Cognitive Fusion Mediates the Relationship between Dispositional Mindfulness and Negative Affects: A Study in a Sample of Spanish Children and Adolescent School Students




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Psychological Inflexibility: Cognitive Fusion and Experiential Avoidance
2.2.2. Dispositional Mindfulness
2.2.3. Positive and Negative Affect
2.2.4. Anxiety
2.2.5. Data Analysis
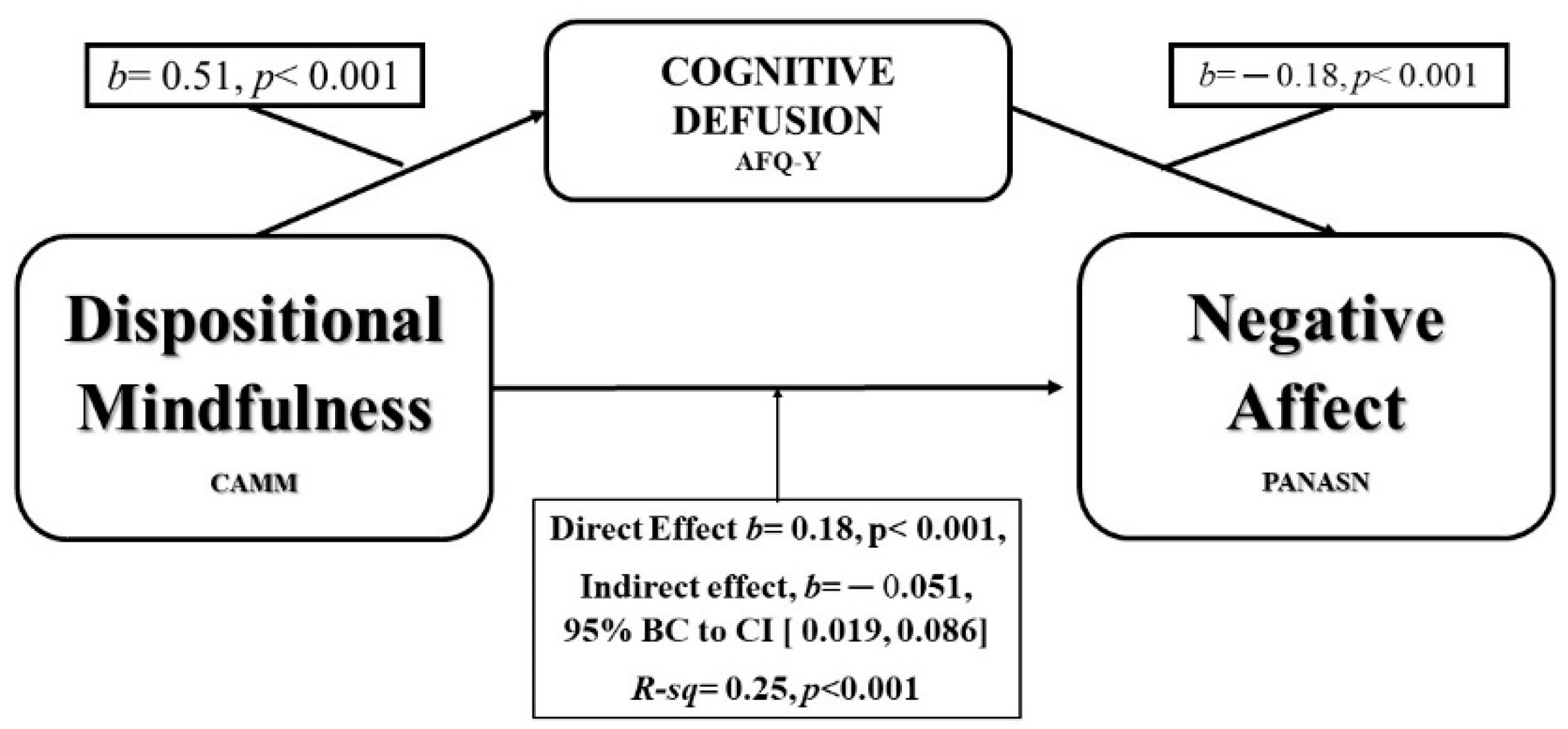
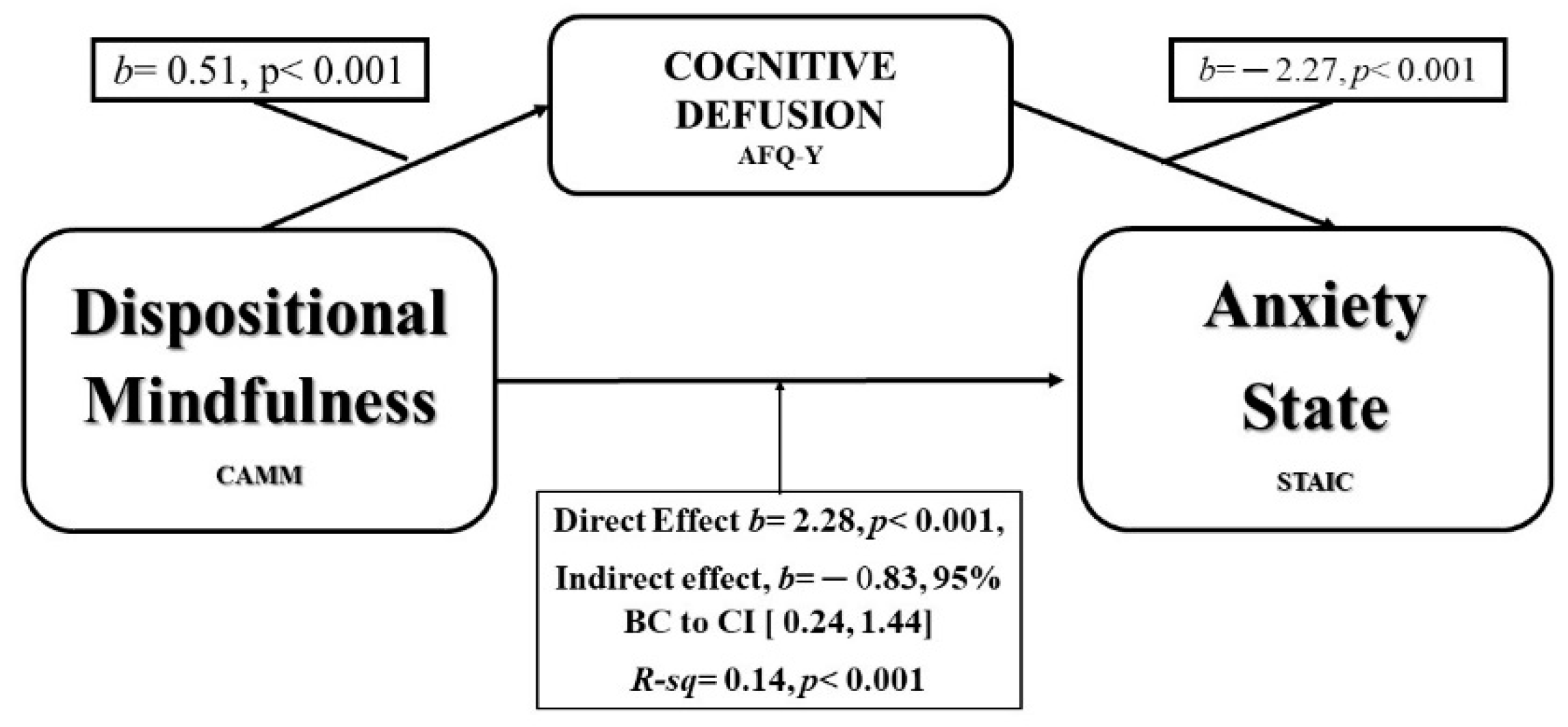
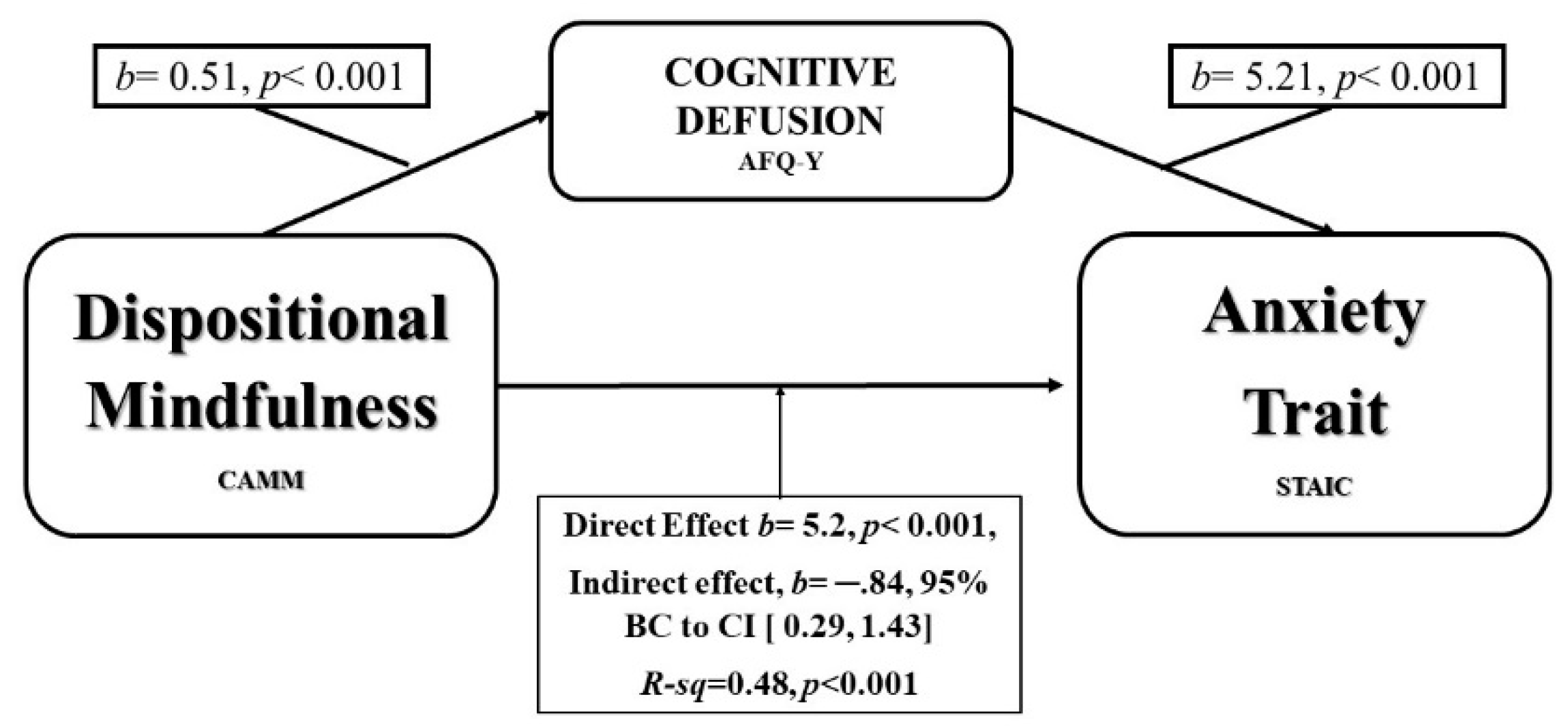
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tomlinson, E.R.; Yousaf, O.; Vitterso, A.; Jones, L. Dispositional Mindfulness and Psychological Health: A Systematic Review. Mindfulness 2018, 9, 23–43. [Google Scholar] [CrossRef] [PubMed]
- Semple, R.; Lee, J. Treating anxiety with mindfulness: Mindfulness-based cognitive therapy for children. In Acceptance and Mindfulness Treatments for Children and Adolescents; Greco, L., Hayes, S., Eds.; New Harbinger Publications: Oakland, CA, USA, 2008; pp. 63–87. ISBN 978-1608826827. [Google Scholar]
- Armstrong, A.; Morrison, K.; Twohig, M. A Preliminary Investigation of Acceptance and Commitment Therapy for Adolescent Obsessive-Compulsive Disorder. J. Cogn. Psychother. 2013, 27, 175–190. [Google Scholar] [CrossRef]
- Meagher, R.; Chessor, D.; Fogliati, V. Treatment of Pathological Worry in Children With Acceptance-Based Behavioural Therapy and a Multisensory Learning Aide: A Pilot Study. Aust. Psychol. 2018, 53, 134–143. [Google Scholar] [CrossRef]
- Hayes, S.C.; Pistorello, J.; Levin, M.E. Acceptance and Commitment Therapy as a Unified Model of Behavior Change. Couns. Psychol. 2012, 40, 976–1002. [Google Scholar] [CrossRef]
- Kashdan, T.; Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 2010, 30, 865–878. [Google Scholar] [CrossRef] [PubMed]
- Keng, S.; Smoski, M.; Robins, C. Effects of mindfulness on psychological health: A review of empirical studies. Clin. Psychol. Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef] [PubMed]
- A-Tjak, J.; Davis, M.; Morina, N.; Powers, M.; Smits, J.; Emmelkamp, P. A Meta-Analysis of the Efficacy of Acceptance and Commitment Therapy for Clinically Relevant Mental and Physical Health Problems. Psychother. Psychosom. 2015, 84, 30–36. [Google Scholar] [CrossRef]
- Simon, E.; Verboon, P. Psychological Inflexibility and Child Anxiety. J. Child Fam. Stud. 2016, 25, 3565–3573. [Google Scholar] [CrossRef]
- Van der Gucht, K.; Griffith, J.W.; Hellemans, R.; Bockstaele, M.; Pascal-Claes, F.; Raes, F. Acceptance and Commitment Therapy (ACT) for Adolescents: Outcomes of a Large-Sample, School-Based, Cluster-Randomized Controlled Trial. Mindfulness 2017, 8, 408–416. [Google Scholar] [CrossRef]
- Goodall, K.; Trejnowska, A.; Darling, S. The relationship between dispositional mindfulness, attachment security and emotion regulation. Personal. Individ. Differ. 2012, 52, 622–626. [Google Scholar] [CrossRef]
- Petrides, K.; García-Gómez, M.; Pérez-González, J.C. Pathways into psychopathology: Modeling the effects of trait emotional intelligence, mindfulness, and irrational beliefs in a clinical sample. Clin. Psychol. Psychother. 2017, 24, 1130–1141. [Google Scholar] [CrossRef] [PubMed]
- Bluth, K.; Blanton, P. Mindfulness and Self-Compassion: Exploring Pathways to Adolescent Emotional Well-Being. J. Child Fam. Stud. 2014, 23, 1298–1309. [Google Scholar] [CrossRef] [PubMed]
- Ciarrochi, J.; Kashdan, T.; Leeson, P.; Heaven, P.; Jordan, C. On being aware and accepting: A one-year longitudinal study into adolescent well-being. J. Adolesc. 2011, 34, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Greco, L.A.; Lambert, W.; Baer, R.A. Psychological inflexibility in childhood and adolescence: Development and evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychol. Assess. 2008, 20, 93–102. [Google Scholar] [CrossRef]
- Valdivia-Salas, S.; Martin-Albo, J.; Zaldivar, P.; Lombas, A.S.; Jimenez, T.I. Spanish Validation of the Avoidance and Fusion Questionnaire for Youth (AFQ-Y). Assessment 2017, 24, 919–931. [Google Scholar] [CrossRef]
- Hayes, S.; Wilson, K. Mindfulness: Method and Process. Clin. Psychol. Sci. Pract. 2006, 10, 161–165. [Google Scholar] [CrossRef]
- Shonin, E.; Van Gordon, W.; Griffiths, M.D. Mindfulness-based interventions: Towards mindful clinical integration. Front. Psychol. 2013, 4, 194. [Google Scholar] [CrossRef]
- Schweiger, M.; Ristallo, A.; Oppo, A.; Pergolizzi, T.; Presti, G.; Moderato, P. Ragazzi in lotta con emozioni e pensieri: La validazione della versione italiana dell’Avoidance and Fusiuon Questionnaire for Youth (I-AFQ.Y). Psicoter. Cogn. Comport. 2017, 23, 141–162. [Google Scholar]
- Livheim, F.; Tengström, A.; Bond, F.; Andersson, G.; Dahl, J.; Rosendahl, I. Psychometric properties of the Avoidance and Fusion Questionnaire for Youth: A psychological measure of psychological inflexibility in youth. J. Context. Behav. Sci. 2016, 5, 103–110. [Google Scholar] [CrossRef]
- Davis, D.; Hayes, J. What are the benefits of mindfulness? A practice review of psychotherapy-related research. Psychotherapy 2011, 48, 198–208. [Google Scholar] [CrossRef]
- Hayes, S.; Wilson, K.; Gifford, E.; Follette, V.; Strosahl, K. Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. J. Consult. Clin. Psychol. 1996, 64, 1152–1168. [Google Scholar] [CrossRef]
- Hayes, S.; Luoma, J.; Bond, F.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef]
- Kashdan, T.; Barrios, V.; Forsyth, J.; Steger, M. Experiential avoidance as a generalized psychological vulnerability: Comparisons with coping and emotion regulation strategies. Behav. Res. Ther. 2006, 44, 1301–1320. [Google Scholar] [CrossRef]
- Lee, J.K.; Orsillo, S.M. Investigating cognitive flexibility as a potential mechanism of mindfulness in Generalized Anxiety Disorder. J. Behav. Ther. Exp. Psychiatry 2014, 45, 208–216. [Google Scholar] [CrossRef]
- Ruiz, F.; Langer Herrera, Á.; Luciano, C.; Cangas, A.; Beltrán, I. Measuring experiential avoidance and psychological inflexibility: The Spanish version of the Acceptance and Action Questionnaire-II. Psicothema 2013, 25, 123–129. [Google Scholar]
- Feldner, M.; Zvolensky, M.; Eifert, G.; Spira, A. Emotional avoidance: An experimental test of individual differences and response suppression using biological challenge. Behav. Res. Ther. 2003, 41, 403–411. [Google Scholar] [CrossRef]
- Abramowitz, J.; Lackey, G.; Wheaton, M. Obsessive–compulsive symptoms: The contribution of obsessional beliefs and experiential avoidance. J. Anxiety Disord. 2009, 23, 160–166. [Google Scholar] [CrossRef]
- Fischer, T.D.; Smout, M.F.; Delfabbro, P.H. The relationship between psychological flexibility, early maladaptive schemas, perceived parenting and psychopathology. J. Context. Behav. Sci. 2016, 5, 169–177. [Google Scholar] [CrossRef]
- Solé, E.; Tomé-Pires, C.; de la Vega, R.; Racine, M.; Castarlenas, E.; Jensen, M.P.; Miró, J. Cognitive Fusion and Pain Experience in Young People. Clin. J. Pain 2016, 32, 602–608. [Google Scholar] [CrossRef]
- Chawla, N.; Ostafin, B. Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. J. Clin. Psychol. 2007, 63, 871–890. [Google Scholar] [CrossRef]
- Bowen, S.; Chawla, N.; Collins, S.E.; Witkiewitz, K.; Hsu, S.; Grow, J.; Clifasefi, S.; Garner, M.; Douglass, A.; Larimer, M.E.; et al. Mindfulness-based relapse prevention for substance use disorders: A pilot efficacy trial. Subst. Abus. 2009, 30, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J.; et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar] [CrossRef]
- Turanzas, J. Adaptación Transcultural de la Escala CAMM (Child and Adolescent Mindfulness Measure) y Estudio Preliminar de sus Características Psicométricas; VIU Valencian International University: Valencia, Spain, 2013. [Google Scholar] [CrossRef]
- Greco, L.; Baer, R.; Smith, G. Assessing mindfulness in children and adolescents: Development and validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychol. Assess. 2011, 23, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Turanzas, J.; Cordón, J.R.; Choca, J.P.; Mestre, J.M. Evaluating the APAC (Mindfulness for Giftedness) Program in a Spanish Sample of Gifted Children: A Pilot Study. Mindfulness 2019, 11, 1–13. [Google Scholar] [CrossRef]
- García-Rubio, C.; Rodríguez-Carvajal, R.; Langer, A.I.; Paniagua, D.; Steinebach, P.; Andreu, C.I.; Vara, M.D.; Cebolla, A. Validation of the Spanish Version of the Child and Adolescent Mindfulness Measure (CAMM) with Samples of Spanish and Chilean Children and Adolescents. Mindfulness 2019, 10, 1502–1517. [Google Scholar] [CrossRef]
- Sandín, B. Escalas Panas de afecto positivo y negativo para niños y adolescentes (PANASN). Rev. Psicopatología Psicol. Clínica 2003, 8, 173–182. [Google Scholar] [CrossRef]
- Laurent, J.; Catanzaro, S.J.; Joiner, T.E., Jr.; Rudolph, K.D.; Potter, K.I.; Lambert, S.; Osborne, L.; Gathright, T. A measure of positive and negative affect for children: Scale development and preliminary validation. Psychol. Assess. 1999, 11, 326–338. [Google Scholar] [CrossRef]
- Spielberger, C.; Goursch, R.; Lushene, R. Cuestionario de Ansiedad Estado—Rasgo, STAI. [Questionnaire State—Trait Anxiety]; TEA Ediciones: Madrid, Spain, 1982; ISBN 978-84-16231-15-7. [Google Scholar]
- Burke, C. Mindfulness-Based Approaches with Children and Adolescents: A Preliminary Review of Current Research in an Emergent Field. J. Child Fam. Stud. 2010, 19, 133–144. [Google Scholar] [CrossRef]
- Harnett, P.H.; Dawe, S. The contribution of mindfulness-based therapies for children and families and proposed conceptual integration. Child Adolesc. Ment. Health 2012, 17, 195–208. [Google Scholar] [CrossRef]
- Kazdin, A.E.; Nock, M.K. Delineating mechanisms of change in child and adolescent therapy: Methodological issues and research recommendations. J. Child Psychol. Psiquiatr. 2003, 44, 1116–1129. [Google Scholar] [CrossRef]
- Kraemer, H.C.; Stice, E.; Kazdin, A.; Offord, D.; Kupfer, D. How Do Risk Factors Work Together? Mediators, Moderators, and Independent, Overlapping, and Proxy Risk Factors. Am. J. Psychiatry 2001, 158, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Breslin, F.; Zack, M.; McMain, S. An Information-Processing Analysis of Mindfulness: Implications for Relapse Prevention in the Treatment of Substance Abuse. Clin. Psychol. Sci. Pract. 2002, 9, 275–299. [Google Scholar] [CrossRef]
- García-Rubio, C.; Luna, T.; Castillo, R.; Rodríguez-Carvajal, R. Impacto de una intervención breve basada en mindfulness en niños: Un estudio piloto. Rev. Interuniv. Form. Profr. 2016, 87, 61–74. [Google Scholar]
- Guerra, J.; García-Gómez, M.; Turanzas, J.; Cordón, J.; Suárez-Jurado, C.; Mestre, J.M. A Brief Spanish Version of the Child and Adolescent Mindfulness Measure (CAMM). A Dispositional Mindfulness Measure. Int. J. Environ. Res. Public Health 2019, 16, 1355. [Google Scholar] [CrossRef]
- Muris, P.; Meesters, C.; Herings, A.; Jansen, M.; Vossen, C.; Kersten, P. Inflexible Youngsters: Psychological and Psychopathological Correlates of the Avoidance and Fusion Questionnaire for Youths in Nonclinical Dutch Adolescents. Mindfulness 2017, 8, 1381–1392. [Google Scholar] [CrossRef]
- Biglan, A.; Hayes, S.; Pistorello, J. Acceptance and Commitment: Implications for prevention science. Prev. Sci. 2008, 9, 139–152. [Google Scholar] [CrossRef]
- Carvalho, J.P.; Hopko, D.R. Journal of Behavior Therapy and Behavioral theory of depression: Reinforcement as a mediating variable between avoidance and depression. J. Behav. Ther. Exp. Psychiatry 2011, 42, 154–162. [Google Scholar] [CrossRef]
- Manos, R.C.; Kanter, J.W.; Busch, A.M. Author’s personal copy Clinical Psychology Review A critical review of assessment strategies to measure the behavioral activation model of depression. Clin. Psychol. Rev. 2010, 30, 547–561. [Google Scholar] [CrossRef]
- Kazdin, A. Mediators and Mechanisms of Change in Psychotherapy Research. Annu. Rev. Clin. Psychol. 2007, 3, 1–27. [Google Scholar] [CrossRef]
- Fergus, T.A. I Really Believe I Suffer From a Health Problem: Examining an Association Between Cognitive Fusion and Healthy Anxiety. J. Clin. Psychol. 2015, 71, 920–934. [Google Scholar] [CrossRef]
- Dyck, M.J.; Denver, E. Can the Emotion Recognition Ability of Deaf Children be Enhanced? A Pilot Study. J. Deaf Stud. Deaf Educ. 2003, 8, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.; Pinto-Gouvela, J.; Marôco, J. The Role of Negative Affect, Rumination, Cognitive Fusion and Mindfulness on Depressive Symptoms in Depressed Outpatients and Normative Individuals. Int. J. Psychol. Psychol. Ther. 2018, 18, 207–220. [Google Scholar]
- Nitzan-Assayag, Y.; Yuval, K.; Tanay, G.; Aderka, I.M. Reduced Reactivity to and Suppression of Thoughts Mediate the Effects of Mindfulness Training on Recovery Outcomes Following Exposure to Potentially Traumatic Stress. Mindfulness 2017, 8, 920–932. [Google Scholar] [CrossRef]
- Gillanders, D.T.; Bolderston, H.; Bond, F.W.; Dempster, M.; Flaxman, P.E.; Campbell, L.; Kerr, S.; Tansey, L.; Noel, P.; Ferenbach, C.; et al. The Development and Initial Validation of the Cognitive Fusion Questionnaire. Behav. Ther. 2014, 45, 83–101. [Google Scholar] [CrossRef]
- Rau, H.K.; Williams, P.G. Dispositional mindfulness: A critical review of construct validation research. Pers. Individ. Differ. 2016, 93, 32–43. [Google Scholar] [CrossRef]
- Hayes, S.; Wilson, K. Acceptance and commitment therapy: Altering the verbal support for experiential avoidance. Behav. Anal. 1994, 17, 289–303. [Google Scholar] [CrossRef]
- Nitzan-Assayag, Y.; Aderka, I.; Bernstein, A. Dispositional mindfulness in trauma recovery: Prospective relations and mediating mechanisms. J. Anxiety Disord. 2015, 36, 25–32. [Google Scholar] [CrossRef]
- Luoma, J.; Hayes, S.; Walser, R. Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists; New Harbinger Publications: Oakland, CA, USA, 2007; ISBN 1-57224-498-4. [Google Scholar]
- Coffman, S.; Dimidjian, S.; Baer, R. Mindfulness-Based Cognitive Therapy for prevention of depressive relapse. In Mindfulness-Based Treatment Approaches Clinician’s Guide to Evidence Base and Applications; Baer, R., Ed.; Elsevier Academic Press: Burlington, MA, USA, 2006; pp. 31–50. ISBN 978-0-12-088519-0. [Google Scholar]
- Kämpfe, C.K.; Gloster, A.T.; Wittchen, H.U.; Helbig-Lang, S.; Lang, T.; Gerlach, A.L.; Richter, J.; Alpers, G.W.; Fehm, L.; Kircher, T.; et al. Experiential avoidance and anxiety sensitivity in patients with panic disorder and agoraphobia: Do both constructs measure the same? Int. J. Clin. Health Psychol. 2012, 12, 5–22. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Min—Max | M (SD) | α | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Age | 8–16 | 11.25 (2.2) | - | * | |||||||||
| 2 Gender | (0: male, 1: female) | - | −0.02 | * | |||||||||
| 3 CF_AFQ_Y | 0–3.38 | 1.03 (0.70) | 0.65 | −0.12 * | 0.02 | * | |||||||
| 4 EA_AFQ_Y | 0–4 | 1.87 (0.89) | 0.76 | −0.36 ** | 0.00 | 0.62 ** | * | ||||||
| 5 AFQ_Y_Total | 0–3.53 | 1.47 (0.72) | 0.82 | −0.29 ** | 0.01 | 0.87 ** | 0.93** | * | |||||
| 6 DM_CAMM | 0.4–4 | 2.66 (0.27) | 0.73 | 0.23 ** | 0.00 | −0.55 ** | −0.60 ** | −0.64 ** | * | ||||
| 7 PA_PANASN | 1–3 | 2.35 (0.37) | 0.72 | −0.05 | 0.15 * | −0.07 | −0.02 | −0.04 | −0.04 | * | |||
| 8 NA_PANASN | 1–2.6 | 1.61 (0.39) | 0.78 | −0.11 * | 0.13 * | 0.40 ** | 0.33 ** | 0.40 ** | −0.47 ** | −0.15 ** | * | ||
| 9 BALANCE | −0.8–2 | 0.74 (0.58) | 0.65 | 0.04 | 0.01 | −0.31 ** | −0.24 ** | −0.30 ** | 0.29 ** | 0.75 ** | −0.77 ** | * | |
| 10 ANX_S | 20–55 | 29.97(6.41) | 0.82 | −0.09 | −0.15 ** | 0.34 ** | 0.24 ** | 0.31 ** | −0.31 ** | −0.29 ** | 0.37 ** | −0.44 ** | * |
| 11 ANX_T | 20–54 | 33.37(7.19) | 0.85 | -0.18 * | 0.07 | 0.50 ** | 0.49 ** | 0.55 ** | −0.67 ** | −0.00 | 0.62 ** | −0.42 ** | 0.34 ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Gómez, M.; Guerra, J.; López-Ramos, V.M.; Mestre, J.M. Cognitive Fusion Mediates the Relationship between Dispositional Mindfulness and Negative Affects: A Study in a Sample of Spanish Children and Adolescent School Students. Int. J. Environ. Res. Public Health 2019, 16, 4687. https://doi.org/10.3390/ijerph16234687
García-Gómez M, Guerra J, López-Ramos VM, Mestre JM. Cognitive Fusion Mediates the Relationship between Dispositional Mindfulness and Negative Affects: A Study in a Sample of Spanish Children and Adolescent School Students. International Journal of Environmental Research and Public Health. 2019; 16(23):4687. https://doi.org/10.3390/ijerph16234687
Chicago/Turabian StyleGarcía-Gómez, María, Joan Guerra, Víctor M. López-Ramos, and José M. Mestre. 2019. "Cognitive Fusion Mediates the Relationship between Dispositional Mindfulness and Negative Affects: A Study in a Sample of Spanish Children and Adolescent School Students" International Journal of Environmental Research and Public Health 16, no. 23: 4687. https://doi.org/10.3390/ijerph16234687
APA StyleGarcía-Gómez, M., Guerra, J., López-Ramos, V. M., & Mestre, J. M. (2019). Cognitive Fusion Mediates the Relationship between Dispositional Mindfulness and Negative Affects: A Study in a Sample of Spanish Children and Adolescent School Students. International Journal of Environmental Research and Public Health, 16(23), 4687. https://doi.org/10.3390/ijerph16234687