Effectiveness of Gas and Chimney Biomass Stoves for Reducing Household Air Pollution Pregnancy Exposure in Guatemala: Sociodemographic Effect Modifiers

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Site and Population
2.2. Stove Use and Other Sources of HAP Exposure
2.3. Personal Exposure Assessment
2.4. Estimation of Pregnancy Average Concentration for PM2.5
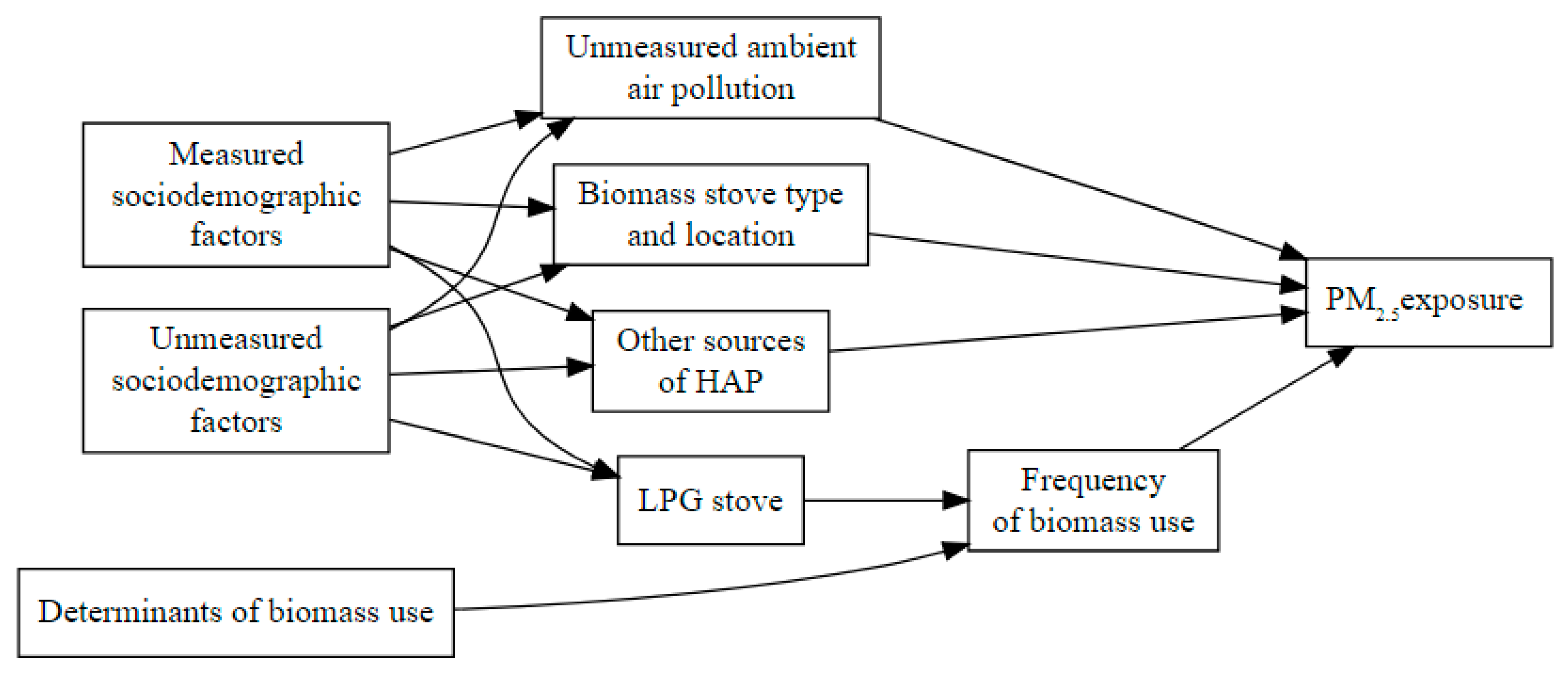
2.5. Directed Acyclic Graph (DAG)
2.6. Analyses to Estimate the Effectiveness of Stove Ownership
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Balakrishnan, K.; Mehta, S. Population Levels of Household Air Pollution and Exposures; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Balakrishnan, K.; Ghosh, S.; Ganguli, B.; Sambandam, S.; Bruce, N.; Barnes, D.F.; Smith, K.R. State and national household concentrations of PM2.5 from solid cookfuel use: Results from measurements and modeling in India for estimation of the global burden of disease. Environ. Health 2013, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Boy, E.; Bruce, N.; Delgado, H. Birth weight and exposure to kitchen wood smoke during pregnancy in rural Guatemala. Environ. Health Perspect. 2002, 110, 109–114. [Google Scholar] [CrossRef]
- Tielsch, J.M.; Katz, J.; Thulasiraj, R.D.; Coles, C.L.; Sheeladevi, S.; Yanik, E.L.; Rahmathullah, L. Exposure to indoor biomass fuel and tobacco smoke and risk of adverse reproductive outcomes, mortality, respiratory morbidity and growth among newborn infants in south India. Int. J. Epidemiol. 2009, 38, 1351–1363. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.M.; Bruce, N.; Eskenazi, B.; Diaz, A.; Pope, D.; Smith, K.R. Impact of reduced maternal exposures to wood smoke from an introduced chimney stove on newborn birth weight in rural Guatemala. Environ. Health Perspect. 2011, 119, 1489–1494. [Google Scholar] [CrossRef]
- Amegah, A.K.; Quansah, R.; Jaakkola, J.J. Household air pollution from solid fuel use and risk of adverse pregnancy outcomes: A systematic review and meta-analysis of the empirical evidence. PLoS ONE 2014, 9, e113920. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.P.; Mishra, V.; Thompson, L.; Siddiqui, A.R.; Rehfuess, E.A.; Weber, M.; Bruce, N.G. Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol. Rev. 2010, 32, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, K.; Ghosh, S.; Thangavel, G.; Sambandam, S.; Mukhopadhyay, K.; Puttaswamy, N.; Sadasivam, A.; Ramaswamy, P.; Johnson, P.; Kuppuswamy, R.; et al. Exposures to fine particulate matter (PM2.5) and birthweight in a rural-urban, mother-child cohort in Tamil Nadu, India. Environ. Res. 2018, 161, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Shezi, B.; Jafta, N.; Naidoo, R.N. Exposure assessment of indoor particulate matter during pregnancy: A narrative review of the literature. Rev. Environ. Health 2020. Available online: https://www.degruyter.com/view/journals/reveh/ahead-of-print/article-10.1515-reveh-2020-0009/article-10.1515-reveh-2020-0009.xml (accessed on 20 October 2020).
- Wu, J.; Xiao, X.; Li, Y.; Yang, F.; Yang, S.; Sun, L.; Ma, R.; Wang, M.C. Personal exposure to fine particulate matter (PM2.5) of pregnant women during three trimesters in rural Yunnan of China. Environ. Pollut. 2020, 256, 113055. [Google Scholar] [CrossRef] [PubMed]
- St Helen, G.; Aguilar-Villalobos, M.; Adetona, O.; Cassidy, B.; Bayer, C.W.; Hendry, R.; Hall, D.B.; Naeher, L.P. Exposure of pregnant women to cookstove-related household air pollution in urban and periurban Trujillo, Peru. Arch. Environ. Occup. Health 2015, 70, 10–18. [Google Scholar] [CrossRef]
- Clasen, T.; Checkley, W.; Peel, J.L.; Balakrishnan, K.; McCracken, J.P.; Rosa, G.; Thompson, L.M.; Barr, D.B.; Clark, M.L.; Johnson, M.A.; et al. Design and Rationale of the HAPIN Study: A Multicountry Randomized Controlled Trial to Assess the Effect of Liquefied Petroleum Gas Stove and Continuous Fuel Distribution. Environ. Health Perspect. 2020, 128, 47008. [Google Scholar] [CrossRef] [PubMed]
- Wylie, B.J.; Kishashu, Y.; Matechi, E.; Zhou, Z.; Coull, B.; Abioye, A.I.; Dionisio, K.L.; Mugusi, F.; Premji, Z.; Fawzi, W.; et al. Maternal exposure to carbon monoxide and fine particulate matter during pregnancy in an urban Tanzanian cohort. Indoor Air 2017, 27, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.; Bruce, N.; Dherani, M.; Jagoe, K.; Rehfuess, E. Real-life effectiveness of ‘improved’ stoves and clean fuels in reducing PM2.5 and CO: Systematic review and meta-analysis. Environ. Int. 2017, 101, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Naeher, L.P.; Leaderer, B.P.; Smith, K.R. Particulate matter and carbon monoxide in highland Guatemala: Indoor and outdoor levels from traditional and improved wood stoves and gas stoves. Indoor Air 2000, 10, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.A.; Chiang, R.A. Quantitative Guidance for Stove Usage and Performance to Achieve Health and Environmental Targets. Environ. Health Perspect. 2015, 123, 820–826. [Google Scholar] [CrossRef]
- Siddiqui, A.R.; Lee, K.; Bennett, D.; Yang, X.; Brown, K.H.; Bhutta, Z.A.; Gold, E.B. Indoor carbon monoxide and PM2.5 concentrations by cooking fuels in Pakistan. Indoor Air 2009, 19, 75–82. [Google Scholar] [CrossRef]
- Albalak, R.; Bruce, N.; McCracken, J.P.; Smith, K.R.; De Gallardo, T. Indoor respirable particulate matter concentrations from an open fire, improved cookstove, and LPG/open fire combination in a rural Guatemalan community. Environ. Sci. Technol. 2001, 35, 2650–2655. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Wang, S.; Aunan, K.; Zhao, M.; Chen, L.; Liu, Z.; Hansen, M.H. Personal exposure to PM2.5 in Chinese rural households in the Yangtze River Delta. Indoor Air 2019, 29, 403–412. [Google Scholar] [CrossRef]
- Baumgartner, J.; Schauer, J.J.; Ezzati, M.; Lu, L.; Cheng, C.; Patz, J.; Bautista, L.E. Patterns and predictors of personal exposure to indoor air pollution from biomass combustion among women and children in rural China. Indoor Air 2011, 21, 479–488. [Google Scholar] [CrossRef]
- Estevez-Garcia, J.A.; Schilmann, A.; Riojas-Rodriguez, H.; Berrueta, V.; Blanco, S.; Villasenor-Lozano, C.G.; Flores-Ramirez, R.; Cortez-Lugo, M.; Perez-Padilla, R. Women exposure to household air pollution after an improved cookstove program in rural San Luis Potosi, Mexico. Sci. Total Environ. 2020, 702, 134456. [Google Scholar] [CrossRef]
- Hollada, J.; Williams, K.N.; Miele, C.H.; Danz, D.; Harvey, S.A.; Checkley, W. Perceptions of Improved Biomass and Liquefied Petroleum Gas Stoves in Puno, Peru: Implications for Promoting Sustained and Exclusive Adoption of Clean Cooking Technologies. Int. J. Environ. Res. Public Health 2017, 14, 182. [Google Scholar] [CrossRef]
- Thompson, L.M.; Hengstermann, M.; Weinstein, J.R.; Diaz-Artiga, A. Adoption of Liquefied Petroleum Gas Stoves in Guatemala: A Mixed-Methods Study. EcoHealth 2018, 15, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Gould, C.F.; Urpelainen, J. The Role of Education and Attitudes in Cooking Fuel Choice: Evidence from two states in India. Energy Sustain. Dev. 2020, 54, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.; Bruce, N.; Higgerson, J.; Hyseni, L.; Ronzi, S.; Stanistreet, D.; Mbatchou, B.; Puzzolo, E. Household Determinants of Liquified Petroleum Gas (LPG) as a Cooking Fuel in South West Cameroon. EcoHealth 2018, 15, 729–743. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, K.; Sambandam, S.; Ghosh, S.; Mukhopadhyay, K.; Vaswani, M.; Arora, N.K.; Jack, D.; Pillariseti, A.; Bates, M.N.; Smith, K.R. Household Air Pollution Exposures of Pregnant Women Receiving Advanced Combustion Cookstoves in India: Implications for Intervention. Ann. Glob. Health 2015, 81, 375–385. [Google Scholar] [CrossRef]
- Wilson, D.L.; Williams, K.N.; Pillarisetti, A. An integrated sensor data logging, survey, and analytics platform for field research and its application in HAPIN, a multi-center household energy intervention trial. Sustainability 2020, 12, 1805. [Google Scholar] [CrossRef]
- Weinstein, J.R.; Thompson, L.M.; Diaz Artiga, A.; Bryan, J.P.; Arriaga, W.E.; Omer, S.B.; McCracken, J.P. Determining gestational age and preterm birth in rural Guatemala: A comparison of methods. PLoS ONE 2018, 13, e0193666. [Google Scholar] [CrossRef]
- Rutstein, S.O. Steps to Constructing the New DHS Wealth Index. Available online: https://dhsprogram.com/programming/wealth%20index/Steps_to_constructing_the_new_DHS_Wealth_Index.pdf (accessed on 10 October 2020).
- WHO. WHO Indoor Air Quality Guidelines: Household Fuel Combustion; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Wolak, M.E.; Fairbairn, D.J.; Paulsen, Y.R. Guidelines for Estimating Repeatability. Methods Ecol. Evol. 2015, 3, 129–137. [Google Scholar] [CrossRef]
- Liu, X.-Q.; Rong, J.-Y.; Liu, X.-Y. Best linear unbiased prediction for linear combinations in general mixed linear models. J. Multivar. Anal. 2008, 99, 1503–1517. [Google Scholar] [CrossRef]
- Pinheiro, J.; Bates, D. Mixed-Effects Models in S and S-PLUS; Springer Science & Business Media: Berlin, Germany, 2006. [Google Scholar]
- Textor, J.; vad der Zander, B.; Gilthorpe, M.K.; Liskiewicz, M.; Ellison, G.T.H. Robust causal inference using directed acyclic graphs: The R package “dagitty”. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef]
- Ruiz-Mercado, I.; Masera, O. Patterns of stove use in the context of fuel-device stacking: Rationale and implications. EcoHealth 2015, 12, 42–56. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.M.; Diaz-Artiga, A.; Weinstein, J.R.; Handley, M.A. Designing a behavioral intervention using the COM-B model and the theoretical domains framework to promote gas stove use in rural Guatemala: A formative research study. BMC Public Health 2018, 18, 253. [Google Scholar] [CrossRef] [PubMed]
- Puzzolo, E.; Pope, D.; Stanistreet, D.; Rehfuess, E.A.; Bruce, N.G. Clean fuels for resource-poor settings: A systematic review of barriers and enablers to adoption and sustained use. Environ. Res. 2016, 146, 218–234. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.J.; Pattanayak, S.K. Who adopts improved fuels and cookstoves? A systematic review. Environ. Health Perspect. 2012, 120, 637–645. [Google Scholar] [CrossRef]
- Heltberg, R. Factors determining household fuel choice in Guatemala. Environ. Dev. Econ. 2005, 10, 337–361. [Google Scholar] [CrossRef]
- McCracken, J.P.; Schwartz, J.; Bruce, N.; Mittleman, M.; Ryan, L.M.; Smith, K.R. Combining individual- and group-level exposure information: Child carbon monoxide in the Guatemala woodstove randomized control trial. Epidemiology 2009, 20, 127–136. [Google Scholar] [CrossRef]
- Sanchez, M.; Mila, C.; Sreekanth, V.; Balakrishnan, K.; Sambandam, S.; Nieuwenhuijsen, M.; Kinra, S.; Marshall, J.D.; Tonne, C. Personal exposure to particulate matter in peri-urban India: Predictors and association with ambient concentration at residence. J. Expo. Sci. Environ. Epidemiol. 2019, 139, 105735. [Google Scholar] [CrossRef] [PubMed]
- Dionisio, K.L.; Howie, S.R.; Dominici, F.; Fornace, K.M.; Spengler, J.D.; Donkor, S.; Chimah, O.; Oluwalana, C.; Ideh, R.C.; Ebruke, B.; et al. The exposure of infants and children to carbon monoxide from biomass fuels in The Gambia: A measurement and modeling study. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 173–181. [Google Scholar] [CrossRef]
- Wafula, E.M.; Onyango, F.E.; Thairu, H.; Boleij, J.S.; Hoek, F.; Ruigewaard, P.; Kagwanja, S.; De Koning, H.; Pio, A.; Kimani, E.; et al. Indoor air pollution in a Kenyan village. East Afr. Med. J. 1990, 67, 24–32. [Google Scholar]
- Saksena, S.; Prasad, R.; Pal, R.; Joshi, V. Patterns of daily exposure to TSP and CO in the Garhwal Himalaya. Atmos. Environ. Part A Gen. Top. 1992, 26, 2125–2134. [Google Scholar] [CrossRef]
- Peel, J.L.; Baumgartner, J.; Wellenius, G.A.; Clark, M.L.; Smith, K.R. Are Randomized Trials Necessary to Advance Epidemiologic Research on Household Air Pollution? Curr. Epidemiol. Rep. 2015, 2, 263–270. [Google Scholar] [CrossRef]
- INE. National Population and Household Census; National Institute of Statistics of Guatemala: Guatemala City, Guatemala, 2018. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Sociodemographic or Environmental Characteristics | LPG Stove n = 59 | No LPG Stove n = 159 |
|---|---|---|
| Maternal Age Group, Years, n (%) | ||
| 18 to 20 | 11 (19) | 41 (26) |
| 21 to 30 | 35 (59) | 80 (50) |
| 31 to 40 | 13 (22) | 38 (24) |
| Education, Years, Median (IQR 1) | 9 (6–10) | 4 (2–6) |
| Spanish Spoken in Household, n (%) | 30 (51) | 23 (15) |
| Urban Residence 2, n (%) | 16 (27) | 12 (8) |
| Wealth Quartile, n (%) | ||
| Low | 10 (17) | 55 (35) |
| Low–Medium | 7 (12) | 55 (35) |
| Medium–High | 13 (22) | 26 (16) |
| High | 29 (49) | 23 (14) |
| Crowding, n (%) 3 | 11 (19) | 66 (42) |
| Wood-Fired Sauna Bath, n (%) | 50 (85) | 153 (96) |
| Secondhand Smoke, n (%) | 17 (29) | 32 (20) |
| Electricity, n (%) | 57 (97) | 139 (87) |
| Characteristics of Biomass Use | Overall 559 (100%) | LPG Stove 149 (27%) | No LPG Stove 410 (73%) |
|---|---|---|---|
| Number of Biomass Stoves | |||
| 0 | 14 (3) | 14 (9) | 0 (0) |
| 1 | 442 (79) | 116 (78) | 326 (80) |
| 2 or 3 | 103 (18) | 19 (13) | 84 (20) |
| Biomass Stove Types 1 | |||
| Chimney Stove | 390 (70) | 113 (76) | 277 (68) |
| Open Fire Stove | 236 (42) | 35 (23) | 201 (49) |
| Main Biomass Stove | |||
| Chimney Stove | 387 (69) | 113 (76) | 274 (67) |
| Open Fire Stove | 158 (28) | 22 (15) | 136 (33) |
| Frequency of Biomass Use | |||
| ≥5 Times per Week | 502 (90) | 98 (66) | 404 (99) |
| <5 Times per Week | 43 (8) | 37 (25) | 6 (1) |
| Cooks Inside Main House with Biomass | 172 (31) | 61 (41) | 111 (27) |
| Median Hours/Day Cooking with Biomass (IQR 2) | 3.0 (2.0–4.0) | 3.0 (1.8–4.0) | 3.0 (3.0–4.0) |
| Descriptors of Personal Exposure | Overall | LPG Stove | No LPG Stove | Chimney Stove 3 | No Chimney Stove 3 |
|---|---|---|---|---|---|
| Subjects | 218 | 59 | 159 | 118 | 60 |
| Measures | 559 | 149 | 410 | 277 | 133 |
| Minimum | 10 | 10 | 11 | 11 | 13 |
| Median (IQR 1) | 79 (47, 137) | 55 (34, 79) | 96 (56, 160) | 78 (51, 125) | 148 (90, 249) |
| Geometric Mean (95% CI) | 83 (78, 89) | 54 (49, 60) | 98 (91, 105) | 80 (74, 87) | 146 (127, 169) |
| Maximum | 1052 | 284 | 1052 | 585 | 1052 |
| Between-Participant Variance | 0.33 | 0.20 | 0.29 | 0.18 | 0.26 |
| Within-Participant Variance | 0.32 | 0.23 | 0.33 | 0.29 | 0.43 |
| ICC 2 (95% CI) | 0.51 (0.42–0.59) | 0.46 (0.27–0.62) | 0.46 (0.36–0.56) | 0.39 (0.25–0.52) | 0.37 (0.16–0.56) |
| Estimate of Exposure | Ownership of Stove | LPG Stove | Chimney Stove 1 | ||
|---|---|---|---|---|---|
| Mean (SD) µg/m3 | n Meeting AQG (%) | Mean (SD) µg/m3 | n Meeting AQG (%) | ||
| 24-h Averages 2 | Owners | 76 (64) | 39 (25) | 105 (89) | 27 (10) |
| n = 559 | Non-owner | 133 (130) | 34 (8) | 192 (169) | 5 (3) |
| Subject Mean 3 | Owners | 56 (51) | 11 (19) | 81 (75) | 7 (6) |
| n = 218 | Non-owner | 96 (101) | 7 (4) | 138 (123) | 1 (2) |
| Typical Exposures 4 | Owners | 57 (33) | 7 (12) | 81 (34) | 0 (0) |
| n = 218 | Non-owner | 96 (53) | 0 (0) | 139 (61) | 0 (0) |
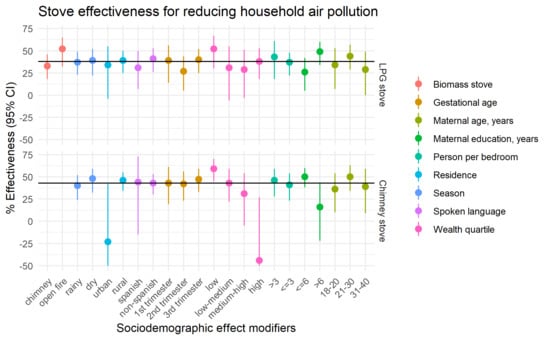
| Determinant | LPG Stove Ownership | Chimney Stove Ownership 1 | ||||
|---|---|---|---|---|---|---|
| n | % Effectiveness (95% CI) | Interaction p-Value 2 | n | % Effectiveness (95% CI) | Interaction p-Value 3 | |
| All | 559 | 38 (25, 49) | ||||
| Biomass Stove | ||||||
| Chimney Stove | 390 | 33 (18, 46) | ||||
| Open fire stove | 169 | 52 (32, 65) | 0.083 | 410 | 43 (31, 53) | |
| Season | ||||||
| Rainy Season | 316 | 37 (23, 49) | 223 | 40 (24, 52) | ||
| Dry Season | 243 | 39 (22, 52) | 0.849 | 187 | 48 (32, 59) | 0.355 |
| Residence | ||||||
| Urban | 69 | 34 (−4, 55) | 37 | 23 (−164, 42) | ||
| Rural | 490 | 39 (25, 50) | 0.732 | 373 | 46 (34, 55) | 0.039 |
| Spoken Language | ||||||
| Spanish | 135 | 31 (7, 50) | 61 | 44 (−15, 73) | ||
| Non-Spanish | 424 | 41 (26, 53) | 0.419 | 349 | 43 (30, 53) | 0.945 |
| Gestational Age | ||||||
| 1st Trimester | 80 | 39 (14, 56) | 58 | 43 (19, 61) | ||
| 2nd Trimester | 169 | 27 (5, 44) | 0.379 | 126 | 42 (23, 56) | 0.921 |
| 3rd Trimester | 299 | 40 (25, 52) | 0.918 | 218 | 47 (33, 59) | 0.704 |
| Wealth Quartile | ||||||
| Low | 168 | 52 (30, 67) | 136 | 59 (45, 70) | ||
| Low–Medium | 154 | 31 (−6, 55) | 0.200 | 135 | 43 (22, 59) | 0.142 |
| Medium–High | 104 | 29 (3, 51) | 0.129 | 76 | 31 (−5, 54) | 0.041 |
| High | 133 | 38 (18, 53) | 0.260 | 63 | −44 (−183, 27) | 0.001 |
| Persons per Bedroom | ||||||
| >3 | 200 | 43 (18, 61) | 177 | 46 (28, 59) | ||
| ≤3 | 359 | 37 (22, 48) | 0.589 | 233 | 41 (23, 54) | 0.672 |
| Maternal Education, Years | ||||||
| ≤6 | 379 | 26 (5, 42) | 304 | 50 (38, 60) | ||
| >6 | 180 | 49 (34, 60) | 0.029 | 106 | 16 (22, 43) | 0.019 |
| Maternal Age, Years | ||||||
| 18 to 20 | 144 | 34 (7, 53) | 114 | 36 (10, 54) | ||
| 21 to 30 | 281 | 44 (29, 57) | 0.379 | 194 | 50 (34, 63) | 0.240 |
| 31 to 40 | 134 | 29 (0, 49) | 0.776 | 102 | 39 (9, 59) | 0.839 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grajeda, L.M.; Thompson, L.M.; Arriaga, W.; Canuz, E.; Omer, S.B.; Sage, M.; Azziz-Baumgartner, E.; Bryan, J.P.; McCracken, J.P. Effectiveness of Gas and Chimney Biomass Stoves for Reducing Household Air Pollution Pregnancy Exposure in Guatemala: Sociodemographic Effect Modifiers. Int. J. Environ. Res. Public Health 2020, 17, 7723. https://doi.org/10.3390/ijerph17217723
Grajeda LM, Thompson LM, Arriaga W, Canuz E, Omer SB, Sage M, Azziz-Baumgartner E, Bryan JP, McCracken JP. Effectiveness of Gas and Chimney Biomass Stoves for Reducing Household Air Pollution Pregnancy Exposure in Guatemala: Sociodemographic Effect Modifiers. International Journal of Environmental Research and Public Health. 2020; 17(21):7723. https://doi.org/10.3390/ijerph17217723
Chicago/Turabian StyleGrajeda, Laura M., Lisa M. Thompson, William Arriaga, Eduardo Canuz, Saad B. Omer, Michael Sage, Eduardo Azziz-Baumgartner, Joe P. Bryan, and John P. McCracken. 2020. "Effectiveness of Gas and Chimney Biomass Stoves for Reducing Household Air Pollution Pregnancy Exposure in Guatemala: Sociodemographic Effect Modifiers" International Journal of Environmental Research and Public Health 17, no. 21: 7723. https://doi.org/10.3390/ijerph17217723
APA StyleGrajeda, L. M., Thompson, L. M., Arriaga, W., Canuz, E., Omer, S. B., Sage, M., Azziz-Baumgartner, E., Bryan, J. P., & McCracken, J. P. (2020). Effectiveness of Gas and Chimney Biomass Stoves for Reducing Household Air Pollution Pregnancy Exposure in Guatemala: Sociodemographic Effect Modifiers. International Journal of Environmental Research and Public Health, 17(21), 7723. https://doi.org/10.3390/ijerph17217723