The Association between the Australian Alcopops Tax and National Chlamydia Rates among Young People—an Interrupted Time Series Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Chlamydia Notification Data
2.2. Denominator Data: Resident Population and Chlamydia Test Data
2.3. Outcome Measures: Population-Based and Test Positivity Rates
2.4. Socio-Economic Data
2.5. Ready-to-Drink Beverage Consumption Data
2.6. Statistical Analysis
2.6.1. Independent Variables
2.6.2. Lagged Associations
2.6.3. Sensitivity Analyses
2.7. Ethics
3. Results
3.1. Descriptive Statistics
3.1.1. Primary Outcome Measure
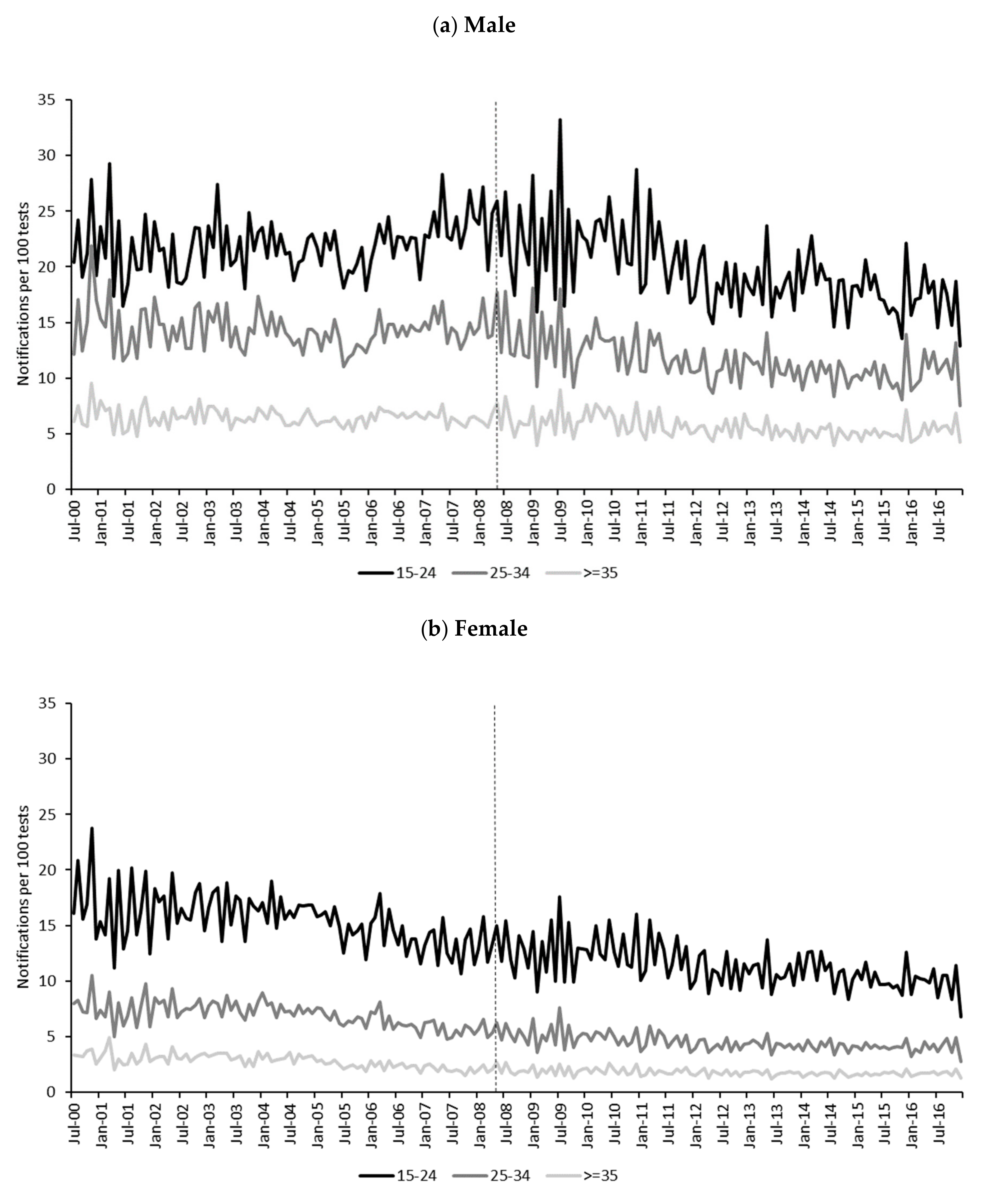
3.1.2. Secondary Outcome Measure
3.2. ARIMA Models
3.2.1. Primary Outcome Measure
3.2.2. Secondary Outcome Measure
3.2.3. Sensitivity Analyses

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Immediate | 3 Month Lag | 6 Month Lag | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | Gender | Model | SR2 | Q | df | p | Est | SE | p | Est | SE | p | Est | SE | p |
| 15–24 | Male | (0,1,1) (0,1,1)12 | 0.61 | 13.65 | 16 | 0.63 | 0.004 | 0.003 | 0.22 | 0.003 | 0.003 | 0.35 | 0.002 | 0.003 | 0.61 |
| Female | (0,1,1) (0,1,0)12 | 0.45 | 19.99 | 17 | 0.28 | -0.002 | 0.005 | 0.71 | −0.002 | 0.005 | 0.73 | −0.001 | 0.005 | 0.84 | |
| 25–34 | Male | (0,1,1) (0,1,0)12 | 0.45 | 19.24 | 17 | 0.32 | -0.002 | 0.004 | 0.60 | −0.004 | 0.005 | 0.41 | −0.004 | 0.005 | 0.34 |
| Female | (0,0,0) (0,1,0)12 | 0.25 | 27.73 | 18 | 0.07 | -0.032 | 0.027 | 0.23 | −0.036 | 0.027 | 0.18 | −0.021 | 0.027 | 0.44 | |
| Immediate | 3 Month Lag | 6 Month Lag | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | Gender | Model | SR2 | Q | df | p | Est | SE | p | Est | SE | p | Est | SE | p |
| 15–24 | Male | (0,0,2) (1,0,0)12 | 0.69 | 21.19 | 16 | 0.17 | −0.865 | 0.688 | 0.21 | −1.181 | 0.689 | 0.09 | −1.439* | 0.688 | 0.04 |
| Female | (0,0,0) (1,0,0)12 | 0.80 | 33.91* | 17 | 0.01 | −0.307 | 0.436 | 0.48 | −0.199 | 0.448 | 0.66 | −0.196 | 0.456 | 0.67 | |
| 25–34 | Male | (0,0,0) (1,0,0)12 | 0.80 | 16.67 | 17 | 0.48 | −0.726* | 0.311 | 0.02 | −0.970* | 0.306 | <0.01 | −1.168* | 0.304 | <0.001 |
| Female | (1,0,1) (1,0,0)12 | 0.90 | 18.08 | 15 | 0.26 | −0.192 | 0.161 | 0.23 | −0.136 | 0.161 | 0.40 | −0.197 | 0.160 | 0.22 | |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Babor, T.; Caetano, R.; Casswell, S.; Edwards, G.; Giesbrecht, N.; Graham, K.; Grube, J. Alcohol: No Ordinary Commodity. Research and Public Policy, 2nd ed.; OUP: Oxford, UK, 2010. [Google Scholar]
- Gilmore, W.; Chikritzhs, T.; Stockwell, T.; Jernigan, D.; Naimi, T.; Gilmore, I. Alcohol: Taking a population perspective. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 426. [Google Scholar] [CrossRef] [Green Version]
- Wagenaar, A.; Salois, M.; Komro, K. Effects of beverage alcohol price and tax levels on drinking: A meta-analysis of 1003 estimates from 112 studies. Addiction 2009, 104, 179–190. [Google Scholar] [CrossRef]
- Wagenaar, A.; Tobler, A.; Komro, K. Effects of Alcohol Tax and Price Policies on Morbidity and Mortality: A Systematic Review. Am. J. Public Health 2010, 100, 2270–2278. [Google Scholar] [CrossRef]
- National Alcohol and Drug Knowledgebase. Secondary analysis of 2016 National Drug Strategy Household Survey. Available online: https://nadk.flinders.edu.au/kb/alcohol/consumption-patterns/drinking-habits-of-australians/ (accessed on 17 September 2019).
- Australian Institute of Health and Welfare. Drinking Patterns in Australia, 2001-2007. Cat. No. PHE 133; AIHW: Canberra, Australia, 2010. [Google Scholar]
- Howard, S.J.; Gordon, R.; Jones, S.C. Australian alcohol policy 2001–2013 and implications for public health. BMC Public Health 2014, 14, 848. [Google Scholar] [CrossRef] [Green Version]
- Gale, M.; Muscatello, D.; Dinh, M.; Byrnes, J.; Shakeshaft, A.; Hayen, A.; MacIntyre, C.R.; Haber, P.; Cretikos, M.; Morton, P. Alcopops, taxation and harm: A segmented time series analysis of emergency department presentations. BMC Public Health 2015, 15, 468. [Google Scholar] [CrossRef] [Green Version]
- Shakeshaft, A.; Doran, C.M.; Byrnes, J. The role of research in the failure of the alcopops excise in Australia: What have we learned? Med. J. Aust. 2009, 191, 223–225. [Google Scholar] [CrossRef]
- Swan, W.; Roxon, N. Press Release: Increased Tax on ‘Ready to Drink’ Alcoholic Beverages; Australian Government: Canberra, Australia, 2008. [Google Scholar]
- Doran, C.M.; Digiusto, E. Using taxes to curb drinking: A report card on the Australian government’s alcopops tax. Drug Alcohol Rev. 2011, 30, 677–680. [Google Scholar] [CrossRef]
- Doran, C.M.; Shakeshaft, A.P. Using taxes to curb drinking in Australia. Lancet 2008, 372, 701–702. [Google Scholar] [CrossRef]
- Chikritzhs, T.; Dietze, P.; Allsop, S.; Daube, M.; Hall, W.; Kypri, K. The “alcopops” tax: Heading in the right direction. MJA 2009, 190, 294–295. [Google Scholar] [CrossRef] [Green Version]
- Skov, S.J.; Chikritzhs, T.N.; Kypri, K.; Miller, P.G.; Hall, W.D.; Daube, M.; Moodie, A.R. Is the “alcopops” tax working? Probably yes but there is a bigger picture. Med. J. Aust. 2011, 195, 3. [Google Scholar] [CrossRef]
- Muller, S.; Piontek, D.; Pabst, A.; Baumeister, S.E.; Kraus, L. Changes in alcohol consumption and beverage preference among adolescents after the introduction of the alcopops tax in Germany. Addiction 2010, 105, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Lensvelt, E.; Liang, W.; Gilmore, W.; Gordon, E.; Hobday, M.; Chikritzhs, T. Effect of the Australian “Alcopops Tax” on Alcohol-Related Emergency Department Presentations for Injury in Two States. J. Stud. Alcohol Drugs 2016, 77, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S.; Pals, J.; White, A.; Connor, J.; Quek, L.-H.; Crilly, J.; Lawrence, D. Effect of the increase in “alcopops” tax on alcohol-related harms in young people: A controlled interrupted time series. Med. J. Aust. 2011, 195, 690–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisely, S.; Crowe, E.; Lawrence, D.; White, A.; Connor, J. A time series analysis of presentations to Queensland health facilities for alcohol-related conditions, following the increase in ‘alcopops’ tax. Aust. Psychiatr. Bull. Royal Aust. N. Z. Coll. Psychiatr. 2013, 21, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Kisely, S.; Lawrence, D. A time series analysis of alcohol-related presentations to emergency departments in Queensland following the increase in alcopops tax. J. Epidemiol. Commun. Health 2016, 70, 181. [Google Scholar] [CrossRef]
- Lintonen, T.; Nevalainen, J. Has the role of personal income in alcohol drinking among teenagers changed between 1983 and 2013: A series of nationally representative surveys in Finland. BMJ Open 2017, 7, e013994. [Google Scholar] [CrossRef] [Green Version]
- Rehm, J.; Gmel, G.E., Sr.; Gmel, G.; Hasan, O.S.M.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.V.; et al. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Status Report on Alcohol and Health; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Staras, S.A.S.; Livingston, M.D.; Wagenaar, A.C. Maryland Alcohol Sales Tax and Sexually Transmitted Infections. Am. J. Prev. Med. 2016, 50, e73–e80. [Google Scholar] [CrossRef] [Green Version]
- Staras, S.A.S.; Livingston, M.D.; Christou, A.M.; Jernigan, D.H.; Wagenaar, A.C. Heterogeneous population effects of an alcohol excise tax increase on sexually transmitted infections morbidity. Addiction 2014, 109, 904–912. [Google Scholar] [CrossRef]
- Markowitz, S.; Kaestner, R.; Grossman, M. An Investigation of the Effects of Alcohol Consumption and Alcohol Policies on Youth Risky Sexual Behaviors. Am. Econ. Rev. 2005, 95, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Chesson, H.; Harrison, P.; Kassler, W.J. Sex under the Influence: The Effect of Alcohol Policy on Sexually Transmitted Disease Rates in the United States. J. Law Econ. 2000, 43, 215–238. [Google Scholar] [CrossRef] [PubMed]
- Harrison, P.; Kassler, W. Alcohol Policy and Sexually Transmitted Disease Rates—United States, 1981–1995. Morb. Mortal. Wkly Rep. 2000, 49, 346–349. [Google Scholar]
- Sen, A.; Luong, M.A.Y. Estimating the Impact of Beer Prices on the Incidence of Sexually Transmitted Diseases: Cross-Province and Time Series Evidence from Canada. Contemp. Econ. Policy 2008, 26, 505–517. [Google Scholar] [CrossRef]
- Ali, H.; Guy, R.J.; Fairley, C.K.; Wand, H.; Chen, M.Y.; Dickson, B.; Connor, C.C.; Marshall, L.; Grulich, A.E.; Kaldor, J.M.; et al. Understanding trends in genital Chlamydia trachomatis can benefit from enhanced surveillance: Findings from Australia. Sex. Transm. Infect. 2012, 88, 552. [Google Scholar] [CrossRef]
- Lau, A.; Spark, S.; Tomnay, J.; Smith, M.T.; Fairley, C.K.; Guy, R.J.; Donovan, B.; Hocking, J.S. Socio-demographic and structural barriers to being tested for chlamydia in general practice. Med. J. Aust. 2016, 204, 112.e111–112.e115. [Google Scholar] [CrossRef] [Green Version]
- Kirby Institute. HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: Annual Surveillance Report 2018; Kirby Institute, UNSW Sydney: Sydney, Australia, 2018. [Google Scholar]
- Callander, D.; Moreira, C.; El-Hayek, C.; Asselin, J.; van Gemert, C.; Watchirs Smith, L.; Nguyen, L.; Dimech, W.; Boyle, D.I.R.; Donovan, B.; et al. Monitoring the Control of Sexually Transmissible Infections and Blood-Borne Viruses: Protocol for the Australian Collaboration for Coordinated Enhanced Sentinel Surveillance (ACCESS). JMIR Res. Protoc. 2018, 7, e11028. [Google Scholar] [CrossRef]
- Abbott, T. Pilot Testing Program for Chlamydia: The Australian Government is Providing $12.5 Million over Four Years for Increased Awareness, Improved Surveillance and a Pilot Testing Program for Chlamydia; Office for the Minister for Health and Ageing: Canberra, Australia, 2005. [Google Scholar]
- Hocking, J.S.; Walker, J.; Regan, D.; Chen, M.Y.; Fairley, C.K. Chlamydia screening—Australia should strive to achieve what others have not. Med. J. Aust. 2008, 188, 106–108. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2016, 46, 348–355. [Google Scholar] [CrossRef] [Green Version]
- Lagarde, M. How to do (or not to do)... Assessing the impact of a policy change with routine longitudinal data. Health Policy Plan 2012, 27, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Apparent Consumption of Alcohol, Australia, 2017–2018. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4307.0.55.0012017-18?OpenDocument (accessed on 18 September 2019).
- Ooi, C. Testing for sexually transmitted infections. Aust. Prescr. 2007, 30, 8–13. [Google Scholar] [CrossRef]
- Sanci, L.; Webb, M.; Hocking, J. Risk taking behaviour in adolescents. Aust. J. Gen. Pract. 2018, 47, 829–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cretikos, M.; Mayne, D.; Reynolds, R.; Spokes, P.; Madeddu, D. Testing-adjusted chlamydia notification trends in New South Wales, Australia, 2000 to 2010. West. Pac. Surveill. Response J. 2014, 5, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, H.; Donovan, B.; Liu, B.; Hocking, J.S.; Agius, P.; Ward, J.; Bourne, C.; Kaldor, J.M.; Guy, R.J. Chlamydia prevention indicators for Australia: Review of the evidence from New South Wales. Sex. Health 2012, 9, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Medicare Benefits Schedule State/Territory Data Extract 2013–2014. Metadata on Date of Medicare Service. Available online: https://meteor.aihw.gov.au/content/index.phtml/itemId/603319 (accessed on 11 July 2019).
- Australian National Audit Office. Administration of Medicare Electronic Claiming Arrangements: An Independent Performance Audit in the Department of Human Services; ANAO: Canberra, Australia, 2017. [Google Scholar]
- McDowall, D.; McCleary, R.; Meidinger, E.; Hay, R. Interrupted Time Series Analysis; SAGE: Thousand Oaks, CA, USA, 1980. [Google Scholar] [CrossRef]
- Latreille, S.; Collyer, A.; Temple-Smith, M. Finding a segue into sex: Young men’s views on discussing sexual health with a GP. Aust. Fam. Physician 2014, 43, 217–221. [Google Scholar]
- Price, M.J.; Ades, A.E.; Soldan, K.; Welton, N.J.; Macleod, J.; Simms, I.; DeAngelis, D.; Turner, K.M.E.; Horner, P.J. The natural history of Chlamydia trachomatis infection in women: A multi parameter evidence synthesis. Health Technol. Assess 2016, 20. [Google Scholar] [CrossRef] [Green Version]
- de Attayde Silva, M.J.P.M.; Dantas Florêncio, G.L.; Erbolato Gabiatti, J.R.; do Amaral, R.L.; Júnior, J.E.; da Silveira Gonçalves, A.K. Perinatal morbidity and mortality associated with chlamydial infection: A meta-analysis study. Braz. J. Infect. Dis. 2011, 15, 533–539. [Google Scholar] [CrossRef] [Green Version]
- Australasian Sexual Health Alliance. Australian STI Management Guidelines for Use in Primary Care. Available online: http://www.sti.guidelines.org.au (accessed on 20 September 2019).
- Hocking, J.S.; Temple-Smith, M.; Guy, R.; Donovan, B.; Braat, S.; Law, M.; Gunn, J.; Regan, D.; Vaisey, A.; Bulfone, L.; et al. Population effectiveness of opportunistic chlamydia testing in primary care in Australia: A cluster-randomised controlled trial. Lancet 2018, 392, 1413–1422. [Google Scholar] [CrossRef]
- Distilled Spirits Industry Council of Australia. Pre-Budget Submission 2007–2008; DSICA: Melbourne, Australia, 2008. [Google Scholar]
- Australian Institute of Health and Welfare. Type of Alcohol Consumed, Recent Drinkers Aged 14 Years and Over, by Short-Term Risk Status, Australia, 2004. Unpublished Data from 2004 National Drug Strategy Household Survey Prepared by the Australian Institute of Health and Welfare; AIHW: Canberra, Australia, 2007. [Google Scholar]
- de Visser, R.O.; Badcock, P.B.; Rissel, C.; Richters, J.; Smith, A.M.A.; Grulich, A.E.; Simpson, J.M. Safer sex and condom use: Findings from the Second Australian Study of Health and Relationships. Sex. Health 2014, 11, 495–504. [Google Scholar] [CrossRef]




| Age | Gender | Notifications | Pre-Alcopops Tax | Post-Alcopops Tax | |||
|---|---|---|---|---|---|---|---|
| Jul 2000 to April 2008 (N = 94) | May 2008 to Dec 2016 (N = 104) | ||||||
| n | % | Median | IQR | Median | IQR | ||
| Per 100,000 population | |||||||
| 15–24 | Male | 195,986 | 20.4 | 39.6 | 26.0–53.0 | 88.0 | 81.5–93.4 |
| Female | 385,047 | 40.1 | 89.5 | 62.4–110.1 | 173 | 159–187 | |
| 25–34 | Male | 135,960 | 14.2 | 29.3 | 20.5–35.5 | 56.0 | 49.2–61.4 |
| Female | 131,851 | 13.7 | 27.8 | 20.3–36.3 | 55.3 | 47.9–59.7 | |
| 35 and older | Male | 72,966 | 7.6 | 4.0 | 3.1–5.3 | 8.4 | 7.3–9.4 |
| Female | 38,884 | 4.1 | 2.1 | 1.6–2.6 | 4.3 | 3.7–4.9 | |
| Total | 960,694 | 100 | 18.3 | 12.6–23.2 | 36.3 | 33.1–38.4 | |
| Per 100 tests | |||||||
| 15–24 | Male | 195,986 | 20.4 | 21.8 | 20.1–23.5 | 18.9 | 17.3–22.1 |
| Female | 385,047 | 40.1 | 15.4 | 13.8–16.9 | 11.0 | 10.0–12.6 | |
| 25–34 | Male | 135,960 | 14.2 | 14.2 | 13.0–15.3 | 11.3 | 10.2–12.6 |
| Female | 131,851 | 13.7 | 6.9 | 6.1–7.8 | 4.3 | 4.0–4.9 | |
| 35 and older | Male | 72,966 | 7.6 | 6.4 | 6.0–7.0 | 5.4 | 4.9–6.2 |
| Female | 38,884 | 4.1 | 2.8 | 2.3–3.2 | 1.7 | 1.6–2.0 | |
| Total | 960,694 | 100 | 10.9 | 10.0–11.8 | 7.8 | 7.0–9.0 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilmore, W.; Chikritzhs, T.; McManus, H.; Kaldor, J.; Guy, R. The Association between the Australian Alcopops Tax and National Chlamydia Rates among Young People—an Interrupted Time Series Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1343. https://doi.org/10.3390/ijerph17041343
Gilmore W, Chikritzhs T, McManus H, Kaldor J, Guy R. The Association between the Australian Alcopops Tax and National Chlamydia Rates among Young People—an Interrupted Time Series Analysis. International Journal of Environmental Research and Public Health. 2020; 17(4):1343. https://doi.org/10.3390/ijerph17041343
Chicago/Turabian StyleGilmore, William, Tanya Chikritzhs, Hamish McManus, John Kaldor, and Rebecca Guy. 2020. "The Association between the Australian Alcopops Tax and National Chlamydia Rates among Young People—an Interrupted Time Series Analysis" International Journal of Environmental Research and Public Health 17, no. 4: 1343. https://doi.org/10.3390/ijerph17041343