Developing an Extended Model of the Relation between Work Motivation and Health as Affected by the Work Ability as Part of a Corporate Age Management Approach


Abstract
:1. Introduction
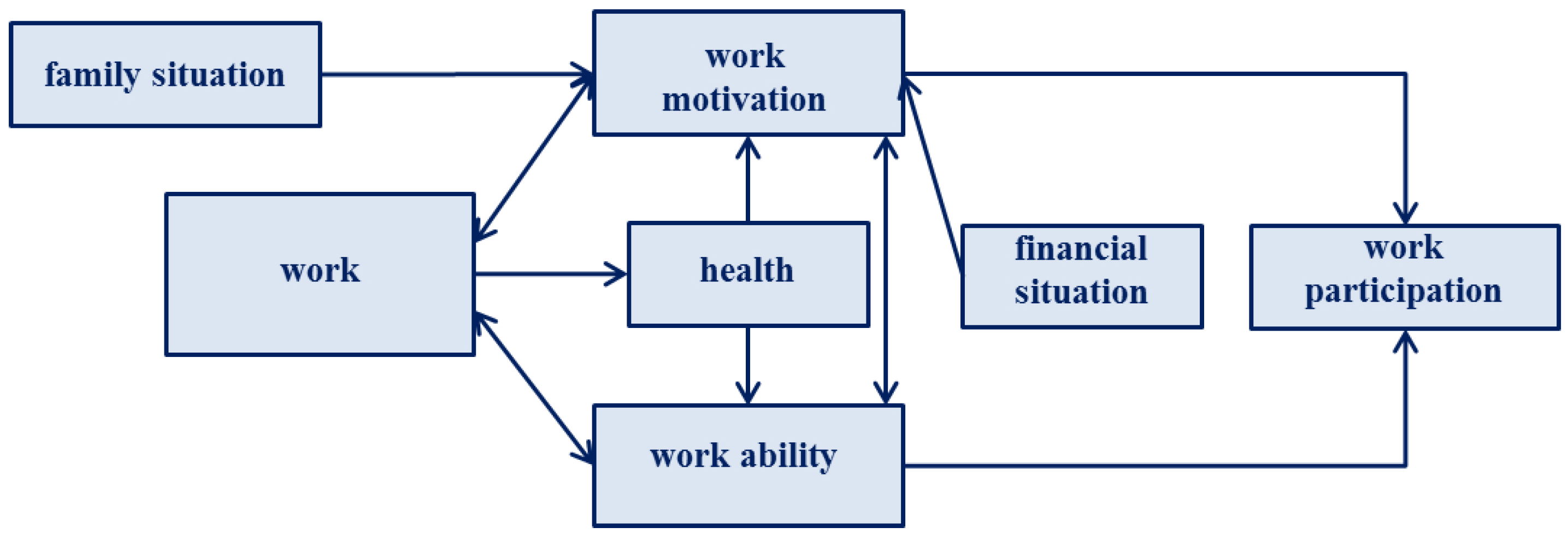
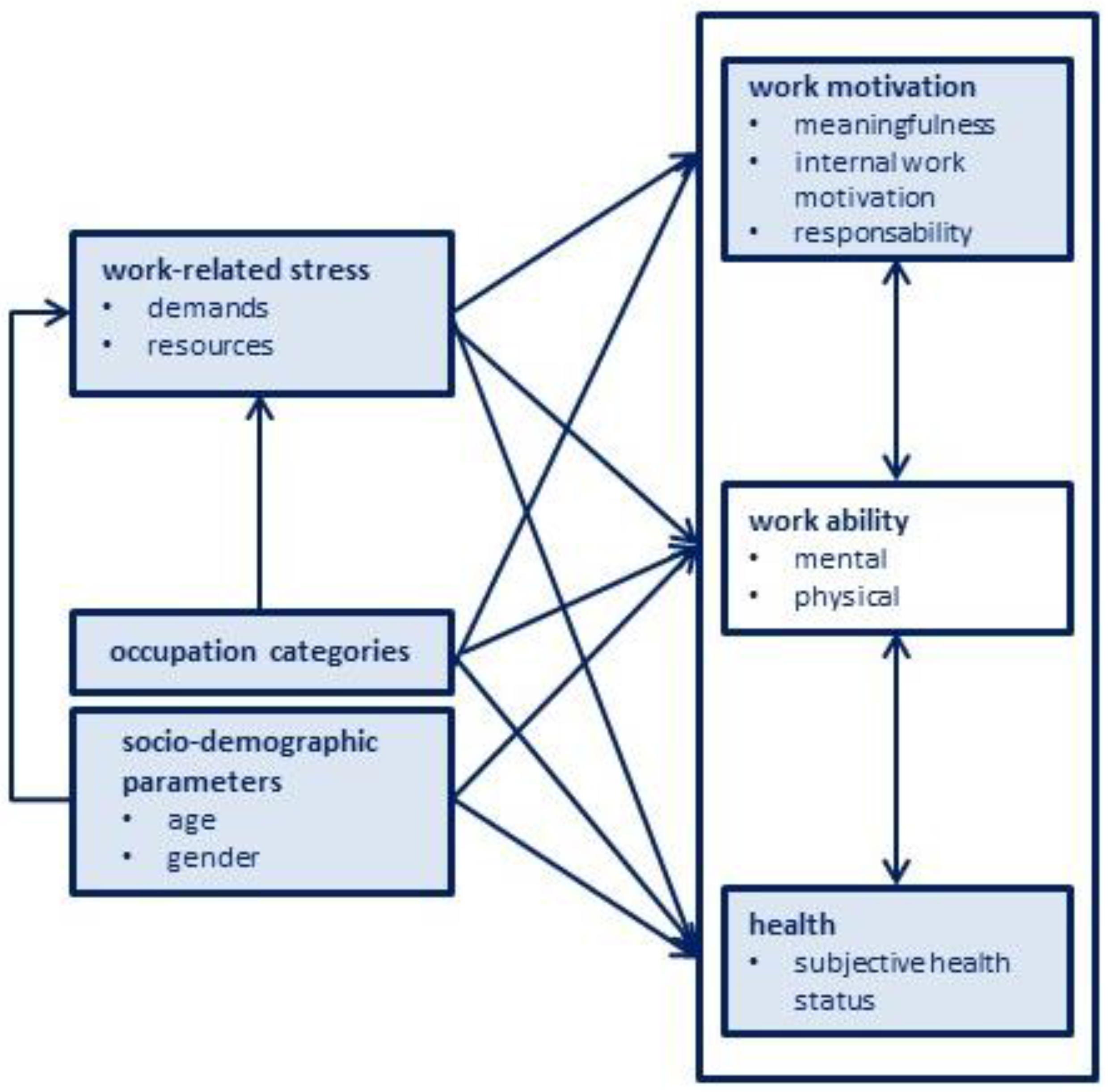
2. Selected Theoretical Models Illustrating the Relation between Work Motivation and Health
3. Current State of Research
4. Factors Influencing Work Motivation and Health
4.1. Socio-Demographic Parameters
4.2. Occupation Categories
4.3. Work-Related Stress
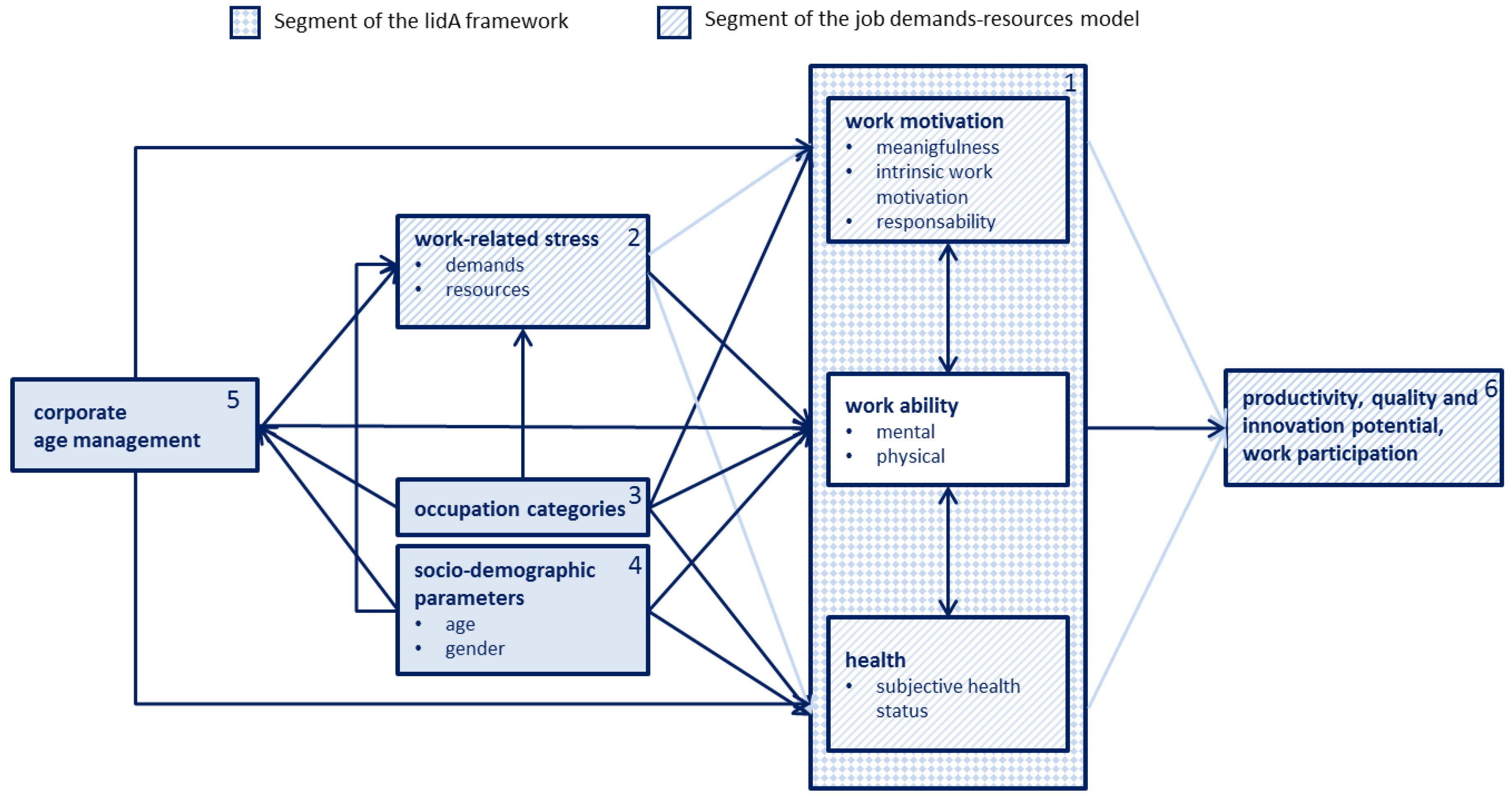
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Colby, S.L.; Ortman, J.M. Projections of the Size and Composition of the U.S. Population: 2014 to 2060; Current Population Reports: Washington, DC, USA, 2015; pp. 25–1143. Available online: https://census.gov/content/dam/Census/library/publications/2015/demo/p25-1143.pdf (accessed on 14 February 2018).
- Hayutin, A.; Beals, M.; Borges, E. The Aging US Workforce: A Chartbook of Demographic Shift; Stanford Center on Longevity: Stanford, CA, USA, 2013; p. 48. Available online: http://longevity3.stanford.edu/wp-content/uploads/2014/01/The_Aging_U.S.-Workforce.pdf (accessed on 14 February 2018).
- Galarneau, D. Portrait of Canada's labour Force: National Household Survey, 2011; Statistics Canada—Catalogue no. 99-012-X2011002; Statistics Canada: Ottawa, ON, Canada, 2013; ISBN 978-1-100-22408-4.
- Eurostat. Population Structure and Ageing. 2015. Available online: http://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing&oldid=253703 (accessed on 14 February 2018).
- OECD (Organisation for Economic Co-operation and Development). Demographic Change in the Netherlands: Strategies for Labour Markets in Transition; OECD: Paris, France, 2013; p. 213. Available online: http://www.oecd.org/cfe/leed/demo_change_netherlands.pdf (accessed on 14 February 2018).
- Hasselhorn, H.M.; Apt, W. Understanding Employment Participation of Older Workers Creating a Knowledge Base for Future Labour Market Challenges; Federal Ministry of Labour and Social Affairs: Berlin, Germany, 2015. Available online: https://www.baua.de/EN/Service/Publications/Cooperation/Gd81.pdf;jsessionid=57250B2D772E29AE493510946D31E353.s2t2?__blob=publicationFile&v=6 (accessed on 28 March 2018).
- Hasselhorn, H.M.; Ebener, M. Gesundheit, Arbeitsfähigkeit und Motivation bei älter werdenden Belegschaften (Health, work ability and work motivation of the ageing workforce). In Fehlzeiten-Report 2014: Erfolgreiche Unternehmen von Morgen-Gesunde Zukunft Heute Gestalten. Zahlen, Daten, Analysen aus allen Branchen der Wirtschaft (Report of Absenteeism 2014: Successful Companies of Tomorrow-Health Future Made Today. Numbers, Data, Facts of All Sectors of Industry and Commerce); Badura, B., Ducki, A., Schröder, H., Klose, J., Meyer, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 75–84. ISBN 978-3-662-43530-4. (In German) [Google Scholar]
- Walker, A. The emergence of age management in Europe. Int. J. Organ. Behav. 2005, 10, 685–697. [Google Scholar]
- Naegele, G.; Walker, A. A Guide to Good Practice in Age Management; European Foundation for the Improvement of Living and Working Conditions: Dublin, Ireland, 2006; ISBN 92-897-0934-0. [Google Scholar]
- Karasek, R.A. Job Demands, Job Decision Latitude, and Mental Strain: Implications for Job Redesign. Adm. Sci. Q. 1979, 24, 285. [Google Scholar] [CrossRef]
- Johnson, J.V. Control, collectivity and the psychosocial work environment. In Job Control and Worker Health; Sauter, S.L., Hurrell, J.J., Cooper, C.L., Eds.; John Wiley & Sons: New York, NY, USA, 1989; pp. 55–74. ISBN 0471923559. [Google Scholar]
- Siegrist, J. Soziale Krisen und Gesundheit (Social Crises and Health); Hogrefe: Göttingen, Germany, 1996; ISBN 978-3801706739. (In German) [Google Scholar]
- Demerouti, E.; Bakker, A.B. The Job Demands–Resources model: Challenges for future research. SA J. Ind. Psychol. 2011, 37, 1–9. [Google Scholar] [CrossRef]
- Peter, R.; Hasselhorn, H.M. Arbeit, Alter, Gesundheit und Erwerbsteilhabe (Work, age, health, and work participation. A theoretical model). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2013, 56, 415–421. (In German) [Google Scholar] [CrossRef] [PubMed]
- Hasselhorn, H.M.; Peter, R.; Rauch, A.; Schröder, H.; Swart, E.; Bender, S.; du Prel, J.B.; Ebener, M.; March, S.; Trappmann, M.; et al. Cohort profile: The lidA Cohort Study-a German Cohort Study on Work, Age, Health and Work Participation. Int. J. Epidemiol. 2014, 43, 1736–1749. [Google Scholar] [CrossRef] [PubMed]
- Ebener, M.; Hasselhorn, H.M. National report: Germany. In Understanding Employment Participation of Older Workers Creating a Knowledge Base for Future Labour Market Challenges; Federal Ministry of Labour and Social Affairs: Berlin, Germany, 2015; pp. 76–79. [Google Scholar]
- Burr, H.; Kersten, N.; Kroll, L.; Hasselhorn, H.M. Selbstberichteter allgemeiner Gesundheitszustand nach Beruf und Alter in der Erwerbsbevölkerung (Self-reported general health by occupation and age in the working population in Germany). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2013, 56, 349–358. (In German) [Google Scholar] [CrossRef] [PubMed]
- Feißel, A. Der Zusammenhang Zwischen Arbeitsmotivation und Gesundheit-Eine Untersuchung im Rahmen der lidA-Studie (The Assocciation between Work Motivation and Health—An Investigation Based on the lidA Study). Master’s Thesis, Otto-von-Guericke-University Magdeburg, Magdeburg, Germany, 2015, unpublished work. (In German). [Google Scholar]
- Feißel, A.; Swart, E.; March, S. The impact of work ability on work motivation and health-a longitudinal analysis based on older worker. J. Occup. Environ. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Björklund, C.; Jensen, I.; Lohela-Karlsson, M. Is a change in work motivation related to a change in mental well-being? J. Vocat. Behav. 2013, 83, 571–580. [Google Scholar] [CrossRef]
- Lohela, M.; Björklund, C.; Vingård, E.; Hagberg, J.; Jensen, I. Does a change in psychosocial work factors lead to a change in employee health? J. Occup. Environ. Med. 2009, 51, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. The “What” and “Why” of Goal Pursuits: Human Needs and the Self-Determination of Behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Locke, E.A.; Latham, G.P. Work motivation and satisfaction: Light at the end of the tunnel. Psychol. Sci. 1990, 1, 240–246. [Google Scholar] [CrossRef]
- Pines, A.M. Burnout: An existential perspective. In Professional Burnout: Recent Developments in Theory and Research; Schaufeli, W., Maslach, C., Eds.; Taylor and Francis: Philadelphia, PA, USA, 1993; pp. 33–51. ISBN 978-1560326830. [Google Scholar]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J.; Tuomi, K. Past, Present and Future of work ability. In Proceedings of the 1stInternational Symposium on Work Ability, Tampere, Finland, 5–6 September 2001; Ilmarinen, J., Lehtinen, S., Eds.; Finnish Institute of Occupational Health: Helsinki, Finland, 2004; pp. 1–25, ISBN 9789518025811. [Google Scholar]
- Tengland, P.A. The concept of work ability. J. Occup. Rehabil. 2011, 21, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. Towards a Longer Worklife! Ageing and the Quality of Worklife in the European Union; Finnish Institute of Occupational Health, Ministry of Social Affairs and Health: Helsinki, Finland, 2005; ISBN 951-802-685-8.
- Fernet, C. The role of work motivation in psychological health. Can. Psychol. Psychol. Can. 2013, 54, 72–74. [Google Scholar] [CrossRef]
- Salmela-Aro, K.; Nurmi, J.E. Employees’ motivational orientation and well-being at work. J. Organ. Chang. Manag. 2004, 17, 471–489. [Google Scholar] [CrossRef]
- Ilmarinen, J. Work ability—A comprehensive concept for occupational health research and prevention. Scand. J. Work Environ. Health 2009, 35, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Illmarinen, J. Ageing Workers in Finland and in the European Union: Their Situation and the Promotion of their Working Ability, Employability and Employment. Geneva Papers Risk Insur. 2001, 26, 623–641. [Google Scholar] [CrossRef]
- Sun, J.; Buys, N.; Wang, X. Depression in employees in privately owned enterprises in China: Is it related to work environment and work ability? Int. J. Environ. Res. Public Health 2013, 10, 1152–1167. [Google Scholar] [CrossRef] [PubMed]
- Prümper, J.; Richenhagen, G. Von der Arbeitsunfähigkeit zum Haus der Arbeitsfähigkeit: Der Work Ability Index und seine Anwendung (From incapacity of work to the House of work capacity: The Work Ability Index and its application). In Ältere Beschäftigte: Zu jung, um alt zu sein. Konzepte-Forschungsergebnisse-Instrumente (Older Worker: Too Young to be Old. Concepts-Research Results-Instruments); Seyfried, B., Ed.; Bertelsmann: Bielefeld, Germany, 2011; pp. 135–146. ISBN 978-3-7639-1144-8. (In German) [Google Scholar]
- Pohjonen, T. Perceived work ability of home care workers in relation to individual and work-related factors in different age groups. Occup. Med. 2001, 51, 209–217. [Google Scholar] [CrossRef]
- Tuomi, K.; Eskelinen, L.; Toikkanen, J.; Jarvinen, E.; Ilmarinen, J.; Klockars, M. Work load and individual factors affecting work ability among aging municipal employees. Scand. J. Work Environ. Health 1991, 17, 128–134. [Google Scholar] [PubMed]
- Abbasi, S.; Asilian Mahabadi, H.; Vosoughi, S. Work Ability of the Personnel of a Petrochemical Company and the Relationship Between Age and Physical Activities. Health Scope 2016, 6. [Google Scholar] [CrossRef]
- Wilke, C.; Ashton, P.; Elis, T.; Biallas, B.; Froböse, I. Analysis of work ability and work-related physical activity of employees in a medium-sized business. BMC Res. Notes 2015, 8, 803. [Google Scholar] [CrossRef] [PubMed]
- Golubic, R.; Milosevic, M.; Knezevic, B.; Mustajbegovic, J. Work-related stress, education and work ability among hospital nurses. J. Adv. Nurs. 2009, 65, 2056–2066. [Google Scholar] [CrossRef] [PubMed]
- Padula, R.S.; da Silva Valente, L.D.S.; de Moraes, M.V.; Chiavegato, L.D.; Cabral, C.M.N. Gender and age do not influence the ability to work. Work 2012, 41, 4330–4332. [Google Scholar] [CrossRef] [PubMed]
- Frerichs, F. Demografischer Wandel in der Erwerbsarbeit—Risiken und Potentiale alternder Belegschaften (Demographical change in the employment—Risks and potentials of aging workforces). J. Labour Mark. Res. 2015, 48, 203–216. [Google Scholar] [CrossRef]
- Rabl, T. Age, discrimination and achievement motives—A study of German Employees. Pers. Rev. 2010, 39, 448–467. [Google Scholar] [CrossRef]
- Kooji, D.; Jansen, P.G.; Dikkers, J.S.E.; de Lange, A.H. The influence of age on the associations between HR practices and both affective commitment and job satisfaction: A meta-analysis. J. Organ. Behav. 2010, 31, 1111–1136. [Google Scholar] [CrossRef]
- Hertel, G.; Thielgen, M.; Rauschenbach, C.; Grube, A.; Stamov-Roßnagel, C.; Krumm, S. Age differences in motivation and stress at work. In Age-Differentiated Work Systems; Schlick, C.M., Frieling, E., Wegge, J., Eds.; Springer: Berlin, Germany; New York, NY, USA, 2013; pp. 119–147. ISBN 9783642350566. [Google Scholar]
- Feißel, A.; Swart, E.; March, S. Gesundheit von älteren Erwerbstätigen-Ergebnisse der Erstbefragung aus der lidA-Studie (Health of older workers. Results of the baseline survey from the lidA study). Zbl Arbeitsmed. 2016, 66, 129–136. [Google Scholar] [CrossRef]
- Faltermaier, T. Geschlechtsspezifische Dimensionen im Gesundheitsverständnis und Gesundheitsverhalten (Gender dimensions in the understanding of health and health behavior). In Fehlzeiten-Report 2007: Arbeit, Geschlecht und Gesundheit, Geschlechteraspekte im Betrieblichen Gesundheitsmanagement. Zahlen, Daten, Analysen aus allen Branchen der Wirtschaft (Work, Gender and Health, Gender Aspects in Occupational Health Management. Numbers, Data, Facts of All Sectors of Industry and Commerce); Badura, B., Schröder, H., Vetter, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2007; ISBN 9783540725435. (In German) [Google Scholar]
- Hasselhorn, H.M.; Freude, G. Der Work-Ability-Index: Ein Leitfaden (The Work Ability Index: A Guide); Wirtschaftsverl. NW, Verl. für Neue Wiss: Bremerhaven, Germany, 2007; ISBN 978-3-86509-702-6. [Google Scholar]
- Tuomi, K.; Huuhtanen, P.; Nykyri, E.; Ilmarinen, J. Promotion of work ability, the quality of work and retirement. Occup. Med. 2001, 51, 318–324. (In German) [Google Scholar] [CrossRef]
- Schreurs, B.; Cuyper, N.D.; van Emmerik, I.J.H.; Notelaers, G.; Witte, H.D. Job demands and resources and their associations with early retirement intentions through recovery need and work enjoyment. SA J. Ind. Psychol. 2011, 37. [Google Scholar] [CrossRef]
- Du Prel, J.B.; Iskenius, M.; Peter, R. Are effort-reward imbalance and social isolation mediating the association between education and depressiveness? Baseline findings from the lidA(§)-study. Int. J. Public Health 2014, 59, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Van Vegchel, N.; De Jonge, J.; Bosma, H.; Schaufeli, W. Reviewing the effort-reward imbalance model: Drawing up the balance of 45 empirical studies. Soc. Sci. Med. 2005, 60, 1117–1131. [Google Scholar] [CrossRef] [PubMed]
- Van Vegchel, N.; De Jonge, J.; Landsbergs, P.A. Occupational Stress in (Inter)action: The Interplay between Job Demands and Job Resources. J. Organ. Behav. 2005, 26, 553–560. [Google Scholar] [CrossRef]
- Wilkins, K.; Beaudet, M.P. Work stress and health. Health Rep. 1998, 10, 47–63. [Google Scholar] [PubMed]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990; ISBN 978-0465028979. [Google Scholar]
- Xanthopoulou, D.; Bakker, A.B.; Demerouti, E.; Schaufeli, W.B. The role of personal resources in the job demands-resources model. Int. J. Stress Manag. 2007, 14, 121–141. [Google Scholar] [CrossRef]
- Varekamp, I.; van Dijk, F.J.H.; Kroll, L.E. Workers with a chronic disease and work disability. Problems and solutions. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2013, 56, 406–414. [Google Scholar] [CrossRef]
- Sporket, M. Alternsmanagement in der betrieblichen Praxis: Motive, Umsetzung und Effekte. Z. Gerontol. Geriatr. 2009, 42, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Slesina, W. Betriebliche Gesundheitsförderung in der Bundesrepublik Deutschland (Workplace Health Promotion in the Federal Republic of Germany). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2008, 51, 296–304. (In German) [Google Scholar] [CrossRef] [PubMed]
- Hymel, P.A.; Loeppke, R.R.; Baase, C.M.; Burton, W.N.; Hartenbaum, N.P.; Hudson, T.W.; McLellan, R.K.; Mueller, K.L.; Roberts, M.A.; Yarborough, C.M.; et al. Workplace health protection and promotion: A new pathway for a healthier-and safer-workforce. J. Occup. Environ. Med. 2011, 53, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J.; Tempel, J. Erhaltung, Förderung und Entwicklung der Arbeitsfähigkeit-Konzepte und Forschungsergebnisse aus Finnland (Preservation, promotion and development of working capacity concepts and research of Finland). In Fehlzeiten-Report 2002: Demographischer Wandel: Herausforderung für die betriebliche Personal- und Gesundheitspolitik; Zahlen, Daten, Analysen aus allen Branchen der Wirtschaft. Zahlen, Daten, Analysen aus allen Branchen der Wirtschaft (Report of Absenteeism 2002. Demographic Change: Challenge for Company Personnel and Health Policy. Numbers, Data, Facts of All Sectors of Indutrry and Commerce); Badura, B., Astor, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2003; pp. 86–99. ISBN 9783540436256. (In German) [Google Scholar]
- Campbell Quick, J.; Macik-Frey, M.; Cooper, C.L. Managerial Dimensions of Organizational Health: The Healthy Leader at Work. J. Manag. Stud. 2007, 44, 189–205. [Google Scholar] [CrossRef]
- Salciuviene, L.; Hopeniene, R.; Dovaliene, A. Perceived Corporate Social Responsibility and its Implementation in Practice: The Case of Lithuanian Small and Medium-Sized Enterprises. Inzinerine Ekonomika-Eng. Econ. 2016, 27. [Google Scholar] [CrossRef]
- Vázquez-Burguete, J.L.; Sahelices-Pinto, C.; Lanero-Carrizo, A. Corporate social responsibility and consumer behavior in the cosmetics sector: A study in the Spanish context. Int. Rev. Public Nonprofit Mark. 2017, 14, 375–390. [Google Scholar] [CrossRef]
- Gharleghi, B.; Afshar Jahanshahi, A.; Nawaser, K. The Outcomes of Corporate Social Responsibility to Employees: Empirical Evidence from a Developing Country. Sustainability 2018, 10, 698. [Google Scholar] [CrossRef]
- Shin, I.; Hur, W.-M.; Kim, M.; Kang, S. Hidden Roles of CSR: Perceived Corporate Social Responsibility as a Preventive against Counterproductive Work Behaviors. Sustainability 2017, 9, 955. [Google Scholar] [CrossRef]
- Schwarze, M.; Egen, C.; Gutenbrunner, C.; Schriek, S. Early Workplace Intervention to Improve the Work Ability of Employees with Musculoskeletal Disorders in a German University Hospital-Results of a Pilot Study. Healthcare 2016, 4, 64. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Level | Measures |
|---|---|
| individual | being a role-model behavior-based preventive approach to overall working conditions (environment promoting physical activities, healthy nutrition at work, addiction prevention, stress management, etc.) |
| interpersonal | appreciation/acceptance of the experience/competences of older employees participation, participation in decision-making, involvement, empowerment creating transparency, meaningfulness, offering support integration in personnel development and recruiting processes flat hierarchies culture of trust age-adequate staff orientation mixed teams corporate social responsibility activities |
| structural | extending opportunities for control/autonomy offering further training opportunities need-based working time and vacation planning reduction of job demands integration into existing management systems age-adequate design of workplaces, work organization and work environment incentive systems for remaining with the company |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feißel, A.; Peter, R.; Swart, E.; March, S. Developing an Extended Model of the Relation between Work Motivation and Health as Affected by the Work Ability as Part of a Corporate Age Management Approach. Int. J. Environ. Res. Public Health 2018, 15, 779. https://doi.org/10.3390/ijerph15040779
Feißel A, Peter R, Swart E, March S. Developing an Extended Model of the Relation between Work Motivation and Health as Affected by the Work Ability as Part of a Corporate Age Management Approach. International Journal of Environmental Research and Public Health. 2018; 15(4):779. https://doi.org/10.3390/ijerph15040779
Chicago/Turabian StyleFeißel, Annemarie, Richard Peter, Enno Swart, and Stefanie March. 2018. "Developing an Extended Model of the Relation between Work Motivation and Health as Affected by the Work Ability as Part of a Corporate Age Management Approach" International Journal of Environmental Research and Public Health 15, no. 4: 779. https://doi.org/10.3390/ijerph15040779