Air Pollution and Incidence of Lung Cancer by Histological Type in Korean Adults: A Korean National Health Insurance Service Health Examinee Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
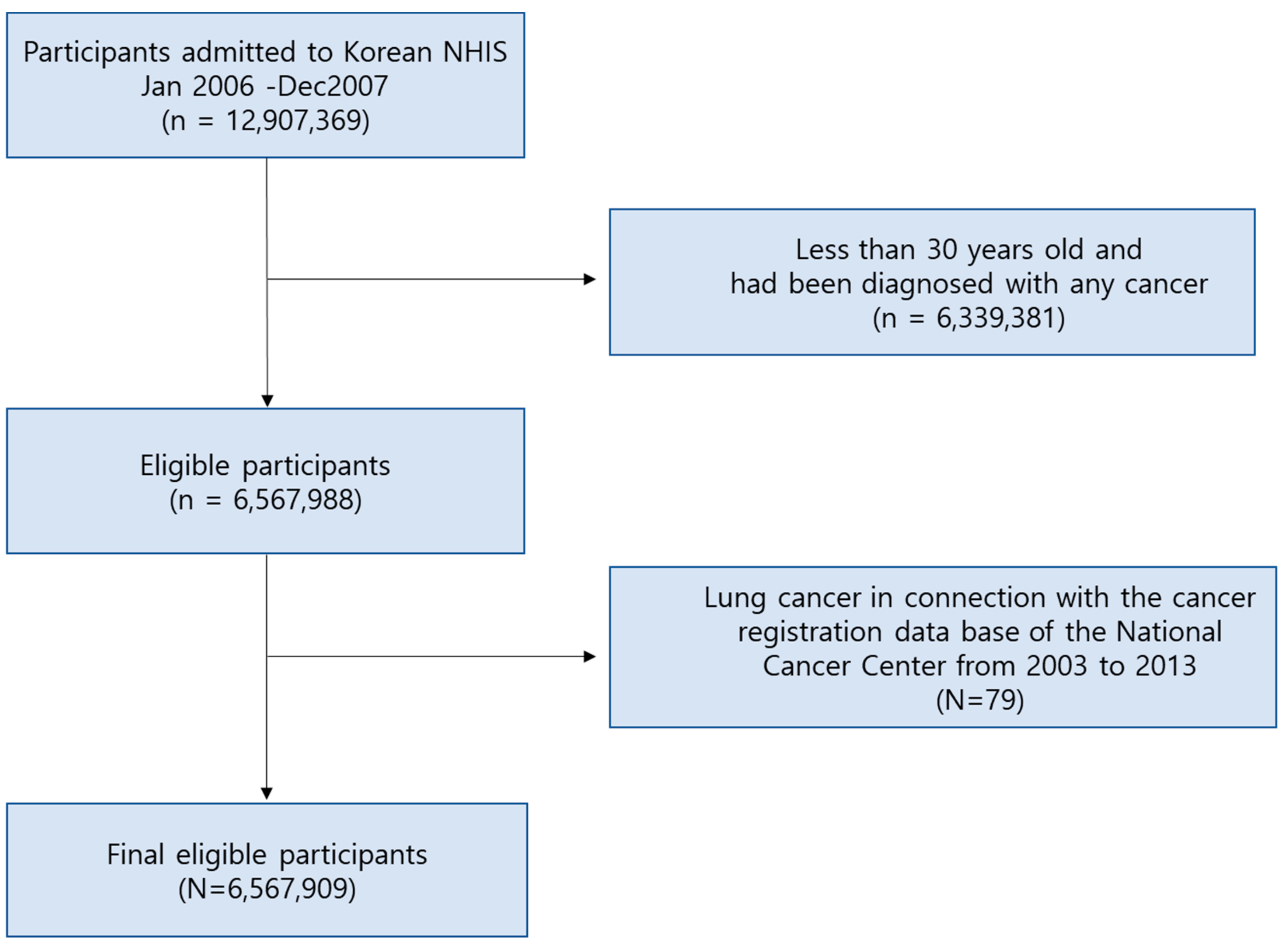
2.1. Study Design and Participants
2.2. Exposure Assessment
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
3.1. Description of the Study Population and Lung Cancer Incidence
3.2. Factors of Demographic and Lifestyle Behavior Affecting the Development of Lung Cancer
3.3. Air Pollution Exposure and Lung Cancer Incidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhu, D.; Cui, B.; Ding, R.; Shi, X.; He, P. Association between particulate matter air pollution and lung cancer. Thorax 2020, 75, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Abbey, D.E.; Nishino, N.; McDonnell, W.F.; Burchette, R.J.; Knutsen, S.F.; Beeson, W.L.; Yang, J.X. Long-Term Inhalable Particles and Other Air Pollutants Related to Mortality in Nonsmokers. Am. J. Respir. Crit. Care Med. 1999, 159, 373–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G.; Speizer, F.E. An Association between Air Pollution and Mortality in Six U.S. Cities. New Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar]
- Park, J.Y.; Jang, S.H. Epidemiology of Lung Cancer in Korea: Recent Trends. Tuberc. Respir. Dis. 2016, 79, 58–69. [Google Scholar]
- Kim, H.C.; Jung, C.Y.; Cho, D.G.; Jeon, J.H.; Lee, J.E.; Ahn, J.S.; Kim, S.J.; Kim, Y.; Kim, Y.-C.; Kim, J.-E.; et al. Clinical Characteristics and Prognostic Factors of Lung Cancer in Korea: A Pilot Study of Data from the Korean Nationwide Lung Cancer Registry. Tuberc. Respir. Dis. 2019, 82, 118–125. [Google Scholar] [CrossRef]
- Hystad, P.; Demers, P.A.; Johnson, K.C.; Carpiano, R.M.; Brauer, M. Long-term Residential Exposure to Air Pollution and Lung Cancer Risk. Epidemiology 2013, 24, 762–772. [Google Scholar] [CrossRef]
- Hamra, G.B.; Guha, N.; Cohen, A.; Laden, F.; Raaschou-Nielsen, O.; Samet, J.M.; Vineis, P.; Forastiere, F.; Saldiva, P.; Yorifuji, T.; et al. Outdoor particulate matter exposure and lung cancer: a systematic review and meta-analysis. Environ. Health Perspect. 2014, 122, 9. [Google Scholar] [CrossRef] [Green Version]
- Tomczak, A.; Miller, A.B.; Weichenthal, S.A.; To, T.; Wall, C.; Van Donkelaar, A.; Martin, R.V.; Crouse, D.L.; Villeneuve, P.J. Long-term exposure to fine particulate matter air pollution and the risk of lung cancer among participants of the Canadian National Breast Screening Study. Int. J. Cancer 2016, 139, 1958–1966. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Park, S.-H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service–National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2016, 46, e15. [Google Scholar] [CrossRef]
- Jung, K.-W.; Park, S.; Kong, H.-J.; Won, Y.-J.; Boo, Y.-K.; Shin, H.-R.; Park, E.-C.; Lee, J.-S. Cancer Statistics in Korea: Incidence, Mortality and Survival in 2006-2007. J. Korean Med Sci. 2010, 25, 1113–1121. [Google Scholar] [CrossRef]
- Shin, H.-R.; Won, Y.J.; Jung, K.W.; Kong, H.J.; Yim, S.H.; Lee, J.K.; Noh, H.I.; Lee, J.K.; Pisani, P.; Park, J.G.; et al. Regional Cancer Registries. Nationwide cancer incidence in Korea, 1999~2001; First result using the national cancer incidence database. Cancer Res. Treat. 2005, 37, 325. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.-W.; Park, S.; Won, Y.-J.; Kong, H.-J.; Lee, J.Y.; Seo, H.G.; Lee, J.-S. Prediction of Cancer Incidence and Mortality in Korea, 2012. Cancer Res. Treat. 2012, 44, 25–31. [Google Scholar] [CrossRef]
- Oh, J.-K.; Lim, M.K.; Yun, E.H.; Choi, M.H.; Hong, S.T.; Chang, S.H.; Park, S.K.; Cho, S.I.; Kim, D.H.; Yoo, K.Y.; et al. Cohort Profile: Community-based prospective cohort from the National Cancer Center, Korea. Int. J. Epidemiol. 2017, 46, e14. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Song, I. National-scale exposure prediction for long-term concentrations of particulate matter and nitrogen dioxide in South Korea. Environ. Pollut. 2017, 226, 21–29. [Google Scholar] [CrossRef]
- Bach, P.B.; Kattan, M.W.; Thornquist, M.D.; Kris, M.G.; Tate, R.C.; Barnett, M.J.; Hsieh, L.J.; Begg, C.B. Variations in lung cancer risk among smokers. J. Natl. Cancer Inst. 2003, 95, 470–478. [Google Scholar] [CrossRef] [Green Version]
- Vineis, P.; Airoldi, L.; Veglia, P.; Olgiati, L.; Pastorelli, R.; Autrup, H.; Dunning, A.; Garte, S.; Gormally, E.; Hainaut, P.; et al. Environmental tobacco smoke and risk of respiratory cancer and chronic obstructive pulmonary disease in former smokers and never smokers in the EPIC prospective study. BMJ 2005, 330, 277. [Google Scholar] [CrossRef] [Green Version]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar]
- Kim, Y.-C.; Won, Y.-J. The Development of the Korean Lung Cancer Registry (KALC-R). Tuberc. Respir. Dis. 2019, 82, 91–93. [Google Scholar] [CrossRef]
- Zhong, Y.J.; Wen, Y.F.; Wong, H.M.; Yin, G.; Lin, R.; Yang, S.Y. Trends and Patterns of Disparities in Burden of Lung Cancer in the United States, 1974–2015. Front. Oncol. 2019, 9, 404. [Google Scholar] [CrossRef]
- Houston, K.A.; Henley, S.J.; Li, J.; White, M.C.; Richards, T.B. Patterns in lung cancer incidence rates and trends by histologic type in the United States, 2004-2009. Lung Cancer 2014, 86, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Iii, C.A.P.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D.; Pope, C.A. Lung Cancer, Cardiopulmonary Mortality, and Long-term Exposure to Fine Particulate Air Pollution. JAMA 2002, 287, 1132–1141. [Google Scholar]
- Puett, R.C.; Hart, J.E.; Yanosky, J.D.; Spiegelman, N.; Wang, M.; Fisher, J.A.; Hong, B.; Laden, F. Particulate Matter Air Pollution Exposure, Distance to Road, and Incident Lung Cancer in the Nurses’ Health Study Cohort. Environ. Health Perspect. 2014, 122, 926–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabrielson, E. Worldwide trends in lung cancer pathology. Respirology. 2006, 11, 533–538. [Google Scholar] [CrossRef]
- Consonni, D.; Carugno, M.; De Matteis, S.; Nordio, F.; Randi, G.; Bazzano, M.; Caporaso, N.E.; Tucker, M.A.; Bertazzi, P.A.; Pesatori, A.C.; et al. Outdoor particulate matter (PM10) exposure and lung cancer risk in the EAGLE study. PLoS ONE 2018, 13, e0203539. [Google Scholar] [CrossRef] [Green Version]
- Lamichhane, D.K.; Kim, H.-C.; Choi, C.-M.; Shin, M.-H.; Shim, Y.M.; Leem, J.-H.; Ryu, J.-S.; Nam, H.-S.; Park, S.-M. Lung Cancer Risk and Residential Exposure to Air Pollution: A Korean Population-Based Case-Control Study. Yonsei Med. J. 2017, 58, 1111–1118. [Google Scholar] [CrossRef]
- Katanoda, K.; Sobue, T.; Satoh, H.; Tajima, K.; Suzuki, T.; Nakatsuka, H.; Tominaga, S.; Takezaki, T.; Nakayama, T.; Nitta, H.; et al. An association between long-term exposure to ambient air pollution and mortality from lung cancer and respiratory diseases in Japan. J. Epidemiol. 2011, 21, 132. [Google Scholar] [CrossRef] [Green Version]
- Vineis, P.; Hoek, G.; Krzyzanowski, M.; Vigna-Taglianti, F.; Veglia, F.; Airoldi, L.; Overvad, K.; Raaschou-Nielsen, O.; Clavel-Chapelon, F.; Linseisen, J.; et al. Lung cancers attributable to environmental tobacco smoke and air pollution in non-smokers in different European countries: A prospective study. Environ. Health Perspect. 2007, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Vineis, P.; Hoek, G.; Krzyzanowski, M.; Vigna-Taglianti, F.; Veglia, F.; Airoldi, L.; Autrup, H.; Dunning, A.M.; Garte, S.; Hainaut, P.; et al. Air pollution and risk of lung cancer in a prospective study in Europe. Int. J. Cancer 2006, 119, 169–174. [Google Scholar] [CrossRef]
- Beeson, W.L.; E Abbey, D.; Knutsen, S.F. Long-term concentrations of ambient air pollutants and incident lung cancer in California adults: results from the AHSMOG study. Adventist Health Study on Smog. Environ. Health Perspect. 1998, 106, 813–823. [Google Scholar] [CrossRef] [Green Version]
- Gharibvand, L.; Shavlik, D.; Ghamsary, M.; Beeson, W.L.; Soret, S.; Knutsen, R.; Knutsen, S.F. The Association between Ambient Fine Particulate Air Pollution and Lung Cancer Incidence: Results from the AHSMOG-2 Study. Environ. Health Perspect. 2016, 125, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Barta, J.; Rojulpote, M.; Lake, M.; McIntire, R.; Juon, H.-S. Occupational Risk, Race, and Lung Cancer Incidence in the National Lung Screening Trial. In C30. Lung Cancer Screening: Lessons from the Front-Line; American Thoracic Society: New York, NY, USA, 2019; p. A4471. [Google Scholar]


{kind=link}
| Mean | SD | Min | 25th Percentile | 50th Percentile | 75th Percentile | Max | |
|---|---|---|---|---|---|---|---|
| PM10 (µg/m3) | 55.80 | 6.30 | 37.99 | 50.40 | 57.30 | 60.90 | 75.95 |
| NO2 (ppm) | 23.90 | 9.00 | 4.16 | 16.30 | 23.50 | 32.10 | 42.66 |
| n (%) | |
|---|---|
| Age | |
| 30–39 yr | 1,860,367 (28.3) |
| 40–49 yr | 2,007,864 (30.6) |
| 50–59 yr | 1,386,946 (21.1) |
| 60–69 yr | 884,183 (13.5) |
| 70–79 yr | 369,650 (5.6) |
| ≥80 yr | 58,899 (0.9) |
| Gender | |
| Male | 4,314,480 (65.7) |
| Female | 2,253,429 (34.3) |
| BMI | |
| <18.5 | 168,578 (2.6) |
| 18.5–22.9 | 2,402,068 (36.6) |
| 23–24.9 | 1,721,017 (26.2) |
| 25–29.9 | 2,063,203 (31.4) |
| ≥30 | 207,735 (3.2) |
| Smoking | |
| Non-smoker | 3637,984 (59.4) |
| Former-smoker | 653,621 (10.7) |
| Current-smoker | 1,829,330 (29.9) |
| Pack-year/current-smoker | 17.1(10.9) |
| Physical activity | |
| None | 3,168,619 (51.6) |
| 1–2/week | 1,798,894 (29.3) |
| 3–4/week | 687,586 (11.2) |
| 5–6/week | 163,074 (2.7) |
| Everyday | 318,890 (5.2) |
| History of COPD | |
| No | 6,484,490 (98.7) |
| Yes | 83,419 (1.3) |
| Lung disease due to external factors | |
| No | 6,564,745 (100.0) |
| Yes | 3,164 (0.05) |
| Interstitial lung disease | |
| No | 6,560,779 (99.9) |
| Yes | 7130 (0.1) |
| Cancer Type | All (n = 6,567,909) | Male (n = 4,314,480) | Female (n = 2,253,429) | |||
|---|---|---|---|---|---|---|
| Cases | Incidence Rate(Per 100,000 Person-Years) | Cases | Incidence Rate(Per 100,000 Person-Years) | Cases | Incidence Rate(Per 100,000 Person-Years) | |
| All lung cancer | 27,518 | 419.0 | 21,912 | 333.6 | 5606 | 85.4 |
| Non-small cell carcinoma | 24,031 | 365.9 | 19,076 | 290.4 | 4955 | 75.4 |
| Squamous cell carcinoma | 7280 | 110.8 | 6912 | 105.2 | 368 | 5.6 |
| Adenocarcinoma | 8223 | 125.2 | 5744 | 87.5 | 2479 | 37.7 |
| Large cell carcinoma | 314 | 4.8 | 291 | 4.4 | 23 | 0.4 |
| Other | 8214 | 125.1 | 6129 | 93.3 | 2085 | 31.7 |
| Small cell carcinoma | 3127 | 47.6 | 2836 | 43.2 | 291 | 4.4 |
| Overall Lung Cancer | ||||||
|---|---|---|---|---|---|---|
| All | Case/At RiskHR (95% CI) | Male | Case/At RiskHR (95% CI) | Female | Case/At RiskHR (95% CI) | |
| Gender | ||||||
| Male | 21,912/4,314,480 | 2.25(2.18–2.32) | ||||
| Female | 5246/2,253,429 | 1.00 (ref.) | ||||
| BMI | ||||||
| <18.5 | 1368/168,578 | 1.68(1.59–1.78) | 1128/85,386 | 1.95(1.84–2.08) | 240/83,192 | 1.43(1.25–1.64) |
| 18.5–22.9 | 11,596/2,402,068 | 1.00 (ref.) | 9608/1,416,418 | 1.00 (ref.) | 1988/985,650 | 1.00 (ref.) |
| 23–24.9 | 6722/1,721,017 | 0.81(0.79–0.83) | 5485/1,192,940 | 0.68(0.65–0.70) | 1237/528,077 | 1.16(1.08–1.24) |
| 25–29.9 | 6972/2,063,203 | 0.70(0.68–0.72) | 5392/1,483,685 | 0.54(0.52–0.55) | 1580/579,518 | 1.34(1.26–1.43) |
| ≥30 | 481/207,735 | 0.48(0.44–0.53) | 285/133,202 | 0.32(0.28–0.36) | 196/74,533 | 1.29(1.12–1.50) |
| Smoking | ||||||
| Non-smoker | 11,266/3,637,984 | 1.00 (ref.) | 6838/1,647,730 | 1.00 (ref.) | 4428/1,990,254 | 1.00 (ref.) |
| Former-smoker | 2960/653,621 | 1.49(1.43–1.55) | 2879/631,592 | 1.10(1.06–1.15) | 81/22,029 | 1.67(1.34–2.08) |
| Current-smoker | 11,242/1,829,330 | 2.04(1.99–2.10) | 10,879/1,773,699 | 1.50(1.46–1.55) | 363/55,631 | 2.95(2.65–3.28) |
| Physical activity | ||||||
| None | 15,139/3,168,619 | 1.00 (ref.) | 11,928/1,870,962 | 1.00 (ref.) | 3211/1,297,657 | 1.00 (ref.) |
| 1–2/week | 5111/1,798,894 | 0.60(0.58–0.62) | 4367/1,384,309 | 0.50(0.48–0.52) | 744/414,585 | 0.73(0.67–0.79) |
| 3–4/week | 2154/687,586 | 0.66(0.63–0.69) | 1740/487,860 | 0.56(0.53–0.59) | 414/199,726 | 0.84(0.76–0.93) |
| 5–6/week | 643/163,074 | 0.83(0.77–0.90) | 510/107,404 | 0.75(0.68–0.81) | 133/55,670 | 0.97(0.82–1.16) |
| Everyday | 2222/318,890 | 1.44(1.38–1.51) | 1855/201,326 | 1.43(1.36–1.50) | 367/117,564 | 1.25(1.12–1.39) |
| Alcohol consumption | ||||||
| None | 13,152/2,956,359 | 1.00 (ref.) | 8925/1,336,835 | 1.00 (ref.) | 4227/1,619,524 | 1.00 (ref.) |
| 2–3/month | 2823/1,161,376 | 0.56(0.54–0.58) | 2444/877,845 | 0.42(0.40–0.44) | 379/283,531 | 0.52(0.47–0.58) |
| 1–2/week | 4310/1,373,243 | 0.72(0.70–0.75) | 4092/1,220,541 | 0.51(0.49–0.53) | 218/152,702 | 0.56(0.49–0.64) |
| 3–4/week | 2545/473,454 | 1.23(1.18–1.29) | 2503/446,658 | 0.84(0.81–0.88) | 42/26,796 | 0.61(0.45–0.83) |
| Everyday | 2736/213,508 | 2.89(2.77–3.01) | 2697/200,618 | 1.99(1.90–2.07) | 39/12,890 | 1.16(0.85–1.59) |
| History of COPD | ||||||
| No | 24,982/6,484,490 | 1.00 (ref.) | 19,968/4,260,123 | 1.00 (ref.) | 5014/2,224,367 | 1.00 (ref.) |
| Yes | 2176/83,419 | 6.64(6.35–6.94) | 1944/54,357 | 7.47(7.13–7.82) | 232/29,062 | 3.47(3.05–3.96) |
| Lung disease due to external factors | ||||||
| No | 27,058/6,564,745 | 1.00 (ref.) | 21,815/4,311,633 | 1.00 (ref.) | 5243/2,253,112 | 1.00 (ref.) |
| Yes | 100/3164 | 7.60(6.24–9.24) | 97/2847 | 6.60(5.40–8.05) | 3/317 | 3.93(1.27–12.20) |
| Interstitial lung disease | ||||||
| No | 26,918/6,560,779 | 1.00 (ref.) | 21,685/4,309,639 | 1.00 (ref.) | 5233/2,251,140 | 1.00 (ref.) |
| Yes | 240/7130 | 8.19(7.21–9.30) | 227/4841 | 9.33(8.19–10.64) | 13/2289 | 2.43(1.41–4.18) |
| Events | PM10 | NO2 | |||
|---|---|---|---|---|---|
| Model1HR (95% CI) | Model2HR (95% CI) | Model1HR (95% CI) | Model2HR (95% CI) | ||
| Male | |||||
| Non-smoker | |||||
| All lung cancer | 6838 | 0.92(0.86–0.97) | 0.95(0.90–1.01) | 0.85(0.80–0.90) | 0.90(0.85–0.96) |
| Non-small cell carcinoma | 6124 | 0.92(0.87–0.98) | 0.96(0.90–1.02) | 0.85(0.80–0.91) | 0.90(0.85–0.96) |
| Squamous cell carcinoma | 1900 | 0.87(0.78–0.97) | 0.94(0.83–1.05) | 0.70(0.62–0.79) | 0.77(0.68–0.88) |
| Adenocarcinoma | 2052 | 0.92(0.83–1.02) | 0.93(0.84–1.04) | 0.95(0.85–1.05) | 0.98(0.88–1.09) |
| Large cell carcinoma | 59 | 1.11(0.61–2.02) | 1.25(0.68–2.30) | 0.66(0.33–1.35) | 0.68(0.32–1.44) |
| Other | 2113 | 0.97(0.87–1.08) | 1.00(0.90–1.11) | 0.91(0.82–1.01) | 0.95(0.85–1.06) |
| Small cell carcinoma | 714 | 0.87(0.72–1.04) | 0.90(0.75–1.09) | 0.82(0.68–0.99) | 0.89(0.74–1.09) |
| Former-smoker | |||||
| All lung cancer | 2879 | 0.91(0.83–0.99) | 0.92(0.84–1.01) | 0.99(0.90–1.08) | 1.03(0.94–1.13) |
| Non-small cell carcinoma | 2569 | 0.93(0.84–1.02) | 0.94(0.85–1.04) | 0.98(0.89–1.08) | 1.03(0.94–1.14) |
| Squamous cell carcinoma | 834 | 0.82(0.68–0.97) | 0.83(0.69–0.99) | 0.84(0.71–1.00) | 0.92(0.77–1.10) |
| Adenocarcinoma | 776 | 1.05(0.89–1.24) | 1.02(0.85–1.21) | 1.20(1.02–1.40) | 1.17(0.96–1.38) |
| Large cell carcinoma | 44 | 0.79(0.37–1.70) | 0.80(0.35–1.83) | 0.54(0.23–1.27) | 0.53(0.20–1.36) |
| Other | 915 | 0.93(0.80–1.10) | 0.99(0.84–1.17) | 0.96(0.82–1.13) | 1.04(0.88–1.22) |
| Small cell carcinoma | 310 | 0.76(0.57–1.02) | 0.76(0.56–1.03) | 1.03(0.79–1.34) | 1.06(0.80–1.40) |
| Current-smoker | |||||
| All lung cancer | 10,879 | 1.00(0.95–1.04) | 1.03(0.98–1.08) | 0.97(0.92–1.02) | 0.99(0.94–1.04) |
| Non-small cell carcinoma | 9241 | 1.01(0.96–1.06) | 1.05(0.99–1.11) | 0.96(0.91–1.01) | 0.98(0.93–1.04) |
| Squamous cell carcinoma | 3755 | 0.97(0.90–1.05) | 1.01(0.93–1.10) | 0.91(0.84–0.99) | 0.97(0.89–1.06) |
| Adenocarcinoma | 2570 | 1.11(1.01–1.21) | 1.14(1.03–1.25) | 1.05(0.96–1.16) | 1.03(0.93–1.14) |
| Large cell carcinoma | 167 | 0.79(0.53–1.18) | 0.87(0.57–1.33) | 0.78(0.51–1.18) | 0.83(0.53–1.30) |
| Other | 2749 | 0.99(0.90–1.08) | 1.02(0.93–1.13) | 0.94(0.85–1.03) | 0.97(0.87–1.07) |
| Small cell carcinoma | 1638 | 0.91(0.80–1.03) | 0.91(0.80–1.03) | 1.03(0.92–1.17) | 1.03(0.90–1.17) |
| Female | |||||
| Non-smoker | |||||
| All lung cancer | 4428 | 0.99(0.92–1.07) | 0.99(0.92–1.07) | 1.00(0.93–1.08) | 1.01(0.93–1.08) |
| Non-small cell carcinoma | 4231 | 0.99(0.92–1.07) | 0.99(0.92–1.07) | 1.02(0.95–1.10) | 1.03(0.95–1.11) |
| Squamous cell carcinoma | 265 | 0.95(0.70–1.29) | 0.97(0.71–1.32) | 0.91(0.66–1.26) | 0.93(0.67–1.29) |
| Adenocarcinoma | 2164 | 0.94(0.85–1.05) | 0.93(0.84–1.04) | 0.96(0.86–1.07) | 0.97(0.87–1.08) |
| Large cell carcinoma | 16 | 0.55(0.12–2.41) | 0.59(0.13–2.48) | 1.39(0.45–4.36) | 1.45(0.46–4.60) |
| Other | 1786 | 1.07(0.95–1.19) | 1.07(0.95–1.20) | 1.12(0.99–1.25) | 1.11(0.99–1.25) |
| Small cell carcinoma | 197 | 0.97(0.68–1.37) | 1.01(0.71–1.45) | 0.52(0.33–0.82) | 0.55(0.35–0.88) |
| Former-smoker | |||||
| All lung cancer | 81 | 1.24(0.75–2.04) | 1.47(0.87–2.48) | 1.06(0.62–1.80) | 1.22(0.70–2.12) |
| Non-small cell carcinoma | 73 | 1.42(0.85–2.37) | 1.68(0.98–2.87) | 1.03(0.59–1.81) | 1.15(0.65–2.07) |
| Squamous cell carcinoma | 14 | 0.57(0.13–2.58) | 0.67(0.14–3.13) | 0.27(0.04–2.07) | 0.31(0.04–2.44) |
| Adenocarcinoma | 24 | 1.36(0.56–3.30) | 1.41(0.56–3.54) | 1.71(0.72–4.05) | 1.81(0.74–4.43) |
| Large cell carcinoma | 1 | - | - | - | - |
| Other | 34 | 2.01(0.99–4.08) | 2.77(1.29–5.96) | 1.02(0.44–2.35) | 1.22(0.51–2.93) |
| Small cell carcinoma | 8 | - | - | 1.35(0.27–6.76) | 1.54(0.29–8.25) |
| Current-smoker | |||||
| All lung cancer | 363 | 0.86(0.67–1.11) | 0.81(0.62–1.07) | 0.92(0.70–1.21) | 0.93(0.70–1.25) |
| Non-small cell carcinoma | 293 | 0.86(0.64–1.14) | 0.85(0.63–1.14) | 0.90(0.66–1.23) | 0.97(0.70–1.34) |
| Squamous cell carcinoma | 69 | 0.48(0.24–0.98) | 0.54(0.27–1.11) | 0.57(0.27–1.20) | 0.70(0.33–1.48) |
| Adenocarcinoma | 97 | 0.80(0.49–1.30) | 0.72(0.42–1.21) | 1.17(0.72–1.89) | 1.14(0.69–1.89) |
| Large cell carcinoma | 3 | 2.07(0.19–23.10) | 2.36(0.21–26.88) | - | - |
| Other | 124 | 1.15(0.76–1.74) | 1.16(0.75–1.80) | 0.90(0.55–1.47) | 0.98(0.59–1.65) |
| Small cell carcinoma | 70 | 0.89(0.50–1.58) | 0.70(0.37–1.30) | 0.99(0.54–1.83) | 0.79(0.40–1.57) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, D.H.; Kwon, S.O.; Kim, S.-Y.; Kim, W.J. Air Pollution and Incidence of Lung Cancer by Histological Type in Korean Adults: A Korean National Health Insurance Service Health Examinee Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 915. https://doi.org/10.3390/ijerph17030915
Moon DH, Kwon SO, Kim S-Y, Kim WJ. Air Pollution and Incidence of Lung Cancer by Histological Type in Korean Adults: A Korean National Health Insurance Service Health Examinee Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(3):915. https://doi.org/10.3390/ijerph17030915
Chicago/Turabian StyleMoon, Da Hye, Sung Ok Kwon, Sun-Young Kim, and Woo Jin Kim. 2020. "Air Pollution and Incidence of Lung Cancer by Histological Type in Korean Adults: A Korean National Health Insurance Service Health Examinee Cohort Study" International Journal of Environmental Research and Public Health 17, no. 3: 915. https://doi.org/10.3390/ijerph17030915