Epidural Analgesia and Neonatal Morbidity: A Retrospective Cohort Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
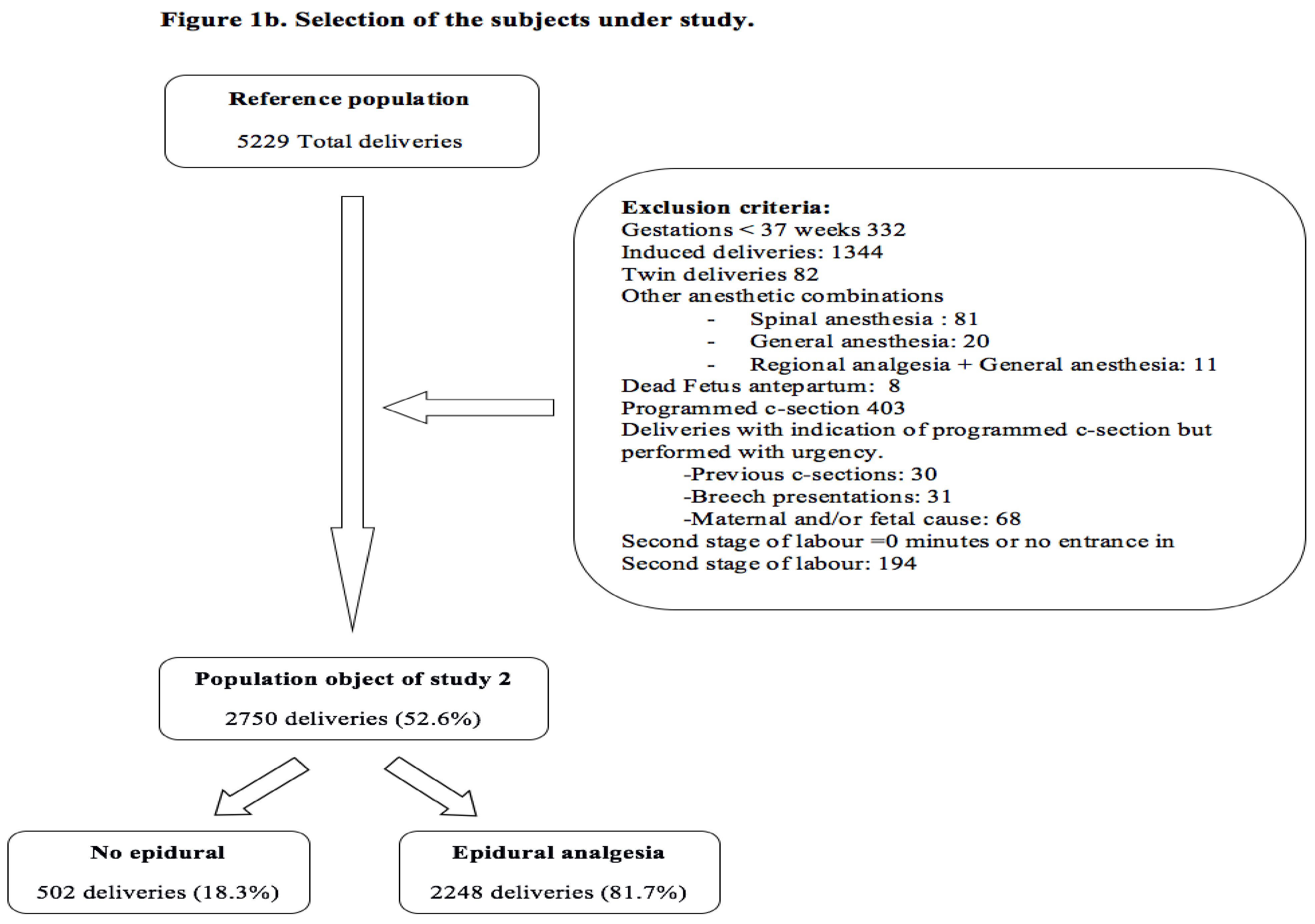
2.1. Design and Participants
2.2. Sources of Information
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jones, L.; Othman, M.; Dowswell, T.; Alfirevic, Z.; Gates, S.; Newburn, M.; Jordan, S.; Lavender, T.; Neilson, J. Pain management for women in labour: An overview of systematic reviews. Cochrane Database Syst. Rev. 2012, CD009234. [Google Scholar] [CrossRef]
- Cheng, Y.W.; Shaffer, B.L.; Nicholson, J.M.; Caughey, A.B. Second stage of labour and epidural use: A larger effect than previously suggested. Obstet. Gynecol. 2017, 123, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Gómez, A.; García-Martínez, O.; Ramos-Torrecillas, J.; De Luna-Bertos, E.; Ruiz, C.; Ocaña-Peinado, F.M. Retrospective study of the association between epidural analgesia during labour and complications for the newborn. Midwifery 2015, 31, 613–636. [Google Scholar] [CrossRef] [PubMed]
- Hung, T.-H.; Hsieh, T.-T.; Liu, H.-P. Differential effects of epidural analgesia on modes of delivery and perinatal outcomes between nulliparous and multiparous women: A retrospective cohort study. PLoS ONE 2015, 10, E0120907. [Google Scholar] [CrossRef] [PubMed]
- Törnell, S.; Ekéus, C.; Hultin, M.; Håkansson, S.; Thunberg, J.; Högberg, U. Low Apgar score, neonatal encephalopathy and epidural analgesia during labour: A Swedish registry-based study. Acta Anaesthesiol. Scand. 2015, 59, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Anim-Somuah, M.; Smyth, R.M.; Jones, L. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst. Rev. 2011, CD000331. [Google Scholar] [CrossRef]
- Gizzo, S.; Di Gangi, S.; Saccardi, C.; Patrelli, T.S.; Paccagnella, G.; Sansone, L.; Barbara, F.; D’Antona, D.; Nardelli, G.B. Epidural Analgesia During Labour: Impact on Delivery Outcome, Neonatal Well-Being, and Early Breastfeeding. Breastfeed. Med. 2012, 7, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Greenwell, E.A.; Wyshak, G.; Ringer, S.A.; Johnson, L.C.; Rivkin, M.J.; Lieberman, E. Intrapartum Temperature Elevation, Epidural Use, and Adverse Outcome in Term Infants. Pediatrics 2012, 129, E447–E454. [Google Scholar] [CrossRef] [PubMed]
- Halpern, S.H.; Leighton, B.L.; Ohlsson, A.; Barrett, J.F.; Rice, A. Effect of epidural vs parenteral opioid analgesia on the progress of labour: A meta-analysis. JAMA 1998, 280, 2105–2110. [Google Scholar] [CrossRef] [PubMed]
- Leighton, B.L.; Halpern, S.H. The effects of epidural analgesia on labour, maternal, and neonatal outcomes: A systematic review. Am. J. Obstet. Gynecol. 2002, 186 (Suppl. 5), S69–S77. [Google Scholar] [PubMed]
- Schuit, E.; Kwee, A.; Westerhuis, M.; Van Dessel, H.; Graziosi, G.; Van Lith, J.; Nijhuis, J.G.; Oei, S.G.; Oosterbaan, H.P.; Schuitemaker, N.W.; et al. A clinical prediction model to assess the risk of operative delivery. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 915–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiklund, I.; Norman, M.; Uvnäs-Moberg, K.; Ransjö-Arvidson, A.-B.; Andolf, E. Epidural analgesia: Breast-feeding success and related factors. Midwifery 2009, 25, e31–e38. [Google Scholar] [CrossRef] [PubMed]
- Leighton, B.L.; Halpern, S.H. Epidural analgesia: Effects on labour progress and maternal and neonatal outcome. Semin. Perinatol. 2002, 26, 122–135. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, F. The effects of maternal labour analgesia on the foetus. Best Pract. Res. Clin. Obstet. Gynaecol. 2010, 24, 289–302. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Cao, L.; Deng, Q.; Sun, L.-Q.; Gu, T.-Y.; Song, J.; Qi, D.Y. The effects of epidural/spinal opioids in labour analgesia on neonatal outcomes: A meta-analysis of randomized controlled trials. Can. J. Anaesth. 2014, 61, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Altman, M.; Sandström, A.; Petersson, G.; Frisell, T.; Cnattingius, S.; Stephansson, O. Prolonged second stage of labour is associated with low Apgar score. Eur. J. Epidemiol. 2015, 30, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Laughon, S.K.; Berghella, V.; Reddy, U.M.; Sundaram, R.; Lu, Z.; Hoffman, M.K. Neonatal and maternal outcomes with prolonged second stage of labour. Obstet. Gynecol. 2014, 124, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Thorngren-Jerneck, K.; Herbst, A. Low 5-minute Apgar score: A population-based register study of 1 million term births. Obstet. Gynecol. 2001, 98, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, J.; Farina, A.; Turchi, G.; Hasegawa, Y.; Zanello, M.; Baroncini, S. Effects of epidural analgesia on labour length, instrumental delivery, and neonatal short-term outcome. J. Anesth. 2013, 27, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, D.; Makhija, B.; Arora, M.; Haritwal, A.; Gurha, P. The effect of epidural analgesia on labour, mode of delivery and neonatal outcome in Nullipara of India, 2011–2014. J. Clin. Diagn. Res. 2014, 8, OC03–OC06. [Google Scholar] [PubMed]
- Georgieva, A.; Moulden, M.; Redman, C.W.G. Umbilical cord gases in relation to the neonatal condition: The EveREst plot. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 168, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Malin, G.L.; Morris, R.K.; Khan, K.S. Strength of association between umbilical cord pH and perinatal and long term outcomes: Systematic review and meta-analysis. BMJ 2010, 340, c1471. [Google Scholar] [CrossRef] [PubMed]
- Yeh, P.; Emary, K.; Impey, L. The relationship between umbilical cord arterial pH and serious adverse neonatal outcome: Analysis of 51,519 consecutive validated samples. BJOG 2012, 119, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Spain, J.E.; Frey, H.A.; Tuuli, M.G.; Colvin, R.; Macones, G.A.; Cahill, A.G. Neonatal morbidity associated with shoulder dystocia maneuvers. Am. J. Obstet. Gynecol. 2015, 212, 353.e1–353.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández-Martínez, A.; Pascual-Pedreño, A.I.; Baño-Garnés, A.B.; del Rocío Melero-Jiménez, M.; Molina-Alarcón, M. Relation between induced labour indications and neonatal morbidity. Arch Gynecol. Obstet. 2014, 290, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, L.M.; Nohr, E.A.; Kjaergaard, H. Mode of delivery after epidural analgesia in a cohort of low-risk nulliparas. Birth 2011, 38, 317–326. [Google Scholar] [CrossRef] [PubMed]
- García-de-Diego, J.M.; Serrano-del-Rosal, R. Universalización, paridad y evolución de la demanda de anestesia epidural durante el parto en Andalucía. Gac. Sanit. 2017. [Google Scholar] [CrossRef] [PubMed]
- Bodner-Adler, B.; Bodner, K.; Kimberger, O.; Wagenbichler, P.; Kaider, A.; Husslein, P.; Mayerhofer, K. The effect of epidural analgesia on obstetric lacerations and neonatal outcome during spontaneous vaginal delivery. Arch Gynecol. Obstet. 2003, 267, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Caliskan, E.; Ozdamar, D.; Doger, E.; Cakiroglu, Y.; Kus, A.; Corakci, A. Prospective case control comparison of foetal intrapartum oxygen saturations during epidural analgesia. Int. J. Obstet. Anesth. 2010, 19, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Ekéus, C.; Hjern, A.; Hjelmstedt, A. The need for epidural analgesia is related to birthweight—A population-based register study. Acta Obstet. Gynecol. Scand. 2009, 88, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Armani, M.; Gaggiano, C.; Dallaglio, S.; Romanini, E.; Sospiri, C.; Magnani, C. Are there any strategies to improve neonatal outcomes associated with epidural analgesia in labour? Acta Biomed. 2013, 84, 117–123. [Google Scholar] [PubMed]
- Decca, L.; Daldoss, C.; Fratelli, N.; Lojacono, A.; Slompo, M.C.; Stegher, C.; Valcamonico, A.; Frusca, T. Labour course and delivery in epidural analgesia: A case-control study. J. Matern. Neonatal. Med. 2004, 16, 115–118. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Epidural Analgesia | p-Value | |
|---|---|---|---|
| No (n = 503) | Yes (n = 2441) | ||
| Maternal Age | 0.665 | ||
| Mean (SD) | 30.8 (5.67) | 30.7 (5.20) | |
| Gestational Age | <0.001 | ||
| Mean (SD) | 39.5 (1.07) | 39.8 (1.06) | |
| Parity | <0.001 | ||
| Nulliparous | 112 (22.3) | 1348 (55.2) | |
| Multiparous | 391 (77.7) | 1093 (44.8) | |
| Previous CS | 0.137 | ||
| No | 478 (95.0) | 2276 (93.2) | |
| Yes | 25 (5.0) | 165 (6.8) | |
| BMI | |||
| Mean (SD) | 24.7 (4.60) | 24.4 (4.54) | 0.579 |
| Newborn weight (grams) | 0.051 | ||
| Mean (SD) | 3271.8 (444.82) | 3313.8 (412.01) | |
| First stage of labor duration (minutes) | <0.001 | ||
| Mean (SD) | 94.4 (97.19) | 270.5 (161.56) | |
| Second stage of labor duration (minutes) | <0.001 | ||
| Mean (SD) | 19.3 (23.12) | 78.4 (63.37) | |
| Type of delivery | <0.001 | ||
| Normal Vaginal | 503 (100.0) | 2006 (82.2) | |
| Instrumental | 0 (0.0) | 194 (7.9) | |
| Emergency CS | 0 (0.0) | 241 (9.9) | |
| Variables | Epidural Analgesia | p- Value Aj * | |||
|---|---|---|---|---|---|
| No (n = 503) n (%) | Yes (n = 2441) n (%) | OR Crude | OR Adjusted * | ||
| Umbilical artery pH | 0.831 | ||||
| ≥7.10 (Ref) | 425 (98.6) | 2164 (98.2) | 1.00 | 1.00 | |
| <7.10 | 6 (1.4) | 39 (1.8) | 1.27 [0.54, 2.99] | 0.78 [0.31, 1.96] | |
| Missing | 72 | 238 | |||
| Apgar at 5 min | 0.993 | ||||
| ≥7 (Ref) | 503 (100.0) | 2430 (99.6) | 1.00 | 1.00 | |
| <7 | 0 (0.0) | 10 (0.4) | NC | NC | |
| Missing | 0 | 0 | |||
| Degree of neonatal resuscitation | 0.992 | ||||
| Basic (Ref) | 503 (100.0) | 2330 (97.1) | 1.00 | 1.00 | |
| Advanced | 0 (0.0) | 71 (2.9) | NC | NC | |
| Missing | 0 | 0 | |||
| Composite morbidity | 0.132 | ||||
| No (Ref) | 497 (98.8) | 2338 (95.8) | 1.00 | 1.00 | |
| Yes | 6 (1.2) | 103 (4.2) | 3.65 [1.59, 8.36] | 1.97 [0.82, 4.74] | |
| Missing | 0 | 0 | |||
| Variables | Second Stage of Labor Duration | p-Value | |||
|---|---|---|---|---|---|
| <1 h (n = 1577) n (%) | 1–2 h (n = 547) n (%) | 2–3 h (n = 357) n (%) | ≥3 h (269)n (%) | ||
| No EA | NC * | ||||
| Normal Vaginal | 476 (94.8) | 18 (3.6) | 6 (1.2) | 2 (0.4) | |
| Instrumental | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| C-section | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Use of EA | <0.001 | ||||
| Normal Vaginal | 1049 (52.4) | 495 (24.7) | 281 (14.0) | 177 (8.8) | |
| Instrumental | 46 (23.7) | 27 (13.9) | 54 (27.8) | 67 (34.5) | |
| CS | 6 (11.5) | 7 (13.5) | 16 (30.8) | 23 (44.2) | |
| Umbilical Artery pH < 7.10 | Aj. OR * | CI 95% | p-Value |
|---|---|---|---|
| Use of EA | 0.89 | 0.33, 2.37 | 0.813 |
| Type of delivery (Ref. Normal Vaginal) | |||
| Instrumental delivery | 2.68 | 1.15, 6.27 | 0.023 |
| C-section | 2.32 | 0.50, 10.73 | 0.282 |
| Second stage of labor duration (Ref. < 1 h) | |||
| 1–2 h | 0.74 | 0.31, 1.78 | 0.497 |
| 2–3 h | 0.83 | 0.32, 2.16 | 0.702 |
| >3 h | 0.81 | 0.48, 2.34 | 0.699 |
| Apgar at 5 min < 7 | Aj. OR * | CI 95% | p-Value |
| Use of EA | NC | NC | 0.933 |
| Type of delivery (Ref. Normal Vaginal) | |||
| Instrumental delivery | 4.11 | 0.59, 28.70 | 0.154 |
| C-section | 8.23 | 0.68, 100.45 | 0.999 |
| Second stage of labor duration (Ref. < 1 h) | |||
| 1–2 h | NC | NC | 0.992 |
| 2–3 h | 0.61 | 0.09, 4.09 | 0.607 |
| >3 h | 0.28 | 0.02, 3.28 | 0.311 |
| Advanced neonatal resuscitation | Aj. OR * | CI 95% | p-Value |
| Use of EA | NC | NC | 0.993 |
| Type of delivery (Ref. Normal Vaginal) | |||
| Instrumental delivery | 2.44 | 1.17, 5.08 | 0.017 |
| C-section | 2.56 | 0.71, 9.24 | 0.151 |
| Second stage of labor duration (Ref. < 1 h) | |||
| 1–2 h | 0.90 | 0.46, 1.78 | 0.766 |
| 2–3 h | 0.66 | 0.29, 1.50 | 0.321 |
| >3 h | 0.38 | 0.13-1.10 | 0.075 |
| Composite morbidity | Aj. OR * | CI 95% | p-Value |
| Use of EA | 1.80 | 0.75, 4.37 | 0.191 |
| Type of delivery (Ref. Normal Vaginal) | |||
| Instrumental delivery | 2.86 | 1.59, 5.12 | <0.001 |
| C-section | 2.20 | 0.73, 6.65 | 0.161 |
| Second stage of labor duration (Ref. < 1 h) | |||
| 1–2 h | 0.85 | 0.49, 1.50 | 0.580 |
| 2–3 h | 0.73 | 0.38, 1.40 | 0.340 |
| >3 h | 0.52 | 0.24, 1.14 | 0.112 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez, A.H.; Almagro, J.J.R.; García-Suelto, M.M.-C.; Barrajon, M.U.; Alarcón, M.M.; Gómez-Salgado, J. Epidural Analgesia and Neonatal Morbidity: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 2092. https://doi.org/10.3390/ijerph15102092
Martínez AH, Almagro JJR, García-Suelto MM-C, Barrajon MU, Alarcón MM, Gómez-Salgado J. Epidural Analgesia and Neonatal Morbidity: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2018; 15(10):2092. https://doi.org/10.3390/ijerph15102092
Chicago/Turabian StyleMartínez, Antonio Hernández, Julián Javier Rodríguez Almagro, María Moreno-Cid García-Suelto, María Ureña Barrajon, Milagros Molina Alarcón, and Juan Gómez-Salgado. 2018. "Epidural Analgesia and Neonatal Morbidity: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 15, no. 10: 2092. https://doi.org/10.3390/ijerph15102092
APA StyleMartínez, A. H., Almagro, J. J. R., García-Suelto, M. M.-C., Barrajon, M. U., Alarcón, M. M., & Gómez-Salgado, J. (2018). Epidural Analgesia and Neonatal Morbidity: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 15(10), 2092. https://doi.org/10.3390/ijerph15102092