The Potential Impact on Farmer Health of Enhanced Export Horticultural Trade between the U.K. and Uganda

Abstract
:1. Introduction
2. Methods
2.1. Measuring Health
2.2. Questionnaire Translation
2.2.1. UK
2.2.2. Uganda
2.3. Sample Recruitment
2.3.1. UK
2.3.2. Uganda
2.4. Data Analysis
3. Results
3.1. Sample Description
3.1.1. UK
3.1.2. Uganda
3.2. Health Scale Correlations
3.3. Comparison of UK Scores with US Norms
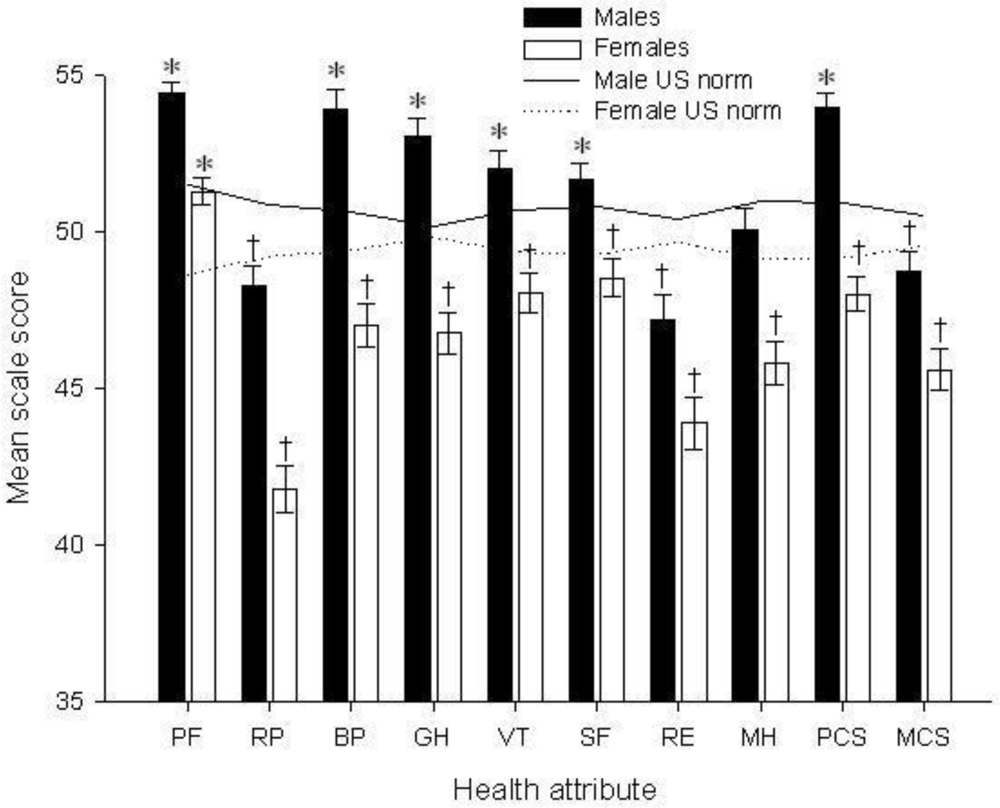
3.4. Comparison of Ugandan Scores with U.S. Norms
3.5. Comparisons of Scores between the U.K. and Uganda for the 18–34 Age Group
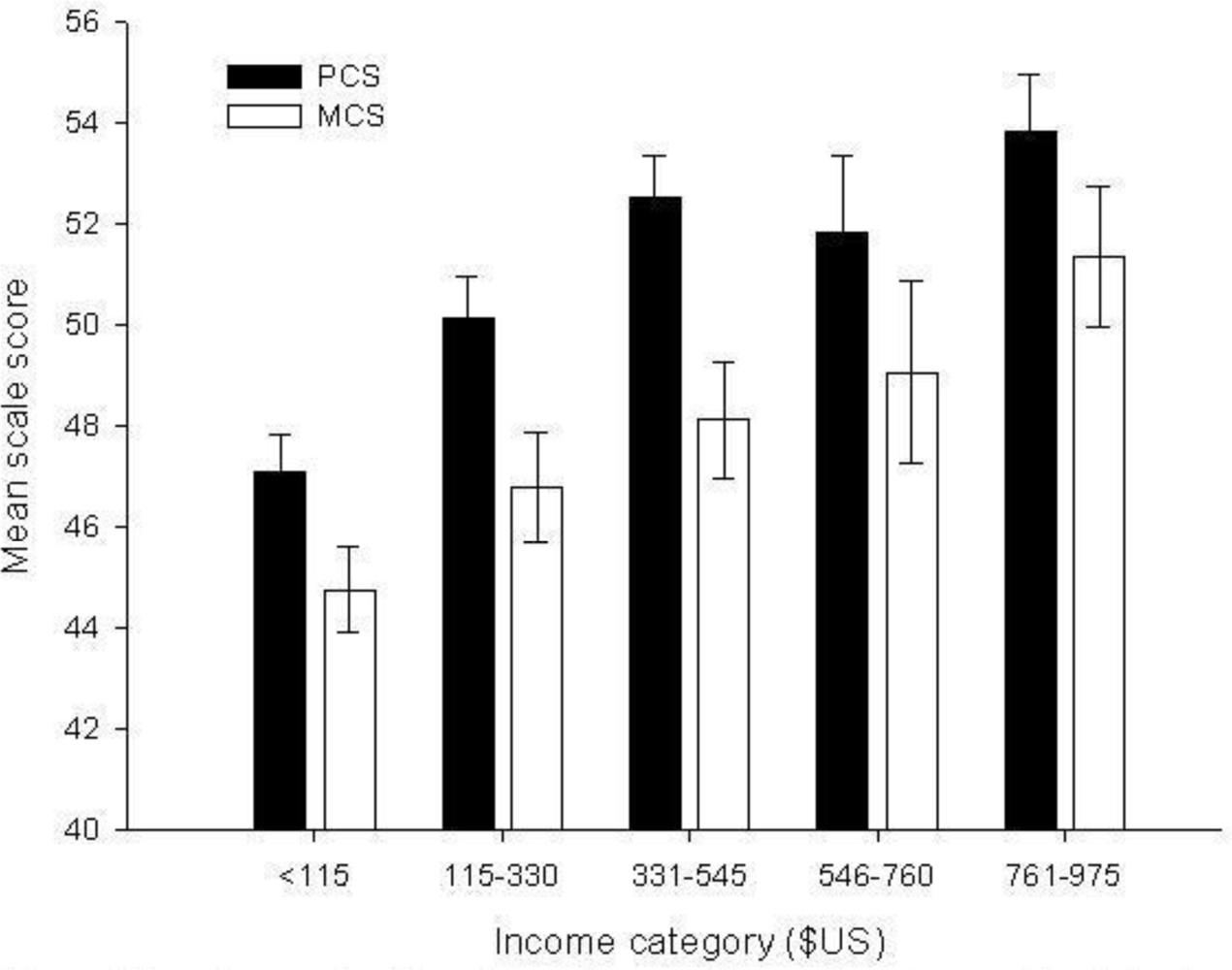
3.6. Contribution of Socio-Demographic Variables to Health Scores
3.7. Longitudinal Assessment of Migrant Workers in the U.K. during 2007
4. Discussion
4.1. Wider Implications
4.2. Agriculture and Tropical diseases: The Case for Malaria
4.3. Ethical Considerations
Acknowledgments
References
- IFOAM. The principles of organic agriculture.
- Rice, RA. Noble goals and challenging terrain: organic and fair trade coffee movements in the global marketplace. J. Agric. Environ. Ethics 2001, 14, 39–66. [Google Scholar]
- Cross, P; Edwards, RT; Hounsome, B; Edwards-Jones, G. Comparative assessment of migrant farm worker health in conventional and organic horticultural systems in the United Kingdom. Sci. Total Environ 2008, 391, 55–65. [Google Scholar]
- Mayer, D. The long-term impact of health on economic growth in Latin America. World Dev 2001, 29, 1025–1033. [Google Scholar]
- Hawkes, C; Ruel, M. The links between agriculture and health: an intersectoral opportunity to improve the health and livelihoods of the poor. Bull. World Health Org 2006, 84, 984–987. [Google Scholar]
- Gabre-Madhin, EZ; Haggblade, S. Successes in African agriculture: Results of an expert survey. World Dev 2004, 32, 745–766. [Google Scholar]
- Jaffee, S. From challenge to opportunity: Transforming Kenya’s fresh vegetable trade in the context of emerging food safety and other standards in Europe; World Bank: Washington, D.C., USA, January 2003. [Google Scholar]
- Minot, N; Ngigi, M. Are horticultural exports a replicable success story? Evidence from Kenya and Côte d’Ivoire; International Food Policy Research Institute: Washington, D.C., USA, 2004. [Google Scholar]
- Lynch, JW; Smith, GD; Kaplan, GA; House, JS. Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ 2000, 320, 1200–1204. [Google Scholar]
- Gough, I; Thomas, T. Why do levels of human-welfare vary among nations? Int. J. Health Serv 1994, 24, 715–748. [Google Scholar]
- Diener, E; Diener, M; Diener, C. Factors predicting the subjective well-being of nations. J. Pers. Soc. Psychol 1995, 69, 851–864. [Google Scholar]
- Mackenbach, JP; Martikainen, P; Looman, CWN; Dalstra, JAA; Kunst, AE; Lahelma, E; Members of the SEdHA working group. The shape of the relationship between income and self-assessed health: An international study. Int. J. Epidemiol 2005, 34, 286–293. [Google Scholar]
- Stronks, K; van de Mheen, H; van den Bos, J; Mackenbach, JP. The interrelationship between income, health and employment status. Int. J. Epidemiol 1997, 26, 592–600. [Google Scholar]
- Van Doorslaer, E; Wagstaff, A; Bleichrodt, H; Calonge, S; Gerdtham, UG; Gerfin, M; Geurts, J; Gross, L; Hakkinen, U; Leu, RE; Odonnell, O; Propper, C; Puffer, F; Rodriguez, M; Sundberg, G; Winkelhake, O. Income-related inequalities in health: Some international comparisons. J. Health Econ 1997, 16, 93–112. [Google Scholar]
- Whitaker, M; Kolavalli, S. Floriculture in Kenya; World Bank report WB0121World Bank: Washington, D.C., USA, 2004. [Google Scholar]
- McCulloch, N; Ota, M. Export horticulture and poverty in Kenya; IDS Working Paper No. 174 174; Institute for Development Studies: Brighton, UK, 2002. [Google Scholar]
- Achterbosch, T; Allbritton, A; Quang, DV; de Jager, A; Njue, E; Sonko, R; Stallen, M; Wertheim-Heck, S; van Wijk, S. Pro-poor horticulture in East Africa & South East Asia; DFID: University of Wageningen: Wageningen, The Netherlands, September 2005; pp. 1–105. [Google Scholar]
- Sonko, R; Njue, E; Ssebuliba, JM; de Jager, A. Pro-poor horticulture In East Africa and South East Asia: The horticultural sector in Uganda; Agricultural Economics Research Institute: Wageningen University and Research Centre: Hague, The Netherlands, 2005. [Google Scholar]
- Kappel, R; Lay, J; Steiner, S. Uganda: No more pro-poor growth? Dev. Policy Rev 2005, 23, 27–53. [Google Scholar]
- Gallup, JL; Sachs, JD. The economic burden of malaria. Am. J. Trop. Med. Hyg 2001, 64, 85–96. [Google Scholar]
- Laxminarayan, R. Does reducing malaria improve household living standards? Trop. Med. Int Health 2004, 9, 267–272. [Google Scholar]
- EIRO. Minimum wages in Europe; Dublin, August 2005.
- HSE. Health and safety in agriculture; HSE: London, UK.
- Villarejo, D. The health of US hired farm workers. Annu. Rev. Public Health 2003, 24, 175–193. [Google Scholar]
- Ware, J; Kosinski, M. SF-36 Physical and Mental Health Summary Scales: A Manual for Users of Version 1, 2nd Ed ed; QualityMetric Incorporated: Lincoln, RI, USA, 2001. [Google Scholar]
- Yost, KJ; Haan, MN; Levine, RA; Gold, EB. Comparing SF-36 scores across three groups of women with different health profiles. Qual. Life Res 2005, 14, 1251–1261. [Google Scholar]
- Kind, P; Dolan, P; Gudex, C; Williams, A. Variations in population health status: results from a United Kingdom national questionnaire survey. BMJ 1998, 316, 736–741. [Google Scholar]
- Ware, J; Snow, K; Kosinski, M. SF-36 Health Survey: Manual and Interpretation Guide; Quality-Metric Incorporated: Lincoln, RI, USA, 1993. [Google Scholar]
- Ware, JE; Gandek, B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J. Clin. Epidemiol 1998, 51, 903–912. [Google Scholar]
- Ware, JE; Gandek, B. Evaluating the readiness of health outcomes measures for use in multinational health technology assessment. Annu. Meet. Int. Soc. Technol. Assess Health Care Int. Soc. Technol. Assess Health Care Meet 1997, 13, 144. [Google Scholar]
- EuroQoL Group. EuroQoL: A new facility for the measurement of heath-related quality of life. Health Pol 1990, 16, 199–208. [Google Scholar]
- Williams, A. The role of the EuroQol instrument in QALY calculations, discussion paper 130; York Centre for Health Economics, University of York: York, UK, 1995. [Google Scholar]
- Sapin, C; Fantino, B; Nowicki, M-L; Kind, P. Usefulness of EQ-5D in assessing health status in primary care patients with major depressive disorder. Health Qual. Life Outcomes 2004, 2, 20. [Google Scholar]
- Joseph, S; Linley, PA; Harwood, J; Lewis, CA; McCollam, P. Rapid assessment of well-being: The Short Depression-Happiness Scale (SDHS). Psychol. Psychother.: Theory Res. Pract 2004, 77, 463–478. [Google Scholar]
- Mela, CF; Kopalle, PK. The impact of collinearity on regression analysis: the asymmetric effect of negative and positive correlations. Appl. Econ 2002, 34, 667–677. [Google Scholar]
- Wyss, K; Wagner, AK; Whiting, D; Mtasiwa, DM; Tanner, M; Gandek, B; Kilima, PM. Validation of the Kiswahili version of the SF-36 Health Survey in a representative sample of an urban population in Tanzania. Qual. Life Res 1999, 8, 111–120. [Google Scholar]
- Wagner, AK; Wyss, K; Gandek, B; Kilima, PM; Lorenz, S; Whiting, D. A Kiswahili version of the SF-36 Health Survey for use in Tanzania: translation and tests of scaling assumptions. Qual. Life Res 1999, 8, 101–110. [Google Scholar]
- Perkins, JJ; Sanson-Fisher, RW. An examination of self- and telephone-administered modes of administration for the Australian SF-36. J. Clin. Epidemiol 1998, 51, 969–973. [Google Scholar]
- Sanson-Fisher, RW; Perkins, JJ. Adaptation and Validation of the SF-36 Health Survey for Use in Australia. J. Clin. Epidemiol 1998, 51, 961–967. [Google Scholar]
- Bowling, A. Just one question: If one question works, why ask several? J. Epidemiol. Commun. Health 2005, 59, 342–345. [Google Scholar]
- Singh-Manoux, A; Gueguen, A; Martikainen, P; Ferrie, J; Marmot, M; Shipley, M. Self-rated health and mortality: short- and long-term associations in the Whitehall II Study. Psychosom. Med 2007, 69, 138–143. [Google Scholar]
- Wannamethee, G; Shaper, AG. Self-assessment of health status and mortality in middle-aged British men. Int. J. Epidemiol 1991, 20, 239–245. [Google Scholar]
- Sachs, J; Malaney, P. The economic and social burden of malaria. Nature 2002, 415, 680–685. [Google Scholar]
- Cho-Min-Naing, ML; Gatton, ML. Costs to the patient for seeking malaria care in Myanmar. Acta Trop 2004, 92, 173–177. [Google Scholar]
- Chuma, JM; Thiede, M; Molyneux, CS. Rethinking the economic costs of malaria at the household level: Evidence from applying a new analytical framework in rural Kenya. Malar J 2006, 5, 76:1–76:14. [Google Scholar]
- MacGregor, J; Vorley, B. Fair Miles? The concept of “food miles” through a sustainable development lens.



{kind=link}
{kind=link}
| PF | RP | BP | GH | VT | SF | RE | MH | PCS | MCS | |
|---|---|---|---|---|---|---|---|---|---|---|
| General (df 901) | 0.1649 | 0.001a | < 0.0001a | 0.002a | 0.0003b | < 0.0001a | 0.8893 | 0.0001a | 0.0002a | 0.0979 |
| Males (df 413) | 0.0442 | 0.005a | 0.0003a | 0.0197a | 0.1084 | < 0.0001a | 0.4111 | < 0.0001a | 0.0048a | 0.0123a |
| Females (df 354) | 0.4467 | 0.1864 | 0.0016a | 0.1591 | 0.0044b | 0.0418a | 0.3837 | 0.714 | 0.7234 | 0.5444 |
| Characterisation details of Ugandan samples compared with U.S. population norms | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | Total | Malaria control | |||||||||
| Scale | Mean | df | p | Mean | df | p | Mean | df | p | Mean | df | p |
| PF | 54.44 | 1064 | < 0.001a | 51.28 | 1486 | < 0.001a | 52.84 | 2552 | < 0.001a | 53.45 | 2372 | < 0.001a |
| RP | 48.25 | 1064 | <0.001b | 41.85 | 1486 | < 0.001b | 45.01 | 2552 | < 0.001b | 46.81 | 2372 | < 0.001b |
| BP | 53.92 | 1063 | < 0.001a | 47.07 | 1486 | < 0.001b | 50.44 | 2551 | 0.312 | 52.34 | 2372 | < 0.001a |
| GH | 53.06 | 1063 | < 0.001a | 46.82 | 1484 | < 0.001b | 49.90 | 2549 | 0.662 | 51.57 | 2370 | 0.002a |
| VT | 51.98 | 1062 | 0.025a | 48.12 | 1485 | < 0.001b | 50.02 | 2549 | 0.962 | 51.59 | 2371 | 0.002a |
| SF | 51.65 | 1064 | 0.124 | 48.54 | 1485 | 0.015b | 50.07 | 2551 | 0.866 | 51.38 | 2371 | 0.006 |
| RE | 47.20 | 1064 | <0.001b | 43.94 | 1486 | < 0.001b | 45.54 | 2552 | < 0.001b | 47.06 | 2372 | < 0.001b |
| MH | 50.02 | 1062 | 0.009b | 45.86 | 1485 | < 0.001b | 47.91 | 2549 | < 0.001b | 49.50 | 2371 | 0.029b |
| PCS | 53.95 | 1060 | < 0.001a | 48.03 | 1484 | 0.002b | 50.94 | 2546 | 0.022a | 52.23 | 2370 | < 0.001a |
| MCS | 48.72 | 1060 | <0.001b | 45.64 | 1484 | < 0.001b | 47.15 | 2546 | < 0.001b | 48.63 | 2370 | < 0.001b |
| Characterisation detailsof Ugandan farm workers aged 18–34 with U.S.population norm | ||||||
|---|---|---|---|---|---|---|
| Total 18 – 34 | Malaria control (18–34) | |||||
| Scale | Mean | df | p | Mean | df | p |
| PF | 54.19 | 629 | 0.745 | 54.60 | 552 | 0.232 |
| RP | 46.28 | 629 | < 0.001b | 48.06 | 552 | <0.001b |
| BP | 52.05 | 629 | 1.000 | 53.65 | 552 | 0.018a |
| GH | 51.70 | 628 | 0.566 | 53.06 | 552 | 0.008a |
| VT | 51.08 | 628 | 0.002a | 52.80 | 552 | <0.001a |
| SF | 50.57 | 629 | 0.830 | 51.40 | 552 | 0.146 |
| RE | 45.69 | 629 | < 0.001b | 47.85 | 552 | <0.001b |
| MH | 48.76 | 627 | 0.590 | 50.24 | 552 | 0.103 |
| PCS | 52.74 | 627 | 0.007b | 53.64 | 552 | 0.755 |
| MCS | 47.26 | 627 | 0.166 | 49.00 | 552 | 0.160 |
| PF | RP | BP | GH | VT | SF | RE | MH | PCS | MCS | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 18–34 age group | U.K. | 50.26 | 47.27 | 48.37 | 49.37 | 51.48 | 45.93 | 47.95 | 46.43 | 51.97 | 46.79 |
| Uganda | 54.19 | 46.28 | 52.05 | 51.70 | 51.08 | 50.57 | 45.69 | 48.76 | 52.74 | 47.26 | |
| df | 826 | 826 | 797 | 779 | 789 | 794 | 804 | 78a8 | 748 | 748 | |
| p | < 0.001a | 0.091 | < 0.001a | < 0.001a | 0.397 | < 0.001a | < 0.001b | < 0.001a | 0.081 | 0.470 | |
| Malaria control 18–34 age group | U.K. | 50.26 | 47.27 | 48.37 | 49.37 | 51.48 | 45.93 | 47.95 | 46.43 | 51.97 | 46.79 |
| Uganda | 54.6 | 48.06 | 53.65 | 53.06 | 52.8 | 51.4 | 47.85 | 50.24 | 53.64 | 49 | |
| df | 749 | 749 | 720 | 703 | 713 | 717 | 727 | 713 | 673 | 673 | |
| p | < 0.001a | 0.442° | < 0.001a | < 0.001a | 0.088° | < 0.001a | 0.867° | < 0.001a | < 0.001a | 0.003a |
| Induction 2007 | 2006 | ||||||
|---|---|---|---|---|---|---|---|
| Mean | n | S.D. | Mean | n | S. D. | p | |
| PF | 54.94 | 193 | 4.42 | 54.1 | 395 | 7.78 | 0.3612 |
| RP | 53.2 | 193 | 6.28 | 50.26 | 395 | 8.55 | < 0.0001 |
| BP | 54.79 | 193 | 8.8 | 48.46 | 395 | 10.54 | < 0.0001 |
| GH | 51.57 | 193 | 8.08 | 49.16 | 395 | 8.99 | 0.0031 |
| VT | 57.05 | 193 | 7.84 | 51.38 | 395 | 9.67 | < 0.0001 |
| SF | 51.74 | 193 | 7.15 | 46.69 | 395 | 10.41 | < 0.0001 |
| RE | 52.88 | 193 | 6.38 | 49.97 | 395 | 9.27 | 0.0003 |
| MH | 51.39 | 193 | 8.88 | 46.1 | 395 | 10.6 | < 0.0001 |
| PCS | 54.46 | 193 | 4.82 | 52.07 | 395 | 6.78 | < 0.0001 |
| MCS | 52.03 | 193 | 7.7 | 46.71 | 395 | 9.98 | < 0.0001 |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Cross, P.; Edwards, R.T.; Nyeko, P.; Edwards-Jones, G. The Potential Impact on Farmer Health of Enhanced Export Horticultural Trade between the U.K. and Uganda. Int. J. Environ. Res. Public Health 2009, 6, 1539-1556. https://doi.org/10.3390/ijerph6051539
Cross P, Edwards RT, Nyeko P, Edwards-Jones G. The Potential Impact on Farmer Health of Enhanced Export Horticultural Trade between the U.K. and Uganda. International Journal of Environmental Research and Public Health. 2009; 6(5):1539-1556. https://doi.org/10.3390/ijerph6051539
Chicago/Turabian StyleCross, Paul, Rhiannon T Edwards, Philip Nyeko, and Gareth Edwards-Jones. 2009. "The Potential Impact on Farmer Health of Enhanced Export Horticultural Trade between the U.K. and Uganda" International Journal of Environmental Research and Public Health 6, no. 5: 1539-1556. https://doi.org/10.3390/ijerph6051539