Spatio-Temporal Modeling of Zika and Dengue Infections within Colombia



Abstract
:1. Introduction
2. Materials and Methods
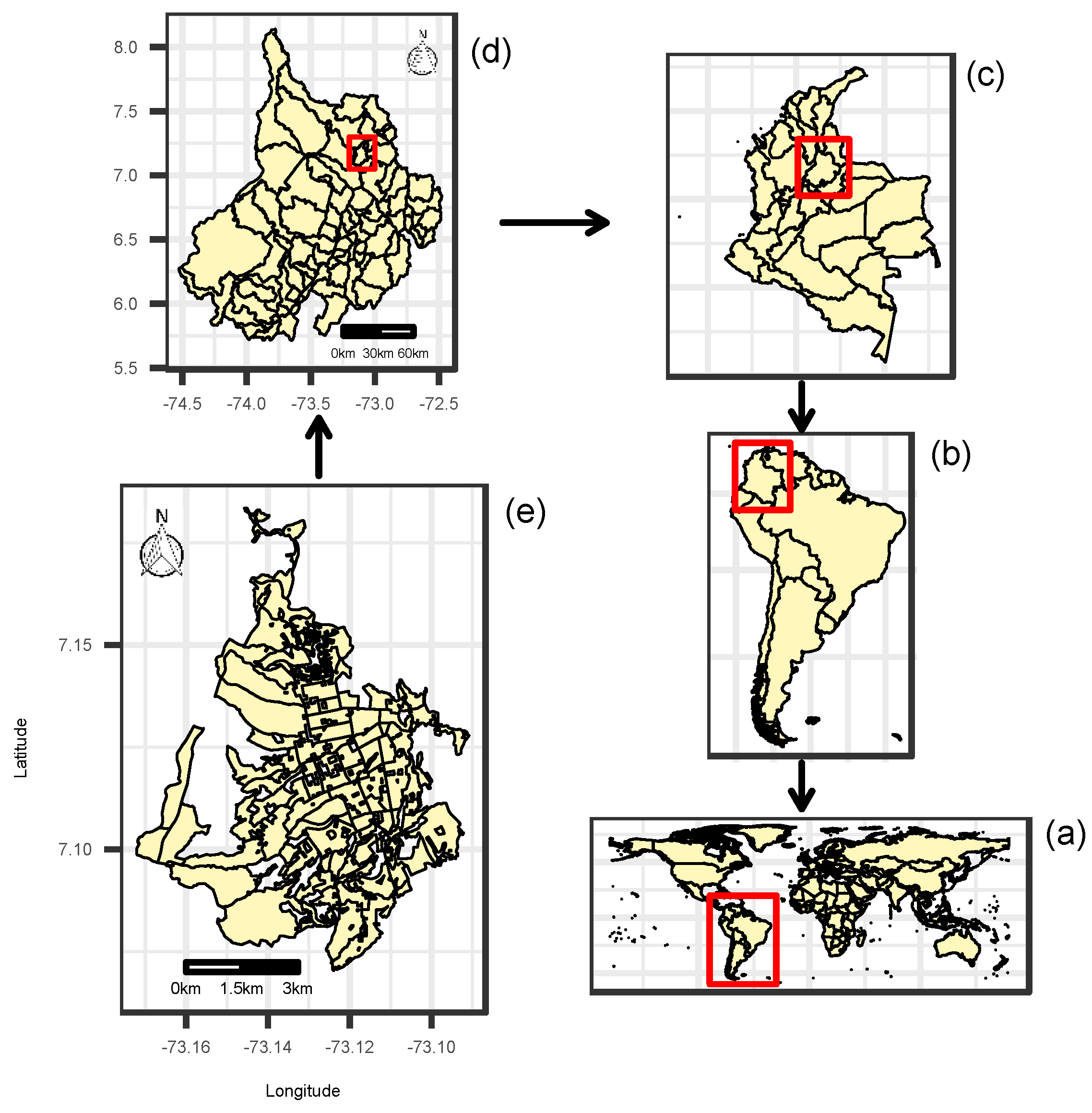
2.1. Zika and Dengue Data in Santander and Bucaramanga, Colombia
2.2. Expected Values for ZVD and Dengue
2.3. Spatio-Temporal Relative Risk Models
2.4. Inference
3. Results
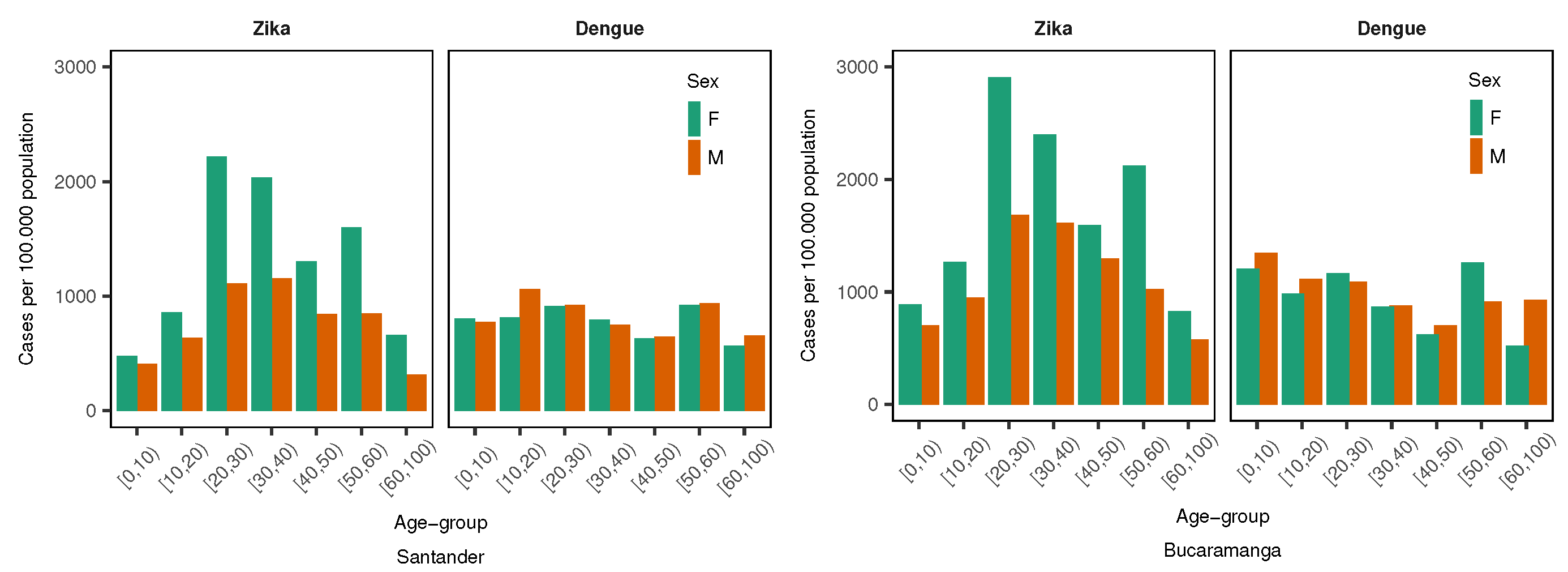
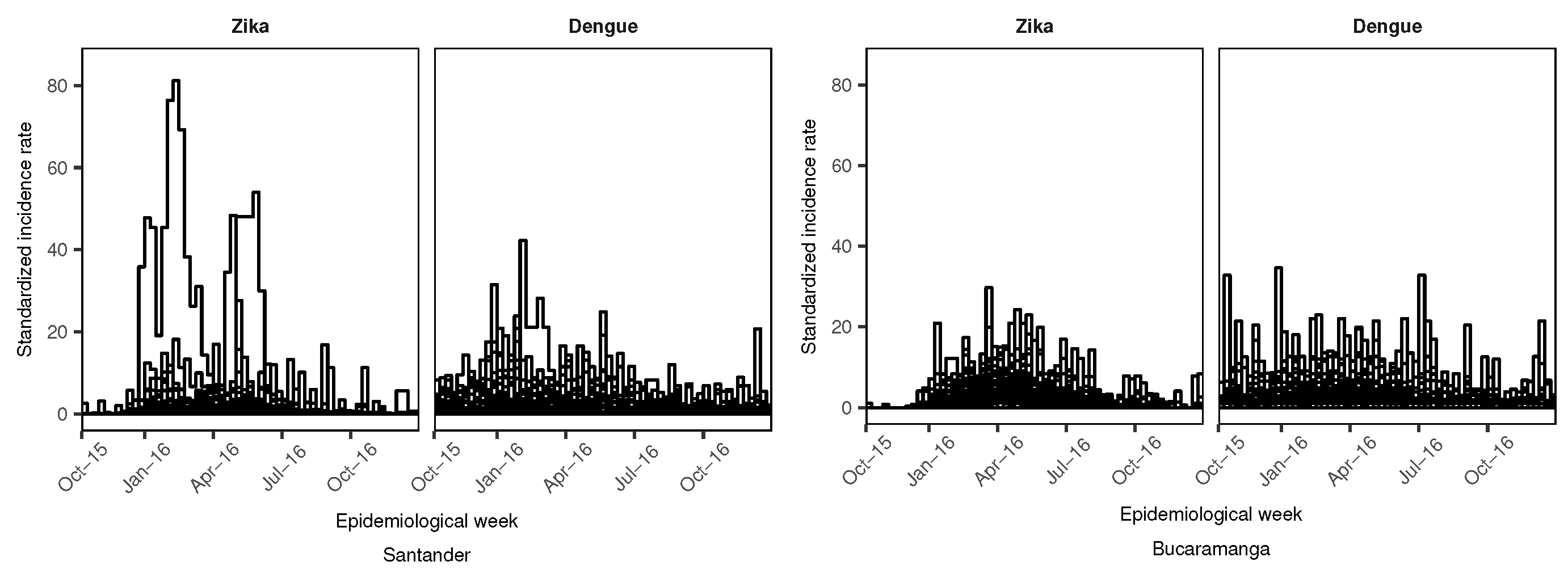
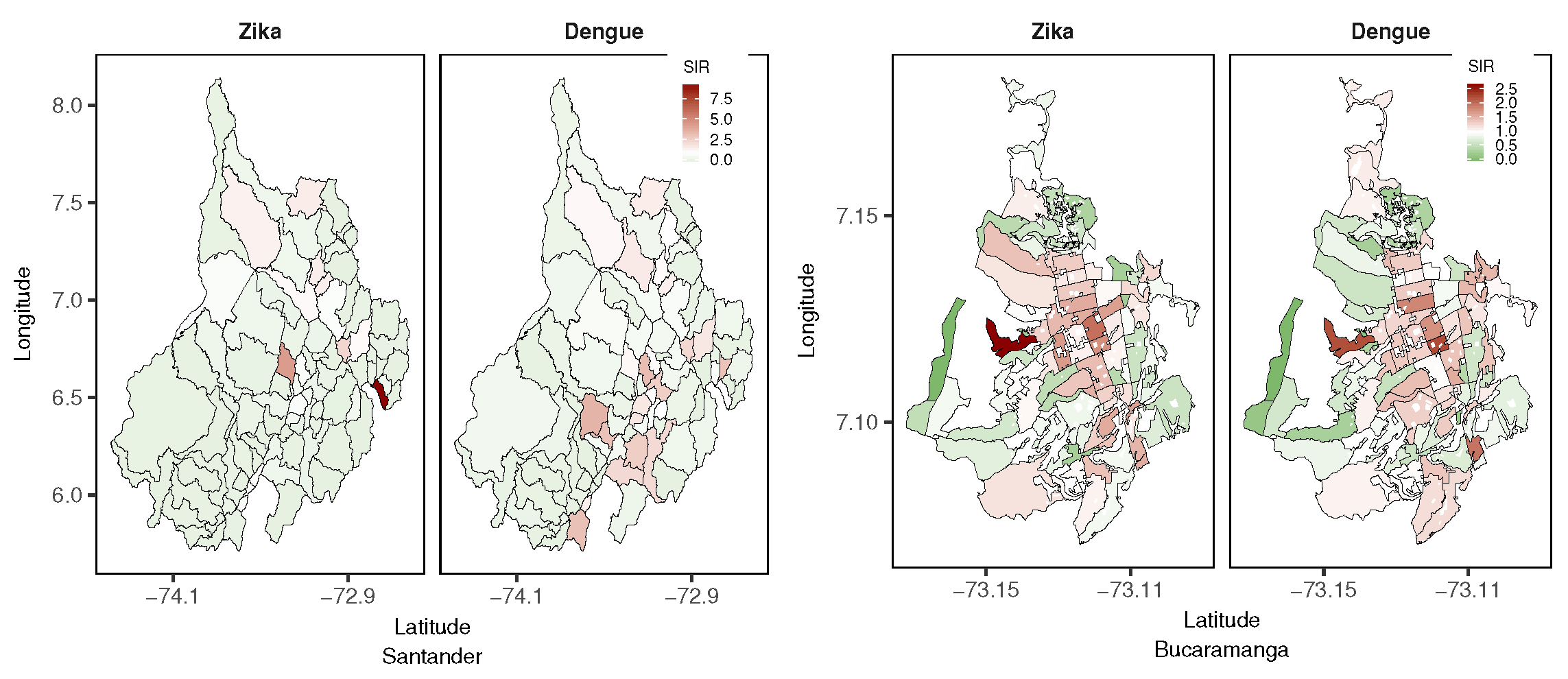
3.1. Exploratory Data Analysis
3.2. Model Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CI | Credible Intervals |
| CAR | Conditional Autorregressive |
| DANE | Departamento Nacional de Estadística |
| EW | Epidemiological Week |
| INLA | Integrated Nested Laplace Approximation |
| IR | Incidence Rate |
| LEB | Local Empirical Bayes |
| LS | Logarithmic Score |
| RW1 | Random Walk 1 |
| RW2 | Random Walk 2 |
| SD | Standard Deviation |
| SIR | Standardized Incidence Ratio |
| SIVIGILA | Sistema de Vigilancia en Salud Pública (Public Health Surveillance System) |
| TSIR | Time-dependent Susceptible-Infectious-Recovered |
| WAIC | Watanabe-Akaike Information Criterion |
| ZVD | Zika Virus Disease |
References
- Villar, L.A.; Rojas, D.P.; Besada-Lombana, S.; Sarti, E. Epidemiological Trends of Dengue Disease in Colombia (2000–2011): A Systematic Review. PLoS. Negl. Trop. Dis. 2015, 9, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Plourde, A.R.; Bloch, E.M. A Literature Review of Zika Virus. Emerg. Infect. Dis. 2016, 22, 1185–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan American Health Organization/World Health Organization. Zika Suspected and Confirmed Cases Reported by Countries and Territories in the Americas Cumulative Cases, 2015–2017; PAHO/WHO: Washington, DC, USA, 2017. [Google Scholar]
- National Health Institute. Weekly Epidemiologic Bulletin: Epidemiological Week Number 52 of 2016, 25 December–31 December; National Health Institute, Direction of Surveillance and Risk Analysis in Public Health: Bogotá, Colombia, 2016. (In Spanish)
- National Health Institute. Event Report: Dengue, 2016; National Health Institute, Direction of Surveillance and Risk Analysis in Public Health: Bogotá, Colombia, 2016. (In Spanish)
- Pacheco, O.; Beltrán, M.; Nelson, C.A.; Diana, V.M.S.; Natalia, T.M.D.; Farr, S.L.; Padilla, A.V.; Tong, V.T.; Esther, M.P.H.; Cuevas, M.S.; et al. Zika Virus Disease in Colombia—Preliminary Report. N. Engl. J. Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Rojas, D.P.; Dean, N.E.; Yang, Y.; Kenah, E.; Quintero, J.; Tomasi, S.; Ramirez, E.L.; Kelly, Y.; Castro, C.; Carrasquilla, G.; et al. The epidemiology and transmissibility of Zika virus in Girardot and San Andres island, Colombia, September 2015 to January 2016. Euro Surveill. 2016, 21, 30283. [Google Scholar] [CrossRef] [PubMed]
- Tolosa, N.; Tinker, S.C.; Pacheco, O.; Valencia, D.; Salas-Botero, D.; Tong, V.T.; Mercado, M.; Gilboaet, S.M. Zika Virus Disease in Children in Colombia, August 2015 to May 2016. Paediatr. Perinat. Epidemiol. 2017, 31, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Patiño-Cadavid, L.J.; Lozada-Riasco, C.O.; Villamil-Gómez, W.E. Mapping Zika in municipalities of one coastal department of Colombia (Sucre) using geographic information systems during the 2015–2016 outbreak: Implications for public health and travel advice. Int. J. Infect. Dis. 2016, 48, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Galindo-Marquez, M.L.; García-Loaiza, C.J. Mapping Zika virus infection using geographical information systems in Tolima, Colombia, 2015–2016. F1000Research 2016, 5, 568. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; García-Loaiza, C.J.; Galindo-Marquez, M.L.; Sabogal-Roman, J.A.; Marin-Loaiza, S.; Lozada-Riascos, C.O.; Díaz-Quijano, F.A. Zika infection GIS-based mapping suggest high transmission activity in the border area of La Guajira, Colombia, a northeastern coast Caribbean department, 2015–2016: Implications for public health, migration and travel. Travel Med. Infect. Dis. 2016, 14, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Haque, U.; Ball, J.D.; García-Loaiza, C.J.; Galindo-Marquez, M.L.; Sabogal-Romanm, J.A.; Marin-Loaiza, S.; Ayala, A.F.; Lozada-Riascos, C.O.; Diaz-Quijano, F.A.; et al. Spatial distribution of Zika virus infection in Northeastern Colombia. Infez. Med. 2017, 3, 241–246. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Ruiz, P.; Tabares, J.; Ossa, C.A.; Yepes-Echeverry, M.C.; Ramirez-Jaramillo, V.; Galindo-Marquez, M.L.; García-Loaiza, C.J.; Sabogal-Roman, J.A.; Parra-Valencia, E.; et al. Mapping the ecoepidemiology of Zika virus infection in urban and rural areas of Pereira, Risaralda, Colombia, 2015–2016: Implications for public health and travel medicine. Travel Med. Infect. Dis. 2017, 18, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Towers, S.; Brauer, F.; Castillo-Chavez, C.; Falconar, A.K.I.; Mubayi, A.; Romero-Vivas, C.M.E. Estimate of the reproduction number of the 2015 Zika virus outbreak in Barranquilla, Colombia, and estimation of the relative role of sexual transmission. Epidemics 2016, 17, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Ospina, J.; Hincapie-Palacio, D.; Ochoa, J.; Molina, A.; Rua, G.; Pajaro, D.; Arrubla, M.; Almanza, R.; Paredes, M.; Mubayi, A. Stratifying the potential local transmission of Zika in municipalities of Antioquia, Colombia. Trop. Med. Int. Health 2017, 22, 1249–1265. [Google Scholar] [CrossRef] [PubMed]
- Sebrango-Rodríguez, C.R.; Martínez-Bello, D.A.; Sánchez-Valdés, L.; Thilakarathne, P.J.; Del Fava, E.; Vand, S.P.; López-Quílez, A.; Shkedy, Z. Parameter Estimation and Real-Time Predictions of a Single Zika Outbreak Using Model Averaging. Epidemiol. Infect. 2017, 145, 2313–2323. [Google Scholar] [CrossRef] [PubMed]
- Lee, D. A comparison of conditional autoregressive models used in Bayesian disease mapping. Spat. Spatio Tempor. Epidemiol. 2011, 2, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Louis, V.R.; Phalkey, R.; Horstick, O.; Ratanawong, P.; Wilder-Smith, A.; Tozan, Y.; Dambach, P. Modeling tools for dengue risk mapping—A systematic review. Int. J. Health Geogr. 2014, 13, 50. [Google Scholar] [CrossRef] [PubMed]
- Lowe, R.; Bailey, T.C.; Stephenson, D.B.; Graham, R.J.; Coelho, C.A.S.; S Carvalho, M.; Barcellos, C. Spatio-temporal modelling of climate-sensitive disease risk: Towards an early warning system for dengue in Brazil. Comput. Geosci. 2011, 37, 371–381. [Google Scholar] [CrossRef] [Green Version]
- Lowe, R.; Bailey, T.; Stephenson, D.; Jupp, T.; Graham, R.; Barcellos, C.; Carvalho, M. The development of an early warning system for climate-sensitive disease risk with a focus on dengue epidemics in Southeast Brazil. Stat. Med. 2013, 32, 864–883. [Google Scholar] [CrossRef] [PubMed]
- Lowe, R.; Barcellos, C.; Coelho, C.; Bailey, T.; Coelho, G.; Graham, R.; Jupp, T.; Massa-Ramalho, W.; Stephenson, D.; Rodó, X. Dengue outlook for the World Cup in Brazil: an early warning model framework driven by real-time seasonal climate forecasts. Lancet Infect. Dis. 2014, 14, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Lowe, R.; Cazelles, B.; Paul, R.; Rodó, X. Quantifying the added value of climate information in a spatio-temporal dengue model. Stoch. Environ. Res. Risk Assess. 2016, 30, 2067–2078. [Google Scholar] [CrossRef]
- Restrepo, A.C.; Baker, P.; Clements, A.C.A. National spatial and temporal patterns of notified dengue cases, Colombia 2007–2010. Trop. Med. Int. Health 2014, 19, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Arboleda, S.; Jaramillo, N.; Peterson, A.T. Mapping Environmental Dimensions of Dengue Fever Transmission Risk in the Aburrá Valley, Colombia. Int. J. Environ. Res. Public Health 2009, 6, 3040–3055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Bello, D.A.; López-Quílez, A.; Torres-Prieto, A. Bayesian dynamic modeling of time series of dengue disease case counts. PLoS. Negl. Trop. Dis. 2017, 11, e0005696. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Bello, D.A.; López-Quílez, A.; Torres Prieto, A. Relative risk estimation of dengue disease at small spatial scale. Int. J. Health Geogr. 2017, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Bello, D.; López-Quílez, A.; Torres Prieto, A. Spatiotemporal modeling of relative risk of dengue disease in Colombia. Stoch. Environ. Res. Risk Assess. 2018, 32, 1587–1601. [Google Scholar] [CrossRef]
- Stewart-Ibarra, A.; Muñoz, Á.; Ryan, S.; Ayala, E.; Borbor-Cordova, M.; Finkelstein, J.; Mejía, R.; Ordoñez, T.; Recalde-Coronel, G.; Rivero, K. Spatiotemporal clustering climate periodicity and social-ecological risk factors for dengue during an outbreak in Machala, Ecuador, in 2010. Infect. Dis. 2014, 14, 610. [Google Scholar] [CrossRef] [PubMed]
- Lippi, C.A.; Stewart-Ibarra, A.M.; Muñoz, Á.G.; Borbor-Cordova, M.J.; Mejía, R.; Rivero, K.; Castillo, K.; Cárdenas, W.B.; Ryan, S.J. The Social and Spatial Ecology of Dengue Presence and Burden during an Outbreak in Guayaquil, Ecuador, 2012. Int. J. Environ. Res. Public Health 2018, 15, 827. [Google Scholar] [CrossRef] [PubMed]
- Wijayanti, S.P.M.; Porphyre, T.; Chase-Topping, M.; Rainey, S.M.; McFarlane, M.; Schnettler, E.; Biek, R.; Kohl, A. The Importance of Socio-Economic Versus Environmental Risk Factors for Reported Dengue Cases in Java, Indonesia. PLoS. Negl. Trop. Dis. 2016, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc. Ser. B 2009, 71, 319–392. [Google Scholar] [CrossRef] [Green Version]
- Knorr-Held, L. Bayesian modelling of inseparable space-time variation in disease risk. Stat. Med. 2000, 19, 2555–2567. [Google Scholar] [CrossRef] [Green Version]
- Abd Naeeim, N.S.; Rahman, N.A. Estimating relative risk for dengue disease in Peninsular Malaysia using INLA. Malays. J. Fund. Appl. Sci. 2017, 13, 721–727. [Google Scholar] [CrossRef]
- National Health Institute of Colombia. Methodology of the Routinary Surveillance Statistical Operation; Health Ministry of Colombia, National Health Institute: Bogotá, Colombia, 2018. (In Spanish)
- National Administrative Department of Statistics (DANE). Urban Sector Level Layer, Department of Santander; National Administrative Department of Statistics (DANE): Bogotá, Colombia, 2005. (In Spanish)
- National Administrative Department of Statistics (DANE). Census 2005; National Administrative Department of Statistics (DANE): Bogotá, Colombia, 2005. (In Spanish)
- Banerjee, S.; Carlin, B.; Gelfand, A. Hierarchical Modeling and Analyisis for Spatial Data; Chapman & Hall/CRC: Boca Raton, FL, USA, 2015; p. 529. [Google Scholar]
- Leroux, B.G.; Lei, X.; Breslow, N. Estimation of disease rates in small areas: A new mixed model for spatial dependence. In Statistical Models in Epidemiology, the Environment and Clinical Trials; Halloran, M., Berry, D., Eds.; Springer: New York, NY, USA, 1999; pp. 179–191. [Google Scholar]
- Ugarte, M.D.; Adin, A.; Goicoa, T.; Militino, A.F. On fitting spatio-temporal disease mapping models using approximate Bayesian inference. Stat. Methods Med. Res. 2014, 23, 507–530. [Google Scholar] [CrossRef] [PubMed]
- Ugarte, M.; Adin, A.; Goicoa, T. Two-level spatially structured models in spatio-temporal disease mapping. Stat. Methods Med. Res. 2016, 25, 1080–1100. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Goicoa, T.; Adin, A.; Ugarte, M.D.; Hodges, J.S. In spatio-temporal disease mapping models, identifiability constraints affect PQL and INLA results. Stoch. Environ. Res. Risk Assess. 2018, 32, 749–770. [Google Scholar] [CrossRef]
- Watanabe, S. Asymptotic equivalence of bayes cross validation and widely applicable information criterion in singular learning theory. J. Mach. Learn. Res. 2010, 11, 3571–3594. [Google Scholar]
- Gneiting, T.; Raftery, A.E. Strictly proper scoring rules, prediction, and estimation. J. Am. Stat. Assoc. 2007, 102, 359–378. [Google Scholar] [CrossRef]
- Krystosik, A.R.; Curtis, A.; Buritica, P.; Ajayakumar, J.; Squires, R.; Dávalos, D.; Pacheco, R.; Bhatta, M.P.; James, M.A. Community context and sub-neighborhood scale detail to explain dengue, chikungunya and Zika patterns in Cali, Colombia. PLoS ONE 2017, 12, e0181208. [Google Scholar] [CrossRef] [PubMed]
- Chien, L.-C.; Lin, R.-T.; Liao, Y.; Francisco, S.S.; Pérez, A. Surveillance on the endemic of Zika virus infection by meteorological factors in Colombia: A population-based spatial and temporal study. BMC Infect. Dis. 2018, 18, 180. [Google Scholar]
- Stewart-Ibarra, A.M.; Hargrave, A.; Diaz, A.; Kenneson, A.; Madden, D.; Romero, M.M.; Molina, J.P.; Macias, S.D. Psychological Distress and Zika, Dengue and Chikungunya Symptoms Following the 2016 Earthquake in Bahía de Caráquez, Ecuador. Int. J. Environ. Res. Public Health 2017, 14, 1516. [Google Scholar] [CrossRef] [PubMed]
- Riou, J.; Chiara, P.; Boelle, P.Y. A comparative analysis of Chikungunya and Zika transmission. Epidemics 2017, 19, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Perkins, T.A.; Metcalf, C.J.E.; Grenfell, B.T.; Tatem, A.J. Estimating drivers of autochthonous transmission of Chikungunya virus in its invasion of the Americas. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, B.S.; Lorenz, C.; Virginio, F.; Suesdek, L.; Chiaravalloti-Neto, F. Potential risks of Zika and chikungunya outbreaks in Brazil: A modeling study. Int. J. Infect. Dis. 2018, 70, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Lowe, R.; Barcellos, C.; Brasil, P.; Cruz, O.G.; Honório, N.A.; Kuper, H.; Carvalho, M.S. The Zika Virus Epidemic in Brazil: From Discovery to Future Implications. Int. J. Environ. Res. Public Health 2018, 15, 96. [Google Scholar] [CrossRef] [PubMed]
- Saiz, J.-C.; Martín-Acebes, M.A.; Bueno-Marí, R.; Salomón, O.D.; Villamil-Jiménez, L.C.; Heukelbach, J.; Alencar, C.H.; Armstrong, P.K.; Ortiga-Carvalho, T.M.; Mendez-Otero, R.; et al. Zika Virus: What Have We Learnt Since the Start of the Recent Epidemic? Front. Microbiol. 2017, 8, 1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallam, M.F.; Fizer, C.; Pilant, A.N.; Whung, P.-Y. Systematic Review: Land Cover, Meteorological, and Socioeconomic Determinants of Aedes Mosquito Habitat for Risk Mapping. Int. J. Environ. Res. Public Health 2017, 14, 1230. [Google Scholar] [CrossRef] [PubMed]
- Romero-Vega, L.; Pacheco, O.; de la Hoz-Restrepo, F.; Díaz-Quijano, F.A. Evaluation of dengue fever reports during an epidemic, Colombia. Rev. Sáude Públ. 2014, 48, 899–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Institute of Colombia. Subregister of Zika in Girardot, Cundinamarca, 2015–2016. Inf. Quinc. Epidemiol. Nac. 2016, 21, 501–522. (In Spanish) [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Zika | Dengue | |||||||
|---|---|---|---|---|---|---|---|---|
| Deviance | p | WAIC | LS | Deviance | p | WAIC | LS | |
| Department of Santander | ||||||||
| No interaction | 6290.6 | 115.7 | 6592.6 | 3307.4 | 8308.4 | 112.7 | 8490.5 | 4236.5 |
| Type I | 4222.8 | 630.5 | 4855.0 | 4570.9 | 7278.4 | 623.9 | 7934.2 | 4156.7 |
| Type II | 4166.2 | 410.4 | 4562.9 | 2362.7 | 6979.7 | 435.3 | 7413.6 | 3738.7 |
| Type III | 4247.6 | 589.1 | 4856.3 | 4147.4 | 7314.4 | 589.0 | 7968.7 | 4143.6 |
| Type IV | 4206.4 | 382.1 | 4593.7 | 2437.6 | 7044.8 | 408.1 | 7470.9 | 3764.0 |
| City of Bucaramanga | ||||||||
| No interaction | 7852.1 | 105.0 | 7970.1 | 3985.3 | 7938.5 | 93.9 | 8042.5 | 4021.4 |
| Type I | 7659.3 | 275.0 | 7949.3 | 3980.8 | 7680.3 | 318.2 | 8018.5 | 4014.6 |
| Type II | 7537.5 | 263.7 | 7808.2 | 3907.3 | 7841.2 | 165.6 | 8024.2 | 4012.8 |
| Type III | 7653.2 | 247.7 | 7913.6 | 3961.5 | 7865.6 | 159.9 | 8040.7 | 4021.2 |
| Type IV | 7576.6 | 218.7 | 7804.1 | 3904.1 | 7839.7 | 155.8 | 8010.4 | 4005.7 |
| Zika | Dengue | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 2.5% | 50% | 97.5% | Mean | SD | 2.5% | 50% | 97.5% | |
| Department of Santander | ||||||||||
| 0.61 | 0.17 | 0.26 | 0.63 | 0.90 | 0.50 | 0.18 | 0.17 | 0.50 | 0.84 | |
| 2.36 | 0.33 | 1.80 | 2.34 | 3.05 | 2.04 | 0.32 | 1.49 | 2.02 | 2.73 | |
| 0.32 | 0.04 | 0.24 | 0.31 | 0.41 | 0.11 | 0.02 | 0.08 | 0.11 | 0.16 | |
| 0.06 | 0.04 | 0.01 | 0.05 | 0.16 | 0.04 | 0.02 | 0.01 | 0.04 | 0.09 | |
| 0.36 | 0.02 | 0.31 | 0.36 | 0.40 | 0.23 | 0.01 | 0.20 | 0.23 | 0.25 | |
| City of Bucaramanga | ||||||||||
| 0.55 | 0.20 | 0.16 | 0.55 | 0.89 | 0.49 | 0.19 | 0.15 | 0.49 | 0.84 | |
| 0.48 | 0.07 | 0.36 | 0.48 | 0.64 | 0.52 | 0.08 | 0.39 | 0.51 | 0.68 | |
| 0.42 | 0.06 | 0.33 | 0.42 | 0.54 | 0.19 | 0.04 | 0.13 | 0.18 | 0.27 | |
| 0.07 | 0.06 | 0.01 | 0.06 | 0.25 | 0.07 | 0.04 | 0.02 | 0.07 | 0.16 | |
| 0.17 | 0.02 | 0.14 | 0.17 | 0.21 | 0.10 | 0.02 | 0.07 | 0.10 | 0.14 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Bello, D.A.; López-Quílez, A.; Torres Prieto, A. Spatio-Temporal Modeling of Zika and Dengue Infections within Colombia. Int. J. Environ. Res. Public Health 2018, 15, 1376. https://doi.org/10.3390/ijerph15071376
Martínez-Bello DA, López-Quílez A, Torres Prieto A. Spatio-Temporal Modeling of Zika and Dengue Infections within Colombia. International Journal of Environmental Research and Public Health. 2018; 15(7):1376. https://doi.org/10.3390/ijerph15071376
Chicago/Turabian StyleMartínez-Bello, Daniel Adyro, Antonio López-Quílez, and Alexander Torres Prieto. 2018. "Spatio-Temporal Modeling of Zika and Dengue Infections within Colombia" International Journal of Environmental Research and Public Health 15, no. 7: 1376. https://doi.org/10.3390/ijerph15071376
APA StyleMartínez-Bello, D. A., López-Quílez, A., & Torres Prieto, A. (2018). Spatio-Temporal Modeling of Zika and Dengue Infections within Colombia. International Journal of Environmental Research and Public Health, 15(7), 1376. https://doi.org/10.3390/ijerph15071376