Serum Uric Acid in Roma and Non-Roma—Its Correlation with Metabolic Syndrome and Other Variables

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Statistical Analysis
3. Results
3.1. Description of the Study Population
3.1.1. Baseline Parameters of Study Cohorts
3.1.2. Uric Acid and Ethnicity
3.2. Uric Acid Levels and Its Relationship to Demographic and Socioeconomic Variables
3.3. Uric Acid and Its Relationship to Biochemical Variables
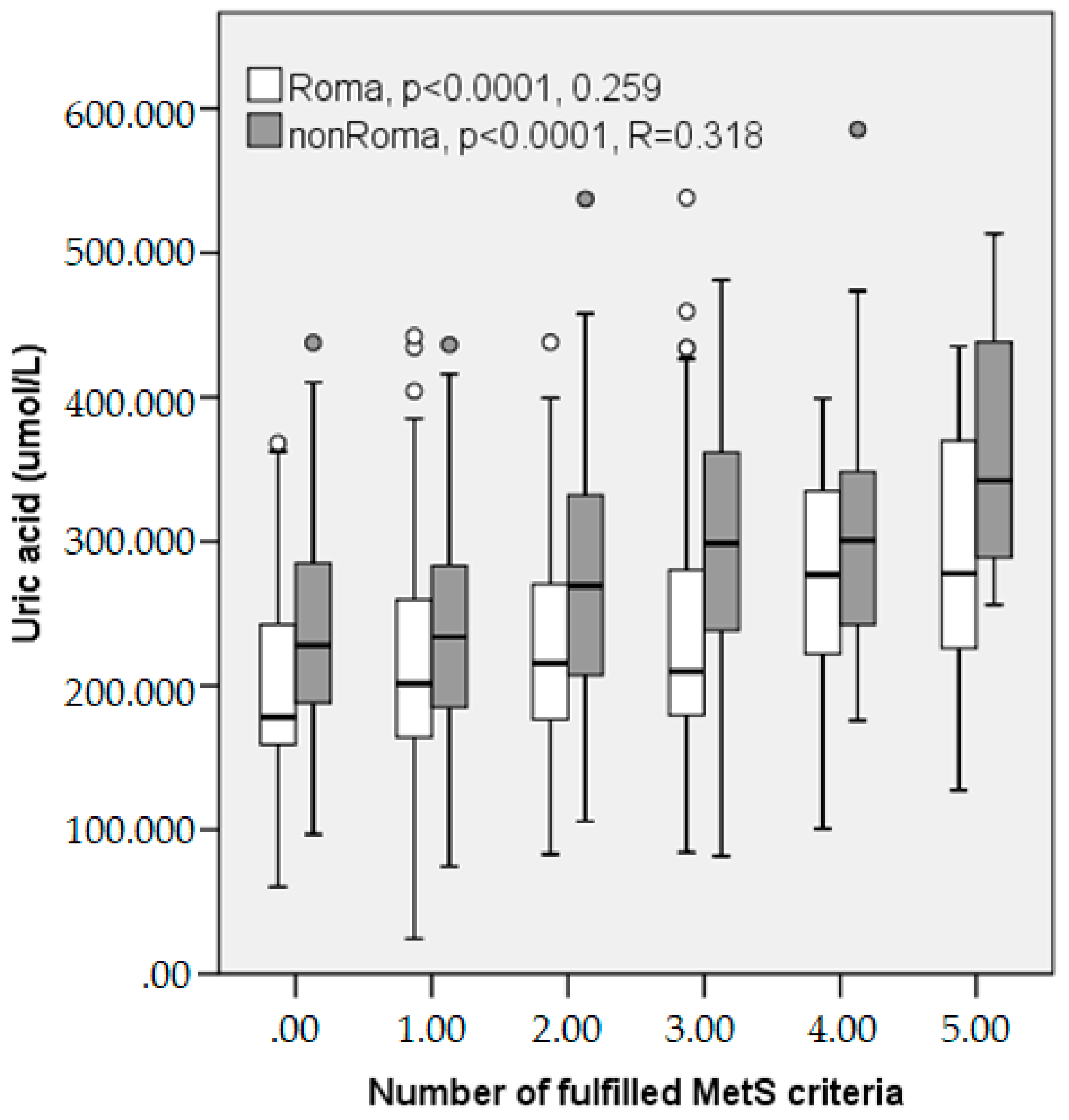
3.4. Uric Acid and Its Relationship to Metabolic Syndrome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baker, D.; Mead, N.; Campbell, S. Inequalities in morbidity and consulting behaviour for socially vulnerable groups. Br. J. Gen. Pract. 2002, 52, 124–130. [Google Scholar] [PubMed]
- Sinha, S.; Misra, P.; Kant, S.; Krishnan, A.; Nongkynrih, B.; Vikram, N.K. Prevalence of metabolic syndrome and its selected determinants among urban adult women in South Delhi, India. Postgrad. Med. J. 2013, 89, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Koupilová, I.; Epstein, H.; Holčík, J.; Hajioff, S.; McKee, M. Health needs of the Roma population in the Czech and Slovak Republics. Soc. Sci. Med. 2001, 53, 1191–1204. [Google Scholar] [CrossRef]
- Chiou, W.K.; Wang, M.H.; Huang, D.H.; Chiu, H.T.; Lee, Y.J.; Lin, J.D. The relationship between serum uric acid level and metabolic syndrome: Differences by sex and age in Taiwanese. J. Epidemiol. 2010, 20, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.; Cherubini, A.; Ble, A.; Bos, A.J.; Maggio, M.; Dixit, V.D.; Lauretani, F.; Bandinelli, S.; Senin, U.; Ferrucci, L. Uric acid and inflammatory markers. Eur. Heart J. 2006, 27, 1174–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, S.M.; Brewer, H.B., Jr.; Cleeman, J.I.; Smith, S.C., Jr.; Lenfant, C. National heart, lung, and blood institute; american heart association. Definition of metabolic syndrome: Report of the national heart, lung, and blood institute/american heart association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, V.; Jailkhani, R. Oxidative stress in noninsulin-dependent diabetes mellitus (NIDDM) patients. Acta Diabetol. 2008, 45, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.C.; Wu, D.A.; Wang, J.H.; Yang, W.C.; Tseng, C.H. Association of C-reactive protein and hyperuricemia with diabetic nephropathy in Chinese type 2 diabetic patients. Acta Diabetol. 2009, 46, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Cheng, Y.; Wang, X.; Pan, Q.; Li, H.; Zhang, L.; Wang, Y. Association between microalbuminuria and cardiovascular disease in type 2 diabetes mellitus of the Beijing Han nationality. Acta Diabetol. 2012, 49, S65–S71. [Google Scholar] [CrossRef] [PubMed]
- Meigs, J.B.; Mittleman, M.A.; Nathan, D.M.; Tofler, G.H.; Singer, D.E.; Murphy-Sheehy, P.M.; Lipinska, I.; D’agostino, R.B.; Wilson, P.W. Hyperinsulinemia, hyperglycemia, and impaired hemostasis: The Framingham Offspring Study. JAMA 2000, 283, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Maloberti, A.; Giannattasio, C.; Dozio, D.; Betelli, M.; Villa, P.; Nava, S.; Cesana, F.; Facchetti, R.; Giupponi, L.; Castagna, F.; et al. Metabolic syndrome in human immunodeficiency virus-positive subjects: Prevalence, phenotype, and related alterations in arterial structure and function. Metab. Syndr. Relat. Disord. 2013, 11, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Maloberti, A.; Maggioni, S.; Occhi, L.; Triglione, N.; Panzeri, F.; Nava, S.; Signorini, S.; Falbo, R.; Casati, M.; Grassi, G.; et al. Sex-related relationships between uric acid and target organ damage in hypertension. J. Clin. Hypertens. 2018, 20, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Hansen, B.; Smith, S.C., Jr.; Cleeman, J.I.; Kahn, R.A.; American Heart Association; National Heart, Lung, and Blood Institute; American Diabetes Association. Clinical management of metabolic syndrome: Report of the American Heart Association/National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Circulation 2004, 109, 551–556. [Google Scholar] [CrossRef] [PubMed]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Lakka, H.M.; Laaksonen, D.E.; Lakka, T.A.; Niskanen, L.K.; Kumpusalo, E.; Tuomilehto, J.; Salonen, J.T. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2002, 288, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P. Ethnicity and cardiovascular risk: Variations in people of African ancestry and South Asian origin. J. Hum. Hypertens. 1997, 11, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Nagy, K.; Fiatal, S.; Sándor, J.; Ádány, R. Distinct Penetrance of Obesity-Associated Susceptibility Alleles in the Hungarian General and Roma Populations. Obes. Facts 2017, 10, 444–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginter, E.; Krajcovicova-Kudlackova, M.; Kacala, O.; Kovacic, V.; Valachovicova, M. Health status of Romanies (Gypsies) in the Slovak Republic and in the neighbouring countries. Bratisl. Lek. Listy 2001, 102, 479–484. [Google Scholar] [PubMed]
- Dolinska, S.; Kudlackova, M.; Ginter, E. The prevalence of female obesity in the world and in the Slovak Gypsy women. Bratisl. Lek. Listy 2007, 108, 207–211. [Google Scholar] [PubMed]
- Madarasová Gecková, A.; Jarčuška, P.; Mareková, M.; Pella, D.; Siegfried, L.; Jarčuška, P.; Halánová, M.; HepaMeta Team. HepaMeta—Prevalence of hepatitis B/C and metabolic syndrome in population living in separated and segregated Roma settlements: A methodology for a cross-sectional population based study using community-based approach. Cent. Eur. J. Public Health 2014, 22, S6–S11. [Google Scholar] [CrossRef]
- Gabrikova, D.; Bernasovska, J.; Sokolova, J.; Stiburkova, B. High frequency of SLC22A12 variants causing renal hypouricemia 1 in the Czech and Slovak Roma population; simple and rapid detection method by allele-specific polymerase chain reaction. Urolithiasis 2015, 43, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.; Japie, C.; Balahura, A.M.; Bartos, D.; Badila, E. Cardiovascular risk factors in a Roma sample population from Romania. Rom. J. Intern. Med. 2018, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Hidvégi, T.; Hetyesi, K.; Biró, L.; Nadas, J.; Jermendy, G. Screening for metabolic syndrome within a minority ethnic group (adult Gypsy people) in Hungary. Bratisl. Lek. Listy 2012, 113, 721–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kósa, Z.; Moravcsik-Kornyicki, Á.; Diószegi, J.; Roberts, B.; Szabó, Z.; Sándor, J.; Ádány, R. Prevalence of metabolic syndrome among Roma: A comparative health examination survey in Hungary. Eur. J. Public Health 2015, 25, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Vozarova de Courten, B.; de Courten, M.; Hanson, R.L.; Zahorakova, A.; Egyenes, H.P.; Tataranni, P.A.; Bennett, P.H.; Vozar, J. Higher prevalence of type 2 diabetes, metabolic syndrome and cardiovascular diseases in gypsies than in non-gypsies in Slovakia. Diabetes Res. Clin. Pract. 2003, 62, 95–103. [Google Scholar] [CrossRef]
- Ying, X.; Jiang, Y.; Qin, G.; Qian, Y.; Shen, X.; Jiang, Z.; Zheng, S.; Song, Z. Association of body mass index, waist circumference, and metabolic syndrome with serum cystatin C in a Chinese population. Medicine 2017, 96, e6289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walldius, G.; Jungner, I.; Holme, I.; Aastveit, A.H.; Kolar, W.; Steiner, E. High apolipoprotein B, 477 low apolipoprotein A–I, and improvement in the prediction of fatal myocardial infarction (AMORIS 478 study): A prospective study. Lancet 2001, 358, 2026–2033. [Google Scholar] [CrossRef]
- Lemieux, I.; Pascot, A.; Prud’homme, D.; Alméras, N.; Bogaty, P.; Nadeau, A.; Bergeron, J.; Després, J.P. Elevated C-reactive protein: Another component of the atherothrombotic profile of abdominal obesity. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.R.; Park, J.K.; Choi, W.J.; Cho, A.R.; Lee, Y.J. Serum ferritin level is positively associated with insulin resistance and metabolic syndrome in postmenopausal women: A nationwide population-based study. Maturitas 2017, 103, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; He, L.; Chen, Y.; Fang, Y.; Yao, Y. Association between serum ferritin levels and metabolic syndrome: An updated meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 13317–13322. [Google Scholar] [PubMed]
- Krcho, P.; Bazárová, J.; Diheneščíková, D. Composition of the mother milk during the first five 428 days in low and high risk population. Acta Med. Port. 2012, 25 (Suppl. 2), 163. [Google Scholar]
- Hales, C.N.; Barker, D.J. The thrifty phenotype hypothesis. Br. Med. Bull. 2001, 60, 5–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, Z.; Rasheed, K.; Kapusta, D.R.; Reisin, E. Potential role of uric acid in metabolic syndrome, hypertension, kidney injury, and cardiovascular diseases: Is it time for reappraisal? Curr. Hypertens. Rep. 2013, 15, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Caliceti, C.; Calabria, D.; Roda, A.; Cicero, A.F.G. Fructose intake, serum uric acid, and cardiometabolic disorders: A Critical Review. Nutrients 2017, 9, 395. [Google Scholar] [CrossRef] [PubMed]
- Reimann, M.; Schutte, A.E.; Malan, L.; Huisman, H.W.; Malan, N.T. Hyperuricaemia is an independent factor for the metabolic syndrome in a sub-Saharan African population: A factor analysis. Atherosclerosis 2008, 197, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Sui, X.; Church, T.S.; Meriwether, R.A.; Lobelo, F.; Blair, S.N. Uric acid and the development of metabolic syndrome in women and men. Metabolism 2008, 57, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Numata, T.; Miyatake, N.; Wada, J.; Makino, H. Comparison of serum uric acid levels between Japanese with and without metabolic syndrome. Diabetes Res. Clin. Pract. 2008, 80, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Clausen, J.O.; Borch-Johnsen, K.; Ibsen, H.; Pedersen, O. Analysis of the relationship between fasting serum uric acid and the insulin sensitivity index in a population-based sample of 380 young healthy Caucasians. Eur. J. Endocrinol. 1998, 138, 63–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conen, D.; Wietlisbach, V.; Bovet, P.; Shamlaye, C.; Riesen, W.; Paccaud, F.; Burnier, M. Prevalence of hyperuricemia and relation of serum uric acid with cardiovascular risk factors in a developing country. BMC Public Health 2004, 4, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schachter, M. Uric acid and hypertension. Curr. Pharm. Des. 2005, 11, 4139–4143. [Google Scholar] [CrossRef] [PubMed]
- Alper, A.B.; Chen, W.; Yau, L.; Srinivasan, S.R.; Berenson, G.S.; Hamm, L.L. Childhood uric acid predicts adult blood pressure—The Bogalusa Heart Study. Hypertension 2005, 45, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Cannon, P.J.; Stason, W.B.; Demartini, F.E.; Sommers, S.C.; Laragh, J.H. Hyperuricemia in primary and renal hypertension. N. Engl. J. Med. 1966, 275, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Masuo, K.; Kawaguchi, H.; Mikami, H.; Ogihara, T.; Tuck, M.L. Serum uric acid and plasma norepinephrine concentrations predict subsequent weight gain and blood pressure elevation. Hypertension 2003, 42, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Facchini, F.; Chen, Y.D.; Hollenbeck, C.B.; Reaven, G.M. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration. JAMA 1991, 266, 3008–3011. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Studied Variables | Roma | Non-Roma | p |
|---|---|---|---|
| Mean ± Standard Error of Mean or Absolute (Relative) Counts | Mean ± Standard Error of Mean or Absolute (Relative) Counts | ||
| Demographics | |||
| Age (in May 2011) | 34.67 ± 0.43 | 33.51 ± 0.37 | <0.043 |
| Male sex | 159(35.9) | 185(45.9) | 0.001 |
| Biochemistry | |||
| Glucose (mmol/L) | 4.84 ± 0.05 | 4.82 ± 0.030 | 0.7400 |
| Creatinine (umol) | 81.90 ± 0.53 | 84.95 ± 0.55 | <0.0001 |
| Uric acid (umol) | 226.54 ± 3.78 | 259.11 ± 4.22 | <0.0001 |
| Albumin (mg/L) | 46.60 ± 0.13 | 47.15 ± 0.15 | 0.0060 |
| AST (ukat/L) | 0.31 ± 0.02 | 0.33 ± 0.01 | <0.0001 |
| ALT (ukat/L) | 0.24 ± 0.02 | 0.25 ± 0.01 | 0.0040 |
| GMT (ukat/L) | 0.43 ± 0.04 | 0.48 ± 0.03 | <0.0001 |
| Cystatin C (mg/L) | 0.60 ± 0.01 | 0.59 ± 0.01 | 0.3470 |
| Cholesterol (mmol/L) | 4.77 ± 0.05 | 5.13 ± 0.05 | <0.0001 |
| Triglycerides (mmol/L) | 1.34 ± 0.05 | 1.24 ± 0.04 | 0.1090 |
| HDL (mmol/L) | 1.08 ± 0.01 | 1.31 ± 0.02 | <0.0001 |
| LDL (mmol/L) | 2.51 ± 0.03 | 2.64 ± 0.03 | 0.0060 |
| ApoA (mmol/L) | 1.52 ± 0.01 | 1.77 ± 0.02 | <0.0001 |
| ApoB100 (mmol/L) | 0.77 ± 0.01 | 0.77 ± 0.01 | 0.8790 |
| hs-CRP (mg/L) | 3.07 ± 0.19 | 1.98 ± 0.14 | <0.0001 |
| Fe (mmol/L) | 15.80 ± 0.32 | 18.56 ± 0.35 | <0.0001 |
| Ferritin (mg/L) | 209.33 ± 13.59 | 177.88 ± 10.45 | 0.0670 |
| Anthropometrics | |||
| BMI index | 26.57 ± 0.29 | 24.87 ± 0.22 | <0.0001 |
| WHR index | 0.87 ± 0.00 | 0.85 ± 0.02 | 0.359 |
| Systolic BP (mmHg) | 123 ± 1 | 122 ± 1 | 0.401 |
| Diastolic BP (mmHg) | 75 ± 1 | 76 ± 0 | 0.070 |
| Socioeconomics | |||
| Employed | 46(10.4) | 284(73.6) | <0.0001 |
| Poverty | 218(48.2) | 49(12.2) | <0.0001 |
| Smoking (any) | 266(59.8) | 110(28.2) | <0.0001 |
| Alcohol (any) | 75(17) | 64(16.5) | 0.844 |
| Education—elementary | 360(81.3) | 9(2.3) | p < 0.0001 |
| Education—apprenticeship | 73(16.5) | 84(21.4) | |
| Education—higher | 10(2.3) | 300(76.3) | |
| Physical activity (≥2/week) | 309(69.9) | 222(57.8) | <0.0001 |
| Imprisonment | 46(10.3) | 4(1.0) | <0.0001 |
| Studied Variables | Roma MetS+ | Roma MetS− | Non-Roma MetS+ | Non-Roma MetS− | p |
|---|---|---|---|---|---|
| Mean ± Standard Error of Mean | Mean ± Standard Error of Mean | Mean ± Standard Error of Mean | Mean ± Standard Error of Mean | ||
| Demographics | |||||
| Age (in May 2011) | 40.21 ± 0.67 | 32.31 ± 0.49 | 37.92 ± 0.76 | 32.37 ± 0.41 | <0.0001 |
| Male sex | 47(35.9) | 111(35.7) | 38(47.5) | 147(46.1) | 0.0200 |
| Biochemistry | |||||
| Glucose (mmol/L) | 5.40 ± 0.14 | 4.61 ± 0.03 | 5.16 ± 0.10 | 4.74 ± 0.03 | <0.0001 |
| Creatinine (umol) | 83.87 ± 1.07 | 81.23 ± 0.61 | 87.72 ± 1.69 | 84.30 ± 0.54 | <0.0001 |
| Uric acid (umol) | 251.61 ± 7.87 | 216.38 ± 4.16 | 303.64 ± 10.40 | 247.96 ± 4.40 | <0.0001 |
| Albumin (mg/L) | 46.22 ± 0.23 | 46.77 ± 0.16 | 46.56 ± 0.31 | 47.31 ± 0.17 | 0.0020 |
| AST (ukat/L) | 0.32 ± 0.03 | 0.30 ± 0.02 | 0.36 ± 0.04 | 0.32 ± 0.01 | <0.0001 |
| ALT (ukat/L) | 0.26 ± 0.02 | 0.23 ± 0.02 | 0.33 ± 0.03 | 0.23 ± 0.01 | <0.0001 |
| GMT (ukat/L) | 0.58 ± 0.07 | 0.37 ± 0.05 | 0.73 ± 0.10 | 0.42 ± 0.03 | <0.0001 |
| Cystatin C (mg/L) | 0.63 ± 0.01 | 0.59 ± 0.01 | 0.65 ± 0.02 | 0.58 ± 0.01 | 0.0010 |
| Cholesterol (mmol/L) | 5.14 ± 0.09 | 4.63 ± 0.05 | 5.60 ± 0.11 | 5.01 ± 0.05 | <0.0001 |
| Triglycerides (mmol/L) | 2.14 ± 0.12 | 1.01 ± 0.03 | 2.09 ± 0.13 | 1.03 ± 0.03 | <0.0001 |
| HDL (mmol/L) | 0.90 ± 0.02 | 1.16 ± 0.02 | 1.06 ± 0.02 | 1.38 ± 0.02 | <0.0001 |
| LDL (mmol/L) | 2.73 ± 0.06 | 2.42 ± 0.04 | 3.01 ± 0.08 | 2.55 ± 0.04 | <0.0001 |
| ApoA (mmol/L) | 1.42 ± 0.02 | 1.56 ± 0.02 | 1.63 ± 0.03 | 1.81 ± 0.02 | <0.0001 |
| ApoB100 (mmol/L) | 0.87 ± 0.02 | 0.72 ± 0.01 | 0.94 ± 0.03 | 0.73 ± 0.01 | <0.0001 |
| hsCRP (mg/L) | 5.20 ± 0.44 | 2.20 ± 0.18 | 3.40 ± 0.46 | 1.62 ± 0.13 | <0.0001 |
| Fe (mmol/L) | 14.23 ± 0.52 | 16.51 ± 0.39 | 18.17 ± 0.63 | 18.62 ± 0.40 | <0.0001 |
| Ferritin (mg/L) | 266.35 ± 25.20 | 187.70 ± 16.31 | 255.65 ± 32.68 | 158.84 ± 10.00 | <0.0001 |
| Anthropometrics | |||||
| BMI index | 31.61 ± 0.50 | 24.42 ± 0.27 | 29.58 ± 0.42 | 23.63 ± 0.21 | <0.0001 |
| WHR index | 0.92 ± 0.01 | 0.85 ± 0.00 | 0.90 ± 0.01 | 0.84 ± 0.03 | 0.0580 |
| Systolic BP (mmHg) | 136 ± 2 | 117 ± 1 | 132 ± 2 | 119 ± 1 | <0.0001 |
| Diastolic BP (mmHg) | 84 ± 1 | 71 ± 1 | 83 ± 1 | 74 ± 1 | <0.0001 |
| Socioeconomics | |||||
| Employed | 16(12.7) | 29(9.4) | 57(73.1) | 227(73.7) | <0.0001 |
| Poverty | 73(55.7) | 139(44.7) | 16(20) | 32(10) | <0.0001 |
| Smoking (any) | 74(57.8) | 184(59.7) | 25(31.6) | 85(27.4) | <0.0001 |
| Alcohol (any) | 19(15) | 55(18) | 15(19.5) | 48(15.5) | 0.7010 |
| Education—elementary | 103(81.1) | 250(81.4) | 3(3.8) | 6(1.9) | <0.0001 |
| Education—apprenticeship | 21(16.5) | 51(16.6) | 24(30) | 60(19.2) | |
| Education—higher | 3(2.4) | 6(2.0) | 53(66.3) | 246(78.8) | |
| Physical activity (≥2/week) | 93(73.2) | 211(69) | 45(57.7) | 177(58.0) | 0.0030 |
| Imprisonment | 12(9.4) | 33(10.7) | 2(2.5) | 2(0.6) | <0.0001 |
| Socio-Economic Variables | Roma | p | Non-Roma | p | |
|---|---|---|---|---|---|
| Mean ± SEM | Mean ± SEM | ||||
| Poverty | No | 219 ± 5.2 | 0.065 | 260 ± 4.5 | 0.564 |
| Yes | 233 ± 5.5 | 252 ± 12.8 | |||
| Alcohol intake | Less than once a month, or never | 222 ± 4.2 | 0.052 | 254 ± 4.5 | 0.007 |
| Once in a month, week, or daily | 241 ± 9.1 | 291 ± 12.7 | |||
| Education | Elementary | 223 ± 4.1 | 0.204 | 280.5 ± 13.4 | 0.691 |
| Apprenticeship | 239 ± 10.4 | 263 ± 9.9 | |||
| Higher | 247 ± 25.5 | 258 ± 4.9 | |||
| Smoking | No | 233 ± 6.3 | 0.105 | 258 ± 5 | 0.428 |
| Yes | 220 ± 4.7 | 263 ± 8.4 | |||
| Physical activity | Once a week or less | 225 ± 4.4 | 0.983 | 261 ± 5.6 | 0.858 |
| 2–3 times a week or more | 225 ± 7.1 | 260 ± 6.9 | |||
| Employed | No | 226 ± 3.9 | 0.489 | 255 ± 9.0 | 0.464 |
| Yes | 217 ± 12.5 | 262 ± 4.9 | |||
| Imprisoned previously | No | 221 ± 3.9 | 0.013 | 260 ± 28.7 | 0.974 |
| Yes | 259±14 | 260 ± 4.3 | |||
| Biochemical Parameters | Roma | Non-Roma | ||
|---|---|---|---|---|
| Corr Coeff | p | Corr Coeff | p | |
| Glucose (mmol/L) | 0.159 | <0.0001 | 0.169 | <0.0001 |
| Creatinine (umol) | 0.391 | <0.0001 | 0.532 | <0.0001 |
| Albumin (mg/L) | 0.203 | <0.0001 | 0.128 | 0.0110 |
| AST (ukat/L) | 0.118 | 0.0130 | 0.245 | <0.0001 |
| ALT (ukat/L) | 0.087 | 0.066 | 0.312 | <0.0001 |
| GMT (ukat/L) | 0.122 | 0.010 | 0.307 | <0.0001 |
| Cystatin C (mg/L) | 0.162 | <0.0001 | 0.226 | <0.0001 |
| Cholesterol (mmol/L) | 0.111 | 0.019 | 0.183 | <0.0001 |
| Triglycerides (mmol/L) | 0.317 | <0.0001 | 0.284 | <0.0001 |
| HDL (mmol/L) | −0.211 | <0.0001 | −0.222 | <0.0001 |
| LDL (mmol/L) | 0.104 | 0.0290 | 0.220 | <0.0001 |
| ApoA (mmol/L) | −0.179 | <0.0001 | −0.223 | <0.0001 |
| ApoB100 (mmol/L) | 0.125 | 0.0080 | 0.208 | <0.0001 |
| hsCRP (mg/L) | 0.259 | <0.0001 | 0.167 | <0.0001 |
| Fe (mmol/L) | 0.123 | 0.0090 | 0.086 | 0.0860 |
| Ferritin (mg/L) | 0.349 | <0.0001 | 0.422 | <0.0001 |
| MetS Criteria | Roma | nonRoma | |||
|---|---|---|---|---|---|
| Mean ± SEM | p | Mean ± SEM | p | ||
| Glucose criterium | No | 223 ± 3.9 | 256 ± 4.3 | ||
| Yes | 261 ± 12.0 | 0.0020 | 298 ± 16.5 | 0.0080 | |
| Low HDL criterium | No | 221 ± 7.0 | 254 ± 5.0 | ||
| Yes | 228 ± 4.5 | 0.3300 | 269 ± 7.7 | 0.0730 | |
| Obesity criterium | No | 210 ± 5.4 | 243 ± 77.7 | ||
| Yes | 239 ± 5.2 | <0.0001 | 280 ± 6.7 | <0.0001 | |
| TG criterium | No | 216 ± 3.9 | 247 ± 4.3 | ||
| Yes | 260 ± 9.2 | <0.0001 | 308.8 ± 10.8 | <0.0001 | |
| BP criterium | No | 217 ± 4.5 | 245 ± 4.9 | ||
| Yes | 251 ± 7.1 | <0.0001 | 290 ± 7.7 | <0.0001 | |
| Variables with Significant Difference between MetS and without MetS | Sig. | Exp(B) | 95% CI for EXP(B) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Uric Acid (umol) | 0.005 | 1.004 | 1.001 | 1.007 |
| Age (years) | <0.0001 | 1.095 | 1.067 | 1.124 |
| Female sex | 0.001 | 0.406 | 0.242 | 0.682 |
| GMT (ukat/L) | 0.007 | 1.450 | 1.108 | 1.897 |
| hsCRP (mg/L) | <0.0001 | 1.151 | 1.086 | 1.219 |
| Fe (mmol/L) | 0.419 | 0.987 | 0.956 | 1.019 |
| Ferritin (mg/L) | 0.327 | 1.000 | 1.000 | 1.001 |
| Roma ethnicity | 0.261 | 0.758 | 0.468 | 1.228 |
| Cholesterol (mmol/L) | <0.0001 | 1.759 | 1.410 | 2.194 |
| Apolipoprotein A | <0.0001 | 0.048 | 0.021 | 0.107 |
| Poverty | 0.053 | 1.535 | 0.995 | 2.367 |
| Constant | <0.0001 | 0.031 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrikova, J.; Janicko, M.; Fedacko, J.; Drazilova, S.; Madarasova Geckova, A.; Marekova, M.; Pella, D.; Jarcuska, P. Serum Uric Acid in Roma and Non-Roma—Its Correlation with Metabolic Syndrome and Other Variables. Int. J. Environ. Res. Public Health 2018, 15, 1412. https://doi.org/10.3390/ijerph15071412
Petrikova J, Janicko M, Fedacko J, Drazilova S, Madarasova Geckova A, Marekova M, Pella D, Jarcuska P. Serum Uric Acid in Roma and Non-Roma—Its Correlation with Metabolic Syndrome and Other Variables. International Journal of Environmental Research and Public Health. 2018; 15(7):1412. https://doi.org/10.3390/ijerph15071412
Chicago/Turabian StylePetrikova, Jana, Martin Janicko, Jan Fedacko, Sylvia Drazilova, Andrea Madarasova Geckova, Maria Marekova, Daniel Pella, and Peter Jarcuska. 2018. "Serum Uric Acid in Roma and Non-Roma—Its Correlation with Metabolic Syndrome and Other Variables" International Journal of Environmental Research and Public Health 15, no. 7: 1412. https://doi.org/10.3390/ijerph15071412
APA StylePetrikova, J., Janicko, M., Fedacko, J., Drazilova, S., Madarasova Geckova, A., Marekova, M., Pella, D., & Jarcuska, P. (2018). Serum Uric Acid in Roma and Non-Roma—Its Correlation with Metabolic Syndrome and Other Variables. International Journal of Environmental Research and Public Health, 15(7), 1412. https://doi.org/10.3390/ijerph15071412