Systematic Review of Behaviour Change Techniques within Interventions to Reduce Environmental Tobacco Smoke Exposure for Children

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Approach
2.2. Search Strategy
2.3. Trial Selection
2.4. Data Extraction
2.5. Quality Assessment
3. Results
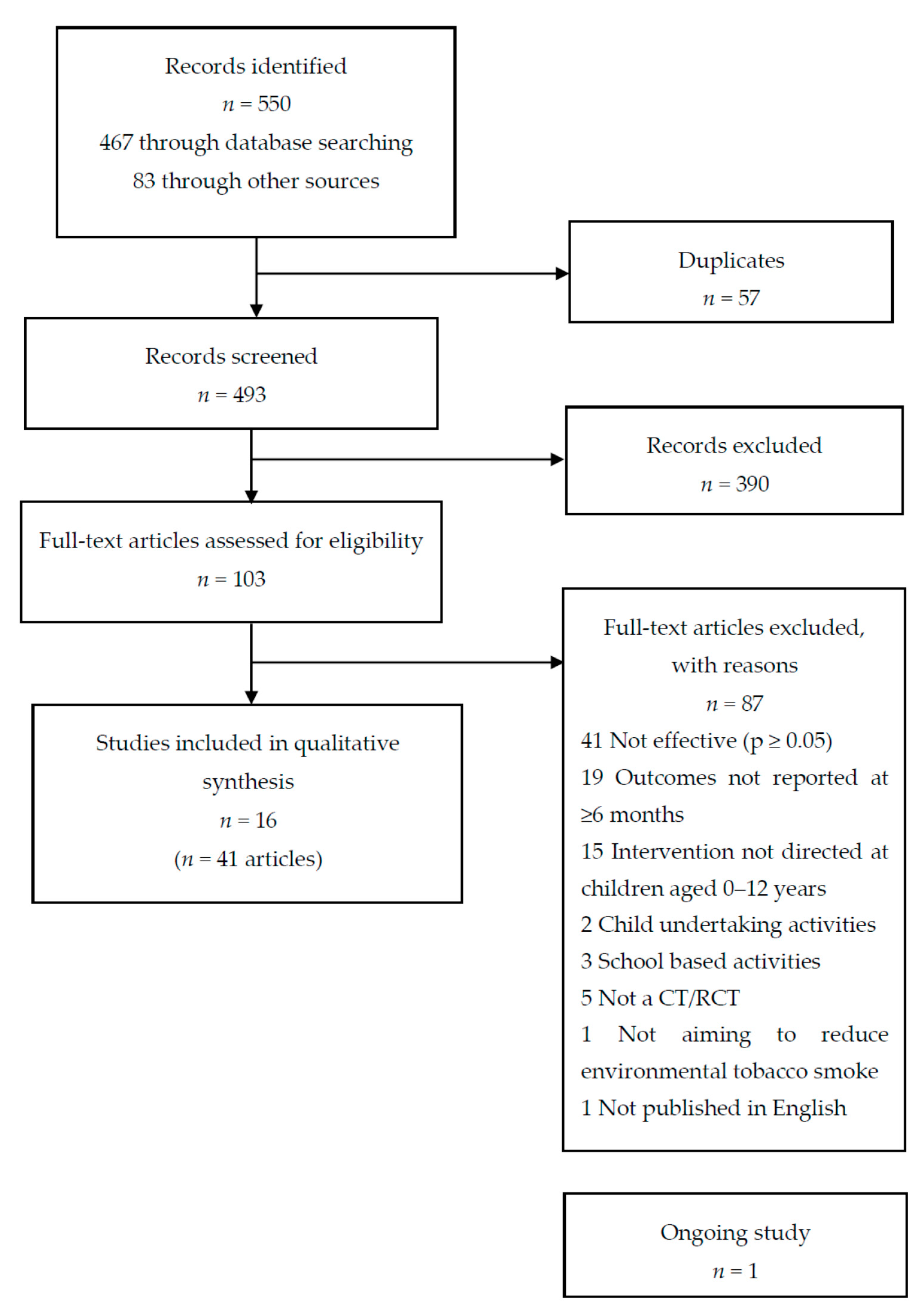
3.1. Numbers of Trials
3.2. Trial Characteristics
3.3. Intervention Characteristics
3.4. Quality Assessment
3.5. Behaviour Change Techniques
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- DoH. Towards a Smokefree Generation. A Tobacco Control Plan for England; Department of Health: London, UK, 2017. [Google Scholar]
- RCP. Passive Smoking and Children; Royal College of Physicians: London, UK, 2010. [Google Scholar]
- Chao, M.R.; Cooke, M.S.; Kuo, C.Y.; Pan, C.H.; Liu, H.H.; Yang, H.J.; Chen, S.C.; Chiang, Y.C.; Hu, C.W. Children are particularly vulnerable to environmental tobacco smoke exposure: Evidence from biomarkers of tobacco-specific nitrosamines, and oxidative stress. Environ. Int. 2018, 120, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.-H.; Hwang, J.H.; Moon, J.S.; Lee, D.-H. Environmental tobacco smoke and children’s health. Korean J. Pediatr. 2012, 55, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Blaakman, S.W.; Borrelli, B.; Wiesenthal, E.N.; Fagnano, M.; Tremblay, P.J.; Stevens, T.P.; Halterman, J.S. Secondhand smoke exposure reduction after NICU discharge: Results of a randomized trial. Acad. Pediatr. 2015, 15, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Raghuveer, G.; White, D.A.; Hayman, L.L.; Woo, J.G.; Villafane, J.; Celermajer, D.; Ward, K.D.; de Ferranti, S.D.; Zachariah, J. Cardiovascular consequences of childhood secondhand tobacco smoke exposure: Prevailing evidence, burden, and racial and socioeconomic disparities: A scientific statement from the American Heart Association. Circulation 2016, 134, e336–e359. [Google Scholar] [CrossRef]
- Diver, W.R.; Jacobs, E.J.; Gapstur, S.M. Secondhand smoke exposure in childhood and adulthood in relation to adult mortality among never smokers. Am. J. Prev. Med. 2018, 55, 345–352. [Google Scholar] [CrossRef]
- Merianos, A.L.; Dixon, C.A.; Mahabee-Gittens, E.M. Secondhand smoke exposure, illness severity, and resource utilization in pediatric emergency department patients with respiratory illnesses. J. Asthma 2017, 54, 798–806. [Google Scholar] [CrossRef]
- Schmitz, J.E.; Nwabuobi, C.K.; Pargas, A.; Camisasca-Lopina, H.; Sinkey, R.G.; Odibo, A.O. Risk factors for neonatal intensive care unit admission among growth restricted fetuses [25P]. Obstet. Gynecol. 2019, 133, 177S. [Google Scholar] [CrossRef]
- Mason, J.; Wheeler, W.; Brown, M.J. The economic burden of exposure to secondhand smoke for child and adult never smokers residing in U.S. public housing. Public Health Rep. 2015, 130, 230–244. [Google Scholar] [CrossRef]
- Lam, T.H.; Leung, G.M.; Ho, L.M. The effects of environmental tobacco smoke on health services utilization in the first eighteen months of life. Pediatrics 2001, 107, E91. [Google Scholar] [CrossRef]
- Vaz, L.R.; Jones, M.J.; Szatkowski, L.; Tata, L.J.; Petrou, S.; Coleman, T. Estimating the health-care costs of children born to pregnant smokers in England: Cohort study using primary and secondary health-care data. Addiction 2018, 113, 1305–1316. [Google Scholar] [CrossRef]
- Adams, E.K.; Miller, V.P.; Ernst, C.; Nishimura, B.K.; Melvin, C.; Merritt, R. Neonatal health care costs related to smoking during pregnancy. Health Econ. 2002, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, C.; Pickett, K.; Parrott, S.; Mdege, N.; Eapen, D. Estimating the Costs to the NHS of Smoking in Pregnancy for Pregnant Women and Infants; Public Health Research Consortium: York, ON, Canada, 2010. [Google Scholar]
- Passey, M.E.; Longman, J.M.; Robinson, J.; Wiggers, J.; Jones, L.L. Smoke-free homes: What are the barriers, motivators and enablers? A qualitative systematic review and thematic synthesis. BMJ Open 2016, 6, e010260. [Google Scholar] [CrossRef] [PubMed]
- Notley, C.; Blyth, A.; Craig, J.; Edwards, A.; Holland, R. Postpartum smoking relapse-a thematic synthesis of qualitative studies. Addiction 2015, 110, 1712–1723. [Google Scholar] [CrossRef] [PubMed]
- Livingstone-Banks, J.; Norris, E.; Hartmann-Boyce, J.; West, R.; Jarvis, M.; Chubb, E.; Hajek, P. Relapse prevention interventions for smoking cessation. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Lewis, S.; Parrott, S.; Wormall, S.; Coleman, T. Re-starting smoking in the postpartum period after receiving a smoking cessation intervention: A systematic review. Addiction 2016, 111, 981–990. [Google Scholar] [CrossRef]
- Chamberlain, C.; O’Mara-Eves, A.; Porter, J.; Coleman, T.; Perlen, S.M.; Thomas, J.; McKenzie, J.E. Psychosocial interventions for supporting women to stop smoking in pregnancy. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Orton, S.; Coleman, T.; Coleman-Haynes, T.; Ussher, M. Predictors of postpartum return to smoking: A systematic review. Nicotine Tob. Res. 2018, 20, 665–673. [Google Scholar] [CrossRef]
- Kanis, J.; Byczkowski, T.; Mahabee-Gittens, E.M. Motivation to quit smoking in parental smokers in the pediatric emergency department. Pediatr. Emerg. Care 2014, 30, 546–551. [Google Scholar] [CrossRef][Green Version]
- Bock, B.C.; Becker, B.M.; Borrelli, B. Smoking behavior and risk perception among the parents of infants in the neonatal intensive care unit. Nicotine Tob. Res. 2008, 10, 47–54. [Google Scholar] [CrossRef]
- McBride, C.M.; Lipkus, I.M.; Emmons, K.M. Understanding the potential of teachable moments: The case of smoking cessation. Health Educ. Res. 2003, 18, 156–170. [Google Scholar] [CrossRef]
- NICE. Smoking: Acute, Maternity and Mental Health Services [PH48]; National Institute for Health and Care Excellence: London, UK, 2013. [Google Scholar]
- NICE. How to Stop Smoking in Pregnancy and Following Childbirth: Public Health Guideline [PH26]; National Institute for Health and Clinical Excellence: London, UK, 2010. [Google Scholar]
- RCP. Hiding in Plain Sight: Treating Tobacco Dependency in the NHS; Royal College of Physicians: London, UK, 2018. [Google Scholar]
- Behbod, B.; Sharma, M.; Baxi, R.; Roseby, R.; Webster, P. Family and carer smoking control programmes for reducing children’s exposure to environmental tobacco smoke. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Flemming, K.; Graham, H.; McCaughan, D.; Angus, K.; Sinclair, L.; Bauld, L. Health professionals’ perceptions of the barriers and facilitators to providing smoking cessation advice to women in pregnancy and during the post-partum period: A systematic review of qualitative research. BMC Public Health 2016, 16, 290. [Google Scholar] [CrossRef] [PubMed]
- Nichols, A.; Clarke, P.; Notley, C. Parental smoking and support in the NICU. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F342. [Google Scholar] [CrossRef] [PubMed]
- Rosen, L.J.; Myers, V.; Winickoff, J.P.; Kott, J. Effectiveness of interventions to reduce tobacco smoke pollution in homes: A systematic review and meta-analysis. IJERPH 2015, 12, 16043–16059. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; West, R.; Sheals, K.; Godinho, C.A. Evaluating the effectiveness of behavior change techniques in health-related behavior: A scoping review of methods used. Transl. Behav. Med. 2018, 8, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Lorencatto, F.; West, R.; Michie, S. Specifying evidence-based behavior change techniques to aid smoking cessation in pregnancy. Nicotine Tob. Res. 2012, 14, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J.; Hardeman, W.; Bauld, L.; Holland, R.; Maskrey, V.; Naughton, F.; Orton, S.; Ussher, M.; Notley, C. A systematic review of behaviour change techniques within interventions to prevent return to smoking postpartum. Addict. Behav. 2018, 92, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (updated July 2019). Available online: www.training.cochrane.org/handbook (accessed on 17 December 2019).
- Abdullah, A.S.; Hua, F.; Khan, H.; Xia, X.; Bing, Q.; Tarang, K.; Winickoff, J.P. Secondhand smoke exposure reduction intervention in Chinese households of young children: A randomized controlled trial. Acad. Pediatr. 2015, 15, 588–598. [Google Scholar] [CrossRef]
- Abdullah, A.S.; Mak, Y.W.; Loke, A.Y.; Lam, T.H. Smoking cessation intervention in parents of young children: A randomised controlled trial. Addiction 2005, 100, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, A.L.; Tingen, M.S.; Nguyen, J.T.; Andrews, J.O.; Heath, J.; Waller, J.L.; Treiber, F.A. Parental smoking cessation: Impacting children’s tobacco smoke exposure in the home. Pediatrics 2018, 141, S96–S106. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.S.C.; Cheung, Y.T.D.; Fong, D.Y.T.; Emmons, K.; Leung, A.Y.M.; Leung, D.Y.P.; Lam, T.H. Family-based smoking cessation intervention for smoking fathers and nonsmoking mothers with a child: A randomized controlled trial. J. Pediatr. 2017, 182, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Emmons, K.M.; Hammond, S.K.; Fava, J.L.; Velicer, W.F.; Evans, J.L.; Monroe, A.D. A randomized trial to reduce passive smoke exposure in low-income households with young children. Pediatrics 2001, 108, 18–24. [Google Scholar] [CrossRef] [PubMed]
- French, G.M.; Groner, J.A.; Wewers, M.E.; Ahijevych, K. Staying smoke free: An intervention to prevent postpartum relapse. Nicotine Tob. Res. 2007, 9, 663–670. [Google Scholar] [CrossRef]
- Greenberg, R.A.; Strecher, V.J.; Bauman, K.E.; Boat, B.W.; Fowler, M.G.; Keyes, L.L.; Denny, F.W.; Chapman, R.S.; Stedman, H.C.; LaVange, L.M.; et al. Evaluation of a home-based intervention program to reduce infant passive smoking and lower respiratory illness. J. Behav. Med. 1994, 17, 273–290. [Google Scholar] [CrossRef]
- Groner, J.A.; Ahijevych, K.; Grossman, L.K.; Rich, L.N. The impact of a brief intervention on maternal smoking behavior. Pediatrics 2000, 105, 267–271. [Google Scholar]
- Hannover, W.; Thyrian, J.R.; Roske, K.; Grempler, J.; Rumpf, H.J.; John, U.; Hapke, U. Smoking cessation and relapse prevention for postpartum women: Results from a randomized controlled trial at 6, 12, 18 and 24 months. Addict. Behav. 2009, 34, 1–8. [Google Scholar] [CrossRef]
- Hovell, M.F.; Zakarian, J.M.; Matt, G.E.; Hofstetter, C.R.; Bernert, J.T.; Pirkle, J. Effect of counselling mothers on their children’s exposure to environmental tobacco smoke: Randomised controlled trial. BMJ 2000, 321, 337–342. [Google Scholar] [CrossRef]
- Hovell, M.F.; Zakarian, J.M.; Matt, G.E.; Liles, S.; Jones, J.A.; Hofstetter, C.R.; Larson, S.N.; Benowitz, N.L. Counseling to reduce children’s secondhand smoke exposure and help parents quit smoking: A controlled trial. Nicotine Tob. Res. 2009, 11, 1383–1394. [Google Scholar] [CrossRef] [PubMed]
- Lepore, S.J.; Collins, B.N.; Coffman, D.L.; Winickoff, J.P.; Nair, U.S.; Moughan, B.; Bryant-Stephens, T.; Taylor, D.; Fleece, D.; Godfrey, M. Kids Safe and Smokefree (KiSS) multilevel intervention to reduce child tobacco smoke exposure: Long-term results of a randomized controlled trial. IJERPH 2018, 15, 1239. [Google Scholar] [CrossRef] [PubMed]
- Ortega, C.G.; Peña, C.C.; Ortega, J.A.; Zafra, M.S.; Moreno, J.L.B.; Esteban, J.A.P.; Cuesta, C.C.; Martín-Cantera, C.; Cerezuela, E.S.; Pou, R.M.C.; et al. Effectiveness of a brief primary care intervention to reduce passive smoking in babies: A cluster randomised clinical trial. J. Epidemiol. Community Health 2015, 69, 249. [Google Scholar] [CrossRef]
- Severson, H.H.; Andrews, J.A.; Lichtenstein, E.; Wall, M.; Akers, L. Reducing maternal smoking and relapse: Long-term evaluation of a pediatric intervention. Prev. Med. 1997, 26, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Duan, Z.; Redmon, P.B.; Eriksen, M.P.; Koplan, J.P.; Huang, C. mHealth intervention is effective in creating smoke-free homes for newborns: A randomized controlled trial study in China. Sci. Rep. 2017, 7, 9276. [Google Scholar] [CrossRef]
- Collins, B.N.; Lepore, S.J. Babies Living Safe & Smokefree: Randomized controlled trial of a multilevel multimodal behavioral intervention to reduce low-income children’s tobacco smoke exposure. BMC Public Health 2017, 17, 249. [Google Scholar] [CrossRef]
- Brown, N.; Luckett, T.; Davidson, P.M.; Di Giacomo, M. Interventions to reduce harm from smoking with families in infancy and early childhood: A systematic review. IJERPH 2015, 12, 3091–3119. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.B.; Mackenzie, L.J.; Freund, M.; Wolfenden, L.; Roseby, R.; Wiggers, J.H. Interventions by health care professionals who provide routine child health care to reduce tobacco smoke exposure in children: A review and meta-analysis. JAMA Pediatrics 2016, 170, 138–147. [Google Scholar] [CrossRef]
- Campbell, K.A.; Fergie, L.; Coleman-Haynes, T.; Cooper, S.; Lorencatto, F.; Ussher, M.; Dyas, J.; Coleman, T. Improving behavioral support for smoking cessation in pregnancy: What are the barriers to stopping and which behavior change techniques can influence these? Application of Theoretical Domains Framework. IJERPH 2018, 15, 359. [Google Scholar] [CrossRef]
- Flemming, K.; McCaughan, D.; Angus, K.; Graham, H. Qualitative systematic review: Barriers and facilitators to smoking cessation experienced by women in pregnancy and following childbirth. J. Adv. Nurs. 2015, 71, 1210–1226. [Google Scholar] [CrossRef]
- Adams, K.; Beem, A.; Diener, E.; Merritt, T. Protecting the vulnerable: The importance of effective parental tobacco-dependence treatment during prenatal and newborn care. Pediatr. Allergy Immunol. Pulmonol. 2012, 25, 3–10. [Google Scholar] [CrossRef]
- Ahlund, S.; Clarke, P.; Hill, J.; Thalange, N.K. Post-traumatic stress symptoms in mothers of very low birth weight infants 2–3 years post-partum. Arch. Womens Ment. Health 2009, 12, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Tsironi, S.; Koulierakis, G. Factors associated with parents’ levels of stress in pediatric wards. J. Child. Health Care 2018, 22, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Cousino, M.K.; Hazen, R.A. Parenting stress among caregivers of children with chronic illness: A systematic review. J. Pediatr. Psychol. 2013, 38, 809–828. [Google Scholar] [CrossRef]
- Schmidt, A.M.; Ranney, L.M.; Pepper, J.K.; Goldstein, A.O. Source credibility in tobacco control messaging. Tob. Regul. Sci. 2016, 2, 31–37. [Google Scholar] [CrossRef]
- de Bruin, M.; Black, N.; Javornik, N.; Viechtbauer, W.; Eisma, M.C.; Hartman-Boyce, J.; Williams, A.J.; West, R.; Michie, S.; Johnston, M. Underreporting of the active content of behavioural interventions: A systematic review and meta-analysis of randomised trials of smoking cessation interventions. Health Psychol. Rev. 2020, 13, 1–19. [Google Scholar] [CrossRef]
- Peters, G.J.; de Bruin, M.; Crutzen, R. Everything should be as simple as possible, but no simpler: Towards a protocol for accumulating evidence regarding the active content of health behaviour change interventions. Health Psychol. Rev. 2015, 9, 1–14. [Google Scholar] [CrossRef]
- ONS. Adult Smoking Habits in the UK. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandlifeexpectancies/bulletins/adultsmokinghabitsingreatbritain/2018#characteristics-of-current-cigarette-smokers-in-the-uk (accessed on 25 March 2020).


{kind=link}
| BCT Code | BCT Label | BCT in Effective Interventions n (% Studies); Max n = 16 |
|---|---|---|
| 1.1 | Goal setting (behaviour) | 8 (50) * |
| 1.2 | Problem solving | 11 (69) * |
| 1.4 | Action planning | 8 (50) * |
| 1.5 | Review behaviour goal(s) | 6 (38) * |
| 1.6 | Discrepancy between current behaviour and goal | 1 (6) |
| 1.7 | Review outcome goal(s) | 1 (6) |
| 1.8 | Behavioural contract | 2 (13) |
| 2.2 | Feedback on behaviour | 3 (19) |
| 2.3 | Self-monitoring of behaviour | 3 (19) |
| 2.6 | Biofeedback | 3 (19) |
| 2.7 | Feedback on outcome(s) of behaviour | 1 (6) |
| 3.1 | Social support (unspecified) | 13 (81) * |
| 3.2 | Social support (practical) | 2 (13) |
| 4.1 | Instruction on how to perform a behaviour | 7 (44) * |
| 5.1 | Information about health consequences | 10 (63) * |
| 5.2 | Salience of consequences | 1 (6) |
| 5.3 | Information about social and environmental consequences | 4 (25) * |
| 5.6 | Information about emotional consequences | 1 (6) |
| 6.1 | Demonstration of the behaviour | 1 (6) |
| 6.2 | Social comparison | 1 (6) |
| 7.1 | Prompts/cues | 2 (13) |
| 8.2 | Behaviour substitution | 4 (25) * |
| 8.7 | Graded tasks | 1 (6) |
| 9.1 | Credible source | 9 (56) * |
| 9.2 | Pros and cons | 3 (19) |
| 10.4 | Social reward | 7 (44) * |
| 10.9 | Self-reward | 2 (13) |
| 11.1 | Pharmacological support | 3 (19) |
| 11.2 | Reduce negative emotions | 3 (19) |
| 12.1 | Restructuring the physical environment | 2 (13) |
| 12.2 | Restructuring the social environment | 2 (13) |
| 12.3 | Avoidance/reducing exposure to cues for the behaviour | 2 (13) |
| 12.5 | Adding objects to the environment | 5 (31) * |
| 13.1 | Identification of self as role model | 1 (6) |
| 13.2 | Framing/reframing | 2 (13) |
| 13.3 | Incompatible beliefs | 1 (6) |
| 13.5 | Identity associated with changed behaviour | 1 (6) |
| 14.4 | Reward approximation | 3 (19) |
| 15.1 | Verbal persuasion about capability | 4 (25) * |
| 15.2 | Mental rehearsal of successful performance | 1 (6) |
| 15.3 | Focus on past success | 2 (13) |
| 16.2 | Imaginary reward | 1 (6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, T.J.; Gentry, S.; Bauld, L.; Boyle, E.M.; Clarke, P.; Hardeman, W.; Holland, R.; Naughton, F.; Orton, S.; Ussher, M.; et al. Systematic Review of Behaviour Change Techniques within Interventions to Reduce Environmental Tobacco Smoke Exposure for Children. Int. J. Environ. Res. Public Health 2020, 17, 7731. https://doi.org/10.3390/ijerph17217731
Brown TJ, Gentry S, Bauld L, Boyle EM, Clarke P, Hardeman W, Holland R, Naughton F, Orton S, Ussher M, et al. Systematic Review of Behaviour Change Techniques within Interventions to Reduce Environmental Tobacco Smoke Exposure for Children. International Journal of Environmental Research and Public Health. 2020; 17(21):7731. https://doi.org/10.3390/ijerph17217731
Chicago/Turabian StyleBrown, Tracey J., Sarah Gentry, Linda Bauld, Elaine M. Boyle, Paul Clarke, Wendy Hardeman, Richard Holland, Felix Naughton, Sophie Orton, Michael Ussher, and et al. 2020. "Systematic Review of Behaviour Change Techniques within Interventions to Reduce Environmental Tobacco Smoke Exposure for Children" International Journal of Environmental Research and Public Health 17, no. 21: 7731. https://doi.org/10.3390/ijerph17217731
APA StyleBrown, T. J., Gentry, S., Bauld, L., Boyle, E. M., Clarke, P., Hardeman, W., Holland, R., Naughton, F., Orton, S., Ussher, M., & Notley, C. (2020). Systematic Review of Behaviour Change Techniques within Interventions to Reduce Environmental Tobacco Smoke Exposure for Children. International Journal of Environmental Research and Public Health, 17(21), 7731. https://doi.org/10.3390/ijerph17217731