
Evaluation of Indoor Air Quality Screening Strategies: A Step-Wise Approach for IAQ Screening




Abstract
:1. Introduction
2. Materials and Methods
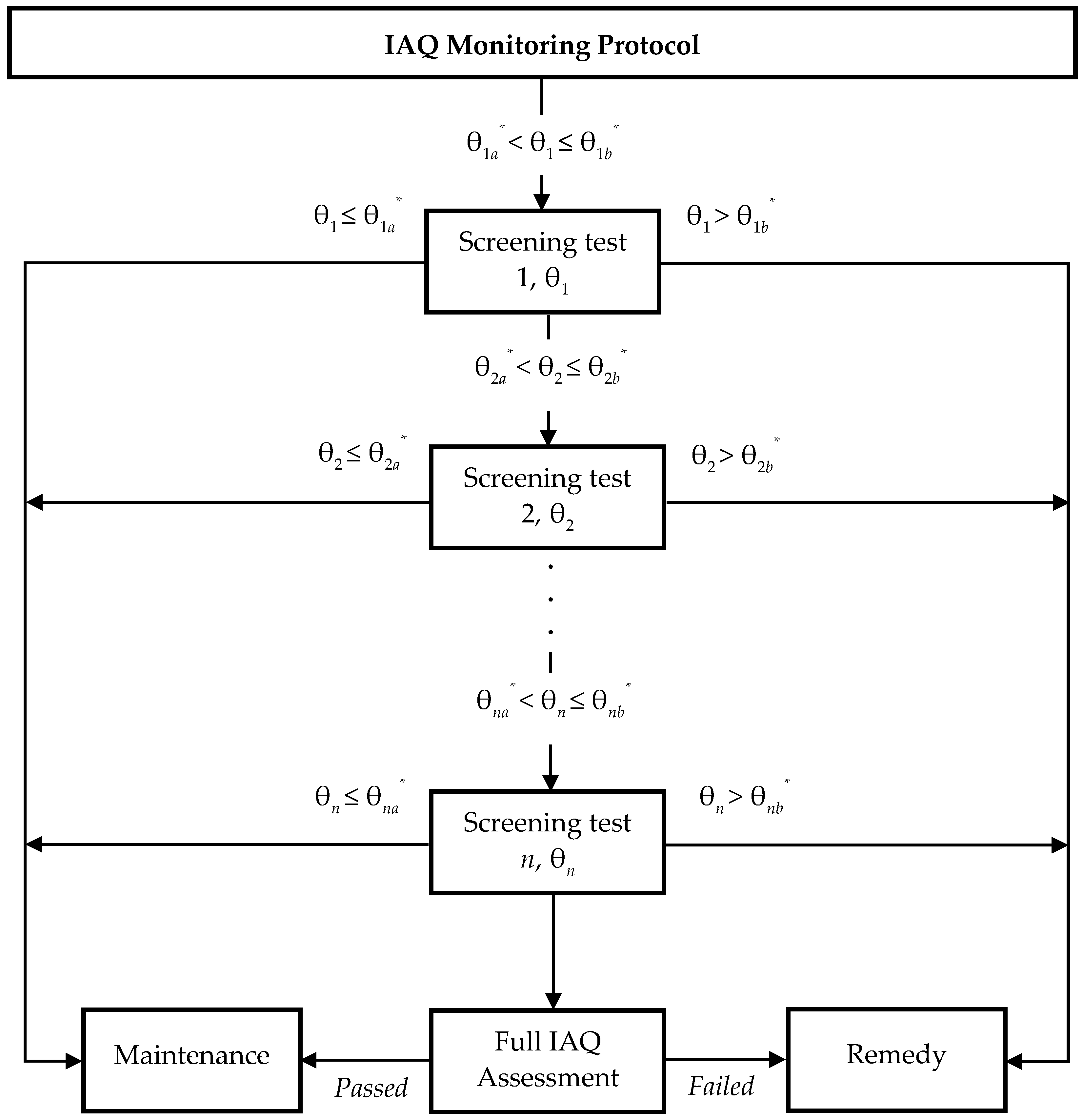
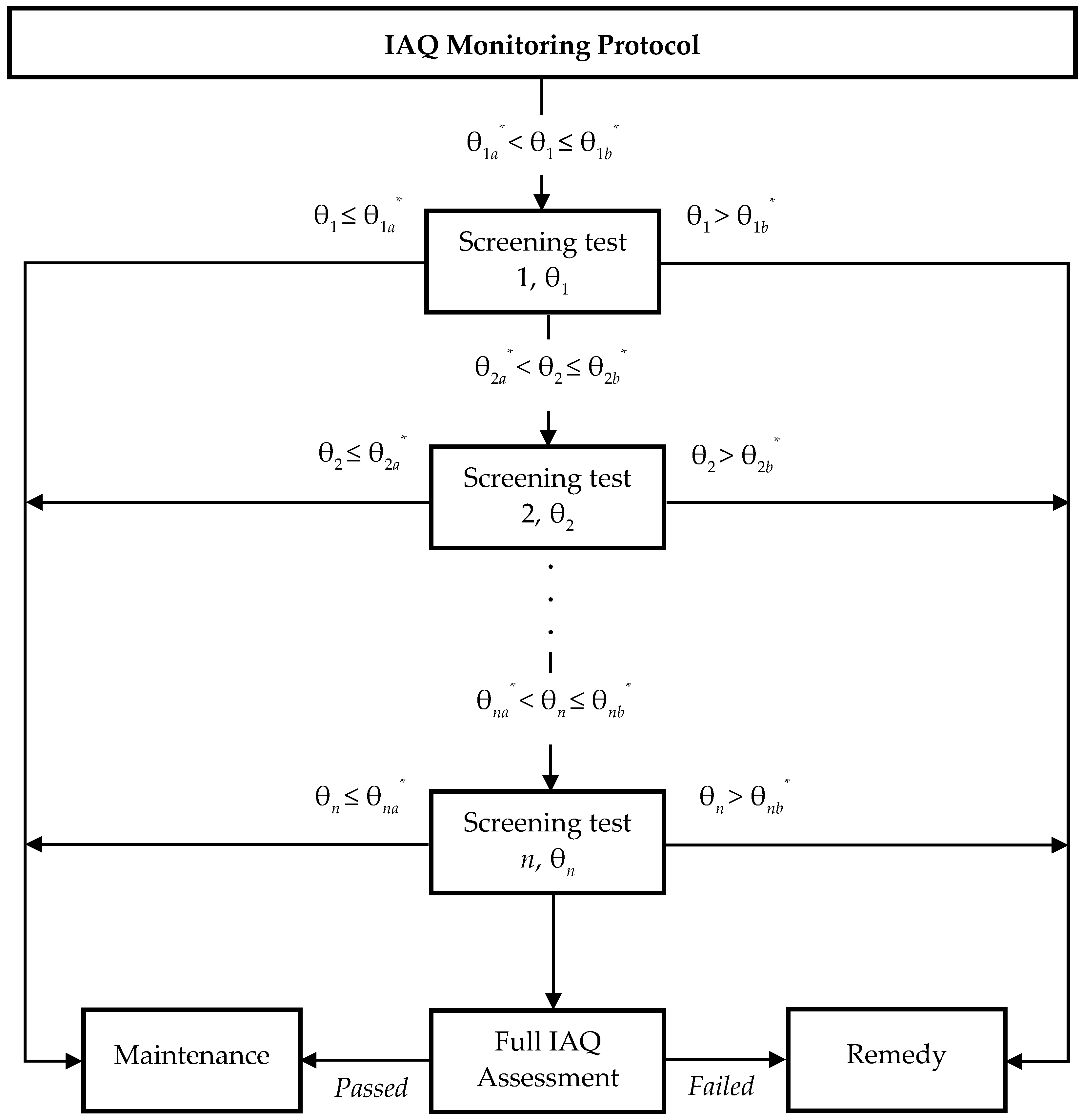
2.1. Concept of Screening Strategy
2.2. IAQ Assessment Database
2.3. IAQ Assessment Database
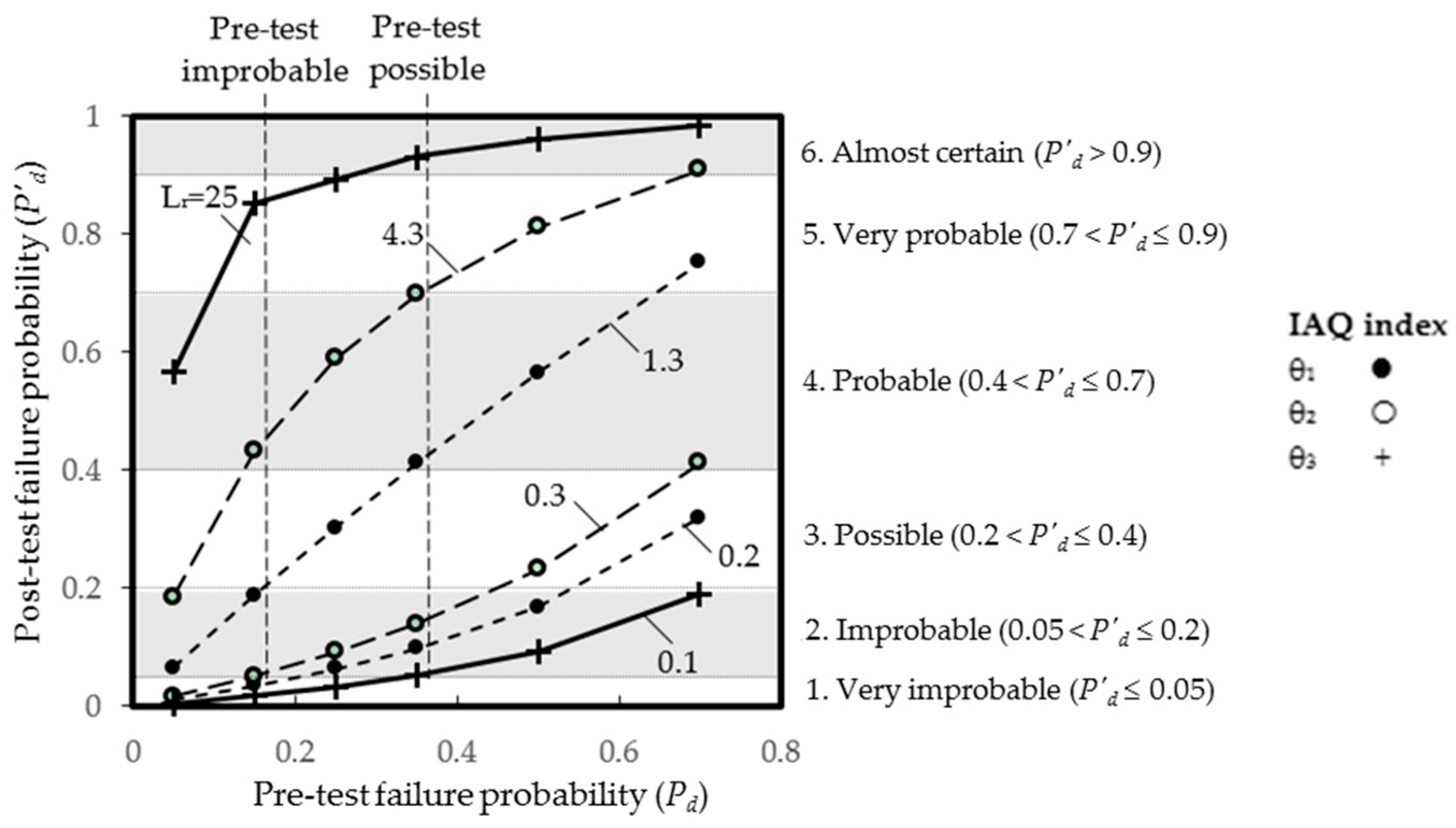
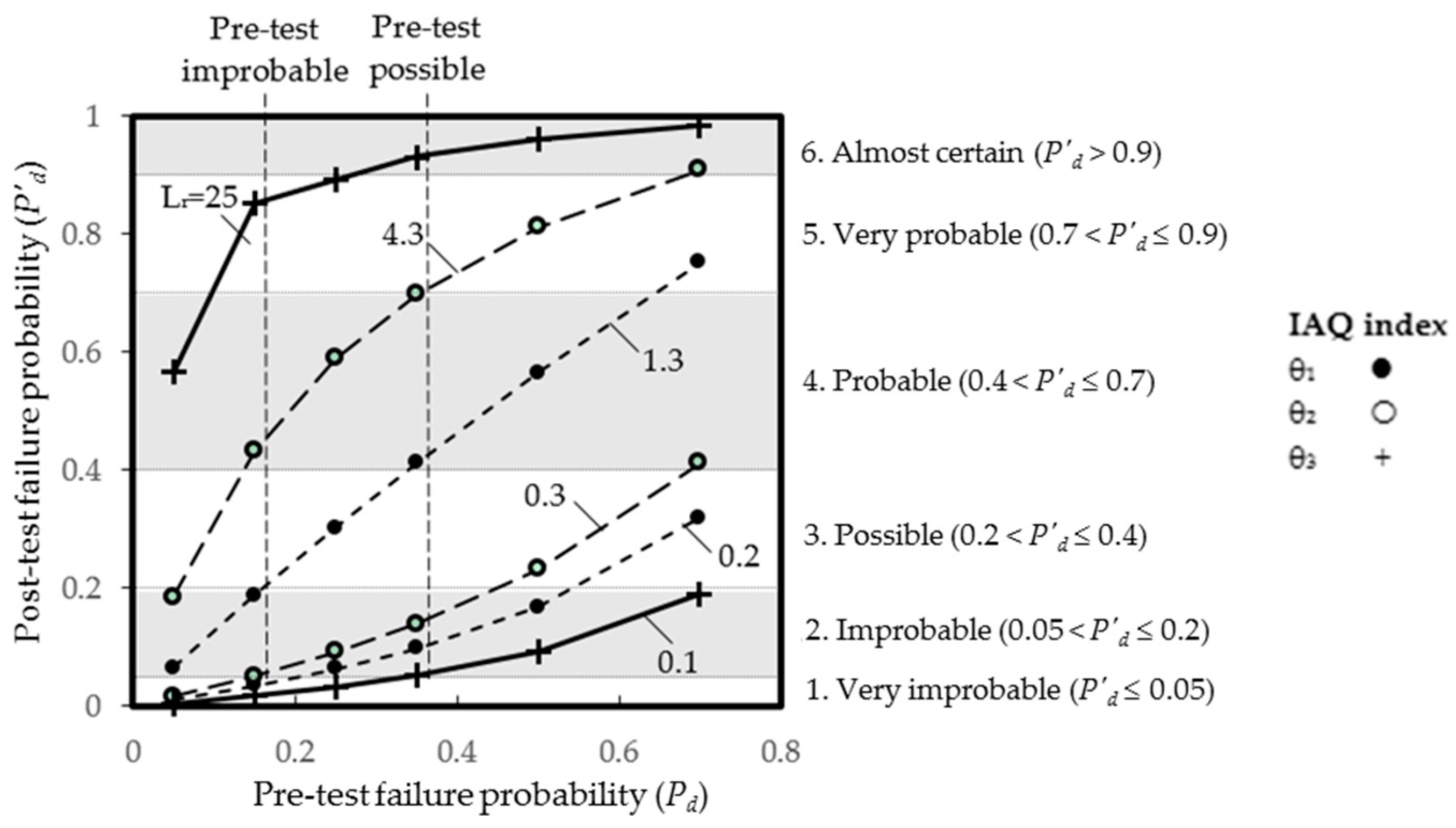
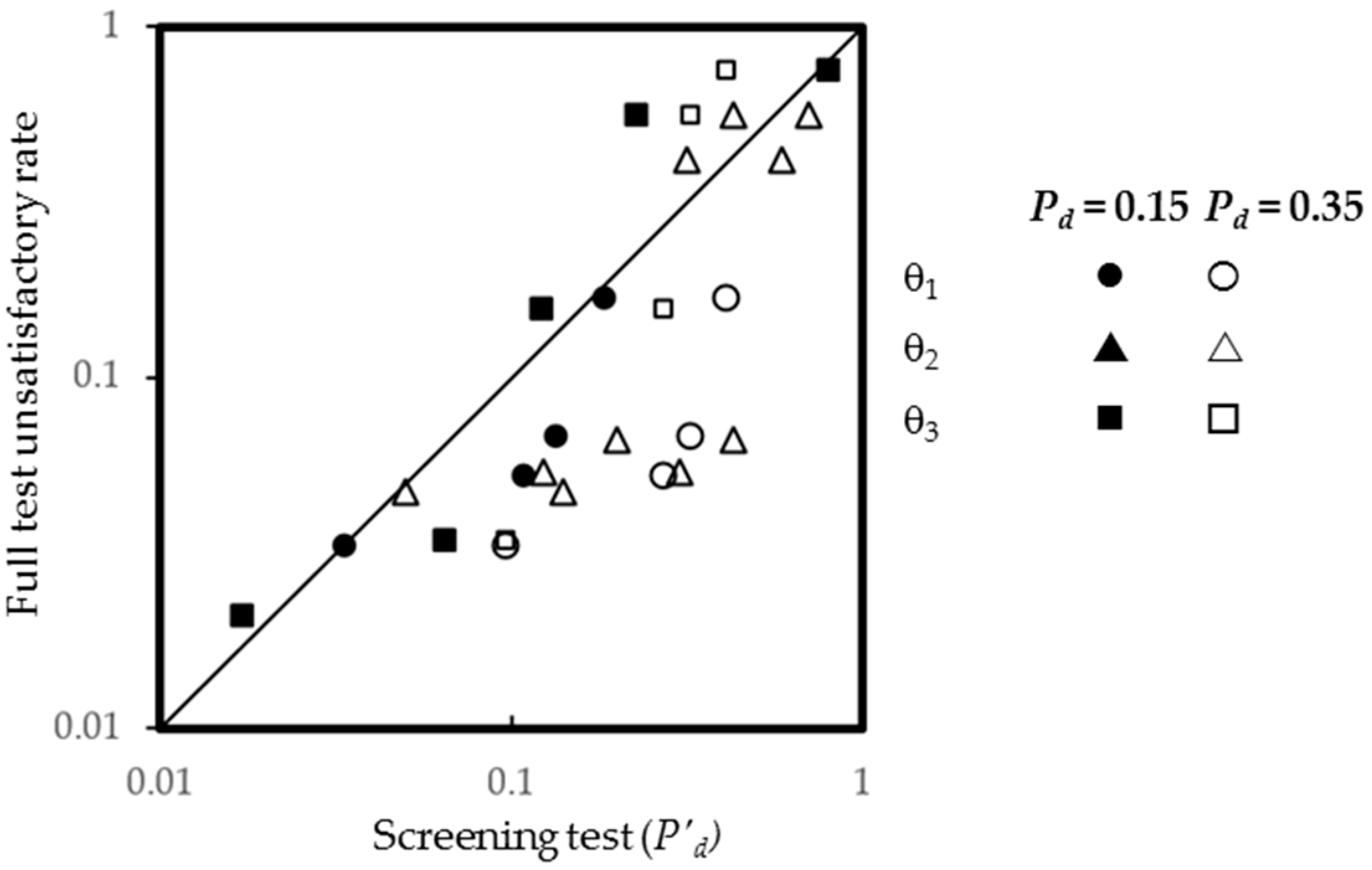
3. Results and Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Burroughs, H.E.; Hansen, S.J. Indoor Air Quality: An Overview—Where Are We? In Managing Indoor Air Quality, 5th ed.; The Farimont Press Inc.: Lilburn, GA, USA, 2011; pp. 1–14. [Google Scholar]
- World Health Organization. Burden of Disease from Household Air Pollution for 2012; Public Health, Social and Environmental Determinants of Health Department, World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Bholah, R.; Fagoonee, I.; Subratty, A. Sick Building Syndrome in Mauritius: Are Symptoms Associated with the Office Environment? Indoor Built Environ. 2000, 9, 44–51. [Google Scholar] [CrossRef]
- Butala, V.; Muhic, S. Perception of Air Quality and the Thermal Environment in Offices. Indoor Built Environ. 2007, 16, 302–310. [Google Scholar] [CrossRef]
- HKEPD Indoor Air Quality Information Centre. Indoor Air Quality (IAQ) Complaint Received by the Government; Hong Kong Environmental Protection Department, Government of the Hong Kong Special Administrative Region: Hong Kong, China, 2012.
- HKEPD Indoor Air Quality Information Centre. Indoor Air Quality (IAQ) Complaint Received by the Government; Hong Kong Environmental Protection Department, Government of the Hong Kong Special Administrative Region: Hong Kong, China, 2014.
- Daniels, M.J.; Dominici, F.; Samet, J.M.; Zeger, S.L. Estimating Particulate Matter-Mortality Dose-Response Curves and Threshold Levels: An Analysis of Daily Time-Series for the 20 Largest US Cities. Am. J. Epidemiol. 2000, 152, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Seppänen, O.A.; Fisk, W.J.; Mendell, M.J. Association of Ventilation Rates and CO2 Concentrations with Health and Other Responses in Commercial and Institutional Buildings. Indoor Air 1999, 9, 226–252. [Google Scholar] [CrossRef] [PubMed]
- Hui, P.S.; Wong, L.T.; Mui, K.W. Feasibility Study of an Express Assessment Protocol for the Indoor Air Quality of Air-conditioned Offices. Indoor Built Environ. 2006, 15, 373–378. [Google Scholar] [CrossRef]
- HKEPD Indoor Air Quality Information Centre. Indoor Air Quality Certification Schemes for Offices and Public Places; Hong Kong Environmental Protection Department, Government of the Hong Kong Special Administrative Region: Hong Kong, China, 2003.
- Wong, L.T.; Mui, K.W.; Hui, P.S. A statistical model for characterizing common air pollutants in air-conditioned offices. Atmos. Environ. 2006, 40, 4246–4257. [Google Scholar] [CrossRef]
- Pauker, S.G.; Kassirer, J.P. The Threshold Approach to Clinical Decision Making. N. Engl. J. Med. 1980, 302, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.T.; Mui, K.W.; Hui, P.S. Screening for Indoor air Quality of Air-Conditioned Offices. Indoor Built Environ. 2007, 16, 438–443. [Google Scholar] [CrossRef]
- Mui, K.W.; Wong, L.W.; Hui, P.S.; Law, K. Epistemic evaluation of policy influence on workplace indoor air quality of Hong Kong in 1996–2005. Build. Serv. Eng. Res. Technol. 2008, 29, 157–164. [Google Scholar] [CrossRef]
- Mui, K.W.; Hui, P.S.; Wong, L.T. Diagnostics of Unsatisfactory Indoor Air Quality in Air-Conditioned Workplaces. Indoor Built Environ. 2011, 20, 313–320. [Google Scholar] [CrossRef]
- Sackett, D.L.; Straus, S.E.; Richardson, W.S.; Rosenberg, W.; Haynes, R.B. Evidence-Based Medicine: How to Practice and Teach EBM, 2nd ed.; Churchill Livingstone: Edinburgh, UK, 2000. [Google Scholar]
- Gilbert, R.; Logan, S. Assessing Diagnostic and Screening Tests. In Evidence-based Pediatrics and Child Health, 2nd ed.; Moyer, V.A., Ed.; BMJ Books: London, UK, 2004; pp. 31–43. [Google Scholar]
- Reagan, R.T.; Mosteller, F.; Youtz, C. Quantitative meanings of verbal probability expressions. J. Appl. Psychol. 1989, 74, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Vick, S.G. Degrees of Belief: Subjective Probability and Engineering Judgment, 2nd ed.; ASCE Press: Reston, VA, USA, 2002. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Parameter | 8-h Exposure Limit | Database A AM (SD) [EFR%] | Database B AM (SD) [EFR%] | p-Value |
|---|---|---|---|---|
| CO2 (ppm) | 1000 | 658 (151) [7%] | 665 (203) [50%] | 0.17 |
| CO (µg∙m−3) | 10,000 | 1105 (4594) [1%] | 1372 (825) [1%] | 0.09 |
| RSP (µg∙m−3) | 180 | 30 (20) [0%] | 27 (30) [3%] | ≤0.05 |
| NO2 (µg∙m−3) | 150 | 27 (17) [0%] | 33 (14) [0.4%] | ≤0.05 |
| O3 (µg∙m−3) | 120 | 40 (38) [13%] | 40 (19) [3%] | 0.39 |
| HCHO (µg∙m−3) | 100 | 48 (103) [15%] | 29 (22) [13%] | ≤0.05 |
| TVOC (µg∙m−3) | 600 | 358 (328) [42%] | 176 (176) [24%] | ≤0.05 |
| Rn (Bq∙m−3) | 200 | 46 (39) [0.6%] | 68 (41) [6%] | ≤0.05 |
| ABC (CFU∙m−3) | 1000 | 505 (385) [38.4%] | 238 (175) [6%] | ≤0.05 |
| k | Screening Level for θ1, θ2, θ3 | Unsatisfactory IAQ | Satisfactory IAQ | Likelihood Ratio, Lr | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Counts (%) | Counts (%) | |||||||||
| θ1 | θ2 | θ3 | θ1 | θ2 | θ3 | θ1 | θ2 | θ3 | ||
| 1 | <0.32 | 0 (0%) | 11 (6.6%) | 5 (3%) | 0 (0%) | 74 (21%) | 93 (26%) | / | 0.3 | 0.1 |
| 2 | 0.32–0.42 | 1 (0.6%) | 64 (38%) | 24 (14%) | 10 (2.8%) | 165 (46%) | 131 (37%) | 0.2 | 0.8 | 0.4 |
| 3 | 0.43–0.53 | 19 (11%) | 61 (37%) | 33 (20%) | 62 (17%) | 96 (27%) | 85 (24%) | 0.7 | 1.4 | 0.8 |
| 4 | 0.54–0.64 | 47 (28%) | 23 (14%) | 33 (20%) | 116 (32%) | 19 (5%) | 43 (12%) | 0.9 | 2.6 | 1.7 |
| 5 | ≥0.65 | 99 (59%) | 8 (4.8%) | 72 (43%) | 161 (45%) | 4 (1%) | 6 (1.7%) | 1.3 | 4.3 | 25 |
| Total count | 167 (100%) | 358 (100%) | ||||||||
| Screening Level | Lr | Nj | (i) Screening Test (Pd = 0.35) | (ii) Screening Test (Pd = 0.15) | Full Test | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| O′d | P′d | Assessment Result | O′d | P′d | Assessment Result | Pj | Assessment Result | |||
| (a) θ1 | ||||||||||
| 0.32–0.42 | 0.2 | 183 | 0.11 | 0.10 | 2. Improbable | 0.04 | 0.03 | 1.Very improbable | 0.03 | 1. Very improbable |
| 0.43–0.53 | 0.7 | 444 | 0.38 | 0.27 | 3. Possible | 0.12 | 0.11 | 2. Improbable | 0.05 | 1. Very improbable |
| 0.54–0.64 | 0.9 | 521 | 0.49 | 0.33 | 3. Possible | 0.16 | 0.14 | 2. Improbable | 0.07 | 2. Improbable |
| ≥0.65 | 1.3 | 1100 | 0.70 | 0.41 | 4. Probable | 0.23 | 0.19 | 2. Improbable | 0.17 | 2. Improbable |
| (b) θ2 | ||||||||||
| <0.32 | 0.3 | 510 | 0.16 | 0.14 | 2. Improbable | 0.05 | 0.05 | 2. Improbable | 0.05 | 1. Very improbable |
| 0.32–0.42 | 0.8 | 870 | 0.43 | 0.30 | 3. Possible | 0.14 | 0.12 | 2. Improbable | 0.05 | 1. Very improbable |
| 0.43–0.53 | 1.4 | 570 | 0.76 | 0.43 | 4. Probable | 0.25 | 0.20 | 3. Possible | 0.07 | 2. Improbable |
| 0.54–0.64 | 2.6 | 211 | 1.40 | 0.58 | 4. Probable | 0.47 | 0.32 | 3. Possible | 0.42 | 4. Probable |
| ≥0.65 | 4.3 | 87 | 2.32 | 0.70 | 4. Probable | 0.76 | 0.43 | 4. Probable | 0.56 | 4. Probable |
| (c) θ3 | ||||||||||
| <0.32 | 0.1 | 865 | 0.05 | 0.05 | 1. Very improbable | 0.02 | 0.02 | 1. Very improbable | 0.02 | 1. Very improbable |
| 0.32–0.42 | 0.4 | 819 | 0.22 | 0.18 | 2. Improbable | 0.07 | 0.07 | 2. Improbable | 0.03 | 1. Very improbable |
| 0.43–0.53 | 0.8 | 327 | 0.43 | 0.30 | 3. Possible | 0.14 | 0.12 | 2. Improbable | 0.16 | 2. Improbable |
| 0.54–0.64 | 1.7 | 144 | 0.92 | 0.48 | 4. Probable | 0.30 | 0.23 | 3. Possible | 0.56 | 4. Probable |
| ≥0.65 | 25 | 93 | 13.5 | 0.93 | 6. Almost certain | 4.41 | 0.82 | 5. Very probable | 0.74 | 5. Very probable |
| Screening Tests | No. of Offices with Predicted Unsatisfactory IAQ (Unsatisfactory Rate) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Very Improbable (P′d ≤ 0.05) | 2. Improbable (0.05 < P′d ≤ 0.2) | 3. Possible (0.2 < P′d ≤ 0.4) | 4. Probable (0.4 < P′d ≤ 0.7) | 5. Very Probable (0.7 < P′d ≤ 0.9) | 6. Almost Certain (P′d > 0.9) | Thresholds T1 0.05 < P′d ≤ 0.9 | Thresholds T2 0.2 < P′d ≤ 0.9 | |||||||
| Nj | Pj | Nj | Pj | Nj | Pj | Nj | Pj | Nj | Pj | Nj | Pj | Nj | Nj | |
| Pd = 0.35 | ||||||||||||||
| θ1 | 183 | 0.03 | 965 | 0.06 | 1100 | 0.17 | 2248 | 2065 | ||||||
| θ2 | 510 | 0.05 | 870 | 0.05 | 868 | 0.20 | 2248 | 1738 | ||||||
| θ3 | 865 | 0.02 | 819 | 0.03 | 327 | 0.16 | 144 | 0.56 | 93 | 0.74 | 1290 | 471 | ||
| (a) θ1, θ2 | 126 | 0.05 | 435 | 0.04 | 872 | 0.06 | 741 | 0.18 | 74 | 0.59 | 2122 | 1687 | ||
| (b) θ1, θ3 | 737 | 0.02 | 448 | 0.06 | 837 | 0.09 | 133 | 0.58 | 3 | 1 | 90 | 0.73 | 1421 | 973 |
| (c) θ2, θ3 | 852 | 0.02 | 407 | 0.04 | 630 | 0.04 | 190 | 0.31 | 80 | 0.76 | 89 | 0.73 | 1307 | 900 |
| (d) θ1, θ2, θ3 | 760 | 0.03 | 544 | 0.03 | 475 | 0.04 | 291 | 0.21 | 92 | 0.73 | 86 | 0.72 | 1402 | 858 |
| Pd = 0.15 | ||||||||||||||
| θ1 | 183 | 0.03 | 2065 | 0.12 | 2065 | 0 | ||||||||
| θ2 | 1380 | 0.05 | 781 | 0.16 | 87 | 0.56 | 2248 | 870 | ||||||
| θ3 | 865 | 0.02 | 1146 | 0.07 | 144 | 0.56 | 93 | 0.74 | 1383 | 237 | ||||
| (a) θ1, θ2 | 546 | 0.04 | 937 | 0.05 | 682 | 0.18 | 83 | 0.58 | 1702 | 765 | ||||
| (b) θ1, θ3 | 903 | 0.02 | 1119 | 0.06 | 133 | 0.58 | 3 | 1 | 90 | 0.73 | 1345 | 226 | ||
| (c) θ2, θ3 | 945 | 0.02 | 968 | 0.05 | 166 | 0.27 | 80 | 0.76 | 35 | 0.89 | 54 | 0.63 | 1249 | 281 |
| (d) θ1, θ2, θ3 | 1007 | 0.02 | 806 | 0.05 | 255 | 0.20 | 91 | 0.70 | 35 | 0.89 | 54 | 0.63 | 1187 | 381 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, L.-t.; Mui, K.-w.; Tsang, T.-w. Evaluation of Indoor Air Quality Screening Strategies: A Step-Wise Approach for IAQ Screening. Int. J. Environ. Res. Public Health 2016, 13, 1240. https://doi.org/10.3390/ijerph13121240
Wong L-t, Mui K-w, Tsang T-w. Evaluation of Indoor Air Quality Screening Strategies: A Step-Wise Approach for IAQ Screening. International Journal of Environmental Research and Public Health. 2016; 13(12):1240. https://doi.org/10.3390/ijerph13121240
Chicago/Turabian StyleWong, Ling-tim, Kwok-wai Mui, and Tsz-wun Tsang. 2016. "Evaluation of Indoor Air Quality Screening Strategies: A Step-Wise Approach for IAQ Screening" International Journal of Environmental Research and Public Health 13, no. 12: 1240. https://doi.org/10.3390/ijerph13121240
APA StyleWong, L.-t., Mui, K.-w., & Tsang, T.-w. (2016). Evaluation of Indoor Air Quality Screening Strategies: A Step-Wise Approach for IAQ Screening. International Journal of Environmental Research and Public Health, 13(12), 1240. https://doi.org/10.3390/ijerph13121240