Digital Training for Non-Specialist Health Workers to Deliver a Brief Psychological Treatment for Depression in Primary Care in India: Findings from a Randomized Pilot Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Sample
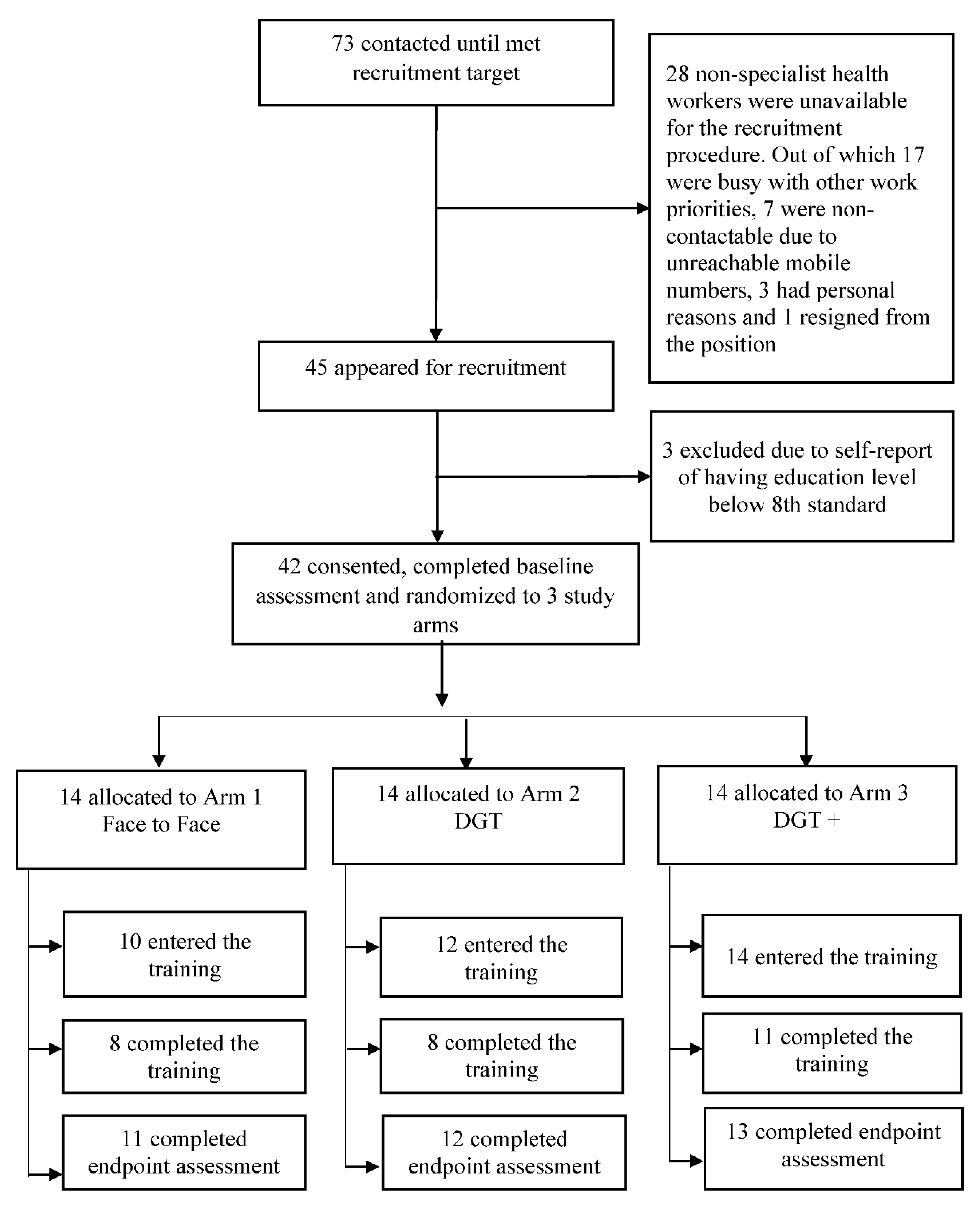
2.2. Recruitment Procedure
2.3. Randomization
2.4. Training Programs
2.4.1. Conventional Face-to-Face Training (F2F)
2.4.2. Digital Training (DGT)
2.4.3. Digital Training with Remote Support (DGT+)
2.5. Outcome Assessment
2.5.1. Acceptability and Feasibility Indicators
2.5.2. Preliminary Effectiveness Outcome
2.6. Data Analysis
3. Results
3.1. Acceptability and Feasibility Indicators
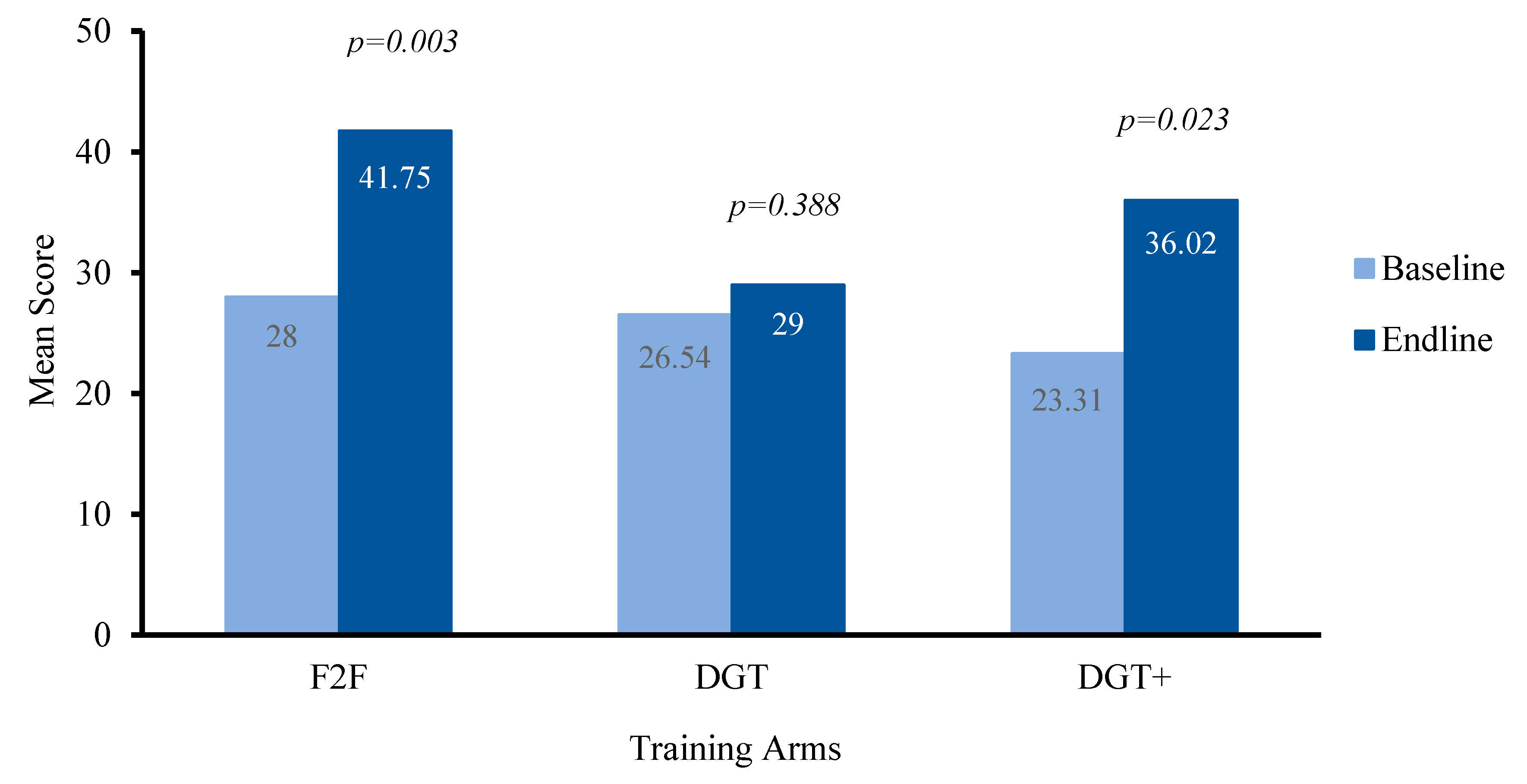
3.2. Preliminary Effectiveness Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sagar, R.; Dandona, R.; Gururaj, G.; Dhaliwal, R.; Singh, A.; Ferrari, A.; Dua, T.; Ganguli, A.; Varghese, M.; Chakma, J.K. The burden of mental disorders across the states of India: The Global Burden of Disease Study 1990–2017. Lancet Psychiatry 2020, 7, 148–161. [Google Scholar] [CrossRef] [Green Version]
- Arvind, B.A.; Gururaj, G.; Loganathan, S.; Amudhan, S.; Varghese, M.; Benegal, V.; Rao, G.N.; Kokane, A.M.; Chavan, B.; Dalal, P. Prevalence and socioeconomic impact of depressive disorders in India: Multisite population-based cross-sectional study. BMJ Open 2019, 9, e027250. [Google Scholar] [CrossRef] [PubMed]
- Pathare, S.; Brazinova, A.; Levav, I. Care gap: A comprehensive measure to quantify unmet needs in mental health. Epidemiol. Psychiatr. Sci. 2018, 27, 463–467. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.; Xiao, S.; Chen, H.; Hanna, F.; Jotheeswaran, A.; Luo, D.; Parikh, R.; Sharma, E.; Usmani, S.; Yu, Y. The magnitude of and health system responses to the mental health treatment gap in adults in India and China. Lancet 2016, 388, 3074–3084. [Google Scholar] [CrossRef]
- Kokane, A.; Pakhare, A.; Gururaj, G.; Varghese, M.; Benegal, V.; Rao, G.N.; Arvind, B.; Shukla, M.; Mitra, A.; Yadav, K. Mental Health Issues in Madhya Pradesh: Insights from National Mental Health Survey of India 2016. In Healthcare; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2019. [Google Scholar]
- World Health Organization. mhGAP Intervention Guide Mental Health Gap Action Programme Version 2.0 for Mental, Neurological and Substance use Disorders in Non-Specialized Health Settings; World Health Organization: Geneva, Switzerland, 2016; pp. 1–173.
- Fairburn, C.G.; Patel, V. The global dissemination of psychological treatments: A road map for research and practice. Am. J. Psychiatry 2014, 171, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Kazdin, A.E. Addressing the treatment gap: A key challenge for extending evidence-based psychosocial interventions. Behav. Res. Ther. 2017, 88, 7–18. [Google Scholar] [CrossRef]
- Raviola, G.; Naslund, J.A.; Smith, S.L.; Patel, V. Innovative Models in Mental Health Delivery Systems: Task Sharing Care with Non-specialist Providers to Close the Mental Health Treatment Gap. Curr. Psychiatry Rep. 2019, 21, 44. [Google Scholar] [CrossRef]
- Singla, D.R.; A Kohrt, B.; Murray, L.K.; Anand, A.; Chorpita, B.F.; Patel, V. Psychological Treatments for the World: Lessons from Low- and Middle-Income Countries. Annu. Rev. Clin. Psychol. 2017, 13, 149–181. [Google Scholar] [CrossRef] [Green Version]
- Hoeft, T.J.; Fortney, J.C.; Patel, V.; Unützer, J. Task-Sharing Approaches to Improve Mental Health Care in Rural and Other Low-Resource Settings: A Systematic Review. J. Rural. Heal. 2016, 34, 48–62. [Google Scholar] [CrossRef]
- Barbui, C.; Purgato, M.; Abdulmalik, J.; Acarturk, C.; Eaton, J.; Gastaldon, C.; Gureje, O.; Hanlon, C.; Jordans, M.; Lund, C.; et al. Efficacy of psychosocial interventions for mental health outcomes in low-income and middle-income countries: An umbrella review. Lancet Psychiatry 2020, 7, 162–172. [Google Scholar] [CrossRef]
- Ministry of Health & Family Welfare. New Pathways New Hope National Mental Health Policy of India; Ministry of Health & Family Welfare, Government of India: New Delhi, India, 2014.
- Ministry of Law and Justice. The Mental Health Care Act 2017; Ministry of Law and Justice, Government of India: New Delhi, India, 2017.
- Directorate General of Health Services. National Mental Health Programme; Ministry of Health & Family Welfare, Government of India: New Delhi, India, 2017.
- Ahuja, S.; Shidhaye, R.; Khan, A.; Roberts, T.; Jordans, M.; Thornicroft, G.; Petersen, I. Understanding mental health system governance in India: Perspectives of key stakeholders. Preprints 2020. [Google Scholar] [CrossRef]
- Barnett, M.L.; Lau, A.S.; Miranda, J. Lay health worker involvement in evidence-based treatment delivery: A conceptual model to address disparities in care. Annu. Rev. Clin. Psychol. 2018, 14, 185–208. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.L.; Gonzalez, A.; Miranda, J.; Chavira, D.A.; Lau, A.S. Mobilizing Community Health Workers to Address Mental Health Disparities for Underserved Populations: A Systematic Review. Adm. Policy Ment. Health 2018, 45, 195–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padmanathan, P.; De Silva, M.J. The acceptability and feasibility of task-sharing for mental healthcare in low and middle income countries: A systematic review. Soc. Sci. Med. 2013, 97, 82–86. [Google Scholar] [CrossRef]
- National Health Mission. Update on ASHA Programme; Ministry of Health and Family Welfare, Government of India: New Delhi, India, 2017.
- Ministry of Health and Family Welfare, Government of India. National Rural Health Mission; Ministry of Health and Family Welfare, Government of India: New Delhi, India, 2011.
- Ved, R.; Scott, K.; Gupta, G.; Ummer, O.; Singh, S.; Srivastava, A.; George, A. How are gender inequalities facing India’s one million ASHAs being addressed? Policy origins and adaptations for the world’s largest all-female community health worker programme. Hum. Resour. Health 2019, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- National Rural Health Mission. ASHA: Which way forward? Evaluation of ASHA Programme; National Rural Health Mission, National Health Systems Resource Center, National Institute of Health and Family Welfare, Government of India: New Delhi, India, 2011.
- Fairburn, C.G.; Cooper, Z. Therapist competence, therapy quality, and therapist training. Behav. Res. Ther. 2011, 49, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Naslund, J.A.; Shidhaye, R.; Patel, V. Digital Technology for Building Capacity of Nonspecialist Health Workers for Task Sharing and Scaling Up Mental Health Care Globally. Harv. Rev. Psychiatry 2019, 27, 181–192. [Google Scholar] [CrossRef]
- Naslund, J.A.; Aschbrenner, K.A.; Araya, R.; Marsch, L.A.; Unützer, J.; Patel, V.; Bartels, S.J. Digital technology for treating and preventing mental disorders in low-income and middle-income countries: A narrative review of the literature. Lancet Psychiatry 2017, 4, 486–500. [Google Scholar] [CrossRef] [Green Version]
- Keelery, S. Mobile Phone Internet Users in India 2015–2023. Available online: https://www.statista.com/statistics/558610/number-of-mobile-internet-user-in-india/ (accessed on 7 August 2020).
- Modi, D.; Dholakia, N.; Gopalan, R.; Venkatraman, S.; Dave, K.; Shah, S.; Desai, G.; Qazi, S.A.; Sinha, A.; Pandey, R.M. mHealth intervention “ImTeCHO” to improve delivery of maternal, neonatal, and child care services—A cluster-randomized trial in tribal areas of Gujarat, India. PloS Med. 2019, 16, e1002939. [Google Scholar] [CrossRef] [Green Version]
- Saha, S.; Kotwani, P.; Pandya, A.; Patel, C.; Shah, K.; Saxena, D.; Puwar, T.; Desai, S.; Patel, D.M.; Sethuraman, A. Addressing comprehensive primary healthcare in Gujarat through mHealth intervention: Early implementation experience with TeCHO+ programme. J. Fam. Med. Prim. Care 2020, 9, 340. [Google Scholar] [CrossRef]
- Rahman, A.; Akhtar, P.; Hamdani, S.U.; Atif, N.; Nazir, H.; Uddin, I.; Nisar, A.; Huma, Z.; Maselko, J.; Sikander, S. Using technology to scale-up training and supervision of community health workers in the psychosocial management of perinatal depression: A non-inferiority, randomized controlled trial. Glob. Ment. Health 2019, 6, e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maulik, P.K.; Kallakuri, S.; Devarapalli, S.; Vadlamani, V.K.; Jha, V.; Patel, A. Increasing use of mental health services in remote areas using mobile technology: A pre–post evaluation of the SMART Mental Health project in rural India. J. Glob. Health 2017, 7, 010408. [Google Scholar] [CrossRef] [PubMed]
- Shields-Zeeman, L.; Pathare, S.; Walters, B.H.; Kapadia-Kundu, N.; Joag, K. Promoting wellbeing and improving access to mental health care through community champions in rural India: The Atmiyata intervention approach. Int. J. Ment. Health Syst. 2017, 11, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonsalves, P.P.; Hodgson, E.S.; Kumar, A.; Aurora, T.; Chandak, Y.; Sharma, R.; Michelson, D.; Patel, V. Design and development of the ‘POD Adventures’ smartphone game: A blended problem-solving intervention for adolescent mental health in India. Front. Public Health 2019, 7, 238. [Google Scholar] [CrossRef] [PubMed]
- Muke, S.; Shrivastava, R.; Mitchell, L.; Khan, A.; Murhar, V.; Tugnawat, D.; Shidhaye, R.; Patel, V.; Naslund, J.A. Acceptability and feasibility of digital technology for training community health workers to deliver evidence-based psychosocial treatment for depression in rural India. Asian J. Psychiatry 2019, 45, 99–106. [Google Scholar] [CrossRef]
- Patel, V.; Weobong, B.; Weiss, H.A.; Anand, A.; Bhat, B.; Katti, B.; Dimidjian, S.; Araya, R.; Hollon, S.D.; King, M. The Healthy Activity Program (HAP), a lay counsellor-delivered brief psychological treatment for severe depression, in primary care in India: A randomised controlled trial. Lancet 2017, 389, 176–185. [Google Scholar] [CrossRef] [Green Version]
- Homitz, D.J.; Berge, Z.L. Using e-mentoring to sustain distance training and education. Learn. Organ. 2008, 15, 326–335. [Google Scholar] [CrossRef]
- Friedman, L.W.; Friedman, H. Using social media technologies to enhance online learning. J. Educ. Online 2013, 10, 1–22. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [Green Version]
- Directorate of Census Operations Madhya Pradesh. Census of India 2011: Provisional Population Totals Madhya Pradesh; Ministry of Home Affairs, Government of India: New Delhi, India, 2011.
- Suryanarayana, M.; Agrawal, A.; Seeta Prabhu, K. Inequality-Adjusted Human Development Index for India’s States; United Nations Development Programme (UNDP): New Delhi, India, 2011. [Google Scholar]
- Menon, P.; Deolalikar, A.; Bhaskar, A. India State Hunger Index: Comparisons of Hunger Across States; International Food Policy Research Institute: Washington, DC, USA, 2009. [Google Scholar]
- Billingham, S.A.; Whitehead, A.L.; Julious, S.A. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom Clinical Research Network database. BMC Med. Res. Methodol. 2013, 13, 104. [Google Scholar] [CrossRef] [Green Version]
- National Health Mission. Nation Health Mission (M.P.); National Health Mission: New Delhi, India, 2018.
- Saprii, L.; Richards, E.; Kokho, P.; Theobald, S. Community health workers in rural India: Analysing the opportunities and challenges Accredited Social Health Activists (ASHAs) face in realising their multiple roles. Hum. Resour. Health 2015, 13, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, K.; George, A.S.; Ved, R.R. Taking stock of 10 years of published research on the ASHA programme: Examining India’s national community health worker programme from a health systems perspective. Health Res. Policy Syst. 2019, 17, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satpathy, S. Indian public health standards (IPHS) for community health centres. Indian J. Public Health 2005, 49, 123–126. [Google Scholar] [PubMed]
- Directorate General of Health Services. Indian Public Health Standard (IPHS) For Community Health Centres (Revised 2010); Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India: New Delhi, India, 2010.
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, N.; Anand, A.; Dimidjian, S.; Shinde, S.; Weobong, B.; Balaji, M.; Hollon, S.D.; Rahman, A.; Wilson, G.T.; Verdeli, H. The Healthy Activity Program lay counsellor delivered treatment for severe depression in India: Systematic development and randomised evaluation. Br. J. Psychiatry 2016, 208, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weobong, B.; Weiss, H.A.; McDaid, D.; Singla, D.R.; Hollon, S.D.; Nadkarni, A.; Park, A.-L.; Bhat, B.; Katti, B.; Anand, A. Sustained effectiveness and cost-effectiveness of the Healthy Activity Programme, a brief psychological treatment for depression delivered by lay counsellors in primary care: 12-month follow-up of a randomised controlled trial. PLoS Med. 2017, 14, e1002385. [Google Scholar] [CrossRef] [PubMed]
- Walker, I.F.; Khanal, S.; Hicks, J.P.; Lamichhane, B.; Thapa, A.; Elsey, H.; Baral, S.C.; Newell, J.N. Implementation of a psychosocial support package for people receiving treatment for multidrug-resistant tuberculosis in Nepal: A feasibility and acceptability study. PLoS ONE 2018, 13, e0201163. [Google Scholar] [CrossRef] [Green Version]
- Jordans, M.J.; Luitel, N.P.; Garman, E.; Kohrt, B.A.; Rathod, S.D.; Shrestha, P.; Komproe, I.H.; Lund, C.; Patel, V. Effectiveness of psychological treatments for depression and alcohol use disorder delivered by community-based counsellors: Two pragmatic randomised controlled trials within primary healthcare in Nepal. Br. J. Psychiatry 2019, 215, 485–493. [Google Scholar] [CrossRef] [Green Version]
- Shidhaye, R.; Baron, E.; Murhar, V.; Rathod, S.; Khan, A.; Singh, A.; Shrivastava, S.; Muke, S.; Shrivastava, R.; Lund, C. Community, facility and individual level impact of integrating mental health screening and treatment into the primary healthcare system in Sehore district, Madhya Pradesh, India. BMJ Glob. Health 2019, 4, e001344. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Shrivastava, R.; Tugnawat, D.; Singh, A.; Dimidjian, S.; Patel, V.; Bhan, A.; Naslund, J.A. Design and Development of a Digital Program for Training Non-specialist Health Workers to Deliver an Evidence-Based Psychological Treatment for Depression in Primary Care in India. J. Technol. Behav. Sci. 2020. [Google Scholar] [CrossRef]
- Jones, B.D. User Guide for Assessing the Components of the MUSIC® Model of Motivation. Available online: https://www.themusicmodel.com/ (accessed on 15 November 2018).
- Jones, B.D. Motivating students to engage in learning: The MUSIC model of academic motivation. International. J. Teach. Learn. High. Educ. 2009, 21, 272–285. [Google Scholar]
- Jones, B.D. An examination of motivation model components in face-to-face and online instruction. Electron. J. Res. Educ. Psychol. 2010, 8, 915–944. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.D. Motivating Students by Design: Practical Strategies for Professors, 2nd ed.; CreateSpace: Charleston, SC, USA, 2018. [Google Scholar]
- Cooper, Z.; Doll, H.; Bailey-Straebler, S.; Bohn, K.; de Vries, D.; Murphy, R.; O’Connor, M.E.; Fairburn, C.G. Assessing therapist competence: Development of a performance-based measure and its comparison with a web-based measure. JMIR Ment. Health 2017, 4, e51. [Google Scholar] [CrossRef] [PubMed]
- Restivo, J.L.; Mitchell, L.; Joshi, U.; Anand, A.; Gugiu, P.C.; Hollon, S.D.; Singla, D.R.; Patel, V.; Naslund, J.A.; Cooper, Z. Assessing health worker competence to deliver a brief psychological treatment for depression: Development and validation of a scalable measure. J. Behav. Cogn. Ther. 2020, in press. [Google Scholar]
- Popham, W.J. Teaching to the Test? Educ. Leadersh. 2001, 58, 16–21. [Google Scholar]
- Yardley, L.; Morrison, L.; Bradbury, K.; Muller, I. The person-based approach to intervention development: Application to digital health-related behavior change interventions. J. Med. Internet Res. 2015, 17, e30. [Google Scholar] [CrossRef]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Rey, D.; Neuhäuser, M. Wilcoxon-Signed-Rank Test. In International Encyclopedia of Statistical Science; Gibbons, J.D., Chakraborti, S., Eds.; Springer: Berlin, Germany, 2011; pp. 1658–1659. [Google Scholar]
- Naslund, J.A.; Gonsalves, P.P.; Gruebner, O.; Pendse, S.R.; Smith, S.L.; Sharma, A.; Raviola, G. Digital Innovations for Global Mental Health: Opportunities for Data Science, Task Sharing, and Early Intervention. Curr. Treat. Options Psychiatry 2019, 6, 337–351. [Google Scholar] [CrossRef]
- Mohr, D.C.; Lyon, A.R.; Lattie, E.G.; Reddy, M.; Schueller, S.M. Accelerating digital mental health research from early design and creation to successful implementation and sustainment. J. Med. Internet Res. 2017, 19, e153. [Google Scholar] [CrossRef]
- Merchant, R.; Torous, J.; Rodriguez-Villa, E.; Naslund, J.A. Digital technology for management of severe mental disorders in low-income and middle-income countries. Curr. Opin. Psychiatry 2020, 33, 501–507. [Google Scholar] [CrossRef]
- Winters, N.; Langer, L.; Nduku, P.; Robson, J.; O’Donovan, J.; Maulik, P.; Paton, C.; Geniets, A.; Peiris, D.; Nagraj, S. Using mobile technologies to support the training of community health workers in low-income and middle-income countries: Mapping the evidence. BMJ Glob. Health 2019, 4, e001421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winters, N.; Langer, L.; Geniets, A. Scoping review assessing the evidence used to support the adoption of mobile health (mHealth) technologies for the education and training of community health workers (CHWs) in low-income and middle-income countries. BMJ Open 2018, 8, e019827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biemba, G.; Chiluba, B.; Yeboah-Antwi, K.; Silavwe, V.; Lunze, K.; Mwale, R.K.; Russpatrick, S.; Hamer, D.H. A mobile-based community health management information system for community health workers and their supervisors in 2 districts of Zambia. Glob. Health Sci. Pract. 2017, 5, 486–494. [Google Scholar] [CrossRef] [Green Version]
- Keogh-Brown, M.; Bachmann, M.; Shepstone, L.; Hewitt, C.; Howe, A.; Ramsay, C.R.; Song, F.; Miles, J.; Torgerson, D.; Miles, S. Contamination in trials of educational interventions. Health Technol. Assess. 2007, 11, ix-107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemp, C.G.; Petersen, I.; Bhana, A.; Rao, D. Supervision of Task-Shared Mental Health Care in Low-Resource Settings: A Commentary on Programmatic Experience. Glob. Health: Sci. Pract. 2019, 7, 150–159. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Socio-Demographic Characteristics | F2F n | DGT n | DGT+ n | p-Value |
|---|---|---|---|---|
| n = 14 | n = 14 | n = 14 | ||
| Gender | 1 | |||
| Female | 11 (79%) | 11 (79%) | 11 (79%) | |
| Male | 3 (21%) | 3 (21%) | 3 (21%) | |
| Designation | 1 | |||
| ASHA | 8 (57%) | 7 (50%) | 8 (57%) | |
| ASHA Facilitator | 3 (21%) | 4 (29%) | 3 (21%) | |
| MPW | 3 (21%) | 3 (21%) | 3 (21%) | |
| Education | 0.51 | |||
| 8th to 10th | 8 (57%) | 9 (64%) | 6 (43%) | |
| Above 10th | 6 (43%) | 5 (36%) | 8 (57%) | |
| Experience in years mean (95% CI) * | 9.73 (6.71, 12.76) | 8.96 (5.37, 12.55) | 8.38 (5.32, 11.44) | 0.8153 |
| Age in years mean (95% CI) * | 36.07 (31.34, 40.80) | 37.71 (32.43, 42.99) | 36 (31.31, 40.68) | 0.8341 |
| Type of mobile phone owned # | 0.931 | |||
| Ordinary mobile phone | 7 (50%) | 6 (43%) | 6 (43%) | |
| Smartphone | 7 (50%) | 7 (50%) | 8 (57%) | |
| Family Size (number of persons in household) mean (95% CI) | 5.3 (4.19, 6.42) | 4.85 (3.07,6.63) | 5.35 (3.62, 7.09) | 0.868 |
| Previous Experience in Mental Health Training ** | (n = 11) | (n = 12) | (n = 14) | 0.591 |
| Yes | 5 (46%) | 8 (67%) | 8 (57%) | |
| No | 6 (54%) | 4 (33%) | 6 (43%) | |
| How many years before took part in the training mean (95% CI) * | 3 (0.67, 5.32) | 3 (2.22, 3.77) | 3.13 (1.6, 4.66) | 0.9814 |
| Number of Participants | F2F (n = 14) | DGT (n = 14) | DGT+ (n = 14) |
|---|---|---|---|
| Started the training | 10 (71%) | 12 (86%) | 14 (100%) |
| Completed the full training (all modules) | 8 (57%) | 8 (57%) | 11 (79%) |
| Did not complete all of the modules in the training | 2 (14%) | 4 (29%) | 3 (21%) |
| Number of phone calls made by participants for seeking technical assistance | NA | 149 | 57 |
| Number of phone calls made by the research team to participants for follow up on their queries | NA | 106 | 87 |
| Registered Queries by Phone | Specific Technical Challenges Encountered |
|---|---|
| Internet related |
|
| Smartphone handling related |
|
| Moodle Learning Management System app related |
|
| Course navigation related |
|
| Smartphone hardware/software related |
|
| Domains of Satisfaction and Acceptability (F2F and DGT) | Study Arms | ||
|---|---|---|---|
| F2F (n = 11) | DGT (n = 12) | DGT+ (n = 13) | |
| Mean (SD) | Mean (SD) | Mean (SD) | |
| Acceptability | 5.6 (0.44) | 5.2 (1.10) | 5.5 (0.52) |
| The instructor was available to answer my questions about the coursework (F2F)./I could find answers to questions I had about the coursework (DGT). | 5.6 (0.51) | 5.1 (1.16) | 5.5 (0.51) |
| The instructor was willing to assist me if I needed help in the course (F2F)./Answers to questions about the coursework were easy to understand (DGT). | 5.4 (0.51) | 5.3 (1.40) | 5.2 (1.14) |
| The instructor cared about how well I did in this course (F2F)./The instructor in the recorded lecture cared about helping me to learn (DGT). | 5.4 (1.26) | 5.3 (1.21) | 5.5 (0.66) |
| The instructor was respectful of me (F2F)./The instructor in the recorded lecture used a respectful tone (DGT). | 5.7 (0.48) | 5.3 (1.21) | 5.5 (0.66) |
| The instructor was friendly (F2F)./The instructor in the recorded lecture used a friendly tone (DGT). | 5.7 (0.48) | 4.8 (1.40) | 5.2 (1.16) |
| I believe that the instructor cared about my feelings (F2F)./The recorded lecture used familiar language and expressions (DGT). | 5.6 (0.51) | 5.4 (1.24) | 5.8 (0.6) |
| Appropriateness | 4.9 (0.57) | 5.0 (0.74) | 5.1 (0.64) |
| The coursework held my attention (F2F/DGT). | 5.4 (0.51) | 5.3 (0.65) | 5.3 (1.10) |
| The instructional methods used in this course held my attention (F2F/DGT). | 4.9 (1.59) | 5.0 (1.27) | 4.9 (1.38) |
| I enjoyed the instructional methods used in this course (F2F/DGT). | 5.3 (0.48) | 5.3 (0.98) | 5.5 (0.77) |
| The instructional methods engaged me in the course (F2F/DGT). | 2.7 (1.88) | 3.3 (1.82) | 4.0 (1.77) |
| I enjoyed completing the coursework (F2F/DGT). | 5.7 (0.48) | 5.3 (1.13) | 5.5 (0.66) |
| The coursework was interesting to me (F2F/DGT). | 5.5 (0.52) | 5.6 (0.66) | 5.5 (0.51) |
| Adoption | 5.5 (0.38) | 5.5 (0.79) | 5.6 (0.43) |
| In general, the coursework was useful to me (F2F/DGT). | 5.2 (0.42) | 5.5 (0.52) | 5.5 (0.51) |
| The coursework was beneficial to me (F2F/DGT). | 5.3 (0.48) | 5.7 (0.65) | 5.7 (0.48) |
| I found the coursework to be relevant to my future (F2F/DGT). | 5.7 (0.48) | 5.4 (0.79) | 5.6 (0.50) |
| I will be able to use the knowledge I gained in this course (F2F/DGT). | 5.6 (0.51) | 5.4 (1.24) | 5.6 (0.50) |
| The knowledge I gained in this course is important for my future (F2F/DGT). | 5.6 (0.51) | 5.6 (1.16) | 5.6 (0.50) |
| Feasibility | 5.2 (0.40) | 5.4 (0.81) | 5.5 (0.42) |
| I had the opportunity to decide for myself how to meet the course goals (F2F/DGT). | 4.9 (1.10) | 5.7 (0.49) | 5.8 (0.43) |
| I was confident that I could succeed in the coursework (F2F/DGT). | 5.1 (1.19) | 5.3 (1.21) | 5.6 (0.50) |
| I had the freedom to complete the coursework my own way (F2F/DGT). | 5.4 (0.51) | 5.3 (0.65) | 5.8 (0.43) |
| I felt that I could be successful in meeting the academic challenges in this course (F2F/DGT). | 5.3 (0.48) | 5.2 (1.19) | 5.2 (1.21) |
| I had options on how to achieve the goals of the course (F2F/DGT). | 4.4 (1.26) | 5.4 (0.79) | 5.2 (1.09) |
| I was capable of getting a high grade in this course (F2F/DGT). | 5.5 (0.52) | 5.0 (1.53) | 5.5 (0.66) |
| I had control over how I learned the course content (F2F/DGT). | 5.0 (1.15) | 5.2 (1.33) | 5.5 (0.66) |
| Throughout the course, I felt that I could be successful on the coursework (F2F/DGT). | 5.3 (0.48) | 5.4 (1.16) | 5.6 (0.51) |
| I had flexibility in what I was allowed to do in this course (F2F/DGT). | 5.5 (0.52) | 5.8 (0.38) | 5.6 (0.51) |
| Focus Group Discussion Themes | F2F (n = 8) | DGT (n = 9) and DGT+ (n = 11) |
|---|---|---|
| Acceptability | ||
| Facilitators |
|
|
| Challenges and/or suggestions to address the challenges |
| |
| Appropriateness | ||
| Facilitators |
|
|
| Challenges and/or suggestions to address challenges |
|
|
| Adoption | ||
| Facilitators |
|
|
| Challenges and/or suggestions to address challenges |
| |
| Feasibility | ||
| Facilitators |
| |
| Challenges and/or suggestions to address challenges |
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muke, S.S.; Tugnawat, D.; Joshi, U.; Anand, A.; Khan, A.; Shrivastava, R.; Singh, A.; Restivo, J.L.; Bhan, A.; Patel, V.; et al. Digital Training for Non-Specialist Health Workers to Deliver a Brief Psychological Treatment for Depression in Primary Care in India: Findings from a Randomized Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 6368. https://doi.org/10.3390/ijerph17176368
Muke SS, Tugnawat D, Joshi U, Anand A, Khan A, Shrivastava R, Singh A, Restivo JL, Bhan A, Patel V, et al. Digital Training for Non-Specialist Health Workers to Deliver a Brief Psychological Treatment for Depression in Primary Care in India: Findings from a Randomized Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(17):6368. https://doi.org/10.3390/ijerph17176368
Chicago/Turabian StyleMuke, Shital S., Deepak Tugnawat, Udita Joshi, Aditya Anand, Azaz Khan, Ritu Shrivastava, Abhishek Singh, Juliana L. Restivo, Anant Bhan, Vikram Patel, and et al. 2020. "Digital Training for Non-Specialist Health Workers to Deliver a Brief Psychological Treatment for Depression in Primary Care in India: Findings from a Randomized Pilot Study" International Journal of Environmental Research and Public Health 17, no. 17: 6368. https://doi.org/10.3390/ijerph17176368