
Health Literacy and Environmental Risks Focusing Air Pollution: Results from a Cross-Sectional Study in Germany


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measures
2.3. Analytic Procedure
3. Results
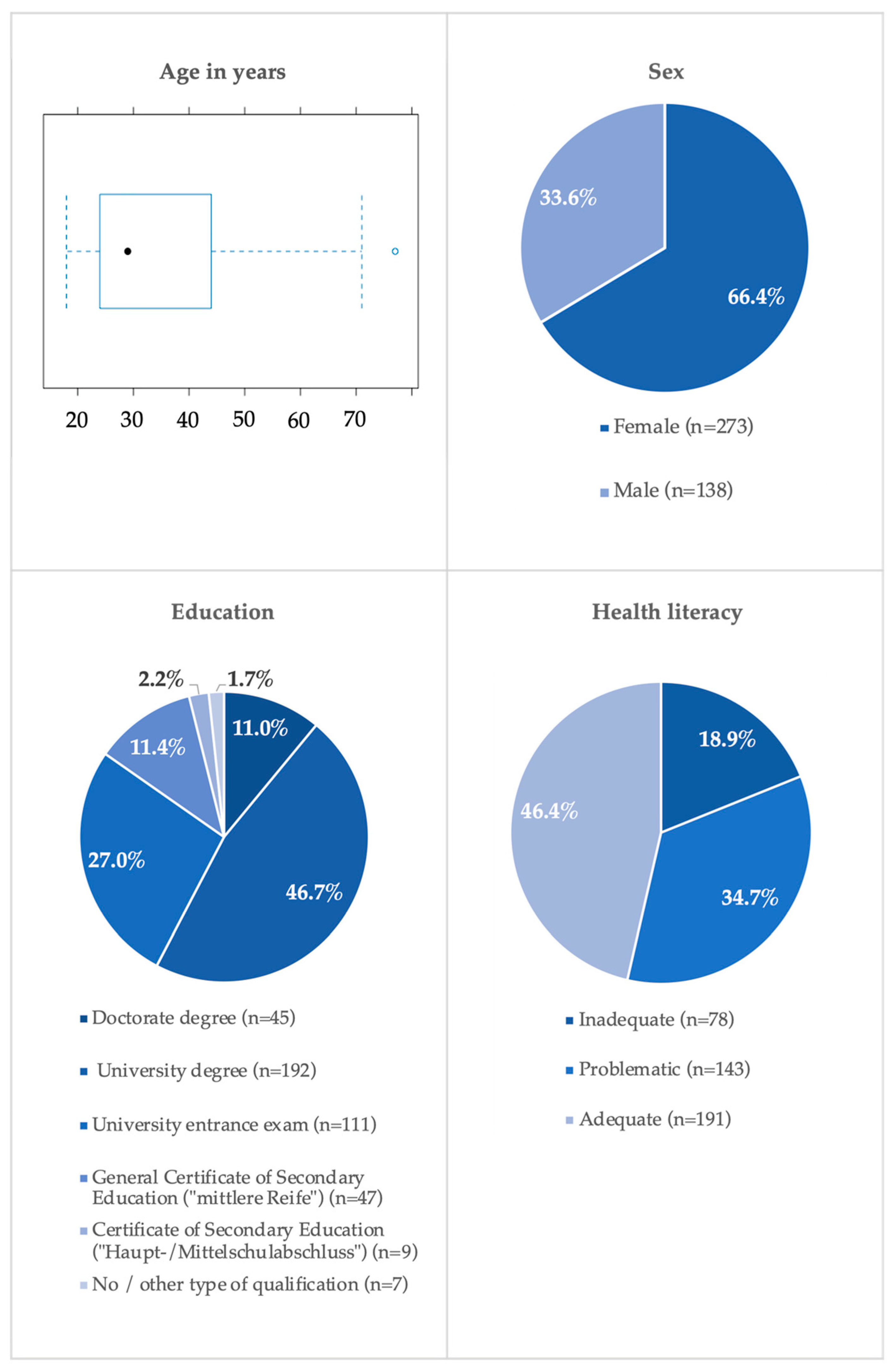
3.1. Sociodemographic Characteristics of the Study Population
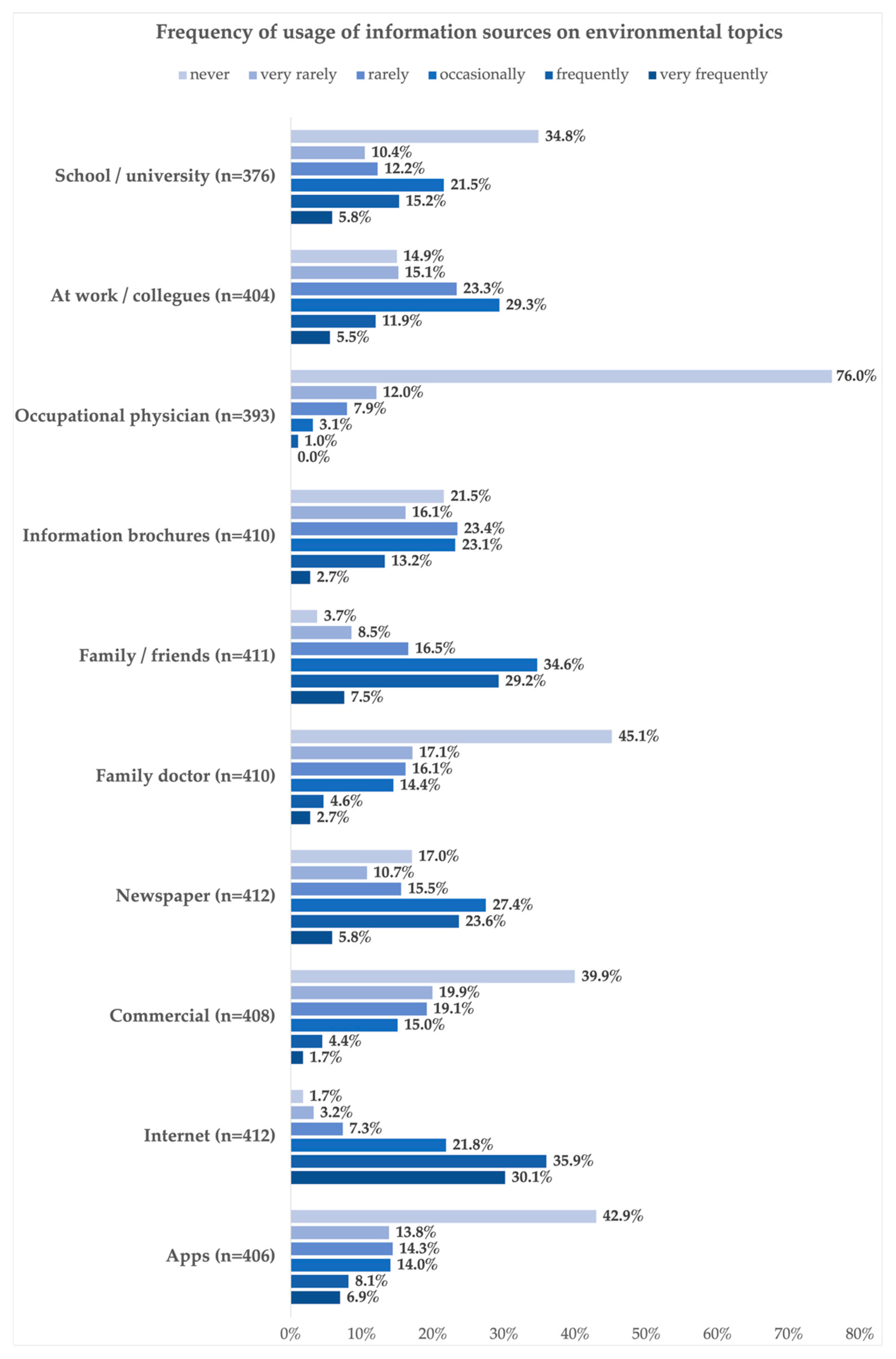
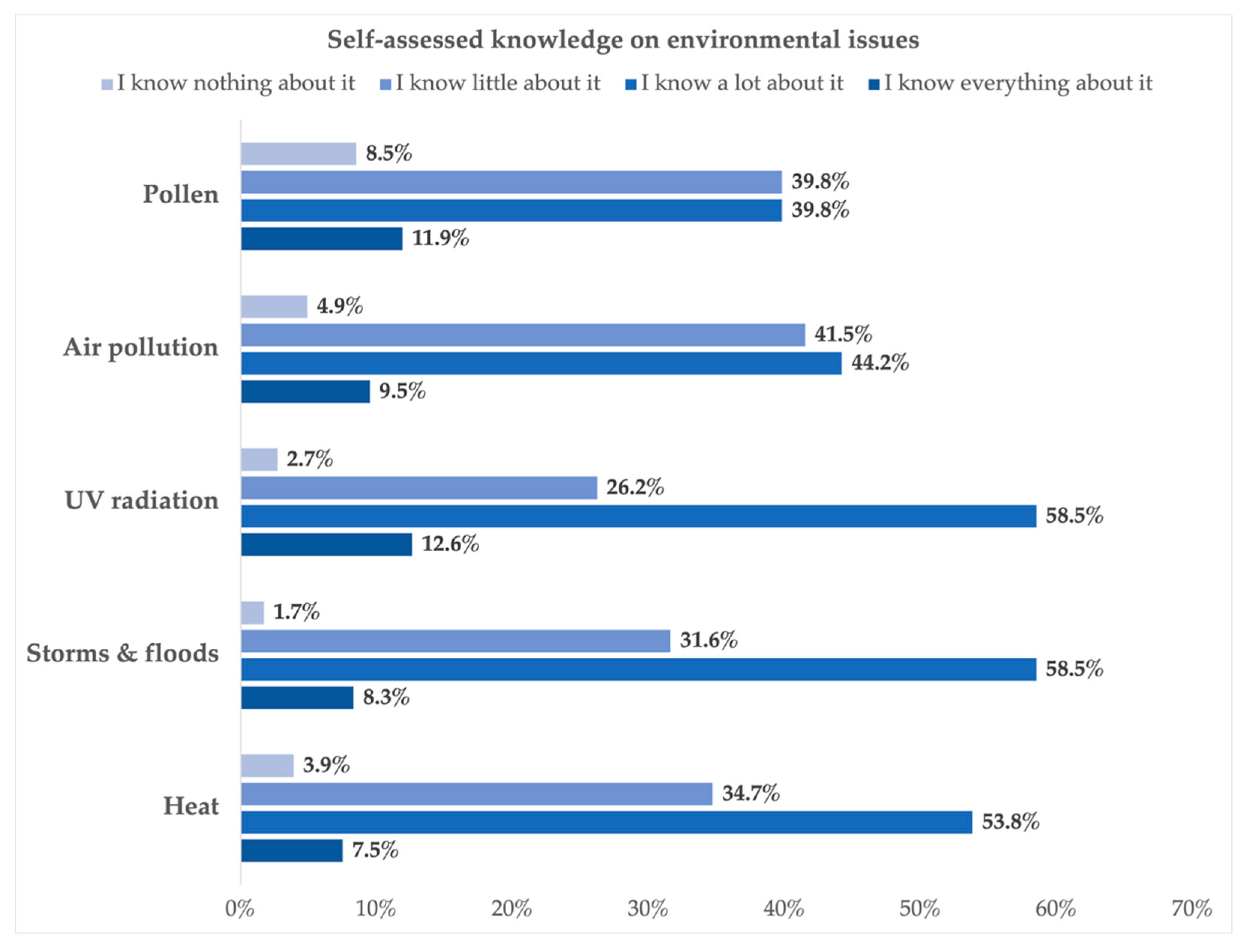
3.2. Information Sources, Knowledge, Attitudes, and Behavior Related to Environmental Issues
3.3. Association between Health Literacy and Environmental Issues
4. Discussion
4.1. Discussion of the Results
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Umweltbundesamt. Umwelt und Gesundheit. Available online: https://www.umweltbundesamt.de/daten/umwelt-gesundheit#strap1 (accessed on 17 October 2023).
- Umweltbundesamt. Umweltschadstoffe und Alterskrankheiten. Available online: https://www.umweltbundesamt.de/umweltschadstoffe-alterskrankheiten (accessed on 17 October 2023).
- Robert Koch-Institut. Umwelt und Gesundheit. Available online: https://www.rki.de/DE/Content/GesundAZ/U/Umwelt_Gesundheit/Umwelt_Gesundheit_inhalt.html (accessed on 17 October 2023).
- World Health Organization. WHO Global Air Quality Guidelines. Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- United States Environmental Protection Agency. Criteria Air Pollutants. Available online: https://www.epa.gov/criteria-air-pollutants (accessed on 17 October 2023).
- World Health Organization. Ambient (Outdoor) Air Pollution. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 17 October 2023).
- Bayerisches Landesamt für Umwelt. Faktenpapier Ultrafeine Partikel; Bayerisches Landesamt für Umwelt: Augsburg, Germany, 2021. [Google Scholar]
- Umweltbundesamt. Warum ist Feinstaub schädlich für den Menschen? Available online: https://www.umweltbundesamt.de/service/uba-fragen/warum-ist-feinstaub-schaedlich-fuer-den-menschen (accessed on 22 February 2024).
- Int Panis, L.; Provost, E.B.; Cox, B.; Louwies, T.; Laeremans, M.; Standaert, A.; Dons, E.; Holmstock, L.; Nawrot, T.; De Boever, P. Short-term air pollution exposure decreases lung function: A repeated measures study in healthy adults. Environ. Health 2017, 16, 60. [Google Scholar] [CrossRef] [PubMed]
- Cosselman, K.E.; Navas-Acien, A.; Kaufman, J.D. Environmental factors in cardiovascular disease. Nat. Rev. Cardiol. 2015, 12, 627–642. [Google Scholar] [CrossRef]
- Münzel, T.; Sørensen, M.; Gori, T.; Schmidt, F.P.; Rao, X.; Brook, J.; Chen, L.C.; Brook, R.D.; Rajagopalan, S. Environmental stressors and cardio-metabolic disease: Part I–epidemiologic evidence supporting a role for noise and air pollution and effects of mitigation strategies. Eur. Heart J. 2017, 38, 550–556. [Google Scholar] [CrossRef]
- Münzel, T.; Sørensen, M.; Gori, T.; Schmidt, F.P.; Rao, X.; Brook, F.R.; Chen, L.C.; Brook, R.D.; Rajagopalan, S. Environmental stressors and cardio-metabolic disease: Part II–mechanistic insights. Eur. Heart J. 2018, 38, 557–564. [Google Scholar] [CrossRef]
- Münzel, T.; Gori, T.; Al-Kindi, S.; Deanfield, J.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur. Heart J. 2018, 39, 3543–3550. [Google Scholar] [CrossRef] [PubMed]
- Mustafić, H.; Jabre, P.; Caussin, C.; Murad, M.H.; Escolano, S.; Tafflet, M.; Périer, M.-C.; Marijon, E.; Vernerey, D.; Empana, J.-P.; et al. Main air pollutants and myocardial infarction: A systematic review and meta-analysis. JAMA 2012, 307, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, S.; Marsland, A.L.; Kinnee, E.J.; Tunno, B.J.; Manuck, S.B.; Gianaros, P.J.; Clougherty, J.E. Long-Term Ambient Air Pollution Exposures and Circulating and Stimulated Inflammatory Mediators in a Cohort of Midlife Adults. Environ. Health Perspect. 2021, 129, 57007. [Google Scholar] [CrossRef]
- Cortese, A.; Lova, L.; Comoli, P.; Volpe, E.; Villa, S.; Mallucci, G.; La Salvia, S.; Romani, A.; Franciotta, D.; Bollati, V.; et al. Air pollution as a contributor to the inflammatory activity of multiple sclerosis. Neuroinflammation 2020, 17, 334. [Google Scholar] [CrossRef]
- DeFranco, E.; Moravec, W.; Xu, F.; Hall, E.; Hossain, M.; Haynes, E.N.; Muglia, L.; Chen, A. Exposure to airborne particulate matter during pregnancy is associated with preterm birth: A population-based cohort study. Environ. Health 2016, 15, 6. [Google Scholar] [CrossRef]
- van Rossem, L.; Rifas-Shiman, S.L.; Melly, S.J.; Kloog, I.; Luttmann-Gibson, H.; Zanobetti, A.; Coull, B.A.; Schwartz, J.D.; Mittleman, M.A.; Oken, E.; et al. Prenatal air pollution exposure and newborn blood pressure. Environ. Health. Perspect. 2015, 123, 353–359. [Google Scholar] [CrossRef]
- Ni, Y.; Szpiro, A.A.; Young, M.T.; Loftus, C.T.; Bush, N.R.; LeWinn, K.Z.; Sathyanarayana, S.; Enquobahrie, D.A.; Davis, R.L.; Kratz, M.; et al. Associations of Pre- and Postnatal Air Pollution Exposures with Child Blood Pressure and Modification by Maternal Nutrition: A Prospective Study in the CANDLE Cohort. Environ. Health Perspect. 2021, 129, 47004. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Kwong, J.C.; Copes, R.; Hystad, P.; van Donkelaar, A.; Tu, K.; Brook, J.R.; Goldberg, M.S.; Martin, R.V.; Murray, B.J.; et al. Exposure to ambient air pollution and the incidence of dementia: A population-based cohort study. Environ. Int. 2017, 108, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-Y.; Li, C.-H.; Martini, S.; Hou, W.-H. Association between air pollution and risk of vascular dementia: A multipollutant analysis in Taiwan. Environ. Int. 2019, 133, 105233. [Google Scholar] [CrossRef]
- Grande, G.; Ljungman, P.L.S.; Eneroth, K.; Bellander, T.; Rizzuto, D. Association Between Cardiovascular Disease and Long-term Exposure to Air Pollution With the Risk of Dementia. JAMA Neurol. 2020, 77, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Steenland, K.; Li, H.; Liu, P.; Zhang, Y.; Lyles, R.H.; Requia, W.J.; Ilango, S.D.; Chang, H.H.; Wingo, T.; et al. A national cohort study (2000-2018) of long-term air pollution exposure and incident dementia in older adults in the United States. Nat. Commun. 2021, 12, 6754. [Google Scholar] [CrossRef] [PubMed]
- Institut und Poliklinik für Arbeits- Sozial- und Umweltmedizin der Friedrich-Alexander-Universität Erlangen-Nürnberg. Bayerischer Projektverbund ultrafeine Partikel. Available online: https://www.ultrafeinepartikel.de (accessed on 20 October 2023).
- World Health Organization. What Are the WHO Air Quality Guidlines? Available online: https://www.who.int/news-room/feature-stories/detail/what-are-the-who-air-quality-guidelines (accessed on 19 October 2023).
- World Health Organization. New WHO Global Air Quality Guidelines Aim to Save Millions of Lives from Air Pollution. Available online: https://www.who.int/news/item/22-09-2021-new-who-global-air-quality-guidelines-aim-to-save-millions-of-lives-from-air-pollution (accessed on 5 October 2021).
- European Commission. Directive 2008/50/EC of the European Parliament and the Council of 21 May 2008 on ambient air quality and cleaner air for Europe. Off. J. Eur. Union 2008, L152, 1–44. [Google Scholar]
- Plaia, A.; Ruggieri, M. Air quality indices: A review. Rev. Environ. Sci. Biotechnol. 2010, 10, 165–179. [Google Scholar] [CrossRef]
- Tan, X.; Han, L.; Zhang, X.; Zhou, W.; Li, W.; Qian, Y. A review of current air quality indexes and improvements under the multi-contaminant air pollution exposure. J. Environ. Manag. 2021, 279, 111681. [Google Scholar] [CrossRef]
- Lelieveld, J.; Klingmuller, K.; Pozzer, A.; Poschl, U.; Fnais, M.; Daiber, A.; Munzel, T. Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur. Heart J. 2019, 40, 1590–1596. [Google Scholar] [CrossRef]
- World Health Organization. Air Pollution. Available online: https://www.who.int/health-topics/air-pollution#tab=tab_1 (accessed on 19 October 2023).
- Nutbeam, D. Health promotion glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Sorensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; Consortium Health Literacy Project; European (HLS-EU). Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institut. Gesundheitskompetenz/Health Literacy. Available online: https://www.rki.de/DE/Content/GesundAZ/G/Gesundheitskompetenz/Gesundheitskompetenz_node.html (accessed on 12 December 2023).
- Orkan, O.; Bauer, U.; Levin-Zamir, D.; Pinheiro, P.; Sørensen, K. International Handbook of Health Literacy: Research, Practice and Policy across the Lifespan; Policy Press: Bristol, UK, 2019. [Google Scholar]
- Rowlands, G.; Trezona, A.; Russell, S.; Lopatina, M.; Pelikan, J.; Paasche-Orlow, M.; Drapkina, O.; Kontsevaya, A.; Sørensen, K. Zusammenfassender. Bericht. 65 des. Health. Evidence. Network; WHO-Regionalbüro für Europa: Kopenhagen, Denmark, 2019. [Google Scholar]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Abel, T.; McQueen, D. Critical health literacy and the COVID-19 crisis. Health Promot. Int. 2020, 35, 1612–1613. [Google Scholar] [CrossRef] [PubMed]
- Uwamahoro, N.S.; Ngwira, B.; Vinther-Jensen, K.; Rowlands, G. Health literacy among Malawian HIV-positive youth: A qualitative needs assessment and conceptualization. Health Promot. Int. 2020, 35, 1137–1149. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Dunzhu, C.; Widdowson, M.A.; Wu, S.; Ciren, P.; Duoji, D.; Pingcuo, W.; Dun, B.; Ma, C.; Li, J.; et al. Infectious disease-specific health literacy in Tibet, China. Health Promot. Int. 2018, 33, 84–91. [Google Scholar] [CrossRef]
- Pfleger, E.; Lutz, R.; Drexler, H. [Environmental risks and health literacy: A systematic review]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2024, 67, 85–98. [Google Scholar] [CrossRef]
- Hou, W.H.; Huang, Y.C.; Lu, C.Y.; Chen, I.C.; Lee, P.C.; Lin, M.Y.; Wang, Y.C.; Sulistyorini, L.; Li, C.Y. A national survey of ambient air pollution health literacy among adult residents of Taiwan. BMC Public Health 2021, 21, 1604. [Google Scholar] [CrossRef]
- Döring, N. Forschungsmethoden und Evaluation in den Sozial- und Humanwissenschaften, 6th ed.; Springer: Berlin/Heidelberg, Germany, 2023. [Google Scholar]
- Röthlin, F.; Pelikan, J.; Ganahl, K. Die Gesundheitskompetenz der 15-jährigen Jugendlichen in Österreich. Abschlussbericht der österreichischen Gesundheitskompetenz Jugendstudie im Auftrag des Hauptverbands der österreichischen Sozialversicherungsträger (HVSV); Ludwig Boltzmann Gesellschaft GmbH: Wien, Austria, 2013. [Google Scholar]
- Capellaro, M.; Sturm, D. Evaluation von Informationssystemen zu Klimawandel und Gesundheit, Band 1; Umweltbundesamt: Dessau-Roßlau, Germany, 2015. [Google Scholar]
- Zok, K.; Kolpatzik, K. Gesundheitliche Belastungen durch Umwelteinflüsse; Wissenschaftliches Institut der AOK (WIdO), AOK-Bundesverband: Berlin, Germany, 2021; Volume 1. [Google Scholar]
- Schmuker, C.; Robra, B.-P.; Kolpatzik, K.; Zok, K.; Klauber, J. Klimawandel und Gesundheit: Welche Rolle Spielt der Klimawandel im Gesundheitsbewusstsein der Befragten? Ergebnisse Einer Deutschlandweiten Bevölkerungsbefragung; MWV Medizinisch Wissenschaftliche Verlagsgesellschaft: Berlin, Germany, 2021; pp. 157–176. [Google Scholar]
- Hayes, A.F. The PROCESS macro for SPSS, SAS, and R. Available online: https://processmacro.org/index.html# (accessed on 30 November 2023).
- Gray, K.M.; Triana, V.; Lindsey, M.; Richmond, B.; Hoover, A.G.; Wiesen, C. Knowledge and Beliefs Associated with Environmental Health Literacy: A Case Study Focused on Toxic Metals Contamination of Well Water. Int. J. Environ. Res. Public Health 2021, 18, 9298. [Google Scholar] [CrossRef]
- Zhao, Y.; Sheng, Y.; Zhou, J.; Wang, H.; Chilufya, M.M.; Liu, X.; Mohamed, A.O.; Han, J.; Qu, C. Influencing factors of residents’ environmental health literacy in Shaanxi province, China: A cross-sectional study. BMC Public Health 2022, 22, 114. [Google Scholar] [CrossRef]
- Hashemi, M.; Khanjani, N.; Saber, M.; Fard, N.K. Evaluating health literacy of Kerman Medical University, School of Public Health students about recycling solid waste. J. Educ. Health Promot. 2012, 1, 23. [Google Scholar] [CrossRef]
- Carducci, A.; Fiore, M.; Azara, A.; Bonaccorsi, G.; Bortoletto, M.; Caggiano, G.; Calamusa, A.; De Donno, A.; De Giglio, O.; Dettori, M.; et al. Environment and health: Risk perception and its determinants among Italian university students. Sci. Total. Environ. 2019, 691, 1162–1172. [Google Scholar] [CrossRef] [PubMed]
- Carducci, A.; Fiore, M.; Azara, A.; Bonaccorsi, G.; Bortoletto, M.; Caggiano, G.; Calamusa, A.; De Donno, A.; De Giglio, O.; Dettori, M.; et al. Pro-Environmental Behaviors: Determinants and Obstacles among Italian University Students. Int. J. Environ. Res. Public Health 2021, 18, 3306. [Google Scholar] [CrossRef]
- Eggers, M.J.; Doyle, J.T.; Lefthand, M.J.; Young, S.L.; Moore-Nall, A.L.; Kindness, L.; Medicine, R.O.; Ford, T.E.; Dietrich, E.; Parker, A.E.; et al. Community Engaged Cumulative Risk Assessment of Exposure to Inorganic Well Water Contaminants, Crow Reservation, Montana. Int. J. Environ. Res. Public Health 2018, 15, 76. [Google Scholar] [CrossRef] [PubMed]
- Baird, B.N. Tolerance for environmental health risks: The influence of knowledge, benefits, voluntariness, and environmental attitudes. Risk Anal. 1986, 6, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Hornberg, C.; Malsch, A.K.; Weissbach, W.; Wiesmüller, G.A. [Environment-related health disorders. Experience and perspectives in the care of patients with environment-related health disorders]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2004, 47, 780–794. [Google Scholar] [CrossRef] [PubMed]
- Proskurnova, E.L. The reasons for the decline in popularity and prospects for the development of linear television. RUDN J. Stud. Lit. Journal. 2020, 25, 146–154. [Google Scholar] [CrossRef]
- Behrens, B.; Bałazińska, E. Adblocker-Tracking: Wie stark sie Ihre Web Analytics Daten beeinflussen. Available online: https://piwikpro.de/blog/wie-stark-adblocker-tracking-und-web-analytics-beeinflussen/ (accessed on 8 November 2023).
- Statista. Anzahl der Smartphone-Nutzer* in Deutschland in den Jahren 2009 bis 2022 und Prognose bis 2027. Available online: https://de.statista.com/statistik/daten/studie/198959/umfrage/anzahl-der-smartphonenutzer-in-deutschland-seit-2010/ (accessed on 8 November 2023).
- Umweltbundesamt. App Luftqualität. Available online: https://www.umweltbundesamt.de/themen/luft/luftqualitaet/app-luftqualitaet (accessed on 8 November 2023).
- Johnston, F.H.; Wheeler, A.J.; Williamson, G.J.; Campbell, S.L.; Jones, P.J.; Koolhof, I.S.; Lucani, C.; Cooling, N.B.; Bowman, D.M.J.S. Using smartphone technology to reduce health impacts from atmospheric environmental hazards. Environ. Res. Lett. 2018, 13, 044019. [Google Scholar] [CrossRef]
- Helmholtz Munich. Wie verbreitet ist Heuschnupfen? Available online: https://www.allergieinformationsdienst.de/krankheitsbilder/heuschnupfen/verbreitung.html#:~:text=Bei%2015%20Prozent%20der%20Erwachsenen,ein%20ähnlicher%20Trend%20zu%20beobachten (accessed on 8 November 2023).
- Umweltbundesamt. 25 Jahre Umweltbewusstseins forschung im Umweltressort: Langfristige Entwicklungen und aktuelle Ergebnisse; Umweltbundesamt: Dessau-Roßlau, Germany, 2021. [Google Scholar]
- Mucke, H.G.; Litvinovitch, J.M. Heat Extremes, Public Health Impacts, and Adaptation Policy in Germany. Int. J. Environ. Res. Public Health 2020, 17, 7862. [Google Scholar] [CrossRef]
- Matandirotya, N. The 2021 Western Germany flood event: The value of flood risk dissemination strategies and social media. JÀMBÁ 2022, 14, 1322. [Google Scholar] [CrossRef]
- Schmitz, S.; Weiand, L.; Becker, S.; Niehoff, N.; Schwartzbach, F.; von Schneidemesser, E. An assessment of perceptions of air quality surrounding the implementation of a traffic-reduction measure in a local urban environment. SCS 2018, 41, 525–537. [Google Scholar] [CrossRef]
- IQAir. Luftqualität in Deutschland: Luftqualitätsindex (AQI) und PM2,5-Luftverschmutzung in Deutschland. Available online: https://www.iqair.com/de/germany (accessed on 9 November 2023).
- European Environment Agency. Luftverschmutzung. Available online: https://www.eea.europa.eu/de/themes/air/intro (accessed on 9 November 2023).
- Hadler, M.; Kraemer, K. Die Wahrnehmung von Umweltgefährdungen: Österreich im internationalen Vergleich. SWS-Rundschau 2014, 54, 413–431. [Google Scholar]
- Özkan, S.; Tüzün, H.; Dikmen, A.U.; Aksakal, N.B.; Çaliskan, D.; Taşçi, Ö.; Günesş, S.C. The Relationship Between Health Literacy Level and Media Used as a Source of Health-Related Information. Health Lit. Res. Pract. 2021, 5, e109–e117. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Hay, J.L.; Waters, E.A.; Kiviniemi, M.T.; Biddle, C.; Schofield, E.; Li, Y.; Kaphingst, K.; Orom, H. Health Literacy and Use and Trust in Health Information. J. Health Commun. 2018, 23, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.; Mieth, L.; Buchner, A. Source memory for advertisements: The role of advertising message credibility. Mem. Cognit. 2021, 49, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.M.; Xu, R.X.; Hu, Y.S.; Ren, L.K.; Qiao, H.; Ding, H.; Liu, Z.L. Chinese Internet Searches Provide Inaccurate and Misleading Information to Epilepsy Patients. Chin. Med. J. 2015, 128, 3324–3328. [Google Scholar] [CrossRef] [PubMed]
- Richter-Kuhlmann, E. Impfungen: Bundeszentrale startet Kampagne. Dtsch. Arztebl. 2012, 109, A-2012. [Google Scholar]
- Villagran, M.; Weathers, M.; Keefe, B.; Sparks, L. Medical Providers as Global Warming and Climate Change Health Educators: A Health Literacy Approach. Commun. Educ. 2010, 59, 312–327. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Breitner-Busch, S.; Mücke, H.; Schneider, A.; Hertig, E. Auswirkungen des Klimawandels auf nicht-übertragbare Erkrankungen durch erhöhte Luftschadstoffbelastungen der Außenluft. J. Health Monit. 2023, 8, 111–131. [Google Scholar] [CrossRef]
- Pharmazeutische Zeitung. Bessere Gesundheits-Kompetenz könnte Milliarden sparen. Available online: https://www.pharmazeutische-zeitung.de/bessere-gesundheits-kompetenz-koennte-milliarden-sparen-143617/ (accessed on 20 February 2024).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | HL | |
|---|---|---|
| HL | 1 | |
| Self-assessed knowledge on: | heat | 0.18 *** |
| storms and floods | 0.22 *** | |
| UV radiation | 0.23 *** | |
| air pollution | 0.19 *** | |
| pollen | 0.19 *** | |
| Model 1 | Model 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Est. | SE | t-Value | p-Value | β | Est. | SE | t-Value | p-Value | β | |
| Intercept | 9.73 | 0.95 | 10.187 | <0.001 | - | 8.79 | 1.12 | 7.85 | <0.001 | - |
| School/university | 0.01 | 0.11 | 0.08 | 0.94 | 0.00 | 0.09 | 0.12 | 0.76 | 0.45 | - |
| At work/collegues | 0.21 | 0.14 | 1.45 | 0.14 | 0.08 | 0.18 | 0.14 | 1.26 | 0.21 | - |
| Occupational physician | −0.41 | 0.27 | −1.55 | 0.12 | −0.10 | −0.39 | 0.27 | −1.44 | 0.15 | - |
| Information brochures | 0.09 | 0.16 | 0.58 | 0.56 | 0.04 | 0.07 | 0.16 | 0.46 | 0.64 | - |
| Family/friends | −0.07 | 0.17 | −0.41 | 0.68 | −0.02 | −0.04 | 0.17 | −0.21 | 0.83 | - |
| Family doctor | 0.15 | 0.15 | 1.00 | 0.32 | 0.06 | 0.09 | 0.16 | 0.59 | 0.56 | - |
| Newspaper | 0.35 | 0.15 | 2.37 | 0.02 * | 0.15 | 0.29 | 0.15 | 1.89 | 0.06 | - |
| Commercial | −0.32 | 0.15 | −2.15 | 0.03 * | −0.12 | −0.27 | 0.16 | −1.71 | 0.09 | - |
| Internet | 0.19 | 0.19 | 1.06 | 0.29 | 0.07 | 0.20 | 0.19 | 1.10 | 0.27 | - |
| Apps | 0.02 | 0.12 | 0.19 | 0.85 | 0.01 | 0.03 | 0.12 | 0.26 | 0.79 | - |
| Age | 0.02 | 0.02 | 1.41 | 0.16 | - | |||||
| Pathway | Effect | Coef. | 95% CI | |
|---|---|---|---|---|
| a1 | Age → Newspaper | direct | 0.2683 *** | 0.0199; 0.0415 |
| a2 | Age → Commercial | direct | −0.1740 *** | −0.0272; −0.0077 |
| b1 | Newspaper → HL | direct | 0.1846 *** | 0.1807; 0.6587 |
| b2 | Commercial → HL | direct | −0.1340 * | −0.6128; −0.0807 |
| a1b1 | Age → Newspaper → HL | indirect | 0.0496 | 0.0198; 0.0845 |
| a2b2 | Age → Commercial → HL | indirect | 0.0233 | 0.0043; 0.0482 |
| c’ | Age → HL | direct | 0.0173 | −0.0095; 0.0441 |
| c | Age →→ HL | IE overall | 0.0728 ** | 0.0331; 0.1162 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pfleger, E.; Drexler, H.; Lutz, R. Health Literacy and Environmental Risks Focusing Air Pollution: Results from a Cross-Sectional Study in Germany. Int. J. Environ. Res. Public Health 2024, 21, 366. https://doi.org/10.3390/ijerph21030366
Pfleger E, Drexler H, Lutz R. Health Literacy and Environmental Risks Focusing Air Pollution: Results from a Cross-Sectional Study in Germany. International Journal of Environmental Research and Public Health. 2024; 21(3):366. https://doi.org/10.3390/ijerph21030366
Chicago/Turabian StylePfleger, Elisabeth, Hans Drexler, and Regina Lutz. 2024. "Health Literacy and Environmental Risks Focusing Air Pollution: Results from a Cross-Sectional Study in Germany" International Journal of Environmental Research and Public Health 21, no. 3: 366. https://doi.org/10.3390/ijerph21030366
APA StylePfleger, E., Drexler, H., & Lutz, R. (2024). Health Literacy and Environmental Risks Focusing Air Pollution: Results from a Cross-Sectional Study in Germany. International Journal of Environmental Research and Public Health, 21(3), 366. https://doi.org/10.3390/ijerph21030366