Hip Osteoarthritis and Physical Workload: Influence of Study Quality on Risk Estimations—A Meta-Analysis of Epidemiological Findings


Abstract
:1. Introduction
2. Materials and Methods
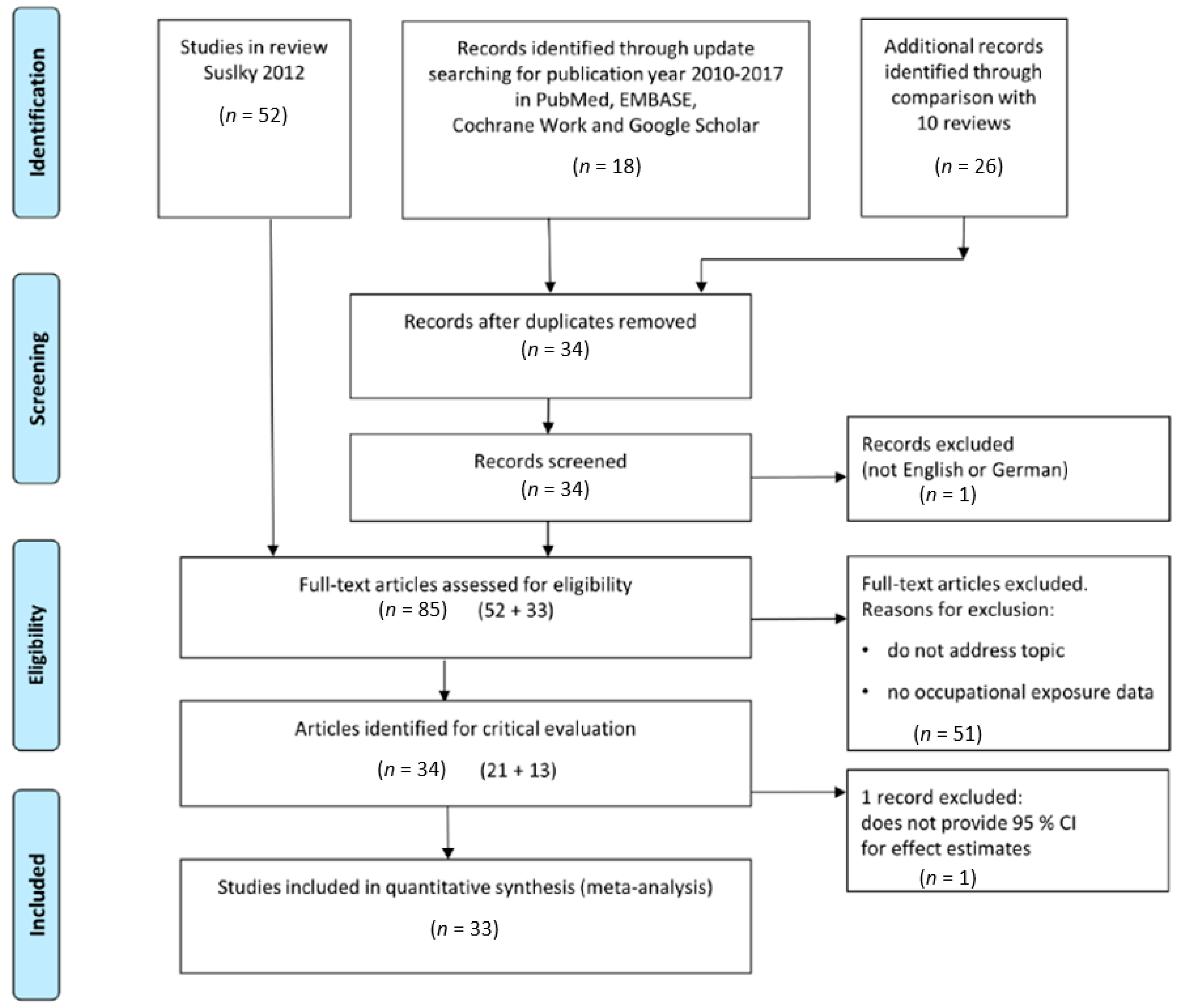
2.1. Systematic Literature Searches
- Studies did not address the topic, or address non-idiopathic hip osteoarthritis
- Absence of occupational exposure data
- Studies did not provide 95% CI for effect estimates
2.2. Classification of Type of Studies for Evidence Comparison
2.3. Classification of Quality Level of Published Studies
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Felson, D.T. Epidemiology of hip and knee osteoarthritis. Epidemiol. Rev. 1988, 10, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Sulsky, S.I.; Carlton, L.; Bochmann, F.; Ellegast, R.; Glitsch, U.; Hartmann, B.; Pallapies, D.; Seidel, D.; Sun, Y. Epidemiological evidence for work load as a risk factor for osteoarthritis of the hip: A systematic review. PLoS ONE 2012, 7, e31521. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Rantz, M.J. Research methods: Managing primary study quality in meta-analyses. Res. Nurs. Health 2003, 26, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; van Straten, A.; Bohlmeijer, E.; Hollon, S.D.; Andersson, G. The effects of psychotherapy for adult depression are overestimated: A meta-analysis of study quality and effect size. Psychol. Med. 2010, 40, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.D.; Golightly, Y.M. State of the evidence. Curr. Opin. Rheumatol. 2015, 27, 276–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmann, A.; Bolm-Audorff, U.; Krone, D.; Seidler, A.; Liebers, F.; Haerting, J.; Freiberg, A.; Unverzagt, S. Occupational Strain as a Risk for Hip Osteoarthritis. Dtsch. Arztebl. Int. 2017, 114, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; Agaliotis, M.; Bridgett, L.; Mackey, M.G. Hip and knee pain: Role of occupational factors. Best Pract. Res. Clin. Rheumatol. 2011, 25, 81–101. [Google Scholar] [CrossRef]
- Harris, E.C.; Coggon, D. Hip osteoarthritis and work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 462–482. [Google Scholar] [CrossRef]
- Hartmann, B.; Seidel, D. Koxarthrosen im Erwerbsalter. Eine Übersicht zum aktuellen Erkenntnisstand. [Coxarthrosis during working life. A review]. Arbeitsmed. Sozialmed. Umweltmed. 2011, 46, 670–686. [Google Scholar]
- Johnson, V.L.; Hunter, D.J. The epidemiology of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2014, 28, 5–15. [Google Scholar] [CrossRef]
- Neogi, T.; Zhang, Y. Epidemiology of osteoarthritis. Rheum. Dis. Clin. N. Am. 2013, 39, 1–19. [Google Scholar] [CrossRef]
- Richmond, S.A.; Fukuchi, R.K.; Ezzat, A.; Schneider, K.; Schneider, G.; Emery, C.A. Are joint injury, sport activity, physical activity, obesity, or occupational activities predictors for osteoarthritis? A systematic review. J. Orthop. Sports Phys. Ther. 2013, 43, B515–B519. [Google Scholar] [CrossRef] [PubMed]
- Spahn, G.; Kaiser, M.; Gantz, S.; Schiltenwolf, M.; Hartmann, B.; Schiele, R.; Hofmann, G.O. Systematisches Literatur-Review und Metaanalyse zur Bestimmung von Risikofaktoren für die Koxarthrose [Risk factors for hip osteoarthritis (coxarthrosis). Results from a systematic review and meta-analysis]. Arbeitsmed. Sozialmed. Umweltmed. 2014, 49, 207–222. [Google Scholar]
- Yucesoy, B.; Charles, L.E.; Baker, B.; Burchfiel, C.M. Occupational and genetic risk factors for osteoarthritis: A review. Work 2015, 50, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Axmacher, B.; Lindberg, H. Coxarthrosis in farmers. Clin. Orthop. Relat. Res. 1993, 287, 82–86. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, K.D.; Chen, J.C.; Callahan, L.F.; Golightly, Y.M.; Helmick, C.G.; Renner, J.B.; Jordan, J.M. Associations of occupational tasks with knee and hip osteoarthritis: The Johnston County Osteoarthritis Project. J. Rheumatol. 2010, 37, 842–850. [Google Scholar] [CrossRef]
- Andersen, S.; Thygesen, L.C.; Davidsen, M.; Helweg-Larsen, K. Cumulative years in occupation and the risk of hip or knee osteoarthritis in men and women: A register-based follow-up study. Occup. Environ. Med. 2012, 69, 325–330. [Google Scholar] [CrossRef]
- Coggon, D.; Kellingray, S.; Inskip, H.; Croft, P.; Campbell, L.; Cooper, C. Osteoarthritis of the hip and occupational lifting. Am. J. Epidemiol. 1998, 147, 523–528. [Google Scholar] [CrossRef]
- Croft, P.; Coggon, D.; Cruddas, M.; Cooper, C. Osteoarthritis of the hip: An occupational disease in farmers. Br. Med. J. 1992, 304, 1269–1272. [Google Scholar] [CrossRef]
- Croft, P.; Cooper, C.; Wickham, C.; Coggon, D. Osteoarthritis of the hip and occupational activity. Scand. J. Work Environ. Health 1992, 18, 59–63. [Google Scholar] [CrossRef]
- Cvijetic, S.; Dekanic-Ozegovic, D.; Campbell, L.; Cooper, C.; Potocki, K. Occupational physical demands and hip osteoarthritis. Arh. Hig. Rada Toksikol. 1999, 50, 371–379. [Google Scholar] [PubMed]
- Elsner, G.; Nienhaus, A.; Beck, W. Coxarthrose und berufliche Belastungen [Coxarthrosis and occupational work load]. Z. Gesundheitswiss. 1995, 3, 131–144. [Google Scholar] [CrossRef]
- Flugsrud, G.B.; Nordsletten, L.; Espehaug, B.; Havelin, L.I.; Meyer, H.E. Risk factors for total hip replacement due to primary osteoarthritis: A cohort study in 50,034 persons. Arthritis Rheum. 2002, 46, 675–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, J.; Ingvarsson, T.; Englund, M.; Lohmander, S. Association between occupation and knee and hip replacement due to osteoarthritis: A case-control study. Arthritis Res. Ther. 2010, 12, R102. [Google Scholar] [CrossRef] [PubMed]
- Heliövaara, M.; Makela, M.; Impivaara, O.; Knekt, P.; Aromaa, A.; Sievers, K. Association of overweight, trauma and workload with coxarthrosis. A health survey of 7217 persons. Acta Orthop. Scand. 1993, 64, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Hubertsson, J.; Turkiewicz, A.; Petersson, I.F.; Englund, M. Understanding Occupation, Sick Leave, and Disability Pension Due to Knee and Hip Osteoarthritis from a Sex Perspective. Arthritis Care Res. 2017, 69, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, S.; Sonne-Holm, S.; Soballe, K.; Gebuhr, P.; Lund, B. The distribution and inter-relationships of radiologic features of osteoarthrosis of the hip. A survey of 4151 subjects of the Copenhagen City Heart Study: The Osteoarthrosis Substudy. Osteoarthr. Cartil. 2004, 12, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Juhakoski, R.; Heliovaara, M.; Impivaara, O.; Kroger, H.; Knekt, P.; Lauren, H.; Arokoski, J.P. Risk factors for the development of hip osteoarthritis: A population-based prospective study. Rheumatology 2009, 48, 83–87. [Google Scholar] [CrossRef]
- Kaila-Kangas, L.; Arokoski, J.; Impivaara, O.; Viikari-Juntura, E.; Leino-Arjas, P.; Luukkonen, R.; Heliövaara, M. Associations of hip osteoarthritis with history of recurrent exposure to manual handling of loads over 20 kg and work participation: A population-based study of men and women. Occup. Environ. Med. 2011, 68, 734–738. [Google Scholar] [CrossRef]
- Lau, E.M.C.; Lam, T.K.; Chan, N.H.; Kumta, S.M. Risk factors for primary osteoarthritis of the hip and knee in the Hong Kong Chinese population. Hong Kong Med. J. 2007, 13, S9–S14. [Google Scholar]
- Plotnikoff, R.; Karunamuni, N.; Lytvyak, E.; Penfold, C.; Schopflocher, D.; Imayama, I.; Johnson, S.T.; Raine, K. Osteoarthritis prevalence and modifiable factors: A population study. BMC Public Health 2015, 15, 1195. [Google Scholar] [CrossRef]
- Pope, D.P.; Hunt, I.M.; Birrell, F.N.; Silman, A.J.; Macfarlane, G.J. Hip pain onset in relation to cumulative workplace and leisure time mechanical load: A population based case-control study. Ann. Rheum. Dis. 2003, 62, 322–326. [Google Scholar] [CrossRef]
- Ratzlaff, C.R.; Steininger, G.; Doerfling, P.; Koehoorn, M.; Cibere, J.; Liang, M.H.; Wilson, D.R.; Esdaile, J.M.; Kopec, J.A. Influence of lifetime hip joint force on the risk of self-reported hip osteoarthritis: A community-based cohort study. Osteoarthr. Cartil. 2011, 19, 389–398. [Google Scholar] [CrossRef]
- Riyazi, N.; Rosendaal, F.R.; Slagboom, E.; Kroon, H.M.; Breedveld, F.C.; Kloppenburg, M. Risk factors in familial osteoarthritis: The GARP sibling study. Osteoarthr. Cartil. 2008, 16, 654–659. [Google Scholar] [CrossRef]
- Roach, K.E.; Persky, V.; Miles, T.; Budiman-Mak, E. Biomechanical aspects of occupation and osteoarthritis of the hip: A case-control study. J. Rheumatol. 1994, 21, 2334–2340. [Google Scholar]
- Rubak, T.S.; Svendsen, S.W.; Soballe, K.; Frost, P. Risk and rate advancement periods of total hip replacement due to primary osteoarthritis in relation to cumulative physical workload. Scand. J. Work Environ Health 2013, 39, 486–494. [Google Scholar] [CrossRef] [Green Version]
- Rubak, T.S.; Svendsen, S.W.; Soballe, K.; Frost, P. Total hip replacement due to primary osteoarthritis in relation to cumulative occupational exposures and lifestyle factors: A nationwide nested case-control study. Arthritis Care Res. 2014, 66, 1496–1505. [Google Scholar] [CrossRef]
- Thelin, A. Hip joint arthrosis: An occupational disorder among farmers. Am. J. Ind. Med. 1990, 18, 339–343. [Google Scholar] [CrossRef]
- Thelin, A.; Jansson, B.; Jacobsson, B.; Strom, H. Coxarthrosis and farm work: A case-referent study. Am. J. Ind. Med. 1997, 32, 497–501. [Google Scholar] [CrossRef]
- Thelin, A.; Vingard, E.; Holmberg, S. Osteoarthritis of the hip joint and farm work. Am. J. Ind. Med. 2004, 45, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Thelin, A.; Holmberg, S. Hip osteoarthritis in a rural male population: A prospective population-based register study. Am. J. Ind. Med. 2007, 50, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Tüchsen, F.; Hannerz, H.; Jensen, M.V.; Krause, N. Socioeconomic status, occupation, and risk of hospitalisation due to coxarthrosis in Denmark 1981–1999. Ann. Rheum. Dis. 2003, 62, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Vingård, E.; Alfredsson, L.; Goldie, I.; Hogstedt, C. Occupation and osteoarthrosis of the hip and knee: A register-based cohort study. Int. J. Epidemiol. 1991, 20, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Vingård, E.; Hogstedt, C.; Alfredsson, L.; Fellenius, E.; Goldie, I.; Koster, M. Coxarthrosis and physical work load. Scand. J. Work Environ. Health 1991, 17, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Vingård, E.; Alfredsson, L.; Fellenius, E.; Hogstedt, C. Disability pensions due to musculo-skeletal disorders among men in heavy occupations. A case-control study. Scand. J. Soc. Med. 1992, 20, 31–36. [Google Scholar]
- Vingård, E.; Alfredsson, L.; Malchau, H. Osteoarthrosis of the hip in women and its relation to physical load at work and in the home. Ann. Rheum. Dis. 1997, 56, 293–298. [Google Scholar] [Green Version]
- Wang, Y.; Simpson, J.A.; Wluka, A.E.; Teichtahl, A.J.; English, D.R.; Giles, G.G.; Graves, S.; Cicuttini, F.M. Is physical activity a risk factor for primary knee or hip replacement due to osteoarthritis? A prospective cohort study. J. Rheumatol. 2011, 38, 350–357. [Google Scholar] [CrossRef]
- Yoshimura, N.; Sasaki, S.; Iwasaki, K.; Danjoh, S.; Kinoshita, H.; Yasuda, T.; Tamaki, T.; Hashimoto, T.; Kellingray, S.; Croft, P.; et al. Occupational lifting is associated with hip osteoarthritis: A Japanese case-control study. J. Rheumatol. 2000, 27, 434–440. [Google Scholar]
- Lievense, A.; Bierma-Zeinstra, S.; Verhagen, A.; Verhaar, J.; Koes, B. Influence of work on the development of osteoarthritis of the hip: A systematic review. J. Rheumatol. 2001, 28, 2520–2528. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis Criteria | Diagnostic Quality Score * (Evidence Level) |
|---|---|
| Anamnesis/questionnaire: hip pain without clinical check | 1 |
| Hip pain and clinical reduction of movement without radiographic features or Radiographic features without clinical examination, without THR (total hip replacement) | 2 |
| Hip pain with clinical reduction of movement and clearly defined radiographic features (joint space narrowing or Kellgren-Lawrence-score grade 2 and above or comparable criteria) or Diagnosis with indication for THR (total hip replacement) | 3 |
| Exposure Assessment | Exposure Quality Score * |
|---|---|
| Profession, job title, classification of occupation | 1 |
| Qualitative specification of exposure in different work activities (lifting, climbing stairs, sitting) | 2 |
| Quantitative specification of exposure in different work activities/physical strains with information on intensity (e.g., load weight steps) and duration | 3 |
| Quantitative specification of exposure (as above) with additional plausibility check (e.g., information on daily work output or special controls through video analysis) | 4 |
| Quantitative, measured exposure with quantitative assessment or modeling of hip joint strain | 5 |
| Study | Design | Outcome Assessment | Study Population | Quality Score of | Confounders Considered/Controlled | Exposure Parameter Estimated | RR/OR ** (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | Age (Years) | Exposure Assessment | Hip OA * Ascertainment | Age | Sex | BMI | Prior Injury | |||||
| Allen 2010 [17] | Cross-sectional | Prevalence | 2729 | >45 | 2 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy lifting | 1.67 (1.26–2.23) |
| Andersen 2012 [18] | Cohort | Incidence | 2.1 million | 25–59 | 1 | 3 | ✓ | ✓ | ✓ | Farmer | 1.96 (1.84–2.08) | |
| Axmacher 1993 [15] | Cross-sectional | Prevalence | 565 farmers | 40–64 | 1 | 2 | ✓ | ✓ | Farmer | 12 (6.7–21.4) | ||
| Coggon 1998 [19] | Case-control | Incidence | 611 cases, 611 controls | 45–91 | 3 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy lifting | 2.3 (1.3–4.4) |
| Croft 1992a [20] | Cross-sectional | Prevalence | 167 farmers, 83 office staff | 60–76 | 1 | 2 | ✓ | ✓ | Farmer | 9.3 (1.9–44.5) | ||
| Croft 1992b [21] | Case-control | Prevalence | 245 cases, 294 controls | 60–75 | 3 | 2 | ✓ | ✓ | Heavy lifting | 2.5 (1.1–5.7) | ||
| Cvijetic 1999 [22] | Cross-sectional | Prevalence | 593 | >45 | 2 | 3 | ✓ | ✓ | ✓ | Heavy physical | 1.22 (0.98–2.46) | |
| Elsner 1995 [23] | Case-control | Prevalence | 220 cases, 198 controls | Median ca. 50 | 1 | 3 | ✓ | ✓ | Heavy lifting | 1.1 (0.65–2.10) | ||
| Flugsrud 2002 [24] | Cohort | Incidence | 50,034 | Mean 55 | 2 | 3 | ✓ | ✓ | ✓ | Heavy physical | 2.10 (1.50–3.00) | |
| Franklin 2010 [25] | Case-control | Prevalence | 1408 cases, 1082 controls | ≥60 | 1 | 3 | ✓ | ✓ | ✓ | Farmer | 3.6 (2.1–6.2) | |
| Heliovaara 1993 [26] | Cross-sectional | Prevalence | 7217 | ≥30 | 2 | 2 | ✓ | ✓ | ✓ | ✓ | Heavy physical | 2.7 (1.7–4.4) |
| Hubertsson 2017 [27] | Cohort | Incidence | 165,179 | 40–70 | 1 | 3 | ✓ | ✓ | Farmer | 1.56 (1.03–2.38) | ||
| Jacobsen 2004a [28] | Cross-sectional | Prevalence | 4151 | 22–93 | 3 | 2 | ✓ | ✓ | ✓ | Heavy lifting | 1.0 | |
| Juhakoski 2009 [29] | Cohort | Incidence | 840 | 30–72 | 2 | 2 | ✓ | ✓ | ✓ | ✓ | Heavy physical | 6.7 (2.3–19.5) |
| Kaila-Kangas 2011 [30] | Cross-sectional | Prevalence | 6556 | 30–97 | 3 | 2 | ✓ | ✓ | ✓ | ✓ | Handling load | 2.3 (1.2–4.3) |
| Lau 2007 [31] | Case-control | Prevalence | 138 cases, 414 controls | not given | 3 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy lifting | 4,15 (1.23–14.0) |
| Plotnikoff 2015 [32] | Cross-sectional | Prevalence | 4733 | ≥18 | 1 | 3 | ✓ | ✓ | Heavy physical | 1.32 (0.34–5.17) | ||
| Pope 2003 [33] | Case-control | Prevalence | 352 cases, 3002 controls | 18–85 | 3 | 1 | ✓ | ✓ | Handling load | 1.74 (1.06–2.86) | ||
| Ratzlaff 2011 [34] | Cohort | Incidence | 2918 | 45–85 | 2 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy physical | 1.80 (0.95–2.82) |
| Riyazi 2008 [35] | Case-control | Prevalence | 93 cases, 345 controls | 40–79 | 1 | 3 | ✓ | ✓ | Heavy physical | 3.3 (1.3–8.2) | ||
| Roach 1994 [36] | Case-control | Prevalence | 99 cases, 233 controls | Mean 68 | 3 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy physical | 2.4 (1.2–4.7) |
| Rubak 2013 [37] | Cohort | Incidence | 1.9 million | 31–71 | 3 | 3 | ✓ | ✓ | Heavy physical | 1.33 (1.17–1.53) | ||
| Rubak 2014 [38] | Case-control nested | Incidence | 1776 cases, 1776 controls | 41–69 | 3 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy physical | 1.35 (1.05–1.74) |
| Thelin 1990 [39] | Case-control | Prevalence | 105 cases, 222 controls | 55–70 | 1 | 3 | ✓ | ✓ | Farmer | 3.2 (1.8–5.5) | ||
| Thelin 1997 [40] | Case-control | Prevalence | 216 cases, 479 controls | <70 | 2 | 2 | ✓ | ✓ | Farmer | 4.45 (2.90–6.83) | ||
| Thelin 2004 [41] | Case-control | Prevalence | 369 cases, 369 controls | 40–71 | 2 | 3 | ✓ | ✓ | ✓ | Farmer | 13.3 (1.2–145.0) | |
| Thelin 2007 [42] | Cohort | Incidence | 3437 | 40–59 | 1 | 2 | ✓ | Farmer | 3.0 (1.7–5.3) | |||
| Tuchsen 2003 [43] | Cohort | Incidence | Not given | 20–59 | 1 | 3 | ✓ | ✓ | Farmer | 2.86 (2.62–3.13) | ||
| Vingard 1991a [44] | Cohort | Incidence | 250,217 | Not given | 1 | 3 | ✓ | ✓ | Farmer | 3.78 (2.91–3.88) | ||
| Vingard 1991b [45] | Case-control | Incidence | 239 cases, 302 controls | 50–70 | 3 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy lifting | 3.31 (1.97–5.57) |
| Vingard 1992 [46] | Case-control | Prevalence | 140 cases, 298 controls | 50–69 | 1 | 3 | ✓ | ✓ | Heavy physical | 12.4 (6.7-23.0) | ||
| Vingard 1997 [47] | Case-control | Prevalence | 230 cases, 273 controls | 50–70 | 3 | 3 | ✓ | ✓ | ✓ | Heavy lifting | 1.5 (0.9–2.5) | |
| Wang 2011 [48] | Cohort | Incidence | 39,023 | 27–75 | 1 | 3 | ✓ | ✓ | ✓ | Heavy physical | 1.13 (0.84–1.52) | |
| Yoshimura 2000 [49] | Case-control | Incidence | 114 cases, 114 controls | ≥45 | 3 | 3 | ✓ | ✓ | ✓ | ✓ | Heavy lifting | 4.1 (1.1–15.2) |
| Exposure Parameters Estimated | Type of Studies | Exposure Score | Diagnostic Score | Number of Studies | Overall ES * (95% CI) | Heterogeneity of Studies (I2) |
|---|---|---|---|---|---|---|
| Heavy physical workload/heavy lifting | Prevalence studies | All studies | All studies | 13 | 2.00 (1.34–2.99) | 76% |
| 1–2 | 1–2 | 1 | 2.70 (1.70–4.40) | - | ||
| All Studies | =3 | 9 | 1.92 (1.02–3.59) | 83% | ||
| ≥3 | All studies | 6 | 1.98 (1.53–2.58) | 0% | ||
| ≥3 | =3 | 3 | 1.94 (1.17–3.20) | 30% | ||
| Incidence Studies | ||||||
| Case-control | ≥3 | =3 | 3 | 2.93 (2.00–4.28) | 0% | |
| Cohort | All studies | All studies | 6 | 1.40 (1.03–1.89) | 71% | |
| 1–2 | 1–2 | 1 | 6.70 (2.30–19.50) | - | ||
| All Studies | =3 | 5 | 1.38 (1.12–1.69) | 54% | ||
| ≥3 | =3 | 2 | 1.33 (1.19–1.50) | 0% | ||
| Farmer | Prevalence studies | 1–2 | All studies | 8 | 4.74 (2.84–7.89) | 68% |
| 1–2 | 1–2 | 4 | 5.38 (2.23–12.97) | 79% | ||
| 1–2 | =3 | 4 | 3.97 (2.17–7.26) | 46% | ||
| Incidence studies | ||||||
| Cohort | 1–2 | All studies | 5 | 2.34 (1.55–3.53) | 96% | |
| 1–2 | 1–2 | 1 | 3.00 (1.70–5.30) | - | ||
| 1–2 | =3 | 4 | 2.34 (1.54–3.54) | 97% |
| Exposure Parameters Estimated | Type of Studies | Exposure Score | Diagnostic Score | Number of Studies | Overall ES * (95% CI) | Heterogeneity of Studies (I2) |
|---|---|---|---|---|---|---|
| Heavy physical workload/heavy lifting | Prevalence studies | All studies | All studies | 8 | 2.25 (1.13–4.47) | 84% |
| 1–2 | 1–2 | 0 | - | - | ||
| All Studies | =3 | 6 | 2.21 (0.85–5.80) | 89% | ||
| ≥3 | All studies | 4 | 2.52 (1.71–3.70) | 0% | ||
| ≥3 | =3 | 2 | 2.74 (1.51–4.96) | 0% | ||
| Incidence studies | ||||||
| Case-control | ≥3 | =3 | 2 | 2.84 (1.91–4.22) | 0% | |
| Cohort | All studies | All studies | 3 | 1.40 (1.07–1.82) | 66% | |
| 1–2 | 1–2 | 0 | - | - | ||
| All Studies | =3 | 3 | 1.40 (1.07–1.82) | 66% | ||
| ≥3 | =3 | 2 | 1.33 (1.19–1.50) | 0% | ||
| Farmer | Prevalence studies | 1–2 | All studies | 7 | 4.69 (2.78–7.89) | 71% |
| 1–2 | 1–2 | 4 | 5.38 (2.23–12.97) | 79% | ||
| 1–2 | =3 | 3 | 3.85 (2.06–7.21) | 56% | ||
| Incidence studies | ||||||
| Cohort | 1–2 | All studies | 5 | 2.34 (1.56–3.53) | 96% | |
| 1–2 | 1–2 | 1 | 3.00 (1.70–5.30) | - | ||
| 1–2 | =3 | 4 | 2.34 (1.54–3.54) | 97% |
| Exposure Parameters Estimated | Type of Studies | Exposure Score | Diagnostic Score | Number of Studies | Overall ES * (95% CI) | Heterogeneity of Studies (I2) |
|---|---|---|---|---|---|---|
| Heavy physical workload/heavy lifting | Prevalence studies | All studies | All studies | 4 | 1.69 (1.04–2.75) | 47% |
| 1–2 | 1–2 | 0 | - | - | ||
| All Studies | =3 | 3 | 2.02 (1.10–3.70) | 42% | ||
| ≥3 | All studies | 3 | 1.69 (0.97–2.94) | 65% | ||
| ≥3 | =3 | 2 | 2.03 (0.94–4.34) | 71% | ||
| Incidence studies | ||||||
| Case-control | ≥3 | =3 | 1 | 0.80 (0.40–1.50) | - | |
| Cohort | All studies | All studies | 3 | 1.06 (0.67–1.69) | 77% | |
| 1–2 | 1–2 | 0 | - | - | ||
| All Studies | =3 | 3 | 1.06 (0.67–1.69) | 77% | ||
| ≥3 | =3 | 2 | 1.01 (0.89–1.15) | 0% | ||
| Farmer | Prevalence studies | 1–2 | All studies | 1 | 0.62 (0.36–1.00) | - |
| 1–2 | 1–2 | 0 | - | - | ||
| 1–2 | =3 | 1 | 0.62 (0.36–1.00) | - | ||
| Incidence studies | ||||||
| Cohort | 1–2 | All studies | 2 | 1.22 (1.12–1.33) | 0% | |
| 1–2 | 1–2 | 0 | - | - | ||
| 1–2 | =3 | 2 | 1.22 (1.12–1.33) | 0% |
| Exposure Parameters Estimated | Independent Parameters in Meta-Regression Model * | β-Values of log (OR/RR) ** | Standard Error (SE) of β-Values |
|---|---|---|---|
| Heavy physical workload/heavy lifting (n = 22 studies) | Cohort study (yes vs. no) | −0.208 | 0.301 |
| Quality score of exposure assessment | −0.183 | 0.210 | |
| Quality score of case assessment | −0.121 | 0.305 | |
| BMI as confounder (yes vs. no) | −0.320 | 0.416 | |
| Prior injury as confounder (yes vs. no) | 0.565 | 0.368 | |
| Farmer (n =13 studies) | Cohort study (yes vs. no) | −0.877 | 0.375 |
| Quality score of exposure assessment | −0.762 | 0.323 | |
| Quality score of case assessment | −0.450 | 0.390 | |
| BMI as confounder (yes vs. no) | −0.503 | 0.587 | |
| Prior injury as confounder (yes vs. no) | −0.234 | 0.448 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Y.; Nold, A.; Glitsch, U.; Bochmann, F. Hip Osteoarthritis and Physical Workload: Influence of Study Quality on Risk Estimations—A Meta-Analysis of Epidemiological Findings. Int. J. Environ. Res. Public Health 2019, 16, 322. https://doi.org/10.3390/ijerph16030322
Sun Y, Nold A, Glitsch U, Bochmann F. Hip Osteoarthritis and Physical Workload: Influence of Study Quality on Risk Estimations—A Meta-Analysis of Epidemiological Findings. International Journal of Environmental Research and Public Health. 2019; 16(3):322. https://doi.org/10.3390/ijerph16030322
Chicago/Turabian StyleSun, Yi, Annette Nold, Ulrich Glitsch, and Frank Bochmann. 2019. "Hip Osteoarthritis and Physical Workload: Influence of Study Quality on Risk Estimations—A Meta-Analysis of Epidemiological Findings" International Journal of Environmental Research and Public Health 16, no. 3: 322. https://doi.org/10.3390/ijerph16030322