

Cardiac and Mental Benefits of Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet plus Forest Bathing (FB) versus MIND Diet among Older Chinese Adults: A Randomized Controlled Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Selection Criteria
2.3. Sample Size
2.4. Intervention and Control
2.4.1. MIND Diet Intervention
2.4.2. MIND-plus-FB Intervention
2.4.3. Control Group
2.5. Primary and Secondary Outcomes
2.6. Statistical Methods
3. Results
3.1. Study Population
3.2. Baseline Characteristics
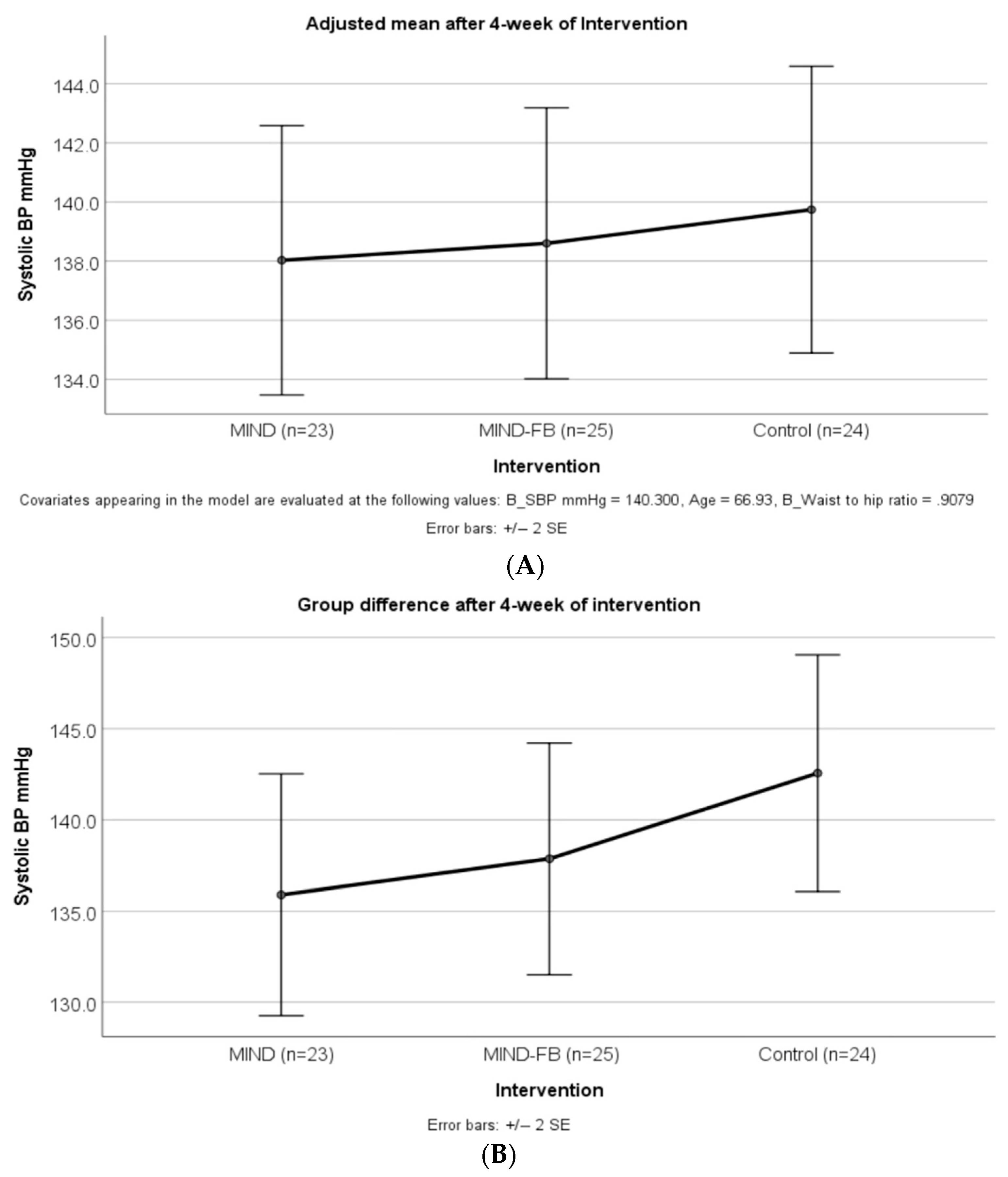
3.3. The Intervention Effect on BP
3.4. Intervention Effect on Other Variables
4. Discussion
Limitation and Implication
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centre for Health Protection. Department of Health. The Government of the Hong Kong Special Administrative Region. Report of Population Health Survey 2014/2015. 2017; pp. 1–297. Available online: https://www.chp.gov.hk/en/static/51256.html (accessed on 7 November 2022).
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.; Ha, S.C.; Luk, K.; Yip, W.; Tsang, C.S.; Wong, M. Update on the Hong Kong Reference Framework for Hypertension Care for Adults in Primary Care Settings—Review of evidence on the definition of high blood pressure and goal of therapy. Hong Kong Med. J. 2019, 25, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zheng, H.; Du, H.-B.; Tian, X.-P.; Jiang, Y.-J.; Zhang, S.-L.; Kang, Y.; Li, X.; Chen, J.; Lu, C.; et al. The multiple lifestyle modification for patients with prehypertension and hypertension patients: A systematic review protocol. BMJ Open 2014, 4, e004920. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Chen, Z.; Zhang, L.; Wang, X.; Hao, G.; Zhang, Z.; Shao, L.; Tian, Y.; Dong, Y.; Zheng, C.; et al. Status of Hypertension in China. Circulation 2018, 137, 2344–2356. [Google Scholar] [CrossRef]
- Zhang, Y.; Moran, A.E. Trends in the Prevalence, Awareness, Treatment, and Control of Hypertension among Young Adults in the United States, 1999 to 2014. Hypertension 2017, 70, 736–742. [Google Scholar] [CrossRef]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Fu, J.; Liu, Y.; Zhang, L.; Zhou, L.; Li, D.; Quan, H.; Zhu, L.; Hu, F.; Li, X.; Meng, S.; et al. Nonpharmacologic Interventions for Reducing Blood Pressure in Adults With Prehypertension to Established Hypertension. J. Am. Heart Assoc. 2020, 9, e016804. [Google Scholar] [CrossRef]
- Becerra-Tomás, N.; Blanco Mejía, S.; Viguiliouk, E.; Khan, T.; Kendall, C.W.C.; Kahleova, H.; Rahelić, D.; Sievenpiper, J.L.; Salas-Salvadó, J. Mediterranean diet, cardiovascular disease and mortality in diabetes: A systematic review and meta-analysis of prospective cohort studies and randomized clinical trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 1207–1227. [Google Scholar] [CrossRef]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. J. Nutr. 2019, 58, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Barnes, L.L.; Bennett, D.A.; Aggarwal, N.T. MIND diet slows cognitive decline with aging. Alzheimer’s Dement. 2015, 11, 1015–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminianfar, A.; Keshteli, A.H.; Esmaillzadeh, A.; Adibi, P. Association between adherence to MIND diet and general and abdominal obesity: A cross-sectional study. Nutr. J. 2020, 19, 1–9. [Google Scholar] [CrossRef]
- Berendsen, A.M.; Kang, J.H.; Feskens, E.J.M.; de Groot, C.P.G.M.; Grodstein, F.; Van De Rest, O. Association of long-term adherence to the mind diet with cognitive function and cognitive decline in American women. J. Nutr. Health Aging 2018, 22, 222–229. [Google Scholar] [CrossRef]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimer’s Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadpour, S.; Ghorbaninejad, P.; Janbozorgi, N.; Shab-Bidar, S. Associations between adherence to MIND diet and metabolic syndrome and general and abdominal obesity: A cross-sectional study. Diabetol. Metab. Syndr. 2020, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cherian, L.; Wang, Y.; Holland, T.; Agarwal, P.; Aggarwal, N.; Morris, M.C. DASH and Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) Diets Are Associated With Fewer Depressive Symptoms Over Time. J. Gerontol. Ser. A 2021, 76, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Yau, K.K.-Y.; Loke, A.Y. Effects of forest bathing on pre-hypertensive and hypertensive adults: A review of the literature. Environ. Health Prev. Med. 2020, 25, 1–17. [Google Scholar] [CrossRef]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.-S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef] [Green Version]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [Green Version]
- Cremonini, A.L.; Caffa, I.; Cea, M.; Nencioni, A.; Odetti, P.; Monacelli, F. Nutrients in the Prevention of Alzheimer’s Disease. Oxidative Med. Cell. Longev. 2019, 2019, 9874159. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, A.L.; Vryonis, M.M.; Protogerou, A.D.; Alexopoulos, E.C.; Achimastos, A.; Papadogiannis, D.; Chrousos, G.P.; Darviri, C. Stress management and dietary counseling in hypertensive patients: A pilot study of additional effect. Prim. Health Care Res. Dev. 2014, 15, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Leserman, J.; Stuart, E.M.; Mamish, M.E.; Deckro, J.P.; Beckman, R.J.; Friedman, R.; Benson, H. Nonpharmacologic Intervention for Hypertension. J. Cardiopulm. Rehabil. 1989, 9, 316–324. [Google Scholar] [CrossRef]
- Stuart, E.M.; Caudill, M.; Leserman, J.; Dorrington, C.; Friedman, R.; Benson, H. Nonpharmacologic treatment of hypertension: A multiple-risk-factor approach. J. Cardiovasc. Nurs. 1987, 1, 1–14. [Google Scholar] [CrossRef]
- Chen, S.T.; Maruthur, N.M.; Appel, L.J. The Effect of Dietary Patterns on Estimated Coronary Heart Disease Risk. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 484–489. [Google Scholar] [CrossRef] [Green Version]
- Agriculture, Fisheries and Conservation Department (AFCD). Available online: https://www.afcd.gov.hk/english/country/cou_vis/cou_vis_cou/cou_vis_cou_ttqbe/cou_vis_cou_ttqbe.html. (accessed on 1 September 2022).
- Chahine, M.N.; Topouchian, J.; Blacher¹, J.; Assemani, N.; Asmar, R.; Ibañez, I.; Agnoletti, D.; Youssef, A. Validation of four devices: Omron M6 Comfort, Omron HEM-7420, Withings BP-800, and Polygreen KP-7670 for home blood pressure measurement according to the European Society of Hypertension International Protocol. Vasc. Health Risk Manag. 2014, 10, 33–44. [Google Scholar] [CrossRef] [Green Version]
- Bolodeoku, J.; Pinkney, S. Imprecision Evaluation of Self-Monitoring of Blood Cholesterol ( SMBC ) Handheld Point of Care Testing Devices: Elemark TM and Cardiochek PA Results. Ann. Clin. Lab. Res. 2019, 7, 290. [Google Scholar] [CrossRef]
- Chen, K.-M.; Snyder, M.; Krichbaum, K. Translation and equivalence: The Profile of Mood States Short Form in English and Chinese. Int. J. Nurs. Stud. 2002, 39, 619–624. [Google Scholar] [CrossRef]
- Shek, D.T. The Chinese Version of the State-Trait Anxiety Inventory: Its Relationsnip to Differerent Measures of Psychological Well-Being. J. Clin. Psychol. 1993, 49, 349–358. [Google Scholar] [CrossRef]
- Rimm, E.B.; Giovannucci, E.L.; Stampfer, M.J.; Colditz, G.A.; Litin, L.B.; Willett, W.C. Reproducibility and Validity of an Expanded Self-Administered Semiquantitative Food Frequency Questionnaire among Male Health Professionals. Am. J. Epidemiol. 1992, 135, 1114–1126. [Google Scholar] [CrossRef]
- Feskanich, D.; Rimm, E.B.; Giovannucci, E.L.; Colditz, G.A.; Stampfer, M.J.; Litin, L.B.; Willett, W.C. Reproducibility and validity of food intake measurements from a semiquantitative food frequency questionnaire. J. Am. Diet. Assoc. 1993, 93, 790–796. [Google Scholar] [CrossRef]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Filippou, C.D.; Thomopoulos, C.G.; Kouremeti, M.M.; Sotiropoulou, L.I.; Nihoyannopoulos, P.I.; Tousoulis, D.M.; Tsioufis, C.P. Mediterranean diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021, 40, 3191–3200. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.; Byrne, M.L.; et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef] [Green Version]
- Arjmand, G.; Abbas-Zadeh, M.; Eftekhari, M.H. Effect of MIND diet intervention on cognitive performance and brain structure in healthy obese women: A randomized controlled trial. Sci. Rep. 2022, 12, 2871. [Google Scholar] [CrossRef]
- Fresán, U.; Bes-Rastrollo, M.; Segovia-Siapco, G.; Sanchez-Villegas, A.; Lahortiga, F.; de la Rosa, P.-A.; Martínez-Gonzalez, M.-A. Does the MIND diet decrease depression risk? A comparison with Mediterranean diet in the SUN cohort. J. Nutr. 2019, 58, 1271–1282. [Google Scholar] [CrossRef]
- Siervo, M.; Lara, J.; Chowdhury, S.; Ashor, A.; Oggioni, C.; Mathers, J.C. Effects of the Dietary Approach to Stop Hypertension (DASH) diet on cardiovascular risk factors: A systematic review and meta-analysis. Br. J. Nutr. 2015, 113, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Shirani, F.; Salehi-Abargouei, A.; Azadbakht, L. Effects of Dietary Approaches to Stop Hypertension (DASH) diet on some risk for developing type 2 diabetes: A systematic review and meta-analysis on controlled clinical trials. Nutrition 2013, 29, 939–947. [Google Scholar] [CrossRef]
- Devore, E.E.; Kang, J.H.; Breteler, M.M.B.; Grodstein, F. Dietary intakes of berries and flavonoids in relation to cognitive decline. Ann. Neurol. 2012, 72, 135–143. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Time | Invitation Activities | Required Physical Activity |
|---|---|---|
| 09:00–09:20 | Share the forest experience | sitting or standing |
| 09:20–09:30 | Sharing circle | sitting or standing |
| 09:30–09:50 | Pleasant of moment by five senses | sitting or standing |
| 09:50–10:00 | Sharing circle | sitting or standing |
| 10:00–10:20 | Slow down physically and mentally | wandering to the designed forest path |
| 10:20–10:30 | Sharing circle | sitting or standing |
| 10:30–10:50 | Build up connection to forest | strolling around the designed path |
| 10:50–11:00 | Sharing circle | sitting or standing |
| MIND Group (n = 23) | MIND-FB Group (n = 25) | Control Group (n = 24) | p Value across All Groups | ||
|---|---|---|---|---|---|
| Age Group | 0.041 | ||||
| <65 years | 9 (39.1) | 14 (56.0) | 5 (20.8) | ||
| 65 years or above | 14 (60.9) | 11 (44.0) | 19 (79.2) | ||
| Gender | 0.636 | ||||
| Female | 19 (82.6) | 19 (76.0) | 17 (70.8) | ||
| Male | 4 (17.4) | 6 (24.0) | 7 (29.2) | ||
| Educational level | 0.103 | ||||
| Primary or below | 8 (34.8) | 3 (12.0) | 12 (50.0) | ||
| Secondary | 10 (43.5) | 14 (56.0) | 10 (41.7) | ||
| Associate degree | 1 (4.3) | 3 (12.0) | 0 (0) | ||
| Bachelor’s degree | 1 (4.3) | 3 (12.0) | 0 (0) | ||
| Master’s degree | 3 (13.0) | 2 (8.0) | 1 (4.2) | ||
| Doctorate degree/PhD degree | 0 (0) | 0 (0) | 1 (4.2) | ||
| Current employment | 0.676 | ||||
| Employed Full time | 3 (13.0) | 5 (20.0) | 5 (20.8) | ||
| Employed Part time | 2 (8.7) | 1 (4.0) | 0 (0) | ||
| Homemaker | 5 (21.7) | 6 (24.0) | 3 (12.5) | ||
| Retired | 13 (56.5) | 13 (52.0) | 16 (66.7) | ||
| Marital Status | 0.559 | ||||
| Married | 15 (65.2) | 15 (60.0) | 12 (50.0) | ||
| Single/Divorced/Separated/Widow | 8 (34.8) | 10 (40.0) | 12 (50.0) | ||
| Frequency for exercise | 0.266 | ||||
| 1 to 2 times a week | 10 (43.5) | 14 (56.0) | 9 (37.5) | ||
| 3 to 4 times a week | 6 (26.1) | 5 (20.0) | 6 (25.0) | ||
| 5 to 6 times a week | 6 (26.1) | 3 (12.0) | 9 (37.5) | ||
| Never | 1 (4.3) | 3 (12.0) | 0 (0) | ||
| Times for exercise per session | 0.184 | ||||
| >40 min | 10 (43.5) | 5 (20.0) | 8 (33.3) | ||
| 30–40 min | 3 (13.0) | 9 (36.0) | 3 (12.5) | ||
| 20–30 min | 3 (13.0) | 3 (12.0) | 8 (33.3) | ||
| 10–20 min | 3 (13.0) | 2 (8.0) | 3 (12.5) | ||
| <10 min | 3 (13.0) | 3 (12.0) | 2 (8.3) | ||
| Never | 1 (4.3) | 3 (12.0) | 0 (0) | ||
| Smoking Habit | 0.357 | ||||
| Smoke 1–10 cigarettes a day | 1 (4.3) | 0 (0) | 0 (0) | ||
| Ex-smoker | 1 (4.3) | 0 (0) | 0 (0) | ||
| Never | 21 (91.3) | 25 (34.7) | 24 (33.3) | ||
| Drinking Habit | 0.280 | ||||
| More than fourteen times a week | 1 (4.3) | 0 (0) | 0 (0) | ||
| Five to seven times a week | 0 (0) | 1 (4.0) | 0 (0) | ||
| Once or twice a week | 1 (4.3) | 3 (12.0) | 0 (0) | ||
| Ex-drinker | 1 (4.3) | 0 (0) | 0 (0) | ||
| Never | 20 (87.0) | 21 (84.0) | 24 (100) | ||
| Relaxation practice | 0.329 | ||||
| Yoga | 2 (8.7) | 0 (0) | 0 (0) | ||
| Tai chi or qigong | 0 (0) | 0 (0) | 1 (4.2) | ||
| Stretching exercise | 4 (17.4) | 5 (20.0) | 5 (20.8) | ||
| Spend time in nature | 3 (13.0) | 5 (20.0) | 1 (4.2) | ||
| Slow deep breathing | 3 (13.0) | 7 (28.0) | 4 (5.6) | ||
| Mindfulness meditation | 1 (4.3) | 1 (4.0) | 2 (8.3) | ||
| Listen to music | 6 (26.1) | 5 (20.0) | 3 (12.5) | ||
| Never | 1 (4.3) | 0 (0) | 4 (16.7) | ||
| Others | 3 (13.0) | 2 (8.0) | 4 (16.7) | ||
| History of Hypertension | 0.556 | ||||
| Hypertension with medication | 14 (60.9) | 13 (52.0) | 14 (58.3) | ||
| Hypertension without medication | 0 (0) | 1 (4.0) | 1 (4.2) | ||
| Pre-hypertension | 9 (39.1) | 9 (36.0) | 9 (37.5) | ||
| Unknown Hypertension | 0 (0) | 2 (8.0) | 0 (0) | ||
| No. of antihypertensive drugs taken | 0.661 | ||||
| 0 | 9 (39.1) | 13 (52.0) | 10 (41.7) | ||
| 1 | 8 (34.8) | 9 (36.0) | 8 (33.3) | ||
| 2 | 4 (17.4) | 1 (4.0) | 5 (20.8) | ||
| 3 | 1 (4.3) | 2 (8.0) | 1 (4.2) | ||
| 4 | 1 (4.3) | 0 (0) | 0 (0) | ||
| MIND Group (n = 23) | MIND-FB Group (n = 25) | Control Group (n = 24) | p Value across All Groups | p Value * | |||
|---|---|---|---|---|---|---|---|
| MIND vs. Control | MIND-FB vs. Control | ||||||
| BMI (kg/m2) | 24.9 ± 3.4 | 24.9 ± 3.3 | 25.7 ± 2.9 | 0.612 | 0.667 | 0.666 | |
| Waist to hip ratio | 0.9 ± 0.04 | 0.89 ± 0.05 | 0.93 ± 0.05 | 0.014 | 0.080 | 0.015 | |
| Body fat (%) | 35.1 ± 6.08 | 35.2 ± 6.9 | 37.3 ± 4.9 | 0.347 | 0.401 | 0.435 | |
| Lipid Panel | |||||||
| Total cholesterol (mmol/L) | 5.4 ± 1.3 | 6.0 ± 1.4 | 5.5 ± 1.2 | 0.213 | 0.953 | 0.361 | |
| LDL-cholesterol (mmol/L) | 2.9 ± 1.2 | 3.4 ± 1.3 | 2.8 ± 1.1 | 0.249 | 0.979 | 0.276 | |
| HDL-cholesterol (mmol/L) | 1.7 ± 0.5 | 1.7 ± 0.3 | 1.8 ± 0.3 | 0.682 | 0.998 | 0.710 | |
| Triglyceride (mmol/L) | 1.8 ± 1.1 | 2.1 ± 1.1 | 2.0 ± 1.2 | 0.602 | 0.804 | 0.928 | |
| Glucose (mmol/L) | 5.9 ± 1.3 | 6.2 ± 1.4 | 6.4 ± 1.6 | 0.652 | 0.640 | 0.960 | |
| BP | |||||||
| SBP (mmHg) | 137.8 ± 14.3 | 141 ± 12.0 | 141.8 ± 17.2 | 0.609 | 0.611 | 0.977 | |
| DBP (mmHg) | 85.1 ± 10.5 | 88.5 ± 9.0 | 80.2 ± 9.7 | 0.014 | 0.199 | 0.011 | |
| Mood state | |||||||
| POMS total (score) | 38.3 ± 13 | 41.8 ± 11.4 | 43.0 ± 14.8 | 0.456 | 0.444 | 0.938 | |
| Tension-anxiety | 4.1 ± 2.9 | 6.2 ± 3.9 | 5.5 ± 3.7 | 0.132 | 0.352 | 0.819 | |
| Depression-dejection | 3.2 ± 3.1 | 4.2 ± 3.5 | 4.7 ± 3.5 | 0.315 | 0.301 | 0.900 | |
| Fatigue-inertia | 6.3 ± 3.6 | 6.6 ± 3.7 | 6.8 ± 3.8 | 0.906 | 0.898 | 0.964 | |
| Anger-hostility | 4.0 ± 2.4 | 4.8 ± 2.6 | 4.1 ± 2.9 | 0.491 | 0.994 | 0.590 | |
| Confusion-bewilderment | 11.3 ± 3.0 | 10.6 ± 1.5 | 11.4 ± 3.1 | 0.542 | 0.988 | 0.562 | |
| Vigor-activity | 9.6 ± 2.8 | 9.5 ± 3.4 | 10.3 ± 4.6 | 0.709 | 0.785 | 0.726 | |
| Anxiety level | |||||||
| STAI-S (score) | 40.4 ± 8.4 | 38.8 ± 8.5 | 36.5 ± 7.0 | 0.246 | 0.220 | 0.568 | |
| STAI-T (score) | 39.8 ± 9.0 | 42.9 ± 8.9 | 42.1 ± 9.5 | 0.499 | 0.679 | 0.951 | |
| Variable | Mean Changes from Baseline to 4 Weeks after Intervention (95% CI) | p Value across All Groups | Effect Size | MIND vs. Control | MIND-FB vs. Control | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIND Group (n = 23) | p Value # | MIND-FB Group (n = 25) | p Value # | Control Group (n = 24) | p Value # | Mean (95% CI) between Group Difference | p Value * | Mean (95% CI) between Group Difference | p Value * | |||
| Adiposity | ||||||||||||
| BMI (kg/m2) | −0.04 (−0.05 to 0.13) | 0.347 | −0.18 (0.18 to 4.93) | 0.065 | 0.05 (−0.24 to 0.14) | 0.604 | 0.552 | 0.02 | −0.86 (−3.13 to 1.41) | 0.639 | −0.91 (−3.14 to 1.31) | 0.588 |
| Waist to hip ratio | −0.01 (−0.00 to 0.37) | 0.156 | 0.00 (−0.00 to 0.00) | 0.856 | −0.01 (−0.00 to 0.02) | 0.070 | 0.019 | 0.08 | −0.03 (−0.06 to−0.00) | 0.050 | −0.03 (−0.07 to −0.00) | 0.029 |
| Body fat (%) | −0.07 (−0.53 to 0.69) | 0.795 | −0.69 (−0.11 to 1.50) | 0.091 | −0.48 (−1.39 to 2.35) | 0.599 | 0.394 | 0.02 | −2.03 (−6.52 to 2.33) | 0.498 | −2.20 (−6.58 to 2.09) | 0.433 |
| Blood pressure | ||||||||||||
| SBP (mmHg) | −1.93 (−2.97 to 6.85) | 0.422 | −3.18 (−2.33 to 8.69) | 0.246 | 0.66 (−4.43 to 3.10) | 0.718 | 0.436 | 0.03 | −5.30 (−15.20 to 4.50) | 0.402 | −2.70 (−12.4 to 6.90) | 0.773 |
| DBP (mmHg) | −1.26 (−1.98 to 4.50) | 0.429 | −2.56 (0.18 to 4.93) | 0.036 | −0.27 (−1.89 to 2.44) | 0.798 | 0.018 | 0.08 | 4.40 (−1.61 to 10.50) | 0.192 | 7.1 (1.24 to 13.10) | 0.014 |
| Cardiovascular risk factor | ||||||||||||
| Total cholesterol (mmol/L) | −0.60 (0.36 to 0.84) | 0.000 | −0.85 (0.37 to 1.34) | 0.001 | −0.57 (0.23 to 0.91) | 0.002 | 0.348 | 0.01 | −0.12 (−0.99 to 0.74) | 0.934 | 0.37 (−0.47 to 1.22) | 0.545 |
| LDL-cholesterol (mmol/L) | −0.33 (0.07 to 0.59) | 0.015 | −0.58 (0.17 to 1.00) | 0.008 | −0.28 (0.03 to 0.52) | 0.026 | 0.805 | 0.01 | −0.04 (−0.74 to 0.83) | 0.990 | 0.39 (−0.03 to 1.16) | 0.442 |
| HDL-cholesterol (mmol/L) | −0.23 (0.09 to 0.38) | 0.002 | −0.14 (0.04 to 0.23) | 0.005 | −0.18 (0.08 to 0.29) | 0.001 | 0.409 | 0.00 | −0.34 (−0.33 to 0.26) | 0.959 | −0.07 (−0.36 to 0.21) | 0.789 |
| Triglyceride (mmol/L) | −0.30 (−0.05 to 0.65) | 0.089 | −0.28 (0.02 to 0.53) | 0.036 | −0.26 (−0.07 to 0.60) | 0.116 | 0.519 | 0.02 | −2.36 (−0.99 to 0.51) | 0.735 | 0.11 (−0.62 to 0.85) | 0.923 |
| Glucose (mmol/L) | −0.68 (0.02 to 1.33) | 0.042 | −0.22 (−0.45 to 0.67) | 0.507 | −0.50 (−0.41 to 1.41) | 0.269 | 0.134 | 0.09 | −0.51 (−1.23 to 0.19) | 0.199 | 0.01 (−0.68 to 0.71) | 0.998 |
| Mood states | ||||||||||||
| POMS total | −1.30 (−3.65 to 6.26) | 0.591 | −6.5 (1.03 to 12.08) | 0.022 | 0.12 (−4.45 to 4.20) | 0.953 | 0.164 | 0.09 | −5.41 (−8.03 to 6.47) | 0.188 | −4.63 (−11.8 to 2.54) | 0.276 |
| Tension-anxiety | 0.04 (−1.22 to 1.14) | 0.940 | −2.20 (0.41 to 3.98) | 0.018 | −0.37 (−0.86 to 1.61) | 0.537 | 0.265 | 0.03 | −1.24 (−3.13 to 0.64) | 0.262 | −0.30 (−2.14 to 1.55) | 0.922 |
| Depression-dejection | 0.17 (−1.24 to 0.89) | 0.740 | −1.36 (−0.23 to 2.95) | 0.092 | −0.12 (−1.21 to 1.46) | 0.849 | 0.194 | 0.06 | −1.34 (−3.20 to 0.51) | 0.200 | −1.05 (−2.86 to 0.77) | 0.357 |
| Fatigue-inertia | −0.91 (−0.39 to 2.22) | 0.162 | −1.48 (0.33 to 2.62) | 0.013 | −0.25 (−0.73 to 1.23) | 0.604 | 0.561 | 0.04 | −0.82 (−3.03 to 1.40) | 0.655 | −0.89 (−3.06 to 1.28) | 0.591 |
| Anger-hostility | −0.26 (−0.85 to 1.37) | 0.633 | −1.24 (0.06 to 2.41) | 0.039 | 1.08 (−2.53 to 0.36) | 0.135 | 0.499 | 0.07 | −0.75 (−2.28 to 0.77) | 0.468 | −0.41 (−1.90 to 1.09) | 0.792 |
| Confusion-bewilderment | −0.52 (−0.61 to 1.65) | 0.351 | −1.28 (0.48 to 2.07) | 0.003 | −0.45 (−0.17 to 10.90) | 0.149 | 0.150 | 0.08 | −0.14 (−1.75 to 1.46) | 0.975 | −1.19 (−2.76 to 0.39) | 0.174 |
| Vigor-activity | −0.17 (−1.10 to 1.45) | 0.781 | 0.64 (−1.94 to 0.66) | 0.321 | 0.16 (−1.16 to 0.82) | 0.732 | 0.665 | 0.01 | −0.89 (−3.30 to 1.51) | 0.648 | −0.58 (−2.93 to 1.78) | 0.827 |
| Anxiety level | ||||||||||||
| STAI-S (score) | −1.70 (−0.72 to 4.29) | 0.155 | −5.28 (2.42 to 8.13 | 0.001 | 2.29 (−5.32 to 0.74) | 0.132 | 0.299 | 0.08 | 1.90 (−3.27 to 7.07) | 0.655 | −1.45 (−6.51 to 3.62) | 0.773 |
| STAI-T (score) | −0.78 (−2.73 to 4.31) | 0.132 | −4.28 (0.49 to 8.06) | 0.028 | −0.75 (−1.28 to 2.78) | 0.454 | 0.605 | 0.02 | −2.27 (−7.69 to 3.15) | 0.577 | −0.97 (−6.28 to 4.34) | 0.900 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yau, K.-Y.; Law, P.-S.; Wong, C.-N. Cardiac and Mental Benefits of Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet plus Forest Bathing (FB) versus MIND Diet among Older Chinese Adults: A Randomized Controlled Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 14665. https://doi.org/10.3390/ijerph192214665
Yau K-Y, Law P-S, Wong C-N. Cardiac and Mental Benefits of Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet plus Forest Bathing (FB) versus MIND Diet among Older Chinese Adults: A Randomized Controlled Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(22):14665. https://doi.org/10.3390/ijerph192214665
Chicago/Turabian StyleYau, Ka-Yin, Pui-Sze Law, and Chung-Ngok Wong. 2022. "Cardiac and Mental Benefits of Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diet plus Forest Bathing (FB) versus MIND Diet among Older Chinese Adults: A Randomized Controlled Pilot Study" International Journal of Environmental Research and Public Health 19, no. 22: 14665. https://doi.org/10.3390/ijerph192214665