1. Introduction
The increasing prevalence of allergic diseases, particularly asthma, in Korea is associated with a higher number of people living in apartment buildings and a higher number of cars since the mid-1980s [
1]. A recent study demonstrated that the prevalence of atopic dermatitis (AD) symptoms in children aged six to seven years in Korea was 5.7% and 11.2% in 2000 and 2010, respectively [
2]. There is a considerable body of evidence showing the relationship between outdoor air pollutants and allergic diseases. However, the indoor environment is of particular interest with regard to its role in the development and aggravation of allergic diseases because young children spend most of their time indoors [
3,
4]. Many studies have reported the relationship between indoor air pollutants and asthma [
5,
6], but fewer have reported the effects of indoor air pollutants on AD, a common and troublesome condition among young children [
7,
8,
9].
Formaldehyde, volatile organic compounds (VOCs), and aromatic compounds are major indoor environmental pollutants. They are emitted by new furniture and finishing materials such as wallpaper, plywood, and polyvinyl chloride (PVC) flooring [
4]. A previous study found that the main source of indoor VOCs and formaldehyde in Korean houses was wallpaper, rather than new furniture or flooring, because wallpaper covers the inner walls and ceilings of houses and has a surface area that is three to four times greater than that of the floor [
10]. According to published literature, indoor air pollutants may play a key role in the development and aggravation of allergic diseases [
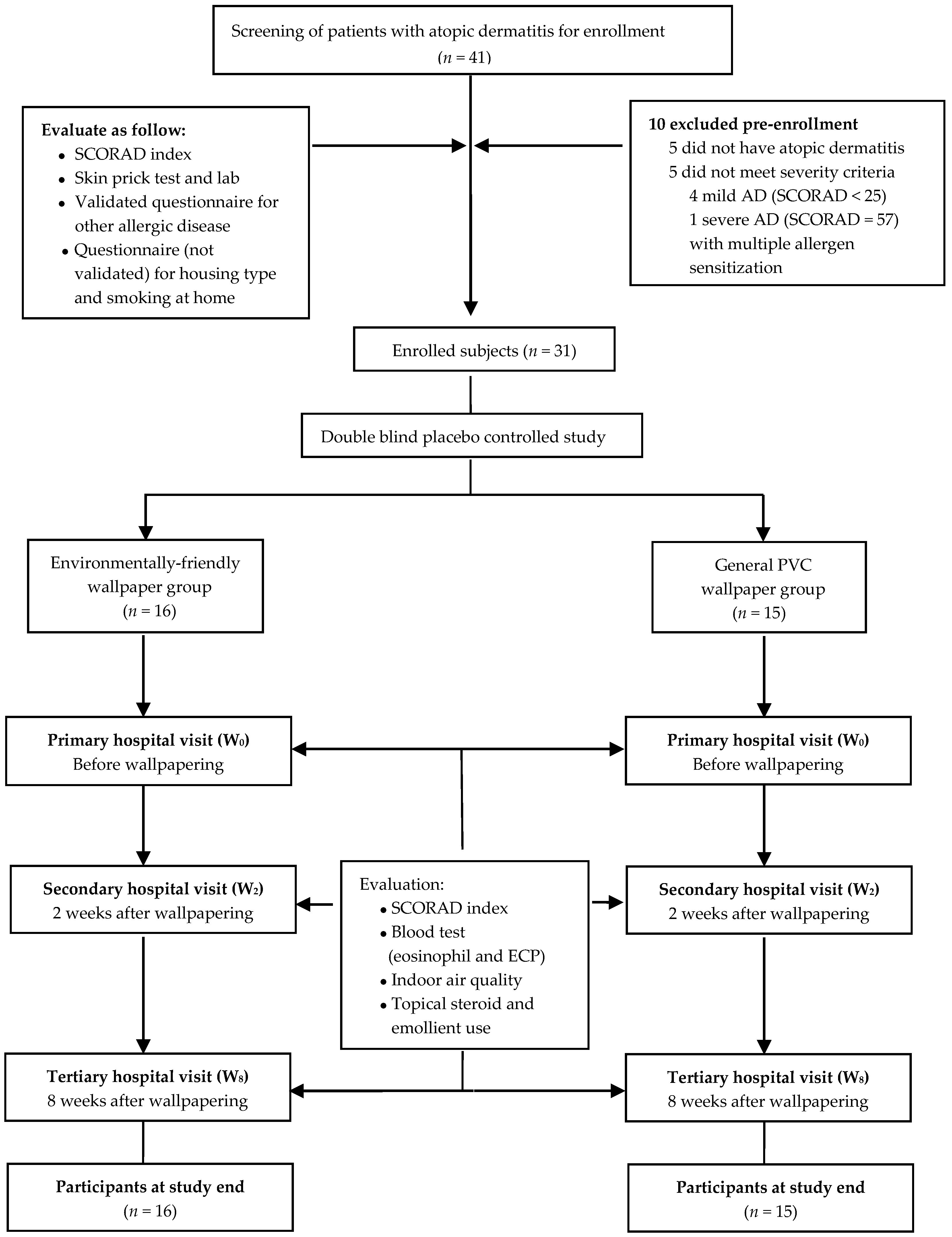
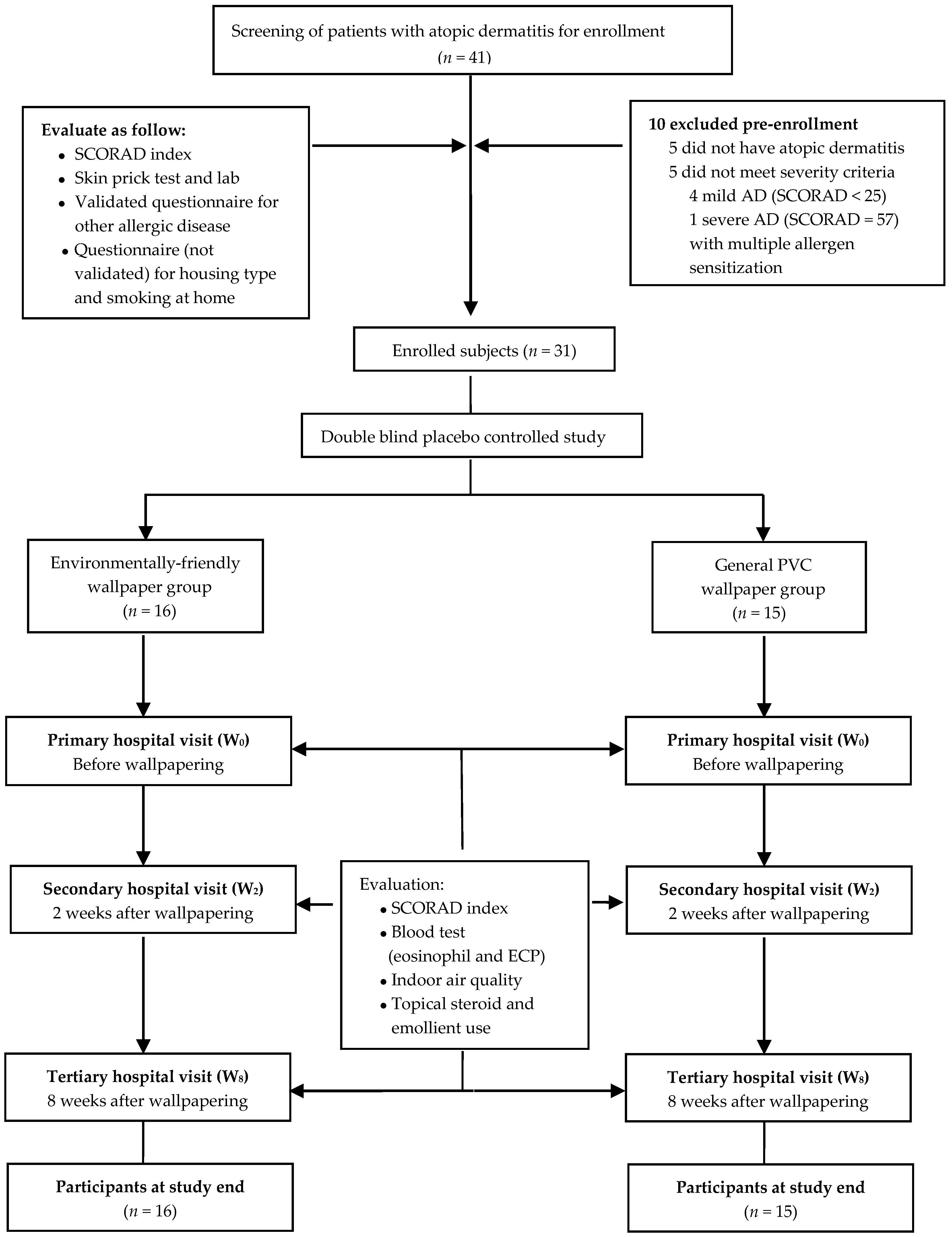
4]. To improve indoor air quality, many products have been made less toxic; as an example, environmentally friendly (EF) wallpaper, without PVCs, is now available. The purpose of this study was to evaluate the effects of wallpapering on indoor air quality and symptoms of AD in children. To the best of our knowledge, this is the first study to measure indoor air pollutant concentrations after EF wallpapering compared to PVC wallpapering. In addition, the Scoring Atopic dermatitis (SCORAD) index in children was calculated before and after wallpapering. The correlation between the concentrations of pollutants and symptoms of AD was evaluated.
4. Discussion
The purpose of our study was to determine the effect of EF wallpaper on indoor air quality and to investigate the association between indoor air quality and symptoms of AD in children.
The mean concentration of TVOCs from the subjects’ house at W
0 (1095 ± 883.7, 1099.1 ± 1636.6 in the EF and PVC-wallpaper groups, respectively) exceeded the current Korean threshold for childcare centers (400 μg/m
3) [
15], and the mean concentration of formaldehyde at W
0 in the EF-wallpaper group was also higher than the recommended threshold (106.3 ± 32.8 and 79.1 ± 22.9 in the EF and PVC-wallpaper groups, respectively). The Korean threshold for formaldehyde in indoor air as specified for an 8 h value is 100 μg/m
3, which is higher than the recommended threshold of other countries [
18]. A previous study reported that the concentration of VOCs in the indoor air of houses of patients with AD and allergic asthma was approximately 1.4–2.0 fold higher than in the houses of the same age group without atopy [
7]. In our study, the concentrations of TVOCs were found to be higher than values in previous studies on eco-friendly materials or in the houses of patients with AD [
19,
20,
21]. These high concentrations were similar to the results shown in a previous study that measured the indoor air quality in an unoccupied newly built building [
22]. The reason that high levels of TVOCs were measured in our study is due to the use of artificial air fresheners or air cleansing, air ventilation, location, and floor level of the apartment, and the surrounding region/area [
21,
22]. High concentrations of VOCs or formaldehyde are associated with the onset of Sick Building Syndrome (SBS) or the aggravation of allergic diseases in newly built buildings [
4,
23,
24]. Some studies have reported that exposure to VOCs can damage the epidermal barrier and exacerbate the adverse effects of house dust mites in patients with AD [
25,
26]. We excluded patients who were sensitized to food or multiple allergens to minimize confounding variables, and AD severity in this study was moderate, not mild. Although we could not evaluate the relationship between AD severity and the concentration of TVOCs, the results suggested that a high concentration of TVOCs had adverse effects on children with AD. We planned wallpapering to improve indoor air quality in terms of indoor air pollutant concentration, and intended to observe changes in indoor air qualities. We expected to see better effects of eco-friendly materials on indoor air quality than the existing materials, such as PVC wallpaper. To sum up, after wallpapering, there was a change in indoor air quality and the concentration of TVOCs continuously decreased by W
2 and W
8 in both groups. The concentration of 5VOCs by W
2 and W
8 was also reduced when compared to W
0 in both groups. However, formaldehyde increased by W
2 and then reduced by W
8. As with the present study, several previous studies estimated indoor quality after remodeling with EF material [
19,
20,
22]. One study reported that the concentration of TVOCs decreased two weeks after wallpapering, but increased at six and 10 weeks after wallpapering. Furthermore, formaldehyde concentrations decreased at two weeks and kept decreasing until 10 weeks [
20]. The change in VOCs and formaldehyde observed were different from the results of our study.
In contrast, the results of the study by Yoo et al. are identical to the changes in the concentrations of indoor air pollutants observed in our study [
22]. Yoo et al. wallpapered with PVC materials and eco-friendly materials in an unoccupied, newly built apartment and measured the concentrations of VOCs and formaldehyde emissions for three months. The results showed that the concentration of TVOCs was higher in the initial phase, followed by a gradual decline as time progressed. For the house built with the PVC materials, compared to those with the eco-friendly material (14 days after eco-friendly wallpapering), it took 50 days more for TVOCs concentration to fall below 1000 μg/m
3. The changes in formaldehyde concentration were alike in both groups: the concentration reached its peak after seven days and remained below 60 μg/m
3 as time progressed. However, according to our findings, it is difficult to say that the natural material-coated wallpaper used is more effective than the PVC wallpapers in terms of indoor air quality. In the second week after wallpapering, the rise of the formaldehyde concentration was higher in the EF-wallpaper group than in the PVC-wallpaper group. In the same week, the concentration of TVOCs decreased in the PVC-wallpaper group more than in the EF-wallpaper group. The concentration of VOCs decreased less with the eco-friendly wallpaper, probably because of NVOC abundance. In general, eco-friendly wallpaper contains less PVC and includes materials that are paper-backed or simply coated with natural material. One study reported that TVOCs and formaldehyde were less likely to be emitted from the paper-backed materials than materials coated with natural substances [
14]. This difference between our finding and Yoo’s findings is probably because we used kenaf as the eco-friendly material, whereas Yoo et al. used PP (polypropylene) resin.
Finally, we studied the positive effects of indoor environment improvements on AD symptoms. AD is a chronically relapsing skin disease characterized by dermal inflammatory infiltrate containing eosinophils. To objectively evaluate AD symptom improvement, we used ECP levels and the SCORAD index to examine the effects of improved indoor air quality [
26,
27]. In our study, the eosinophil count or ECP showed no statistical significance. Interestingly, an improvement in the SCORAD index was observed during the study period. The decrease in the SCORAD index from W
0 to W
8 was significantly greater in the EF-wallpaper group than in the PVC-wallpaper group (
Table 6). These findings were consistent with those reported in previous studies [
19,
20]. In both groups, statistically significant improvements in the patients’ symptoms were observed when the TVOCs and formaldehyde contents decreased by the eighth week after wallpapering, but not in the second week. In our air quality evaluation in the second week after wallpapering, the result of the EF-wallpaper group was not significantly different from that of the PVC-wallpaper group, but the EF-wallpaper group showed an improved SCORAD index result. We assumed that the natural-coated wallpaper emits NVOC that positively affects AD symptoms. Therefore, a generalized linear model procedure was used to determine the pollutants associated with the SCORAD index. The SCORAD index showed a positive correlation with TVOCs and 5VOCs, except styrene, and showed a negative correlation with NVOC % (
Table 7). This indicated that the symptoms associated with AD were worse when the concentrations of VOCs and formaldehyde were higher. Additionally, the eco-friendly wallpaper, which had a small reduction in the ratio of VOCs concentration after two weeks, showed better improvements in terms of clinical signs than the PVC wallpapers, probably because of the NVOCs that have risen in the same weeks. Most VOCs are generated artificially, but some are derived from natural sources and named NVOCs [
16]. NVOCs that are emitted by forests are believed to be beneficial for health in comparison with other VOCs. Phytoncides are the representative material of NVOCs. Chemical and pharmacological studies on phytoncides have reported that they have anti-inflammatory and anti-oxidant activities [
28,
29]. Furthermore, they are reportedly associated with an amelioration in conditions such as allergies, multiple sclerosis, and Parkinson’s disease [
30]. Interestingly, the concentration of NVOCs at two and eight weeks was statistically higher in the EF-wallpaper group than in the PVC-wallpaper group (
Table 5). In addition, the results of our study showed that the SCORAD index was negatively correlated with NVOC/VOCs (NVOC %). This is the first study to show that the higher NVOC % values from natural sources may improve AD symptoms.
This study had several limitations. We could not evaluate the persistent effects of wallpapering. However, considering that Yoo et al. [
22] reported that the concentrations of VOCs were maintained consistently after 60 days (eight to nine weeks), we assume that the short-term evaluation at eight weeks more accurately reflected the effect of wallpapering. In contrast, long-term observations may be influenced by various factors missed in our study design. Other limitations included the small number of participants. The statistical power of our minimal sample size was 80% with a significance level of 5%. Another limitation is the short-term sampling. Because human activities and environmental conditions before and during sampling have an effect on the concentration of VOCs, short-term sampling can be inappropriate for assessing the average air pollutant concentrations over long periods. However, some effort was put into ensuring consistency in the measurements by following a set pattern of ventilation prior to sampling. In addition, these results do not solely indicate causality with respect to AD symptom improvement and changing wallpaper. Regular visits to the doctor also may have played a role in improving AD symptoms. Thus, adequately applying emollients or topical steroid during the study period may have also elicited improvement in AD symptoms, and thus, these factors cannot be ignored against the setting of EF-wallpaper use.
Despite these limitations, this is the first pediatric study comparing indoor air pollutant concentrations between EF wallpapering and PVC wallpapering, using the SCORAD index. We also analyzed the effects of air pollutants on AD, particularly the correlation between the concentrations of the pollutants and the symptoms of AD. The results showed the beneficial effects of EF wallpapering on indoor air quality. Furthermore, indoor air quality has an important role in symptom management for children with AD. Further studies are needed to evaluate the long-term effects of EF wallpaper on indoor air quality improvement, with a focus on the effects of NVOCs which are considered to improve AD symptoms.




{kind=link}