Use of Meditation and Cognitive Behavioral Therapies for the Treatment of Stress, Depression and Anxiety in Students. A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
- How many interventions have been conducted with students from 2007 to 2018? What kind of meditation programs and/or cognitive-behavioral therapy has been used?
- What effect do different interventions have on the treatment of stress, anxiety, and depression?
- What treatment factors influence students’ stress, anxiety, and depression?
2. Materials and Methods
2.1. Search Strategy
2.2. Population and Literary Sample
2.3. Coding of Articles
2.4. Effect Size Index
2.5. Analysis of Meta-Analysis Data
2.6. Evaluation of the Methodological Quality of the Primary Studies
3. Results
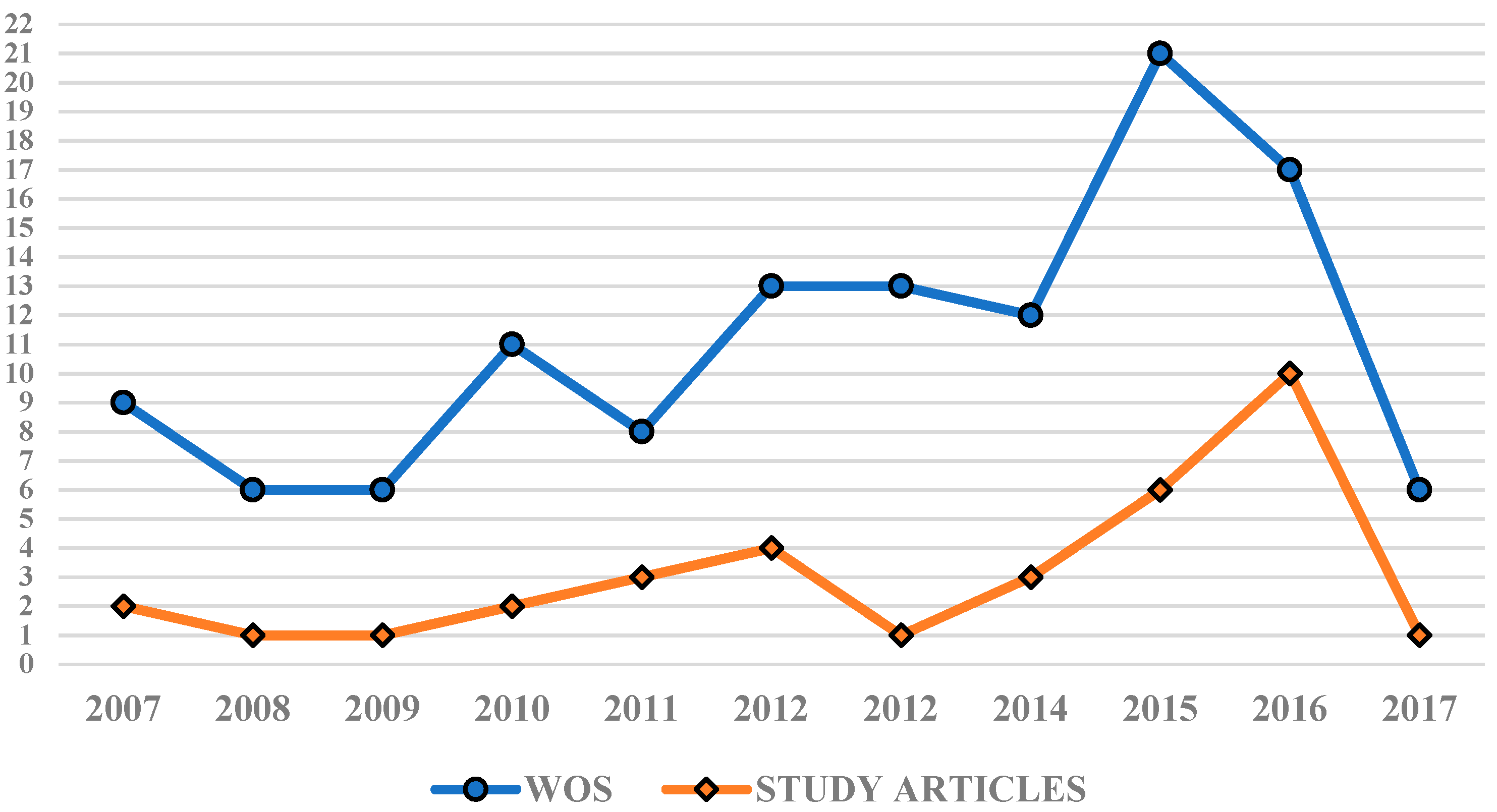
3.1. Evolution of Scientific Production
3.2. Results Generated by Study Interventions Targeting Stress
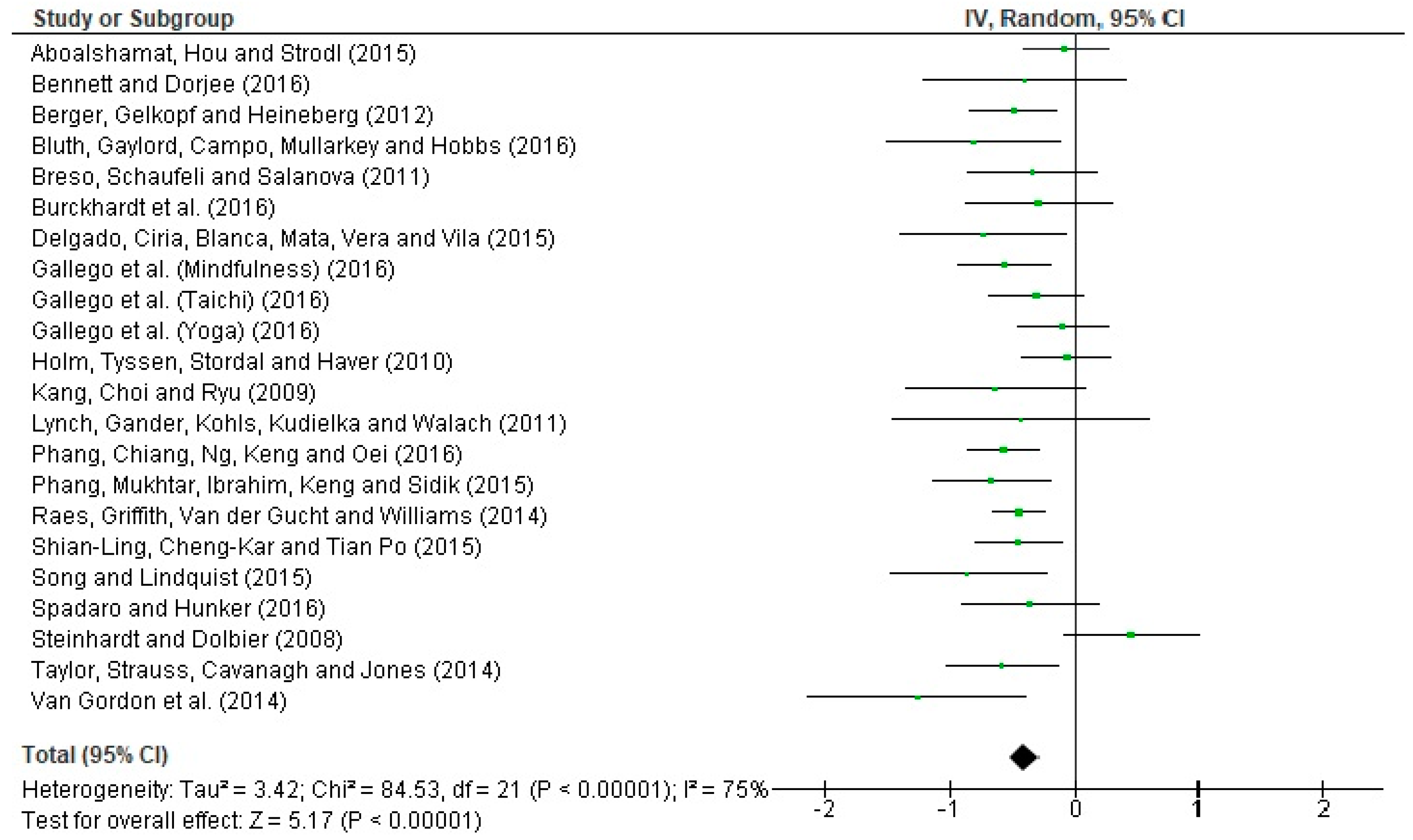
3.2.1. Study Results According to the Stress Treatment
3.2.2. Moderation Analysis
3.2.3. Control of Publication Bias.
3.3. Results Generated by the Interventions of the Study of Anxiety
3.3.1. Study Results Relating to Anxiety Treatment
3.3.2. Moderation Analysis
3.3.3. Control of Publication Bias
3.4. Results Generated by Intervention Studies for Depression
3.4.1. Study Results of Depression Interventions
3.4.2. Moderation Analysis
3.4.3. Control of Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lo, K.; Waterland, J.; Todd, P.; Gupta, T.; Bearman, M.; Hassed, C.; Keating, J. Group interventions to promote mental health in health professional education: A systematic review and meta-analysis of randomised controlled trials. Adv. Health Sci. Educ. 2017, 23, 1–35. [Google Scholar] [CrossRef]
- Werner, A.; Perry, Y.; Calear, A.; Newby, J.; Christensen, H. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 51, 30–47. [Google Scholar] [CrossRef] [Green Version]
- North, C.; Pfefferbaum, B. Mental health response to community disasters: A systematic review. J. Am. Med. Assoc. 2013, 310, 507–518. [Google Scholar] [CrossRef]
- Pozo, C.; Bretones, B.; Martos, J.; Cid, N.; Alonso, E. Well-being in university students: Flourishing and engagement as strategies against academic stress. Psychol. Health 2013, 28, 293. [Google Scholar]
- Álvarez, J.; Aguilar, J.; Lorenzo, J. La ansiedad ante los exámenes en estudiantes universitarios: Relaciones con variables personales y académicas. Electr. J. Res. Educ. Psychol. 2012, 10, 333–354. [Google Scholar]
- Saxena, S.; Funk, M.; Chisholm, D. World health assembly adopts comprehensive mental health action plan 2013–2020. Lancet 2013, 381, 1970–1971. [Google Scholar] [CrossRef]
- OMS. Draft Comprehensive Mental Health Action Plan 2013–2020; WHO: Ginebra, Switzerland, 2013. [Google Scholar]
- Schönfeld, P.; Brailovskaia, J.; Bieda, A.; Zhang, X.; Margraf, J. The effects of daily stress on positive and negative mental health: Mediation through self-efficacy. Int. J. Clin. Health Psychol. 2016, 16, 1–10. [Google Scholar] [CrossRef]
- Ando, M. An intervention program focused on self-understanding and interpersonal interactions to prevent psychosocial distress among Japanese university students. J. Adolesc. 2011, 34, 929–940. [Google Scholar] [CrossRef]
- Fida, R.; Paciello, M.; Tramontano, C.; Fontaine, R.; Barbaranelli, C.; Farnese, M. An integrative approach to understanding counterproductive work behavior: The roles of stressors, negative emotions, and moral disengagement. J. Bus. Ethics 2015, 130, 131–144. [Google Scholar] [CrossRef]
- Piccolo, L.; Giacomoni, C.; Julio-Costa, A.; Oliveira, S.; Zbornik, J.; Haase, V.; Salles, J. Reading anxiety in L1: Reviewing the concept. Early Child. Educ. J. 2017, 45, 537–543. [Google Scholar] [CrossRef]
- Torrano, R.; Ortigosa, J.; Riquelme, A.; López, J. Assessment of test anxiety in compulsory secondary education students. Revista de Psicologia Clinica Con Ninos y Adolescentes 2017, 4, 103–110. [Google Scholar]
- Shin, L.; Liberzon, I. The neurocircuitry of fear, stress, and anxiety disorders. Focus 2011, 9, 311–334. [Google Scholar] [CrossRef]
- Saxena, S. Dialogues between neurscience and society. In Global Mental Health and Neuroscience: Challenges and Oportunities; Society for Neurosciences: San Diego, CA, USA, 2016. [Google Scholar]
- King, K.; Strunk, C.; Sorter, M. Preliminary effectiveness of surviving the Teens® Suicide Prevention and Depression Awareness Program on adolescents’ suicidality and self-efficacy in performing help-seeking behaviors. J. Sch. Health 2011, 81, 581–590. [Google Scholar] [CrossRef]
- Townsend, L.; Musci, R.; Stuart, E.; Ruble, A.; Beaudry, M.; Schweizer, B.; Wilcox, H. The association of school climate, depression literacy, and mental health stigma among high school students. J. Sch. Health 2017, 87, 567–574. [Google Scholar] [CrossRef]
- Harring, H.; Montgomery, K.; Hardin, J. Perceptions of body weight, weight management strategies, and depressive symptoms among US college students. J. Am. Coll. Health 2010, 59, 43–50. [Google Scholar] [CrossRef]
- Raes, F.; Griffith, J.; Van der Gucht, K.; Williams, J. School-based prevention and reduction of depression in adolescents: A cluster-randomized controlled trial of a mindfulness group program. Mindfulness 2014, 5, 477–486. [Google Scholar] [CrossRef]
- Bennett, K.; Dorjee, D. The impact of a Mindfulness-Based Stress Reduction course (MBSR) on well-being and academic attainment of sixth-form students. Mindfulness 2016, 7, 105–114. [Google Scholar] [CrossRef]
- Song, Y.; Lindquist, R. Effects of mindfulness-based stress reduction on depression, anxiety, stress and mindfulness in Korean nursing students. Nurse Educ. Today 2015, 35, 86–90. [Google Scholar] [CrossRef]
- Dvorakova, K.; Kishida, M.; Li, J.; Elavsky, S.; Broderick, P.; Agrusti, M.; Greenberg, M. Promoting healthy transition to college through mindfulness training with first-year college students: Pilot randomized controlled trial. J. Am. Coll. Health 2017, 65, 259–267. [Google Scholar] [CrossRef]
- Johnson, C.; Burke, C.; Brinkman, S.; Wade, T. Effectiveness of a school-based mindfulness program for transdiagnostic prevention in young adolescents. Behav. Res. Ther. 2016, 81, 1–11. [Google Scholar] [CrossRef]
- Taylor, B.; Strauss, C.; Cavanagh, K.; Jones, F. The effectiveness of self-help mindfulness-based cognitive therapy in a student sample: A randomised controlled trial. Behav. Res. Ther. 2014, 63, 63–69. [Google Scholar] [CrossRef]
- Singh, N.; Lancioni, G.; Karazsia, B.; Felver, J.; Myers, R.; Nugent, K. Effects of samatha meditation on active academic engagement and math performance of students with attention deficit/hyperactivity disorder. Mindfulness 2016, 7, 68–75. [Google Scholar] [CrossRef]
- Dick, A.; Niles, B.; Street, A.; Di Martino, D.; Mitchell, K. Examining mechanisms of change in a yoga intervention for women: The influence of mindfulness, psychological flexibility, and emotion regulation on PTSD symptoms. J. Clin. Psychol. 2014, 70, 1170–1182. [Google Scholar] [CrossRef]
- Yeh, G.; Wang, C.; Wayne, P.; Phillips, R. The effect of tai chi exercise on blood pressure: A systematic review. Prev. Cardiol. 2008, 11, 82–89. [Google Scholar] [CrossRef]
- Hutton, B.; Catalá-López, F.; Moher, D. La extensión de la declaración PRISMA para revisiones sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clín. 2016, 147, 262–266. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.; Ioannidis, J.P.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, 1–28. [Google Scholar] [CrossRef]
- Fleiss, J. Measuring nominal scale agreement among many raters. Psychol. Bull. 1971, 76, 378–382. [Google Scholar] [CrossRef]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.; Koch, G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Hedges, L.; Shymansky, J.; Woodworth, G. Modern Methods of Meta-Analysis; National Science Teachers Association: Washington, DC, USA, 1989. [Google Scholar]
- Orwin, R. A fail-safe N for effect size in meta-analysis. J. Educ. Stat. 1983, 8, 157–159. [Google Scholar] [CrossRef]
- Rosenthal, R. The «file drawer problem» and tolerance for null results. Psychol. Bull. 1979, 86, 638–641. [Google Scholar] [CrossRef]
- Botella-Ausina, J.; Sánchez-Meca, J. Meta-Análisis en Ciencias Sociales y de la Salud; Editorial Síntesis: Madrid, Spain, 2015. [Google Scholar]
- Aboalshamat, K.; Hou, X.; Strodl, E. The impact of a self-development coaching programme on medical and dental students’ psychological health and academic performance: A randomised controlled trial. BMC Med. Educ. 2015, 15, 1–13. [Google Scholar] [CrossRef]
- Berger, R.; Gelkopf, M.; Heineberg, Y. A teacher-delivered intervention for adolescents exposed to ongoing and intense traumatic war-related stress: A quasi-randomized controlled study. J. Adolesc. Health 2012, 51, 453–461. [Google Scholar] [CrossRef]
- Bluth, K.; Gaylord, S.; Campo, R.; Mullarkey, M.; Hobbs, L. Making friends with yourself: A mixed methods pilot study of a mindful self-compassion program for adolescents. Mindfulness 2016, 7, 479–492. [Google Scholar] [CrossRef]
- Breso, E.; Schaufeli, W.; Salanova, M. Can a self-efficacy-based intervention decrease burnout, increase engagement, and enhance performance? A quasi-experimental study. High. Educ. 2011, 61, 339–355. [Google Scholar] [CrossRef]
- Burckhardt, R.; Manicavasagar, V.; Batterham, P.; Hadzi-Pavlovic, D. A randomized controlled trial of strong minds: A school-based mental health program combining acceptance and commitment therapy and positive psychology. J. Sch. Psychol. 2016, 57, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Delgado, L.; Ciria, L.; Blanca, B.; Mata, J.; Vera, M.; Vila, J. Dissociation between the cognitive and interoceptive components of mindfulness in the treatment of chronic worry. J. Behav. Ther. Exp. Psychiatry 2015, 48, 192–199. [Google Scholar] [CrossRef]
- Gallego, J.; Aguilar, J.; Cangas, A.; Rosado, A.; Langer, A. Effect of mind/body interventions on levels of anxiety, stress and depression among future primary school teacher: A controlled study. Revista de Psicodidáctica 2016, 21, 87–101. [Google Scholar] [CrossRef]
- Holm, M.; Tyssen, R.; Stordal, K.; Haver, B. Self-development groups reduce medical school stress: A controlled intervention study. BMC Med. Educ. 2010, 10, 8. [Google Scholar] [CrossRef]
- Kang, Y.; Choi, S.; Ryu, E. The effectiveness of a stress coping program based on mindfulness meditation on the stress, anxiety, and depression experienced by nursing students in Korea. Nurse Educ. Today 2009, 29, 538–543. [Google Scholar] [CrossRef]
- Lynch, S.; Gander, M.; Kohls, N.; Kudielka, B.; Walach, H. Mindfulness-based coping with university life: A non-randomized wait-list-controlled pilot evaluation. Stress Health 2011, 27, 365–375. [Google Scholar] [CrossRef]
- Phang, C.; Mukhtar, F.; Ibrahim, N.; Keng, S.; Sidik, S. Effects of a brief mindfulness-based intervention program for stress management among medical students: The Mindful-Gym randomized controlled study. Adv. Health Sci. Educ. 2015, 20, 1115–1134. [Google Scholar] [CrossRef]
- Phang, C.; Chiang, K.; Ng, L.; Keng, S.; Oei, T. Effects of brief group mindfulness-based cognitive therapy for stress reduction among medical students in a malaysian university. Mindfulness 2016, 7, 189–197. [Google Scholar] [CrossRef]
- Shian-Ling, K.; Cheng-Kar, P.; Tian Po, O. Effects of a brief mindfulness-based intervention program on psychological symptoms and well-being among medical students in malaysia: A controlled study. Int. J. Cogn. Ther. 2015, 8, 335–350. [Google Scholar]
- Spadaro, K.; Hunker, D. Exploring the effects of an online asynchronous mindfulness meditation intervention with nursing students On Stress, mood, And Cognition: A descriptive study. Nurse Educ. Today 2016, 39, 163–169. [Google Scholar] [CrossRef]
- Steinhardt, M.; Dolbier, C. Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. J. Am. Coll. Health 2008, 56, 445–453. [Google Scholar] [CrossRef]
- Van Gordon, W.; Shonin, E.; Sumich, A.; Sundin, E.; Griffiths, M. Meditation Awareness Training (MAT) for psychological well-being in a sub-clinical sample of university students: A controlled pilot study. Mindfulness 2014, 5, 381–391. [Google Scholar] [CrossRef]
- Bradley, R.; McCraty, R.; Atkinson, M.; Tomasino, D.; Daugherty, A.; Arguelles, L. Emotion self-regulation, psychophysiological coherence, and test anxiety: Results from an experiment using electrophysiological measures. Appl. Psychophysiol. Biofeedback 2010, 35, 261–283. [Google Scholar] [CrossRef]
- Brennan, J.; McGrady, A.; Lynch, D.; Schaefer, P.; Whearty, K. A stress management program for higher risk medical students: Preliminary findings. Appl. Psychophysiol. Biofeedback 2016, 41, 301–305. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, X.; Wang, L.; Zhang, X. A randomized controlled trial of the effects of brief mindfulness meditation on anxiety symptoms and systolic blood pressure in Chinese nursing students. Nurse Educ. Today 2013, 33, 1166–1172. [Google Scholar] [CrossRef]
- McGrady, A.; Brennan, J.; Lynch, D.; Whearty, K. A wellness program for first year medical students. Appl. Psychophysiol. Biofeedback 2012, 37, 253–260. [Google Scholar] [CrossRef]
- Ricarte, J.; Ros, L.; Latorre, J.; Beltran, M. Mindfulness-based intervention in a rural primary school: Effects on attention, concentration and mood. Int. J. Cogn. Ther. 2015, 8, 258–270. [Google Scholar] [CrossRef]
- Ruiz-Aranda, D.; Salguero, J.; Cabello, R.; Palomera, R.; Fernández-Berrocal, P. Can an emotional intelligence program improve adolescents’ psychosocial adjustment? Results from the intemo project. Soc. Behav. Pers. 2012, 40, 1373–1379. [Google Scholar] [CrossRef]
- Shearer, A.; Hunt, M.; Chowdhury, M.; Nicol, L. Effects of a brief mindfulness meditation intervention on student stress and heart rate variability. Int. J. Stress Manag. 2016, 23, 232–254. [Google Scholar] [CrossRef]
- Spahn, C.; Walther, J.; Nusseck, M. The effectiveness of a multimodal concept of audition training for music students in coping with music performance anxiety. Psychol. Music 2016, 44, 893–909. [Google Scholar] [CrossRef]
- Huedo, T.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistics or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef]
- Jain, S.; Shapiro, S.; Swanick, S.; Roesch, S.; Mills, P.; Bell, I.; Schwartz, G. A randomized controlled trial of mindfulness meditation versus relaxation training: Effects on distress, positive states of mind, rumination, and distraction. Ann. Behav. Med. 2007, 33, 11–21. [Google Scholar] [CrossRef]
- Roberts-Wolfe, D.; Sacchet, M.; Hastings, E.; Roth, H.; Britton, W. Mindfulness training alters emotional memory recall compared to active controls: Support for an emotional information processing model of mindfulness. Front. Hum. Neurosci. 2012, 6, 13–25. [Google Scholar] [CrossRef]
- Zenner, C.; Herrnleben, S.; Walach, H. Mindfulness based interventions in schools—A systematic review and meta-analysis. Front. Psychol. 2014, 5, 603–623. [Google Scholar] [CrossRef]
- Guillaumie, L.; Boiral, O.; Champagne, J. A mixed-methods systematic review of the effects of mindfulness on nurses. J. Adv. Nurs. 2017, 73, 1017–1034. [Google Scholar] [CrossRef]
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disord. 2013, 148, 1–11. [Google Scholar] [CrossRef]
- Meiklejohn, J.; Phillips, C.; Freedman, M.; Griffiths, M.; Biegel, G.; Roach, A.; Saltzman, A. Integrating mindfulness training into K-12 education: Fostering the resilience of teachers and students. Mindfulness 2012, 3, 291–307. [Google Scholar] [CrossRef]
- Oriol-Granado, X.; Mendoza-Lira, M.; Covarrubias-Apablaza, C.; Molina-López, V. Positive emotions, autonomy support and academic performance of university students: The mediating role of academic engagement and self-efficacy. Revista de Psicodidáctica 2017, 22, 45–53. [Google Scholar] [CrossRef]
- Jordans, M.; Tol, W.; Komproe, I.; De Jong, J. Systematic review of evidence and treatment approaches: Psychosocial and mental health care for children in war. Child Adolesc. Ment. Health 2009, 14, 2–14. [Google Scholar] [CrossRef]
- Montero-Cobo, J.L.; Polaino-Rodríguez, C.; Puertas-Molero, P.; González-Valero, G. Design of a diagnosis of needs for adolescent students: Physical Education as an action resource. Educ. Sport Health Phys. Act. 2018, 2, 105–123. [Google Scholar]
- Berger, R.; Pat-Horenczyk, R.; Gelkopf, M. School-based intervention for prevention and treatment of elementary-students’ terror-related distress in Israel: A quasi-randomized controlled trial. J. Trauma. Stress 2007, 20, 541–551. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/s (Year) | Country | Educational Stage (Range or Average Age) *1 | Sample (EG-CG) *2 | Study Type | Intervention Strategy *3 | Instrument *4 | Effect Size (d) | 95% CI |
|---|---|---|---|---|---|---|---|---|
| Aboalshamat, Hou, and Strodl (2015) [37] | Saudi Arabia | UE (20–22) | 130 (65-65) | Quasi-experimental (6 weeks) | Self-development programme (HBUSS) | DASS-21 | −0.066 | [−0.410, 0.277] |
| Bennett and Dorjee (2016) [19] | Wales | SE (16–18) | 24 (11-13) | Quasi-experimental (8 weeks) | MBSR | DASS-21 | −0.402 | [−1.213, 0.408] |
| Berger, Gelkopf, and Heineberg (2012) [38] | Israel | SE (12.8 ± 1.0) | 154 (107-47) | Quasi-experimental (16 sessions) | EES | DSM IV | −0.480 | [−0.830, −0.142] |
| Bluth, Gaylord, Campo, Mullarkey, and Hobbs (2016) [39] | USA | SE (14–17) | 34 (16-18) | Quasi-experimental (6 weeks) | MFY | PSS | −0.823 | [−1.524, −0.122] |
| Breso, Schaufeli, Salanova (2011) [40] | Spain | UE (18–26) | 71 (21-50) | Quasi-experimental (4 sessions) | CBT | MBI-SS | −0.330 | [−0.842, 0.182] |
| Burckhardt, Manicavasagar, Batterham, Hadzi-Pavlovic (2016) [41] | Australia | SE (15–18) | 46 (24-22) | Quasi-experimental (12 weeks) | Strong Minds Condition (mindfulness) | DASS-21 | −0.290 | [−0.872, 0.291] |
| Delgado, Ciria, Blanca, Mata, Vera, and Vila (2015) [42] | Spain | UE (21.5 ± 3.94) | 41 (27-14) | Quasi-experimental (3 weeks) | MBSR | PSS | −0.745 | [−1.410, −0.08] |
| Gallego, Aguilar, Cangas, Rosado, and Langer (2016) [43] | Spain | UE (18–49) | 282 (237-45) | Quasi-experimental (16 sessions) | Mindfulness (MBCT) | DASS-21 | −0.561 | [−0.929, −0.192] |
| Yoga | −0.094 | [−0.456, 0.266] | ||||||
| Tai Chi | −0.301 | [−0.680, 0.076] | ||||||
| Holm, Tyssen, Stordal, and Haver (2010) [44] | Norway | UE (23.6 ± 3.4) | 140 (47-93) | Quasi-experimental (12 sessions/12 weeks) | Self-development and discussion groups | PMSS | −0.061 | [−0.412, 0.288] |
| Kang, Choi, and Ryu (2009) [45] | South Korea | UE (22.47 ± 1.17) | 32 (16-16) | Quasi-experimental (8 sessions) | MBSR | PWI-SF | −0.642 | [−1.353, 0.068] |
| Lynch, Gander, Kohls, Kudielka, and Walach (2011) [46] | England | UE (19–46) | 16 (10-6) | Quasi-experimental (8 sessions) | MBCUL (MBCT/MBSR) | PSS | −0.448 | [−1.472, 0.575] |
| Phang, Mukhtar, Ibrahim, Keng, and Sidik (2015) [47] | Malaysia | UE (21.04 ± 1.13) | 75 (37-38) | Quasi-experimental (5 weeks) | MBSM (MBCT/MBSR) | PSS | −0.669 | [−1.135, −0.204] |
| Phang, Chiang, Ng, Keng, and Oei (2016) [48] | Malaysia | UE (21–25) | 104 | Pre-experimental (4 weeks) | Mindful-Gym (MBCT/MBSR) | PSS | −0.567 | [−0.844, −0.290] |
| Raes et al. (2014) [18] | Belgium | SE (13–20) | 357 (182-175) | Quasi-experimental (8 weeks) | MBCT | DASS-21 | −0.443 | [−0.653, −0.233] |
| Shian-Ling, Cheng-Kar, and Tian Po (2015) [49] | Malaysia | UE (21–24) | 134 (77-57) | Quasi-experimental (4 weeks) | Mindful-Gym | PSS | −0.174 | [−0.517, 0.168] |
| Song and Lindquist (2015) [20] | South Korea | UE (19.6 ± 1.7) | 44 (21-23) | Quasi-experimental (10 weeks) | MBSR | DASS-21 | −0.866 | [−1.484, −0.247] |
| Spadaro and Hunker (2016) [50] | USA | UE (18–25) | 26 | Pre-experimental (8 weeks) | MBSR | PSS | −0.352 | [−0.9, 0.195] |
| Steinhardt and Dolbier (2008) [51] | USA | UE (18–53) | 57 (30-27) | Quasi-experimental (4 weeks) | Transforming Lives Resilience Education | CD–RISC | 0.467 | [−0.06, 0.993] |
| Taylor et al. (2014) [23] | England | UE (28.61 ± 9.12) | 79 (40-39) | Quasi-experimental (8 weeks) | MBCT-SH | DASS-21 | −0.576 | [−1.026, −0.126] |
| Van Gordon, Shonin, Sumich, Sundin, and Griffiths (2014) [52] | England | UE (20–42) | 25 (14-11) | Quasi-experimental (8 weeks) | MAT | DASS-21 | −1.297 | [−2.165, −0.429] |
| Study Groups | K * | M * | CI to 95% | p * |
|---|---|---|---|---|
| According treatment duration | ||||
| Short duration (0–4 weeks) | 5 | −0.33 | [−0.68, 0.01] | 0.26 |
| Medium duration (from 5 to 8 weeks) | 10 | −0.46 | [−0.62, −0.30] | |
| Long duration (more than 9 weeks) | 5 | −0.34 | [−0.52, −0.15] | |
| According the educational stage of students receiving treatment | ||||
| Secondary Education | 5 | −0.46 | [−0.62, −0.29] | 0.52 |
| University | 15 | −0.38 | [−0.53, −0.23] | |
| According to intervention strategy | ||||
| Cognitive-behavioral programs | 5 | −0.12 | [−0.40, 0.16] | 0.004 * |
| Programs based on mindfulness | 15 | −0.53 | [−0.64, −0.42] | |
| Body therapy programs (Yoga-Tai Chi) | 2 | −0.19 | [−0.45, 0.07] | |
| Author/s (Year) | Country | Educational Stage (Range or Average Age)*1 | Sample (EG-CG)*2 | Study Type | Intervention strategy*3 | Instrument*4 | Effect Size (d) | 95% CI |
|---|---|---|---|---|---|---|---|---|
| Aboalshamat, Hou, and Strodl (2015) [37] | Saudi Arabia | UE (20–22) | 130 (65-65) | Quasi-experimental (6 weeks) | Self-development program (HBUSS) | DASS-21 | −0.122 | [−0.466, 0.222] |
| Ando (2011) [9] | Japan | UE (19.1 ± 1.5) | 191 (157-34) | Quasi-experimental (11 sessions/11 weeks) | Successful Self Program | Profile of Mood Status | −0.124 | [−0.495, 0.246] |
| Bennett and Dorjee (2016) [19] | Wales | SE (16–18) | 24 (11-13) | Quasi-experimental (8 weeks) | MBSR | DASS-21 | 0.111 | [−0.692, 0.914] |
| Berger, Pat-Horenczyk, and Gelkopf (2007) [38] | Israel | PE (7–11) | 142 (70-72) | Quasi-experimental (8 sessions) | OTT manual | SCARED | −0.957 | [−1.304, −0.61] |
| Bluth, Gaylord, Campo, Mullarkey, and Hobbs (2016) [39] | USA | SE (14–17) | 34 (16-18) | Quasi-experimental (6 weeks) | MFY | STAI | −0.664 | [−1.356, 0.027] |
| Bradley, McCraty, Atkinson, Tomasino, Daugherty, and Arguelles (2010) [53] | USA | SE (15.3 ± 0.45) | 48 (27-21) | Quasi-experimental (12 weeks) | Test Edge | TAI | −0.835 | [−1.429, −0.241] |
| Brennan, McGrady, Lynch, Schaefer, Whearty (2016) [54] | USA | UE (23.3 ± 2.3) | 42 | Pre-experimental (4 sessions per semester) | Stress management and relaxation strategy | BAI | −0.549 | [−0.985, −0.114] |
| Burckhardt, Manicavasagar, Batterham, Hadzi-Pavlovic (2016) [41] | Australia | SE (15–18) | 46 (24-22) | Quasi-experimental (12 weeks) | SMC (mindfulness) | DASS-21 | 0.034 | [−0.544, 0.613] |
| Chen, Yang, Wang, and Zhang (2013) [55] | China | UE (19.5 ± 0.87) | 60 (30-30) | Quasi-experimental (7 sessions/1 week) | Mindfulness meditation training | SAS | −0.440 | [−0.952, 0.071] |
| Dvorakova et al. (2017) [21] | USA | UE (18.2 ± 0.4) | 109 (55-54) | Quasi-experimental (8 sessions/6 weeks) | Mindfulness (L2B) | GAD | −0.170 | [−0.546, 0.205] |
| Gallego, Aguilar, Cangas, Rosado, and Langer (2016) [43] | Spain | UE (18–49) | 282 (237-45) | Quasi-experimental (16 sessions) | Mindfulness (MBCT) | DASS-21 | −0.640 | [−1.010, −0.269] |
| Yoga | −0.519 | [−0.886, −0.152] | ||||||
| Tai Chi | −0.589 | [−0.973, −0.204] | ||||||
| Johnson et al. (2016) [22] | Australia | SE (13.63 ± 0.43) | 258 (111-147) | Quasi-experimental (12 weeks) | MBCT/MBSR | DASS-21 | 0.192 | [−0.054, 0.439] |
| Kang, Choi, and Ryu (2009) [45] | South Korea | UE (22.47 ± 1.17) | 32 (16-16) | Quasi-experimental (8 sessions) | MBSR | STAI | −0.505 | [−1.209, 0.198] |
| Lynch, Gander, Kohls, Kudielka, and Walach (2011) [46] | England | UE (19–46) | 16 (10-6) | Quasi-experimental (8 sessions) | MBCUL (MBCT/MBSR) | HADS | −0.55 | [−1.579, 0.479] |
| McGrady, Brennan, Lynch, and Whearty (2012) [56] | USA | UE (23.4 ± 2.36) | 134 (52-82) | Quasi-experimental (8 sessions) | Wellness programs strategies | BAI | 0.120 | [−0.226, 0.468] |
| Raes et al. (2014) [18] | Belgium | SE (13–20) | 357 (182-175) | Quasi-experimental (8 weeks) | MBCT | DASS-21 | −0.443 | [−0.653, −0.233] |
| Ricarte, Ros, Latorre, and Beltrán (2015) [57] | Spain | PE (6–13) | 90 (45-45) | Quasi-experimental (8 weeks) | MBI | STATIC | −0.799 | [−1.228, −0.369] |
| Ruiz-Aranda, Salguero, Cabello, Palomera, and Fernández-Berrocal (2012) [58] | Spain | SE (13–16) | 147 (78-69) | Quasi-experimental (10 weeks) | Training program (INTEMO Project) | BASC | −0.331 | [−0.657, −0.005] |
| Shearer, Hunt, Chowdhury, and Nicol (2016) [59] | USA | UE (-) | 74 (52-22) | Quasi-experimental (4 weeks) | MBSR | STAI | −0.205 | [−0.704, 0.294] |
| Shian-Ling, Cheng-Kar, and Tian Po (2015) [49] | Malaysia | UE (21–24) | 134 (77-57) | Quasi-experimental (4 weeks) | Mindful-Gym | DASS-21 | −0.250 | [−0.594, 0.093] |
| Song and Lindquist (2015) [20] | South Korea | UE (19.6 ± 1.7) | 44 (21-23) | Quasi-experimental (10 weeks) | MBSR | DASS-21 | −0.511 | [−1.112, 0.089] |
| Spadaro and Hunker (2016) [50] | USA | UE (18–25) | 26 | Pre-experimental (8 weeks) | MBSR | HADS | −0.607 | [−1.163, −0.051] |
| Spahn, Walther, and Nusseck (2016) [60] | Germany | UE (22.1 ± 2.3) | 21 (13-8) | Quasi-experimental (14 weeks) | Seminars to overcome the MPA | STAI | −0.149 | [−1.031, 0.732] |
| Steinhardt and Dolbier (2008) [51] | USA | UE (18–53) | 57 (30-27) | Quasi-experimental (4 weeks) | Transforming Lives Resilience Education | CD–RISC | 0.467 | [−0.06, 0.993] |
| Taylor et al. (2014) [23] | England | UE (28.61 ± 9.12) | 79 (40-39) | Quasi-experimental (8 weeks) | MBCT-SH | DASS-21 | −0.561 | [−1.011, −0.111] |
| Van Gordon, Shonin, Sumich, Sundin, and Griffiths (2014) [52] | England | UE (20–42) | 25 (14-11) | Quasi-experimental (8 weeks) | MAT | DASS-21 | −1.297 | [−2.165, −0.429] |
| Study Groups | K * | M * | 95% CI | p * |
|---|---|---|---|---|
| According to treatment length | ||||
| Short duration (0–4 weeks) | 3 | −0.03 | [−0.45, 0.39] | 0.20 |
| Medium duration (from 5 to 8 weeks) | 14 | −0.45 | [−0.64, −0.26] | |
| Long duration (more than 9 weeks) | 9 | −0.36 | [−0.56, −0.17] | |
| According to the educational stage of students receiving treatment | ||||
| Primary Education | 2 | −0.88 | [−1.15, −0.61] | 0.0009 * |
| Secondary Education | 7 | −0.27 | [−0.54, −0.01] | |
| University | 17 | −0.40 | [−0.55, −0.22] | |
| According to intervention strategy | ||||
| Cognitive-behavioral programs | 8 | −0.27 | [−0.61, 0.07] | 0.39 |
| Programs based on mindfulness | 18 | −0.40 | [−0.54, −0.24] | |
| Body therapy programs (Yoga-Tai Chi) | 2 | −0.52 | [−0.88, −0.15] | |
| Author/s (Year) | Country | Educational Stage (Range or Average Age)*1 | Sample (EG-CG)*2 | Study Type | Intervention Strategy*3 | Instrument*4 | Effect Size (d) | CI to 95% |
|---|---|---|---|---|---|---|---|---|
| Aboalshamat, Hou, and Strodl (2015) [37] | Saudi Arabia | UE (20–22) | 130 (65-65) | Quasi-experimental (6 weeks) | Self-Development Program (HBUSS) | DASS-21 | −0.226 | [−0.571, 0.118] |
| Ando (2011) [9] | Japan | UE (19.1 ± 1.5) | 191 (157-34) | Quasi-experimental (11 sessions/11 weeks) | Successful Self Program. | Profile of Mood Status | −0.361 | [−0.733, 0.011] |
| Bennett and Dorjee (2016) [19] | Wales | ES (16–18) | 24 (11-13) | Quasi-experimental (8 weeks) | MBSR | DASS-21 | −0.566 | [−1.385, 0.252] |
| Bluth, Gaylord, Campo, Mullarkey, and Hobbs (2016) [39] | USA | SE (14–17) | 34 (16-18) | Quasi-experimental (6 weeks) | MFY | SMFQ | −0.611 | [−1.299, 0.078] |
| Brennan, McGrady, Lynch, Schaefer, Whearty (2016) [54] | USA | UE (23.3 ± 2.3) | 42 | Pre-experimental (4 sessions per semester) | Stress management and relaxation strategy | BDI-II | −0.035 | [−0.463, 0.392] |
| Burckhardt, Manicavasagar, Batterham, Hadzi-Pavlovic (2016) [41] | Australia | SE (15–18) | 46 (24-22) | Quasi-experimental (12 weeks) | Strong Minds Condition (mindfulness) | DASS-21 | −0.264 | [−0.845, 0.316] |
| Chen, Yang, Wang, and Zhang (2013) [55] | China | UE (19.5 ± 0.87) | 60 (30-30) | Quasi-experimental (7 sessions/1 week) | Mindfulness meditation training | SDS | 0.086 | [−0.419, 0.592] |
| Delgado, Ciria, Blanca, Mata, Vera, and Vila (2015) [42] | Spain | UE (21.5 ± 3.94) | 41 (27-14) | Quasi-experimental (3 weeks) | MBSR | BDI | −0.607 | [−1.266, 0.051] |
| Dvorakova et al. (2017) [21] | USA | UE (18.2 ± 0.4) | 109 (55-54) | Quasi-experimental (8 sessions/6 weeks) | Mindfulness (L2B) | PHQ | −0.245 | [−0.622, 0.131] |
| Gallego, Aguilar, Cangas, Rosado, and Langer (2016) [43] | Spain | UE (18–49) | 282 (237-45) | Quasi-experimental (16 sessions) | Mindfulness (MBCT) | DASS-21 | −0.353 | [−0.717, 0.011] |
| Yoga | −0.474 | [−0.840, −0.108] | ||||||
| Tai Chi | −0.056 | [−0.432, 0.320] | ||||||
| Jain et al. (2007) [62] | USA | UE (18–61) | 81 (51-30) | Quasi-experimental (4 weeks) | Mindfulness (MBSR) | DER | −0.842 | [−1.384, −0.299] |
| Relaxation training | 0.202 | [−0.335, 0.740] | ||||||
| Johnson et al. (2016) [22] | Australia | SE (13.63 ± 0.43) | 258 (111-147) | Quasi-experimental (12 weeks) | MBCT/MBSR | DASS-21 | −0.067 | [−0.314, 0.178] |
| Kang, Choi, and Ryu (2009) [45] | South Korea | UE (22.47 ± 1.17) | 32 (16-16) | Quasi-experimental (8 sessions) | MBSR | BDI | −0.703 | [−1.417, 0.010] |
| Lynch, Gander, Kohls, Kudielka, and Walach (2011) [46] | England | UE (19–46) | 16 (10-6) | Quasi-experimental (8 sessions) | MBCUL (MBCT/MBSR) | HADS | −0.318 | [−1.336, 0.700] |
| McGrady, Brennan, Lynch, and Whearty (2012) [56] | USA | UE (23.4 ± 2.36) | 134 (52-82) | Quasi-experimental (8 sessions) | Wellness strategies | BDI-II | −0.214 | [−0.562, 0.134] |
| Raes et al. (2014) [18] | Belgium | SE (13–20) | 357 (182-175) | Quasi-experimental (8 sessions) | MBCT | DASS-21 | −0.443 | [−0.653, −0.233] |
| Roberts-Wolfe, Sacchet, Hastings, Roth, and Britton (2012) [63] | USA | UE (20.10 ± 2.67) | 58 (35-23) | Quasi-experimental (12 weeks) | Samatha and Vipassana | MASQ | −0.247 | [−0.775, 0.280] |
| Ruiz-Aranda, Salguero, Cabello, Palomera, and Fernández-Berrocal (2012) [58] | Spain | SE (13–16) | 147 (78-69) | Quasi-experimental (10 weeks) | Training program (INTEMO Project) | BASC | −0.319 | [−0.644, 0.007] |
| Shearer, Hunt, Chowdhury, and Nicol (2016) [59] | USA | UE (-) | 74 (52-22) | Quasi-experimental (4 weeks) | MBSR | BDI-II | −0.270 | [−0.770, 0.230] |
| Shian-Ling, Cheng-Kar, and Tian Po (2015) [49] | Malaysia | UE (21–24) | 134 (77-57) | Quasi-experimental (4 weeks) | Mindful-Gym | DASS-21 | −0.445 | [−0.791, −0.098] |
| Song and Lindquist (2015) [20] | South Korea | UE (19.6 ± 1.7) | 44 (21-23) | Quasi-experimental (10 weeks) | MBSR | DASS-21 | −0.715 | [−1.325, −0.104] |
| Spadaro and Hunker (2016) [50] | USA | UE (18–25) | 26 | Pre-experimental (8 weeks) | MBSR | HADS | 0.072 | [−0.471, 0.616] |
| Steinhardt and Dolbier (2008) [51] | USA | UE (18–53) | 57 (30-27) | Quasi-experimental (4 weeks) | Transforming Lives Resilience Education | CD–RISC | 0.467 | [−0.06, 0.993] |
| Taylor et al. (2014) [23] | England | UE (28.61 ± 9.12) | 79 (40-39) | Quasi-experimental (8 weeks) | MBCT-SH | DASS-21 | −0.465 | [−0.912, −0.018] |
| Van Gordon, Shonin, Sumich, Sundin, and Griffiths (2014) [52] | England | UE (20–42) | 25 (14-11) | Quasi-experimental (8 weeks) | MAT | DASS-21 | −1.297 | [−2.165, −0.429] |
| Study Groups | K * | M * | CI to 95% | p * |
|---|---|---|---|---|
| According to treatment length | ||||
| Short duration (0–4 weeks) | 5 | −0.25 | [−0.64, 0.14] | 0.32 |
| Medium duration (from 5 to 8 weeks) | 12 | −0.33 | [−0.47, −0.19] | |
| Long duration (more than 9 weeks) | 8 | −0.25 | [−0.38, −0.13] | |
| According to the educational stage of students receiving treatment | ||||
| Secondary Education | 6 | −0.31 | [−0.47, −0.14] | 0.21 |
| University | 19 | −0.27 | [−0.40, −0.15] | |
| According to intervention strategy | ||||
| Cognitive-behavioral programs | 6 | −0.06 | [−0.27, 0.14] | 0.000 * |
| Programs based on mindfulness | 20 | −0.40 | [−0.51, −0.27] | |
| Body therapy programs (Yoga-Tai Chi) | 2 | −0.27 | [−0.67, 0.14] | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Valero, G.; Zurita-Ortega, F.; Ubago-Jiménez, J.L.; Puertas-Molero, P. Use of Meditation and Cognitive Behavioral Therapies for the Treatment of Stress, Depression and Anxiety in Students. A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4394. https://doi.org/10.3390/ijerph16224394
González-Valero G, Zurita-Ortega F, Ubago-Jiménez JL, Puertas-Molero P. Use of Meditation and Cognitive Behavioral Therapies for the Treatment of Stress, Depression and Anxiety in Students. A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(22):4394. https://doi.org/10.3390/ijerph16224394
Chicago/Turabian StyleGonzález-Valero, Gabriel, Félix Zurita-Ortega, José Luis Ubago-Jiménez, and Pilar Puertas-Molero. 2019. "Use of Meditation and Cognitive Behavioral Therapies for the Treatment of Stress, Depression and Anxiety in Students. A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 22: 4394. https://doi.org/10.3390/ijerph16224394