Biomechanical Effect of UHMWPE and CFR-PEEK Insert on Tibial Component in Unicompartmental Knee Replacement in Different Varus and Valgus Alignments

Abstract
:1. Introduction
2. Materials and Methods
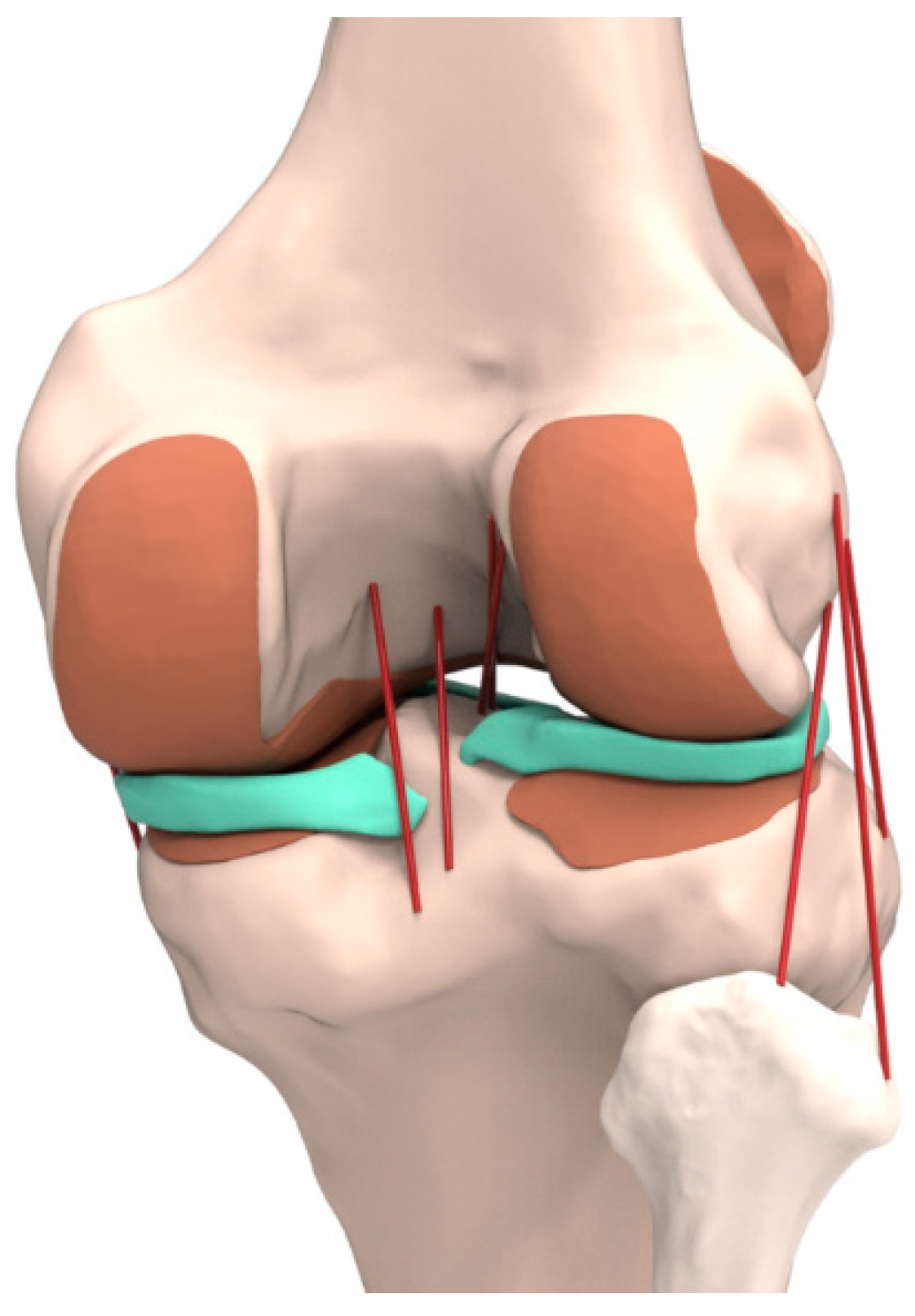
2.1. Intact Knee Joint Model
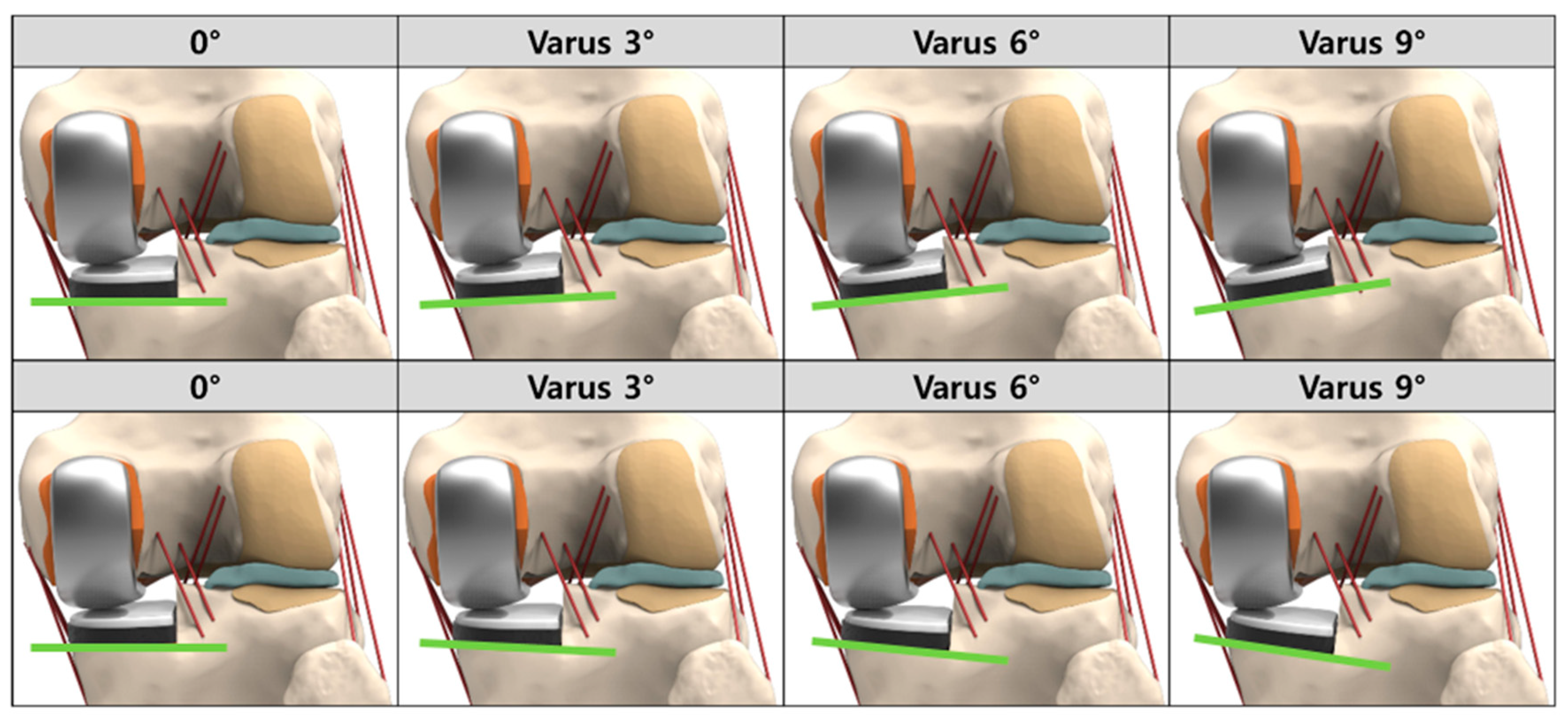
2.2. UKR Model
2.3. Loading and Boundary Conditions
3. Results
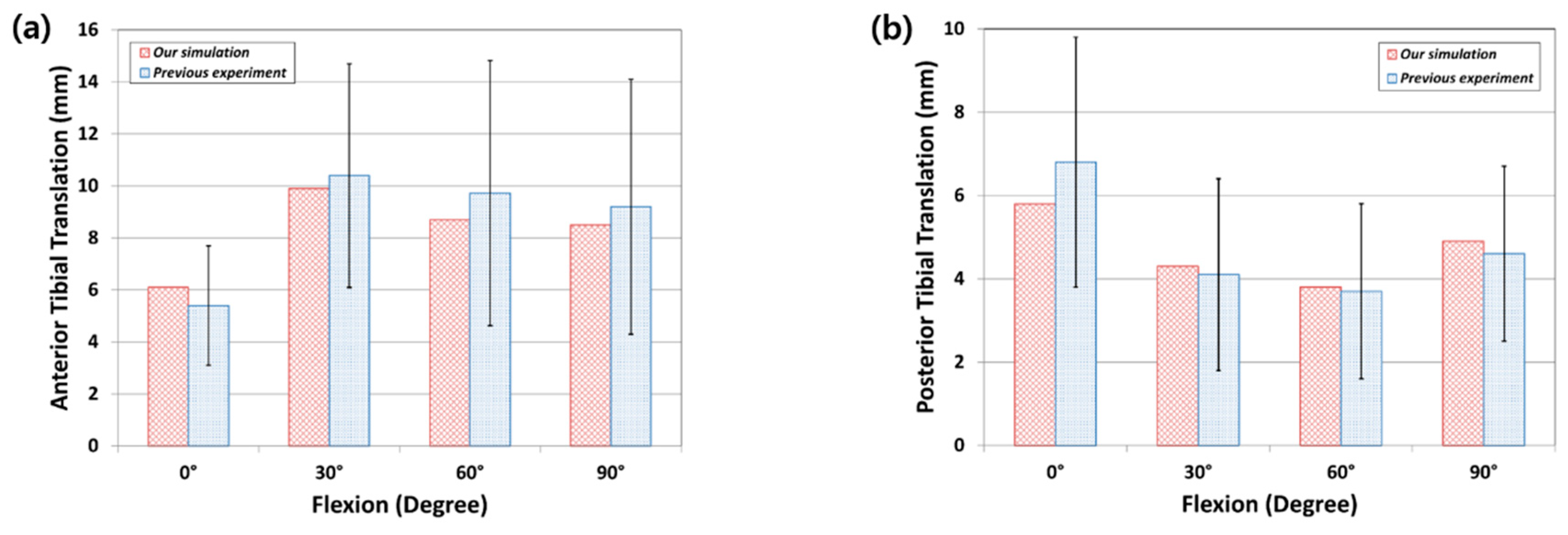
3.1. FE Model Validation
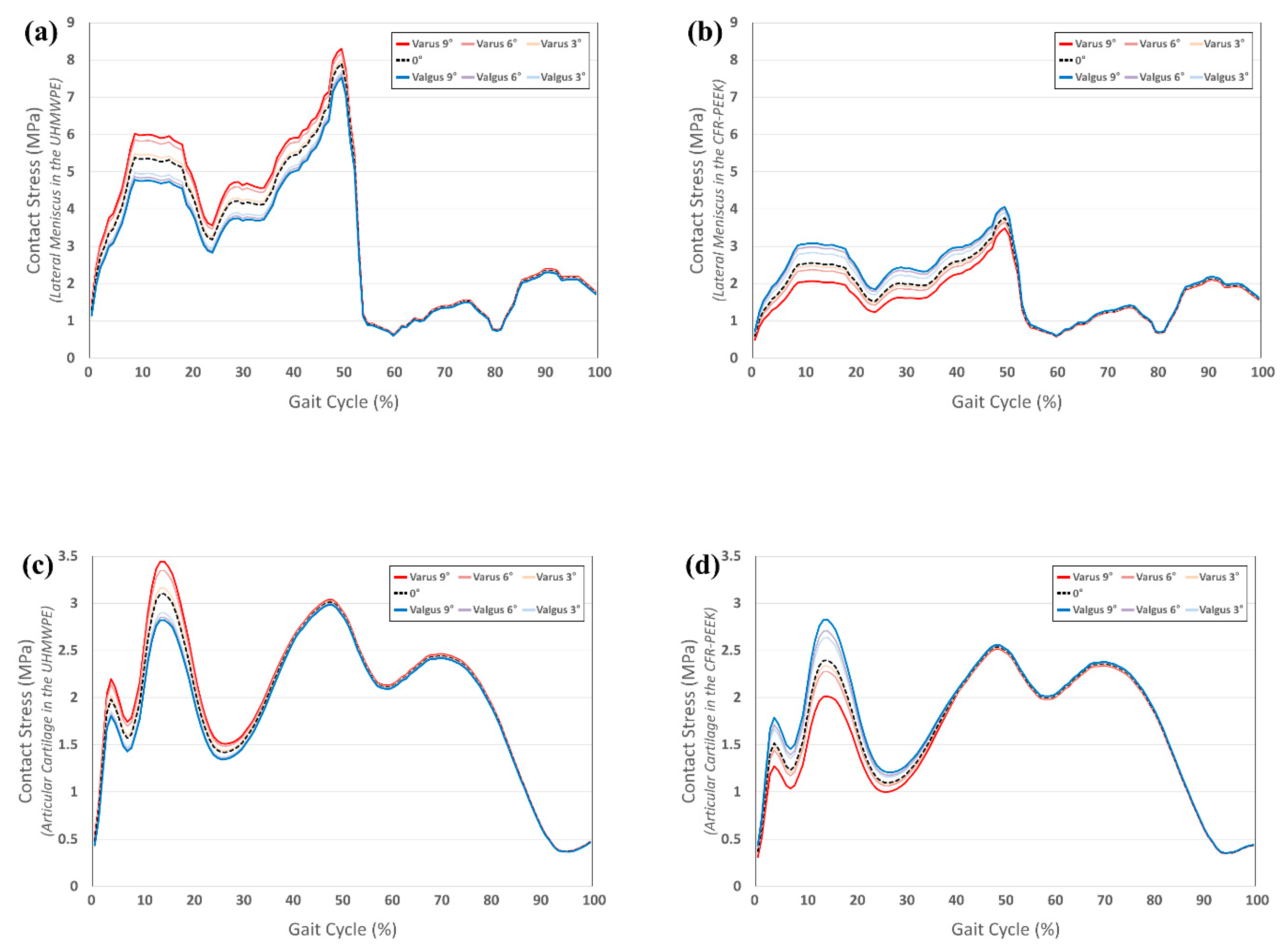
3.2. Comparison of Contact Stress on Other Compartments in UHMWPE and CFR-PEEK Tibial Component in Varus/Valgus Alignment
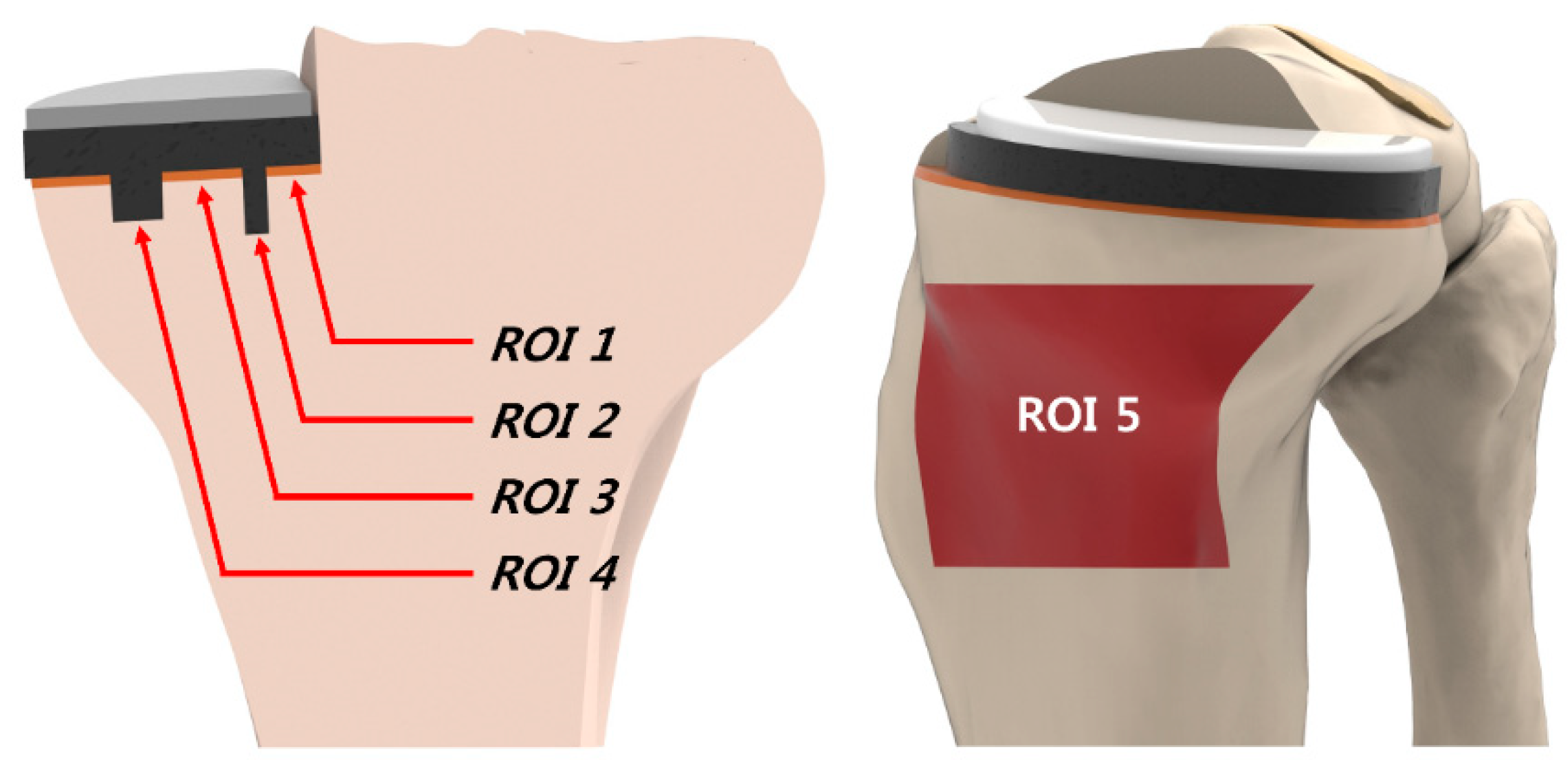
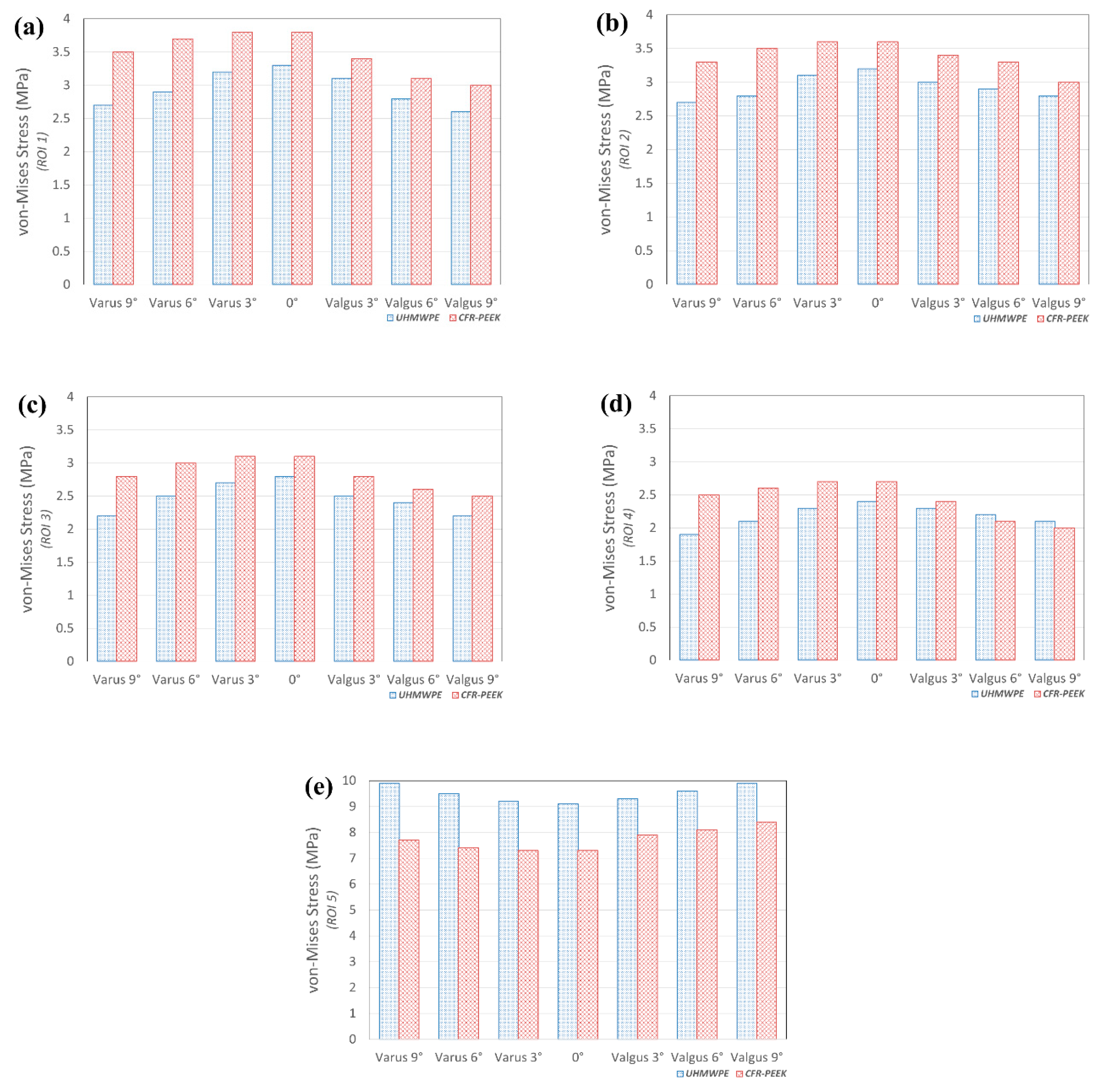
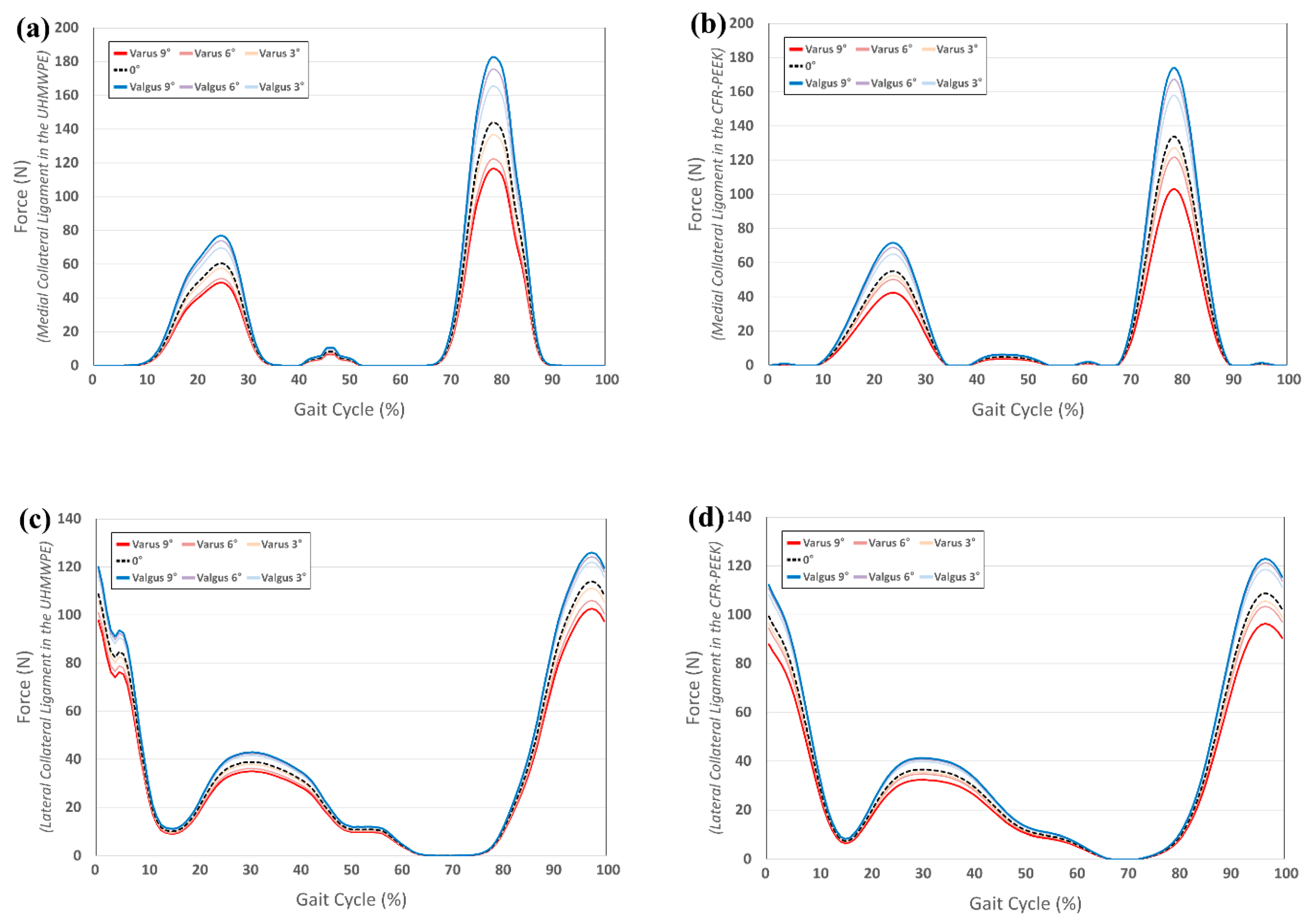
3.3. Comparison of Von-Mises Stress in Tibial Bone and Collateral Ligament Force in UHMWPE and CFR-PEEK Tibial Component in Varus/Valgus Alignment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Berger, R.A.; Meneghini, R.M.; Jacobs, J.J.; Sheinkop, M.B.; Della Valle, C.J.; Rosenberg, A.G.; Galante, J.O. Results of unicompartmental knee arthroplasty at a minimum of ten years of follow-up. J. Bone Joint Surg. Am. 2005, 87, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Riddle, D.L.; Jiranek, W.A.; McGlynn, F.J. Yearly incidence of unicompartmental knee arthroplasty in the United States. J. Arthroplast. 2008, 23, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, T.; Sato, T.; Tanifuji, O.; Kobayashi, K.; Koga, Y.; Yamagiwa, H.; Omori, G.; Endo, N. In vivo pre- and postoperative three-dimensional knee kinematics in unicompartmental knee arthroplasty. J. Orthop. Sci. 2013, 18, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Pandit, H.; Jenkins, C.; Gill, H.S.; Barker, K.; Dodd, C.A.; Murray, D.W. Minimally invasive Oxford phase 3 unicompartmental knee replacement: Results of 1000 cases. J. Bone Joint Surg. Br. 2011, 93, 198–204. [Google Scholar] [CrossRef] [PubMed]
- McAuley, J.P.; Engh, G.A.; Ammeen, D.J. Revision of failed unicompartmental knee arthroplasty. Clin. Orthop. Relat. Res. 2001, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, J.N.; Andriacchi, T.P.; Galante, J. Factors influencing walking and stairclimbing following unicompartmental knee arthroplasty. J. Arthroplast. 1986, 1, 109–115. [Google Scholar] [CrossRef]
- Wilcox, P.G.; Jackson, D.W. Unicompartmental knee arthroplasty. Orthop. Rev. 1986, 15, 490–495. [Google Scholar]
- Goodfellow, J.W.; Kershaw, C.J.; Benson, M.K.; O′Connor, J.J. The Oxford Knee for unicompartmental osteoarthritis. The first 103 cases. J. Bone Joint Surg. Br. 1988, 70, 692–701. [Google Scholar] [CrossRef]
- Klemme, W.R.; Galvin, E.G.; Petersen, S.A. Unicompartmental knee arthroplasty. Sequential radiographic and scintigraphic imaging with an average five-year follow-up. Clin. Orthop. Relat. Res. 1994, 301, 233–238. [Google Scholar]
- Weale, A.E.; Murray, D.W.; Baines, J.; Newman, J.H. Radiological changes five years after unicompartmental knee replacement. J. Bone Joint Surg. Br. 2000, 82, 996–1000. [Google Scholar] [CrossRef]
- Kennedy, W.R.; White, R.P. Unicompartmental arthroplasty of the knee. Postoperative alignment and its influence on overall results. Clin. Orthop. Relat. Res. 1987, 221, 278–285. [Google Scholar]
- Blunn, G.W.; Joshi, A.B.; Minns, R.J.; Lidgren, L.; Lilley, P.; Ryd, L.; Engelbrecht, E.; Walker, P.S. Wear in retrieved condylar knee arthroplasties. A comparison of wear in different designs of 280 retrieved condylar knee prostheses. J. Arthroplast. 1997, 12, 281–290. [Google Scholar] [CrossRef]
- Brockett, C.L.; Carbone, S.; Fisher, J.; Jennings, L.M. PEEK and CFR PEEK as an Alternative to UHMWPE in Total Knee Replacement; ORS Annual Meeting Las Vegas: Las Vegas, NV, USA, 2015. [Google Scholar]
- Brockett, C.L.; Carbone, S.; Fisher, J.; Jennings, L.M. PEEK and CFR-PEEK as alternative bearing materials to UHMWPE in a fixed bearing total knee replacement: An experimental wear study. Wear 2017, 374–375, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Scholes, S.C.; Unsworth, A. Pitch-based carbon-fibre-reinforced poly (ether-ether-ketone) OPTIMA assessed as a bearing material in a mobile bearing unicondylar knee joint. Proc. Inst. Mech. Eng. H 2009, 223, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Cartier, P.; Sanouiller, J.L.; Grelsamer, R.P. Unicompartmental knee arthroplasty surgery. 10-year minimum follow-up period. J. Arthroplast. 1996, 11, 782–788. [Google Scholar] [CrossRef]
- Thornhill, T.S.; Scott, R.D. Unicompartmental total knee arthroplasty. Orthop. Clin. N. Am. 1989, 20, 245–256. [Google Scholar]
- Kim, Y.S.; Kang, K.T.; Son, J.; Kwon, O.R.; Choi, Y.J.; Jo, S.B.; Choi, Y.W.; Koh, Y.G. Graft extrusion related to the position of allograft in lateral meniscal allograft transplantation: Biomechanical comparison between parapatellar and transpatellar approaches using finite element analysis. Arthroscopy 2015, 31, 2380–2391. [Google Scholar] [CrossRef]
- Kang, K.T.; Kim, S.H.; Son, J.; Lee, Y.H.; Chun, H.J. Computational model-based probabilistic analysis of in vivo material properties for ligament stiffness using the laxity test and computed tomography. J. Mater. Sci. Mater. Med. 2016, 27, 183. [Google Scholar] [CrossRef]
- Kwon, O.R.; Kang, K.T.; Son, J.; Suh, D.S.; Baek, C.; Koh, Y.G. Importance of joint line preservation in unicompartmental knee arthroplasty: Finite element analysis. J. Orthop. Res. 2017, 35, 347–352. [Google Scholar] [CrossRef]
- Kang, K.T.; Kim, S.H.; Son, J.; Lee, Y.H.; Kim, S.; Chun, H.J. Probabilistic evaluation of the material properties of the in vivo subject-specific articular surface using a computational model. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 1390–1400. [Google Scholar] [CrossRef]
- Pena, E.; Calvo, B.; Martinez, M.A.; Palanca, D.; Doblare, M. Why lateral meniscectomy is more dangerous than medial meniscectomy. A finite element study. J. Orthop. Res. 2006, 24, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Kayabasi, O.; Ekici, B. The effects of static, dynamic and fatigue behavior on three-dimensional shape optimization of hip prosthesis by finite element method. Mater. Des. 2007, 28, 2269–2277. [Google Scholar] [CrossRef]
- Hoffler, C.E.; Moore, K.E.; Kozloff, K.; Zysset, P.K.; Goldstein, S.A. Age, gender, and bone lamellae elastic moduli. J. Orthop. Res. 2000, 18, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, D.E.; Seedhom, B.B. The ′instantaneous′ compressive modulus of human articular cartilage in joints of the lower limb. Rheumatology 1999, 38, 124–132. [Google Scholar] [CrossRef]
- Haut Donahue, T.L.; Hull, M.L.; Rashid, M.M.; Jacobs, C.R. How the stiffness of meniscal attachments and meniscal material properties affect tibio-femoral contact pressure computed using a validated finite element model of the human knee joint. J. Biomech. 2003, 36, 19–34. [Google Scholar] [CrossRef]
- Guess, T.M.; Thiagarajan, G.; Kia, M.; Mishra, M. A subject specific multibody model of the knee with menisci. Med. Eng. Phys. 2010, 32, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Takeda, Y.; Xerogeanes, J.W.; Livesay, G.A.; Fu, F.H.; Woo, S.L. Biomechanical function of the human anterior cruciate ligament. Arthroscopy 1994, 10, 140–147. [Google Scholar] [CrossRef]
- Blankevoort, L.; Huiskes, R. Validation of a three-dimensional model of the knee. J. Biomech. 1996, 29, 955–961. [Google Scholar] [CrossRef] [Green Version]
- Zimmer, I. Zimmer Unicompartmental High Flex Knee: Intramedullary, Spacer Block Option and Extramedullary Minimally Invasive Surgical Techniques; Zimmer Biomet: Warsaw, IN, USA, 2005. [Google Scholar]
- Inoue, S.; Akagi, M.; Asada, S.; Mori, S.; Zaima, H.; Hashida, M. The Valgus Inclination of the Tibial Component Increases the Risk of Medial Tibial Condylar Fractures in Unicompartmental Knee Arthroplasty. J. Arthroplast. 2016, 31, 2025–2030. [Google Scholar] [CrossRef]
- Pegg, E.C.; Walter, J.; Mellon, S.J.; Pandit, H.G.; Murray, D.W.; D′Lima, D.D.; Fregly, B.J.; Gill, H.S. Evaluation of factors affecting tibial bone strain after unicompartmental knee replacement. J. Orthop. Res. 2013, 31, 821–828. [Google Scholar] [CrossRef]
- Godest, A.C.; Beaugonin, M.; Haug, E.; Taylor, M.; Gregson, P.J. Simulation of a knee joint replacement during a gait cycle using explicit finite element analysis. J. Biomech. 2002, 35, 267–275. [Google Scholar] [CrossRef]
- Innocenti, B.; Truyens, E.; Labey, L.; Wong, P.; Victor, J.; Bellemans, J. Can medio-lateral baseplate position and load sharing induce asymptomatic local bone resorption of the proximal tibia? A finite element study. J. Orthop. Surg. Res. 2009, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.-T.; Koh, Y.-G.; Son, J.; Yeom, J.S.; Park, J.-H.; Kim, H.-J. Biomechanical evaluation of pedicle screw fixation system in spinal adjacent levels using polyetheretherketone, carbon-fiber-reinforced polyetheretherketone, and traditional titanium as rod materials. Compos. Part B Eng. 2017, 130, 248–256. [Google Scholar] [CrossRef]
- Knight, L.A.; Pal, S.; Coleman, J.C.; Bronson, F.; Haider, H.; Levine, D.L.; Taylor, M.; Rullkoetter, P.J. Comparison of long-term numerical and experimental total knee replacement wear during simulated gait loading. J. Biomech. 2007, 40, 1550–1558. [Google Scholar] [CrossRef] [PubMed]
- Greco, A.C.; Erck, R.; Ajayi, O.; Fenske, G. Effect of reinforcement morphology on high-speed sliding friction and wear of PEEK polymers. Wear 2011, 271, 2222–2229. [Google Scholar] [CrossRef]
- Suggs, J.F.; Li, G.; Park, S.E.; Steffensmeier, S.; Rubash, H.E.; Freiberg, A.A. Function of the anterior cruciate ligament after unicompartmental knee arthroplasty: An in vitro robotic study. J. Arthroplast. 2004, 19, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Standardization, I.O. f. ISO 14243-1: Implants for Surgery—Wear of Total Knee-Joint Prostheses—Part 1: Loading and Displacement Parameters for Wear-Testing Machines with Load Control and Corresponding Environmental Conditions for Test; International Organization for Standardization: Geneva, Switzerland, 2002. [Google Scholar]
- Halloran, J.P.; Clary, C.W.; Maletsky, L.P.; Taylor, M.; Petrella, A.J.; Rullkoetter, P.J. Verification of predicted knee replacement kinematics during simulated gait in the Kansas knee simulator. J. Biomech. Eng. 2010, 132, 081010. [Google Scholar] [CrossRef]
- Kutzner, I.; Heinlein, B.; Graichen, F.; Bender, A.; Rohlmann, A.; Halder, A.; Beier, A.; Bergmann, G. Loading of the knee joint during activities of daily living measured in vivo in five subjects. J. Biomech. 2010, 43, 2164–2173. [Google Scholar] [CrossRef]
- Kang, K.T.; Koh, Y.G.; Son, J.; Kwon, O.R.; Baek, C.; Jung, S.H.; Park, K.K. Measuring the effect of femoral malrotation on knee joint biomechanics for total knee arthroplasty using computational simulation. Bone Joint Res. 2016, 5, 552–559. [Google Scholar] [CrossRef]
- Keene, G.; Simpson, D.; Kalairajah, Y. Limb alignment in computer-assisted minimally-invasive unicompartmental knee replacement. J. Bone Joint Surg. Br. 2006, 88, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.A.; Hast, M.W.; Granger, J.F.; Piazza, S.J.; Siston, R.A. Biomechanical effects of total knee arthroplasty component malrotation: A computational simulation. J. Orthop. Res. 2011, 29, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Sawatari, T.; Tsumura, H.; Iesaka, K.; Furushiro, Y.; Torisu, T. Three-dimensional finite element analysis of unicompartmental knee arthroplasty—The influence of tibial component inclination. J. Orthop. Res. 2005, 23, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Iesaka, K.; Tsumura, H.; Sonoda, H.; Sawatari, T.; Takasita, M.; Torisu, T. The effects of tibial component inclination on bone stress after unicompartmental knee arthroplasty. J. Biomech. 2002, 35, 969–974. [Google Scholar] [CrossRef]
- Simpson, D.J.; Price, A.J.; Gulati, A.; Murray, D.W.; Gill, H.S. Elevated proximal tibial strains following unicompartmental knee replacement—A possible cause of pain. Med. Eng. Phys. 2009, 31, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.D.; Guo, W.S.; Zhang, Q.D.; Liu, Z.H.; Cheng, L.M. Finite Element Analysis of Mobile-bearing Unicompartmental Knee Arthroplasty: The Influence of Tibial Component Coronal Alignment. Chin. Med. J. 2015, 128, 2873–2878. [Google Scholar] [CrossRef] [PubMed]
- Innocenti, B.; Pianigiani, S.; Ramundo, G.; Thienpont, E. Biomechanical Effects of Different Varus and Valgus Alignments in Medial Unicompartmental Knee Arthroplasty. J. Arthroplast. 2016, 31, 2685–2691. [Google Scholar] [CrossRef]
- Hernigou, P.; Deschamps, G. Alignment influences wear in the knee after medial unicompartmental arthroplasty. Clin. Orthop. Relat. Res. 2004, 423, 161–165. [Google Scholar] [CrossRef]
- Segal, N.A.; Anderson, D.D.; Iyer, K.S.; Baker, J.; Torner, J.C.; Lynch, J.A.; Felson, D.T.; Lewis, C.E.; Brown, T.D. Baseline articular contact stress levels predict incident symptomatic knee osteoarthritis development in the MOST cohort. J. Orthop. Res. 2009, 27, 1562–1568. [Google Scholar] [CrossRef] [Green Version]
- Heyse, T.J.; El-Zayat, B.F.; De Corte, R.; Scheys, L.; Chevalier, Y.; Fuchs-Winkelmann, S.; Labey, L. Balancing UKA: Overstuffing leads to high medial collateral ligament strains. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3218–3228. [Google Scholar] [CrossRef]
- Berger, R.A.; Nedeff, D.D.; Barden, R.M.; Sheinkop, M.M.; Jacobs, J.J.; Rosenberg, A.G.; Galante, J.O. Unicompartmental knee arthroplasty. Clinical experience at 6- to 10-year followup. Clin. Orthop. Relat. Res. 1999, 367, 50–60. [Google Scholar]
- Innocenti, B.; Bilgen, O.F.; Labey, L.; van Lenthe, G.H.; Sloten, J.V.; Catani, F. Load sharing and ligament strains in balanced, overstuffed and understuffed UKA. A validated finite element analysis. J. Arthroplast. 2014, 29, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.L.; Burstein, A.H.; Santavicca, E.A.; Insall, J.N. Performance of the tibial component in total knee replacement. J. Bone Joint. Surg. Am. 1982, 64, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.B.; Finlay, J.B. The influence of tibial component intramedullary stems and implant-cortex contact on the strain distribution of the proximal tibia following total knee arthroplasty. An in vitro study. Clin. Orthop. Relat. Res. 1986, 208, 95–99. [Google Scholar] [CrossRef]
- Taylor, M.; Tanner, K.E.; Freeman, M.A. Finite element analysis of the implanted proximal tibia: A relationship between the initial cancellous bone stresses and implant migration. J. Biomech. 1998, 31, 303–310. [Google Scholar] [CrossRef]
- Au, A.G.; Raso, V.J.; Liggins, A.B.; Otto, D.D.; Amirfazli, A. A three-dimensional finite element stress analysis for tunnel placement and buttons in anterior cruciate ligament reconstructions. J. Biomech. 2005, 38, 827–832. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Material Properties |
|---|---|
| Cortical bone [23,24] | E1 = E2 = 11.5 GPa E3 = 17 GPa ν12 = 0.51, ν23 = ν13 = 0.31 |
| Cancellous bone [23,24] | E = 2.13 GPa ν = 0.3 |
| Articular cartilage [25] | E = 15 MPa ν = 0.47 |
| Menisci [26] | Ec = 120 MPa (in the circumferential direction) Ea = Er = 20 MPa MPa (in the axial and radial directions.) vcr = 0.3 (for axial directions) var = vac = 0.3 (for circumferential and radial directions) |
| Materials | Material Properties |
|---|---|
| CoCr | E = 195 GPa v = 0.3 |
| Ti6Al4V | E = 110 GPa v = 0.3 |
| UHMWPE | E = 685 MPa v = 0.47 |
| CFR-PEEK | E = 18000 MPa v = 0.4 |
| PMMA | E = 1940 MPa and v = 0.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koh, Y.-G.; Hong, H.-T.; Kang, K.-T. Biomechanical Effect of UHMWPE and CFR-PEEK Insert on Tibial Component in Unicompartmental Knee Replacement in Different Varus and Valgus Alignments. Materials 2019, 12, 3345. https://doi.org/10.3390/ma12203345
Koh Y-G, Hong H-T, Kang K-T. Biomechanical Effect of UHMWPE and CFR-PEEK Insert on Tibial Component in Unicompartmental Knee Replacement in Different Varus and Valgus Alignments. Materials. 2019; 12(20):3345. https://doi.org/10.3390/ma12203345
Chicago/Turabian StyleKoh, Yong-Gon, Hyoung-Taek Hong, and Kyoung-Tak Kang. 2019. "Biomechanical Effect of UHMWPE and CFR-PEEK Insert on Tibial Component in Unicompartmental Knee Replacement in Different Varus and Valgus Alignments" Materials 12, no. 20: 3345. https://doi.org/10.3390/ma12203345