Facilitators and Barriers Associated with Uptake of HIV Self-Testing among Men Who Have Sex with Men in Chongqing, China: A Cross-Sectional Survey

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
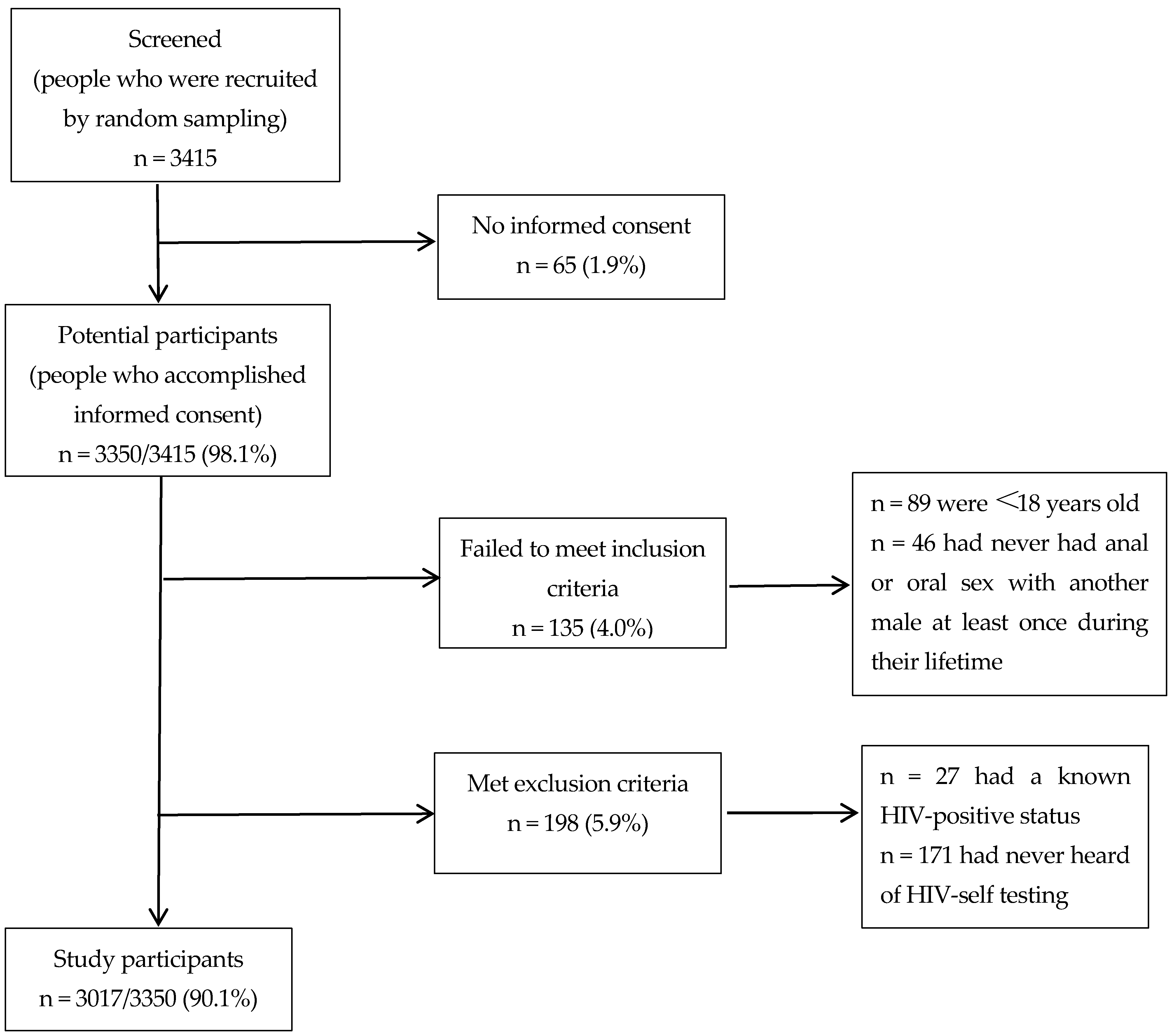
2.2. Study Design and Participants
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Sociodemographic Characteristics and HIVST Uptake
3.2. Accuracy
3.3. Binary Logistic Regression to Identify Factors Influencing HIV Self-Testing
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singh, S.; Song, R.; Johnson, A.S.; McCray, E.; Hall, H.I. HIV incidence, prevalence, and undiagnosed infections in US men who have sex with men. Ann. Intern. Med. 2018, 168, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Beyrer, C.; Baral, S.D.; Van Griensven, F.; Goodreau, S.M.; Chariyalertsak, S.; Wirtz, A.L.; Brookmeyer, R. Global epidemiology of HIV infection in men who have sex with men. Lancet 2012, 380, 367–377. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS. The Gap Report of Site; UNAIDS: New York, NY, USA, 2014; Volume 2014, Available online: http://files.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2014/UNAIDS_Gap_report_en.pdf (accessed on 7 October 2016).
- National Health and Family Planning Commission of the People’s Republic of China. China AIDS Response Progress Report; Chinese Health and Family Planning Commission: Beijing, China, 2015; Available online: http://www.unaids.org/sites/default/files/country/documents/CHN_narrative_report_2015.pdf (accessed on 12 October 2016).
- Tang, S.; Tang, W.; Meyers, K.; Chan, P.; Chen, Z.; Tucker, J.D. HIV and syphilis among men who have sex with men and transgender individuals in China: A scoping review. Lancet 2016, 388, S74. [Google Scholar] [CrossRef]
- Zeng, X.; Zhong, X.; Peng, B.; Zhang, Y.; Kong, C.; Liu, X.; Huang, A. Prevalence and associated risk characteristics of HIV infection based on anal sexual role among men who have sex with men: A multi-city cross-sectional study in Western China. Int. J. Infect. Dis. 2016, 49, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walensky, R.P.; Freedberg, K.A.; Weinstein, M.C.; Paltiel, A.D. Cost-effectiveness of HIV testing and treatment in the United States. Clin. Infect. Dis. 2007, 45, S248–S254. [Google Scholar] [CrossRef] [PubMed]
- 90–90–90 An Ambitious Treatment Target to Help End the AIDS Epidemic of Site. Available online: http://www.unaids.org/ (accessed on 15 November 2016).
- Technology Landscape HIV Rapid Diagnostic Tests for Self-Testing of Site. Available online: http://unitaid.eu/assets/UNITAID_HIV_rapid_diagnostic_tests_for_self-testing.pdf (accessed on 17 November 2016).
- WHO Claimed 30% HIV Infected Remain Undiagnosed and Encouraged More HIV Testing in China. 2015. Available online: http://china.caixin.com/2015-12-01/100880481.html (accessed on 18 November 2016).
- Nitika, P.P.; Jigyasa, S.; Sushmita, S.; Sabrina, P.; Caroline, V.; Lawrence, J.; Keertan, D.; Peeling, R.W. Supervised and unsupervised self-testing for HIV in high-and low-risk populations: A systematic review. PLoS Med. 2013, 10, e1001414. [Google Scholar]
- Ren, X.L.; Wu, Z.Y.; Mi, G.D.; Mcgoogan, J.; Rou, K.M.; Yan, Z. Uptake of HIV self-testing among men who have sex with men in Beijing, China: A cross-sectional study. Biomed. Environ. Sci. 2017, 30, 407–417. [Google Scholar]
- Tao, J.; Li, M.; Qian, H.; Wang, L.; Zhang, Z.; Ding, H.; Ji, Y.; Li, D.; Xiao, D.; Hazlitt, M. Home-based HIV testing for men who have sex with men in China: A novel community-based partnership to complement government programs. PLoS ONE 2014, 9, e102812. [Google Scholar] [CrossRef]
- Liu, Y.; Sun, X.; Qian, H.; Yin, L.; Yan, Z.; Wang, L.; Jiang, S.; Lu, H.; Ruan, Y.; Shao, Y. Qualitative assessment of barriers and facilitators of access to HIV testing among men who have sex with men in China. AIDS Patient Care STDs 2015, 29, 481–489. [Google Scholar] [CrossRef]
- Wei, C.; Yan, H.; Yang, C.; Raymond, H.F.; Li, J.; Yang, H.; Zhao, J.; Huan, X.; Stall, R. Accessing HIV testing and treatment among men who have sex with men in China: A qualitative study. AIDS Care 2014, 26, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Estem, K.S.; Catania, J.; Klausner, J.D. HIV self-testing: A review of current implementation and fidelity. Curr. HIV/AIDS Rep. 2016, 13, 107–115. [Google Scholar] [CrossRef]
- Xun, H.; Kang, D.; Huang, T.; Qian, Y.; Li, X.; Wilson, E.C.; Yang, S.; Jiang, Z.; Gong, C.; Tao, X. Factors associated with willingness to accept oral fluid HIV rapid testing among most-at-risk populations in China. PLoS ONE 2013, 8, e80594. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhang, Z.; Li, D.; Liu, Y.; Pan, S.W.; Qi, X.; Wang, B.; Luo, F.; Xiao, D.; Shao, Y. Willingness to use the oral fluid HIV rapid test among men who have sex with men in Beijing, China. PLoS ONE 2013, 8, e64652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HIV/AIDS. HIVST of Site. Available online: https://www.who.int/hiv/topics/self-testing/en/ (accessed on 17 November 2019).
- Han, L.; Candidate, B.; Bien, C.H.; Wei, C.; Muessig, K.E.; Yang, M.; Candidate, B.; Liu, F.; Yang, L.; Meng, G. HIV self-testing among online MSM in China: Implications for expanding HIV testing among key populations. J. Acquir. Immune Defic. Syndr. 2014, 67, 216–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, D.A.; Golden, M.R.; Hughes, J.P.; Farquhar, C.; Stekler, J. Acceptability and ease of use of home self-testing for HIV among men who have sex with men. In Proceedings of the 19th Conference on Retroviruses and Opportunistic Infections, Seattle, WA, USA, 5–8 March 2012. [Google Scholar]
- Carballo-Diéguez, A.; Frasca, T.; Dolezal, C.; Balan, I. Will gay and bisexually active men at high risk of infection use over-the-counter rapid HIV tests to screen sexual partners? J. Sex Res. 2012, 49, 379–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, F.; Tang, W.; Cheng, W.; Lin, P.; Wu, Q.; Cai, Y.; Tang, S.; Fan, L.; Zhao, Y.; Chen, X. Acceptability and feasibility of a social entrepreneurship testing model to promote HIV self-testing and linkage to care among men who have sex with men. HIV Med. 2017, 18, 376–382. [Google Scholar] [CrossRef]
- Wong, H.T.H.; Tam, H.Y.; Chan, D.P.C.; Lee, S.S. Usage and acceptability of HIV self-testing in men who have sex with men in Hong Kong. AIDS Behav. 2015, 19, 505–515. [Google Scholar] [CrossRef]
- Kinney, S.; Lea, C.; Kearney, G.; Kinsey, A.; Amaya, C. Predictors for using a hiv self-test among migrant and seasonal farmworkers in North Carolina. Int. J. Environ. Res. Public Health 2015, 12, 8348–8358. [Google Scholar] [CrossRef] [Green Version]
- Choko, A.T.; MacPherson, P.; Webb, E.L.; Willey, B.A.; Feasy, H.; Sambakunsi, R.; Mdolo, A.; Makombe, S.D.; Desmond, N.; Hayes, R. Uptake, accuracy, safety, and linkage into care over two years of promoting annual self-testing for hiv in blantyre, malawi: A community-based prospective study. PLoS Med. 2015, 12, e1001873. [Google Scholar] [CrossRef] [Green Version]
- Krause, J.; Subklew-Sehume, F.; Kenyon, C.; Colebunders, R. Acceptability of hiv self-testing: A systematic literature review. BMC Public Health 2013, 1, 735. [Google Scholar] [CrossRef] [Green Version]
- De la Fuente, L.; Rosales-Statkus, M.E.; Hoyos, J.; Pulido, J.; Santos, S.; Bravo, M.J.; Barrio, G.; Fernández-Balbuena, S.; Belza, M.J.; Madrid Rapid HIV Testing Group. Are participants in a street-based HIV testing program able to perform their own rapid test and interpret the results? PLoS ONE 2012, 7, e46555. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Roehler, M.; Miller, T.; Kardos, K.; Almeidasantos, A. Development of an oral fluid self-test for HIV infection: Evaluation in a population of unknown risk. In Proceedings of the XIX International AIDS Conference, Washington, DC, USA, 22–27 July 2012. [Google Scholar]
- Tang, W.; Wu, D. Opportunities and challenges for HIVST in China. Lancet HIV 2018, 5, e611–e612. [Google Scholar] [CrossRef]
- Zhang, C.; Li, X.; Brecht, M.-L.; Koniak-Griffin, D. Can self-testing increase HIV testing among men who have sex with men: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0188890. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.R.; Patel, S.; Clarke, E.; Khan, A.W.; Doshi, B.; Radcliffe, K.W.; European Collaborative Clinical Group (ECCG). Guidance and practice on frequency of HIV and sexually transmitted infection testing in men who have sex with men–what is the European situation? Int. J. STD AIDS 2014, 25, 213–218. [Google Scholar] [CrossRef]
- Templeton, D.J.; Read, P.; Varma, R.; Bourne, C. Australian sexually transmissible infection and HIV testing guidelines for asymptomatic men who have sex with men 2014: A review of the evidence. Sex. Health 2014, 11, 217–229. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.; Le, B.; Finlayson, T.; Oster, A.; DiNenno, E. Prevalence and awareness of HIV infection among men who have sex with men-21 cities, United States, 2008. Morb. Mortal. Wkly. Rep. 2010, 59, 1201–1207. [Google Scholar]
- The Gap Report [EB/OL] of Site. Available online: http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_en.pdf (accessed on 2 May 2017).
- Pilcher, C.D.; Louie, B.; Facente, S.; Keating, S.; Hackett, J., Jr.; Vallari, A.; Hall, C.; Dowling, T.; Busch, M.P.; Klausner, J.D. Performance of rapid point-of-care and laboratory tests for acute and established HIV infection in San Francisco. PLoS ONE 2013, 8, e80629. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.E.; El-Sadr, W.M.; Zerbe, A.; Branson, B.M. Rapid HIV self-testing: Long in coming but opportunities beckon. Aids 2013, 27, 1687–1695. [Google Scholar] [CrossRef] [Green Version]
- Yan, H.; Yang, H.; Raymond, H.F.; Li, J.; Shi, L.E.; Huan, X.; Wei, C. Experiences and correlates of HIV self-testing among men who have sex with men in Jiangsu province, China. AIDS Behav. 2015, 19, 485–491. [Google Scholar] [CrossRef] [Green Version]
- Kurth, A.E.; Cleland, C.M.; Chhun, N.; Sidle, J.E.; Were, E.; Naanyu, V.; Emonyi, W.; Macharia, S.M.; Sang, E.; Siika, A.M. Accuracy and Acceptability of Oral Fluid HIV Self-Testing in a General Adult Population in Kenya. Aids Behav. 2016, 20, 870–879. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Lu, H.; Raymond, H.F.; Sun, Y.; Jia, Y.; He, X.; Fan, S.; Shao, Y.; McFarland, W.; Xiao, Y.; et al. Untested and undiagnosed: Barriers to HIV testing among men who have sex with men, Beijing, China. Sex. Transm. Infect. 2012, 88, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, Z.; Tang, Z.; Nong, Q.; Li, Y. Promoting HIV testing with home self-test kit among men who have sex with men in China: A feasibility study. Lancet 2015, 386, S68. [Google Scholar] [CrossRef]


{kind=link}
| Constructs | Items |
|---|---|
| Basic knowledge | Is AIDS an incurable severe infectious disease? |
| Are MSM a group of people who are currently the most severely affected by HIV in China? | |
| Can you identify a positive patient by their appearance? | |
| Do sexually transmitted diseases (STDs) increase the risk of HIV infection? | |
| Does using a condom correctly protect against HIV transmission? | |
| Does using new drugs (methamphetamine, ecstasy, K powder, and so on) increase the risk of HIV infection? | |
| Should HIV testing and counseling be actively sought-after high-risk behaviors (needle sharing, drug use, unsafe sex, etc.)? | |
| Does intentional transmission of HIV/AIDS bear legal responsibility? |
| Characteristics | All Participants | Uptake of HIVST (n = 470) | |
|---|---|---|---|
| (n = 3017) | n | Percent (95% CI) | |
| Age | |||
| 18–26 years old | 1272 | 254 | 20.0% (17.8%–22.3%) |
| 27–36 years old | 1283 | 179 | 14.0% (12.1%–16.0%) |
| 37–76 years old | 462 | 36 | 7.8% (5.5%–10.6%) |
| Marital status | |||
| Unmarried | 2623 | 439 | 16.7% (15.3%–18.2%) |
| Married | 392 | 30 | 7.7% (5.2%–10.7%) |
| Ethnicity | |||
| Han | 2990 | 463 | 15.5% (14.2%–16.8%) |
| Minority | 27 | 6 | 22.2% (8.6%–42.3%) |
| Household registration | |||
| Chongqing | 2397 | 342 | 14.3% (12.9%–15.7%) |
| Other provinces | 620 | 127 | 20.5% (17.4%–23.9%) |
| Duration of residency in Chongqing | |||
| <1 year | 89 | 22 | 24.7% (16.2%–35.0%) |
| 1–2 years | 63 | 11 | 17.5% (9.1%–29.1%) |
| >2 years | 2865 | 436 | 15.2% (13.9%–16.6%) |
| Highest level of education | |||
| Junior high school and below | 235 | 19 | 8.1% (4.9%–12.3%) |
| High school or technical secondary school | 639 | 97 | 15.2% (12.5%–18.2%) |
| College and above | 2142 | 353 | 16.5% (14.9%–18.1%) |
| Sexual orientation | |||
| Homosexual | 2480 | 415 | 16.7% (15.3%–18.3%) |
| Heterosexual | 3 | 0 | |
| Bisexual | 481 | 45 | 9.4% (6.9%–12.3%) |
| Undetermined | 52 | 9 | 17.3% (8.2%–30.3%) |
| Number of HIV tests conducted in the last year | |||
| 0–1 time | 1900 | 321 | 16.1% (14.5%–17.8%) |
| ≥2 times | 374 | 148 | 39.6% (34.6%–44.7%) |
| Scores of basic HIV/AIDS knowledge | |||
| 0–5 | 241 | 23 | 9.5% (6.1%–14.0%) |
| 6–8 | 2776 | 446 | 16.1% (14.7%–17.5%) |
| HIV Antibody Detection Results | Total | ||
|---|---|---|---|
| Positive | Negative | ||
| Participant self-testing result | |||
| Positive | 118 | 3 | 121 |
| Negative | 41 | 301 | 342 |
| Total | 159 | 304 | 463 |
| Variable | Estimated Parameter | p-Value | OR 1 | 95.0% CI | aOR 2 | 95.0% CI |
|---|---|---|---|---|---|---|
| Age | ||||||
| 18–26 years old | 1.00 | 1.00 | ||||
| 27–36 years old | −0.43 | p < 0.001 * | 0.65 | 0.53–0.80 | 0.65 | 0.53–0.81 |
| ≥37 years old | −1.08 | p < 0.001 * | 0.34 | 0.24–0.49 | 0.37 | 0.26–0.55 |
| Highest level of education | ||||||
| Junior high school and below | 1.00 | 1.00 | ||||
| High school or secondary school | 0.71 | 0.007 * | 2.04 | 1.21–3.41 | 1.62 | 0.96–2.75 |
| College and above | 0.81 | 0.001 * | 2.24 | 1.38–3.64 | 1.67 | 1.02–2.75 |
| Marital status | ||||||
| Unmarried | 1.00 | 1.00 | ||||
| Married | −0.89 | p < 0.001 * | 0.41 | 0.28–0.61 | 0.64 | 0.42–0.98 |
| Ethnicity | ||||||
| Han ethnicity | 1.00 | 1.00 | ||||
| Minor ethnicity | 0.44 | 0.340 | 1.56 | 0.63–3.88 | 1.50 | 0.60–3.78 |
| Duration of residing in Chongqing | ||||||
| <1 year | 1.00 | 1.00 | ||||
| 1–2 years | −0.44 | 0.287 | 0.64 | 0.29–1.45 | 0.61 | 0.27–1.37 |
| >2 years | −0.60 | 0.016 * | 0.55 | 0.33–0.89 | 0.58 | 0.35–0.95 |
| Scores of basic HIV/AIDS knowledge | ||||||
| 0–5 | 1.00 | 1.00 | ||||
| 6–8 | 0.60 | 0.008 * | 1.8 | 1.17–2.82 | 1.66 | 1.06–2.61 |
| Frequency of condom use when having sex with other men | ||||||
| Never | 1.00 | 1.00 | ||||
| Sometimes | 0.13 | 0.657 | 1.14 | 0.64–2.03 | 1.07 | 0.60–1.93 |
| Every time | −0.25 | 0.401 | 0.78 | 0.44–1.39 | 0.73 | 0.41–1.131 |
| How many regular male sexual partners have you had in the last 6 months? | ||||||
| Zero | 1.00 | 1.00 | ||||
| One | 0.16 | 0.376 | 1.17 | 0.83–1.66 | 1.20 | 0.84–1.71 |
| Two | 0.15 | 0.456 | 1.17 | 0.78–1.74 | 1.18 | 0.79–1.778 |
| More than three | 0.29 | 0.365 | 1.34 | 0.71–2.52 | 1.47 | 0.78–2.80 |
| Number of HIV tests done conducted in the last year | ||||||
| 0–1 time | 1.00 | 1.00 | ||||
| ≥2 times | 1.23 | p < 0.001 * | 3.41 | 2.68–4.33 | 3.34 | 2.62–4.25 |
| Have you ever taken drugs? | ||||||
| Yes | 1.00 | 1.00 | ||||
| No | 0.280 | 0.482 | 1.32 | 0.61–2.88 | 1.29 | 0.59–2.82 |
| Have you ever been diagnosed with STDs? | ||||||
| Yes | 1.00 | 1.00 | ||||
| No | 0.46 | 0.88 | 1.58 | 0.93–2.69 | 1.54 | 0.90–2.62 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Wu, G.; Lu, R.; Ou, R.; Hu, L.; Yin, Y.; Zhang, Y.; Yan, H.; Zhao, Y.; Luo, Y.; et al. Facilitators and Barriers Associated with Uptake of HIV Self-Testing among Men Who Have Sex with Men in Chongqing, China: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 1634. https://doi.org/10.3390/ijerph17051634
Liu Y, Wu G, Lu R, Ou R, Hu L, Yin Y, Zhang Y, Yan H, Zhao Y, Luo Y, et al. Facilitators and Barriers Associated with Uptake of HIV Self-Testing among Men Who Have Sex with Men in Chongqing, China: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2020; 17(5):1634. https://doi.org/10.3390/ijerph17051634
Chicago/Turabian StyleLiu, Ying, Guohui Wu, Rongrong Lu, Rong Ou, Ling Hu, Yiping Yin, Yangchang Zhang, Hongjia Yan, Yong Zhao, Yetao Luo, and et al. 2020. "Facilitators and Barriers Associated with Uptake of HIV Self-Testing among Men Who Have Sex with Men in Chongqing, China: A Cross-Sectional Survey" International Journal of Environmental Research and Public Health 17, no. 5: 1634. https://doi.org/10.3390/ijerph17051634