranking; remediation options | Identification of at-risk individuals or populations; weighting of risk based socio-economic, health, and environmental conditions | Systematic, interdisciplinary approaches; integration of natural, social, and environmental sciences and designs |
| Using the Results of CRA | Solution-oriented, data-supported, value-driven decision-making | Implementation of exposure and risk reduction actions; source attribution; protective standards for land use or other policies | Dose addition with relative potency and toxic equivalency factors or to develop a hazard index; stakeholder feedback and participation to inform research and development that supports local efforts |
5. Discussion
5.1. Similarities and Differences in Community, State, and Federal CRA Phases
5.2. Research Gaps and Recommendations for a Consistent CRA Process
- Define Purpose—the main goal of the CRA around which analysis, characterization, and management are implemented.
- Define Objectives—objectives of each group and individual, for transparency and in support of the purpose; to extent possible, these should be achievable and measureable.
- Engage Partnership—determine the core personnel responsible for conducting the CRA and seeing it through to completion, and identify stakeholders, experts, agencies and others to invite, either as ongoing partners or as consultants on specific topics or for a limited timeframe.
- Define Roles and Responsibilities—clearly articulate the role of each partner in conducting the CRA, and the specific responsibilities for which they will be held accountable.
- Determine Scope—temporal (e.g., historical, current, or future conditions), spatial (e.g., neighborhood, state, or national), receptors (e.g., defined community or sensitive subpopulations), and the level of information/quantification needed to make a decision (e.g., qualitative informational evidence, semi-quantitative indicators or surrogates, or quantitative absolute toxicological risk estimates).
- Identify Stressors and Assets—create a broad list of the primary issues of concern, and identify any related and possibly synergistic or antagonistic stressors or assets, respectively (assets are benefits to a CRA, either by reducing a risk or building capacity to address them); a conceptual model is often useful, but not necessary for this step.
- Rank Stressors—implement a meaningful risk ranking methodology; because of the analytic-deliberative nature of CRAs, it is advisable to develop methods that can consolidate multiple stressors into a single risk estimate, as well as to develop methods to assess the relative risk between stressors, which can be accomplished by integrating risk assessment and decision analysis into a common framework.
- Prioritize Solutions—use results of the stressor ranking to develop and prioritize solutions, based on the ability of risk-reduction efforts to address multiple stressors, high-ranking stressors, or on the feasibility of implementation (i.e., taking actions against risks that can easily be targeted with available resources in order to build capacity and remediate obvious stressors first).
- Summarize Analysis Plan—based on information collected and analytic-deliberative outcomes, detail the precise approach required to perform the CRA.
- Evaluate Results of Risk Reduction Actions—after implementing solutions and risk management options, develop measures of success to track effectiveness and adapt planning.
6. Conclusions
7. Disclaimer
Acknowledgments
Author Contributions
Conflicts of Interest
References
- U.S. Environmental Protection Agency. Office of Research and Development. Risk Assessment Forum, Framework for Cumulative Risk Assessment. Available online: http://www.epa.gov/raf/publications/framework-cra.htm (accessed on 22 April 2015).
- Callahan, M.A.; Sexton, K. If cumulative risk assessment is the answer, what is the question? Environ. Health Perspect. 2007, 115, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Sadd, J.L.; Pastor, M.; Morello-Frosch, R.; Scoggins, J.; Jesdale, B. Playing it safe: Assessing cumulative impact and social vulnerability through an environmental justice screening method in the south coast air basin, California. Int. J. Environ. Res. Public Health 2011, 8, 1441–1459. [Google Scholar] [CrossRef] [PubMed]
- Faust, J.B. Perspectives on cumulative risks and impacts. Int. J. Toxicol. 2010, 29, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Sexton, K.; Linder, S.H. The role of cumulative risk assessment in decisions about environmental justice. Int. J. Environ. Res. Public Health 2010, 7, 4037–4049. [Google Scholar] [CrossRef] [PubMed]
- Sexton, K.; Linder, S.H. Cumulative risk assessment for combined health effects from chemical and nonchemical stressors. Am. J. Public Health 2011, 101, S81–S88. [Google Scholar] [CrossRef] [PubMed]
- Sexton, K. Cumulative risk assessment: An overview of methodological approaches for evaluating combined health effects from exposure to multiple environmental stressors. Int. J. Environ. Res. Public Health 2012, 9, 370–390. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Concepts, Methods and Data Sources for Cumulative Health Risk Assessment of Multiple Chemicals, Exposures and Effects: A Resource Document. Available online: http://cfpub.epa.gov/ncea/cfm/recordisplay.cfm?deid=190187 (accessed on 22 April 2015).
- Heaney, C.D.; Wilson, S.M.; Wilson, O.R. The west end revitalization association’s community-owned and-managed research model: Development, implementation, and action. Progr. Community Health Partnersh. Res. Educ. Action 2007, 1, 339–349. [Google Scholar] [CrossRef]
- Israel, B.A.; Eng, E.; Schulz, A.J.; Parker, E.A.; Satcher, D. Methods in Community-Based Participatory Research; Jossey-Bass.: San Francisco, CA, USA, 2005. [Google Scholar]
- O’Fallon, L.R.; Dearry, A. Community-based participatory research as a tool to advance environmental health sciences. Environ. Health Perspect. 2002, 110, S155–S159. [Google Scholar] [CrossRef]
- Srinivasan, S.; Collman, G.W. Evolving partnerships in community. Environ. Health Perspect. 2005, 113, 1814–1816. [Google Scholar] [CrossRef]
- Wilson, S.M.; Wilson, O.R.; Heaney, C.D.; Cooper, J. Use of EPA collaborative problem-solving model to obtain environmental justice in North Carolina. Prog. Community Health Partnersh. Res. Educ. Action 2007, 1, 327–337. [Google Scholar] [CrossRef]
- Renn, O. A model for an analytic-deliberative process in risk management. Environ. Sci. Technol. 1999, 33, 3049–3055. [Google Scholar] [CrossRef]
- Dake, K. Orienting dispositions in the perception of risk an analysis of contemporary worldviews and cultural biases. J. Cross-Cult. Psychol. 1991, 22, 61–82. [Google Scholar] [CrossRef]
- Drottz-Sjöberg, B.-M. Perception of Risk: Studies of Risk Attitudes, Perceptions and Definitions; Center for Risk Research: Stokholm, Sweden, 1991. [Google Scholar]
- Bullard, R.D.; Warren, R.C.; Johnson, G.S. The Quest for Environmental Justice: Human Rights and the Politics of Pollution; Counterpoint Press: Berkeley, CA, USA, 2005. [Google Scholar]
- National Environmental Justice Advisory Council. Ensuring Risk Reduction in Communities with Multiple Stressors: Environmental Justice and Cumulative Risks/Impacts; Cumulative Risks Impacts Work Group, National Environmental Justice Advisory Council: New Orleans, LA, USA, 2004. [Google Scholar]
- Clougherty, J.E.; Levy, J.I.; Kubzansky, L.D.; Ryan, P.B.; Suglia, S.F.; Canner, M.J.; Wright, R.J. Synergistic effects of traffic-related air pollution and exposure to violence on urban asthma etiology. Environ. Health Perspect. 2007, 115, 1140–1146. [Google Scholar] [CrossRef] [PubMed]
- Clougherty, J.E.; Kubzansky, L.D. A framework for examining social stress and susceptibility to air pollution in respiratory health. Environ Health Perspect. 2009, 117, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Brody, J.G.; Morello-Frosch, R.; Zota, A.; Brown, P.; Pérez, C.; Rudel, R.A. Linking exposure assessment science with policy objectives for environmental justice and breast cancer advocacy: The Northern California household exposure study. Am. J. Public Health 2009, 99, S600–S609. [Google Scholar] [CrossRef] [PubMed]
- Morello-Frosch, R.; Shenassa, E.D. The environmental “riskscape” and social inequality: Implications for explaining maternal and child health disparities. Environ. Health Perspect. 2006, 114, 1150–1153. [Google Scholar] [CrossRef]
- Su, J.G.; Morello-Frosch, R.; Jesdale, B.M.; Kyle, A.D.; Shamasunder, B.; Jerrett, M. An index for assessing demographic inequalities in cumulative environmental hazards with application to Los Angeles, California. Environ. Sci. Technol. 2009, 43, 7626–7634. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.A. Evaluating cumulative risk assessment for environmental justice: A community case study. Environ. Health Perspect. 2002, 110, 203. [Google Scholar] [CrossRef] [PubMed]
- Krieg, E.J.; Faber, D.R. Not so black and white: Environmental justice and cumulative impact assessments. Environ. Impact Assess. Rev. 2004, 24, 667–694. [Google Scholar] [CrossRef]
- Harris, R. Environmental Justice Considerations; The Office of Research, Development/Regional Cumulative Risk Assessment Workshop and Expo: Dallas, TX, USA, 2002. [Google Scholar]
- Lewis, A.S.; Sax, S.N.; Wason, S.C.; Campleman, S.L. Non-chemical stressors and cumulative risk assessment: An overview of current initiatives and potential air pollutant interactions. Int. J. Environ. Res. Public Health 2011, 8, 2020–2073. [Google Scholar] [CrossRef] [PubMed]
- Polkowski, R. Environmental Justice Case Study: Toxic Waste in Chester, Pennsylvania. Available online: http://www.umich.edu/~snre492/polk.html (accessed on 1 November 2011).
- U.S. Environmental Protection Agency, Office of Pollution Prevention and Toxics. Baltimore Community Environmental Partnership Air Committee Technical Report. Community Risk-Based Air Screening: A case study in Baltimore, Maryland. Available online: http://yosemite.epa.gov/oar/communityassessment.nsf/d2cea01886a35f4085256e1900591902/aa83857f10d2012a852576a5002c785f!OpenDocument (accessed on 22 April 2015).
- Recommendations of the CAL/EPA Advisory Committee on Environmental Justice to the CAL/EPA Interagency Working Group on Environmental Justice; Final Report, Canadian Energy Pipeline Association (CEPA); California Environmental Protection Agency: Sacremento, Cal., USA, 2003.
- Fleming, C. When environmental justice hits the local agenda: A profile of spartanburg and spartanburg county, South Carolina. Public Manag. Mag. 2004, 86, 1–10. [Google Scholar]
- Habisreutinger, P.; Gunderson, D.E. Real estate reuse opportunities within the regenesis project area: A case study. Int. J. Constr. Educ. Res. 2006, 2, 53–63. [Google Scholar] [CrossRef]
- ReGenesis. Regenesis Environmental Justice Demonstration Project: Community Revitalization through Partnerships. Available online: http://www.regenesisproject.org/ (accessed on 20 May 2011).
- U.S. Environmental Protection Agency. Towards an Environmental Justice Collaborative Model: Case Studies of Six Partnerships Used to Address Environmental Justice Issues in Communities. Available online: http://www.epa.gov/evaluate/pdf/ej/towards-ej-collaborative-model-case-studies-six-partnerships.pdf (accessed on 22 April 2015).
- U.S. Environmental Protection Agency. EPA’s Environmental Justice Collaborative Problem-Solving Model. Available online: http://www.epa.gov/compliance/ej/resources/publications/grants/cps-manual-12-27-06.pdf (accessed on 22 April 2015).
- Kloc, K. Zones of inequity: Cumulative air pollution and hot spots in the San Francisco bay area. 2009. [Google Scholar]
- U.S. Environmental Protection Agency, Office of Pesticide Programs. Peliminary Cumulative Risk Assessment of the Organophosphorus Pesticides. Available online: http://www.epa.gov/oppsrrd1/cumulative/pra_op_methods.htm (accessed on 22 April 2015).
- U.S. Environmental Protection Agency. Preliminary OP Cumulative Risk Assessment (part 1). Available online: http://www.epa.gov/oppsrrd1/cumulative/pra-op/ (accessed on 22 April 2015).
- U.S. Environmental Protection Agency. Summary of the Clean Water Act. Available online: http://www.epa.gov/regulations/laws/cwa.html (accessed on 22 April 2015).
- U.S. Environmental Protection Agency. Safe Drinking Water Act (SDWA). Available online: http://water.epa.gov/lawsregs/rulesregs/sdwa/index.cfm#sdwafs (accessed on 22 April 2015).
- U.S. Environmental Protection Agency. Guidelines for the Health Risk Assessment of Chemical Mixtures. Available online: http://cfpub.epa.gov/ncea/cfm/recordisplay.cfm?deid=22567 (accessed on 22 April 2015).
- U.S. Environmental Protection Agency. Supplemental Guidance for Conducting Health Risk Assessment of Chemical Mixtures. Available online: http://cfpub.epa.gov/ncea/cfm/recordisplay.cfm?deid=20533 (accessed on 22 April 2015).
- O’Neil, S.G. Superfund: Evaluating the impact of executive order 12898. Environ. Health Perspect. 2007, 115, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Sara Overview. Available online: http://www.epa.gov/superfund/policy/sara.htm (accessed on 22 April 2015).
- U.S. Environmental Protection Agency. Introduction to the Hazard Ranking System (HRS). Available online: http://www.epa.gov/superfund/programs/npl_hrs/hrsint.htm (accessed on 22 April 2015).
- Clean Air Act (CAA) of 1970. 42 U.S. Code 7401-7671. USA, 1970. Available online: https://www.law.cornell.edu/uscode/text/42/7401 (accessed on 23 April 2015).
- National Research Council (NRC). National Research Council. Committee on Health Impact Assessment. Improving Health in the United States: The Role of Health Impact Assessment; National Academies Press: Washington, D.C., USA, 2011. [Google Scholar]
- U.S. Environmental Protection Agency. National Environmental Policy Act. Available online: http://www.epa.gov/region1/nepa (accessed on 22 April 2015).
- National Environmental Policy Act (NEPA) of 1969. 42 U.S. Code 4321. USA, 1969. Available online: https://www.law.cornell.edu/uscode/text/42/4321 (accessed on 23 April 2015).
- National Research Council (NRC). National Research Council. Committee on Improving Risk Analysis Approaches Used by the us EPA. Science and Decisions: Advancing Risk Assessment; National Academies Press: Washington, D.C., USA, 2009. [Google Scholar]
- Gottlieb, L.M.; Fielding, J.E.; Braveman, P.A. Health impact assessment: Necessary but not sufficient for healthy public policy. Public Health Rep. 2012, 127, 156–162. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barzyk, T.M.; Wilson, S.; Wilson, A. Community, State, and Federal Approaches to Cumulative Risk Assessment: Challenges and Opportunities for Integration. Int. J. Environ. Res. Public Health 2015, 12, 4546-4571. https://doi.org/10.3390/ijerph120504546
Barzyk TM, Wilson S, Wilson A. Community, State, and Federal Approaches to Cumulative Risk Assessment: Challenges and Opportunities for Integration. International Journal of Environmental Research and Public Health. 2015; 12(5):4546-4571. https://doi.org/10.3390/ijerph120504546
Chicago/Turabian StyleBarzyk, Timothy M., Sacoby Wilson, and Anthony Wilson. 2015. "Community, State, and Federal Approaches to Cumulative Risk Assessment: Challenges and Opportunities for Integration" International Journal of Environmental Research and Public Health 12, no. 5: 4546-4571. https://doi.org/10.3390/ijerph120504546
APA StyleBarzyk, T. M., Wilson, S., & Wilson, A. (2015). Community, State, and Federal Approaches to Cumulative Risk Assessment: Challenges and Opportunities for Integration. International Journal of Environmental Research and Public Health, 12(5), 4546-4571. https://doi.org/10.3390/ijerph120504546