Biomechanical Behaviour and Biocompatibility of Ureidopyrimidinone-Polycarbonate Electrospun and Polypropylene Meshes in a Hernia Repair in Rabbits

 , and
, and
Abstract
:
1. Introduction
2. Results
2.1. Dry Mesh
2.2. Clinical Findings and Gross Anatomy
2.3. Biomechanical Testing of the Explants
2.4. Inflammatory Response and Neovascularization
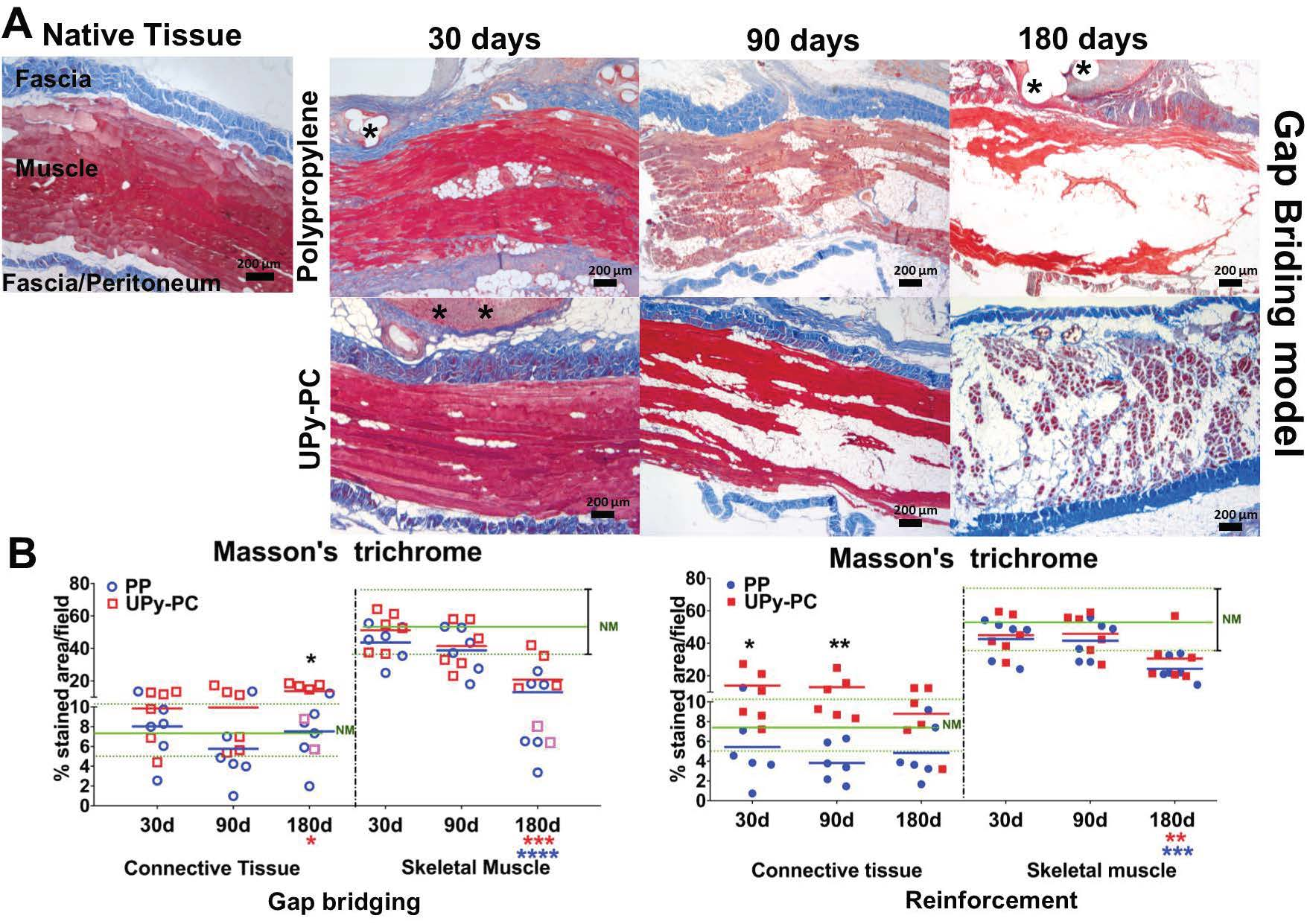
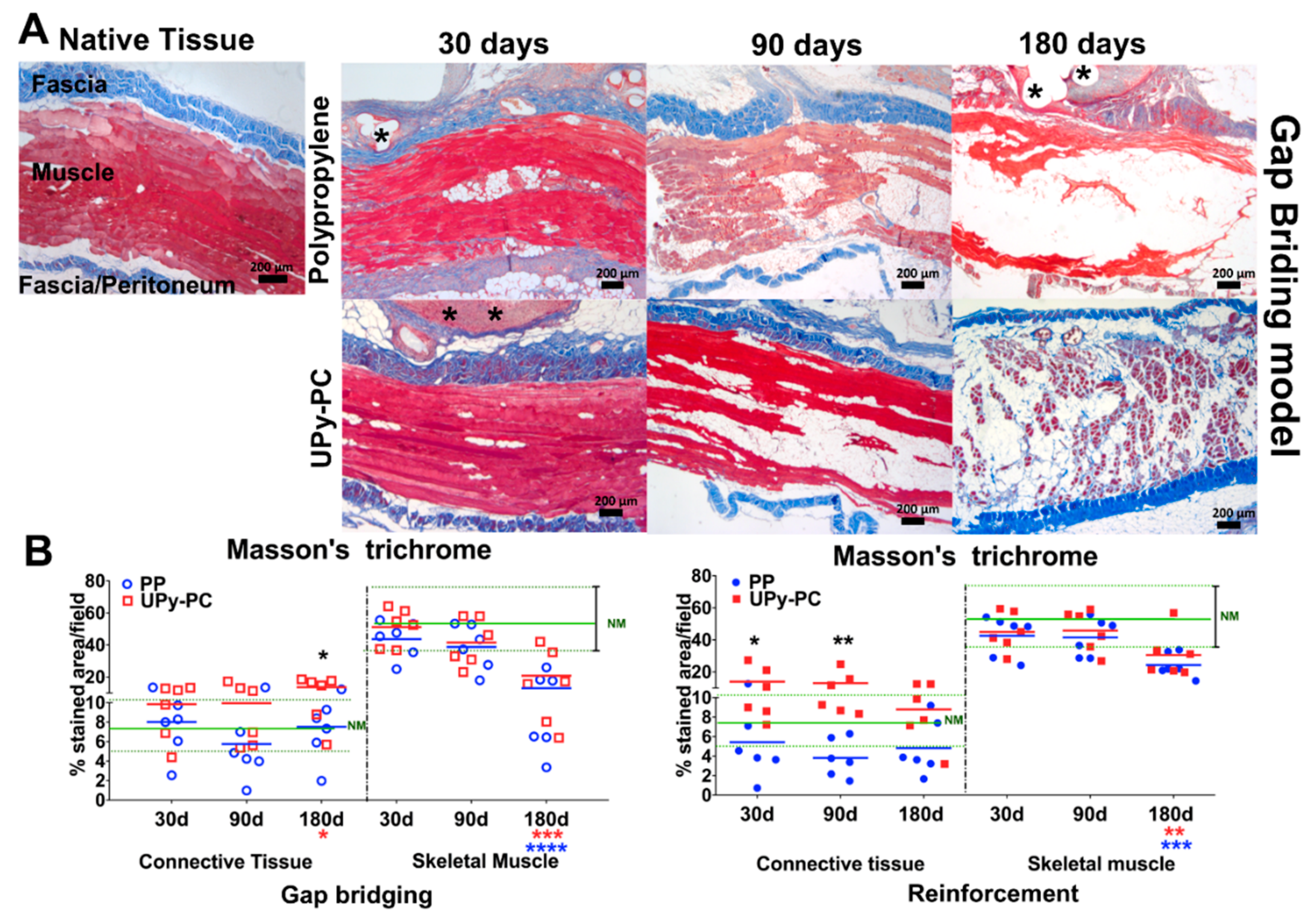
2.5. Musculofascial Characteristics of the Explants
3. Discussion
4. Material and Methods
4.1. Meshes
4.2. Study Design and Surgical Procedure
4.3. Clinical Examination and Sizing of the Implants
4.4. Biomechanical Testing of Explants
4.5. Histology
4.6. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Flum, D.R.; Horvath, K.; Koepsell, T. Have outcomes of incisional hernia repair improved with time? A population-based analysis. Ann. Surg. 2003, 237, 129–135. [Google Scholar] [PubMed]
- Christmann-Schmid, C.; Marjoribanks, J.; Maher, C.; Baessler, K.; Feiner, B.; Haya, N. Transvaginal mesh or grafts compared with native tissue repair for vaginal prolapse. Cochrane Database Syst. Rev. 2016, 2, CD012079. [Google Scholar]
- Olsen, A.L.; Smith, V.J.; Bergstrom, J.O.; Colling, J.C.; Clark, A.L. Epidemiology of Surgically Managed Pelvic Organ Prolapse and Urinary Incontinence. Am. Coll. Obstet. Gynecol. 1997, 89, 501–506. [Google Scholar] [CrossRef]
- Burger, J.W.A.; Luijendijk, R.W.; Hop, W.C.J.; Halm, J.A.; Verdaasdonk, E.G.G.; Jeekel, J. Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann. Surg. 2004, 240, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Todros, S.; Pavan, P.G.; Natali, A.N. Synthetic surgical meshes used in abdominal wall surgery: Part I—Materials and structural conformation. J. Biomed. Mater. Res. Part B Appl. Biomater. 2017, 105, 689–699. [Google Scholar]
- Klosterhalfen, B.; Junge, K.; Klinge, U. The lightweight and large porous mesh concept for hernia repair. Expert Rev. Med. Devices 2005, 2, 103–117. [Google Scholar] [CrossRef]
- Liang, R.; Abramowitch, S.; Knight, K.; Palcsey, S.; Nolfi, A.; Feola, A.; Stein, S.; Moalli, P.A. Vaginal degeneration following implantation of synthetic mesh with increased stiffness. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 233–243. [Google Scholar]
- Junge, K.; Klinge, U.; Binnebösel, M.; Jansen, P.L.; Neumann, U.P.; von Trotha, K.T.; Rosch, R. Mesh biocompatibility: Effects of cellular inflammation and tissue remodelling. Langenbeck’s Arch. Surg. 2011, 397, 255–270. [Google Scholar]
- Brown, C.N.; Finch, J.G. Which mesh for hernia repair? Ann. R. Coll. Surg. Engl. 2010, 92, 272–278. [Google Scholar] [CrossRef]
- Klinge, U.; Klosterhalfen, B.; Müller, M.; Schumpelick, V. Foreign body reaction to meshes used for the repair of abdominal wall hernias. Eur. J. Surg. 1999, 165, 665–673. [Google Scholar] [PubMed]
- Maurer, M.M.; Röhrnbauer, B.; Feola, A.; Deprest, J.; Mazza, E. Prosthetic meshes for repair of hernia and pelvic organ prolapse: Comparison of biomechanical properties. Materials 2015, 8, 2794–2808. [Google Scholar]
- Feola, A.; Abramowitch, S.; Jallah, Z.; Stein, S.; Barone, W.; Palcsey, S.; Moalli, P. Deterioration in biomechanical properties of the vagina following implantation of a high-stiffness prolapse mesh. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 224–232. [Google Scholar]
- Junge, K.; Klinge, U.; Prescher, A.; Giboni, P.; Niewiera, M.; Schumpelick, V. Elasticity of the anterior abdominal wall and impact for reparation of incisional hernias using mesh implants. Hernia 2001, 5, 113–118. [Google Scholar]
- Deeken, C.R.; Lake, S.P. Mechanical properties of the abdominal wall and biomaterials utilized for hernia repair. J. Mech. Behav. Biomed. Mater. 2017, 74, 411–427. [Google Scholar] [CrossRef]
- Culbertson, E.J.; Xing, L.; Wen, Y.; Franz, M.G. Reversibility of abdominal wall atrophy and fibrosis after primary or mesh herniorrhaphy. Ann. Surg. 2013, 257, 142–149. [Google Scholar] [PubMed]
- Deeken, C.R.; Eliason, B.J.; Pichert, M.D.; Grant, S.A.; Frisella, M.M.; Matthews, B.D. Differentiation of biologic scaffold materials through physicomechanical, thermal, and enzymatic degradation techniques. Ann. Surg. 2012, 255, 595–604. [Google Scholar]
- Scott, J.R.; Deeken, C.R.; Martindale, R.G.; Rosen, M.J. Evaluation of a fully absorbable poly-4-hydroxybutyrate/absorbable barrier composite mesh in a porcine model of ventral hernia repair. Surg. Endosc. 2016, 30, 3691–3701. [Google Scholar]
- SCENIHR. Opinion on The Safety of Surgical Meshes Used in Urogynecological Surgery. Available online: https://ec.europa.eu/health/scientific_committees/emerging/docs/scenihr_o_049.pdf (accessed on 5 October 2018).
- Elango, S.; Perumalsamy, S.; Ramachandran, K.; Vadodaria, K. Mesh materials and hernia repair. BioMedicine 2017, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Hympanova, L.; da Cunha, M.G.M.C.; Rynkevic, R.; Wach, R.A.; Olejnik, A.K.; Dankers, P.Y.W.; Arts, B.; Mes, T.; Bosman, A.W.; Albersen, M. Experimental reconstruction of an abdominal wall defect with electrospun polycaprolactone-ureidopyrimidinone mesh conserves compliance yet may have insufficient strength. J. Mech. Behav. Biomed. Mater. 2018, 88, 431–441. [Google Scholar] [CrossRef]
- Webber, M.J.; Appel, E.A.; Meijer, E.W.; Langer, R. Supramolecular biomaterials. Nat. Mater. 2015, 15, 13–26. [Google Scholar] [CrossRef]
- Vashaghian, M.; Ruiz-Zapata, A.M.; Kerkhof, M.H.; Zandieh-Doulabi, B.; Werner, A.; Roovers, J.P.; Smit, T.H. Toward a New Generation of Pelvic Floor Implants With Electrospun Nanofibrous Matrices: A Feasibility Study. Neurourol. Urodyn. 2017, 37, 565–573. [Google Scholar]
- Mollet, B.B.; Comellas-Aragonès, M.; Spiering, A.J.H.; Sontjens, S.H.M.; Meijer, E.W.; Dankers, P.Y.W. A modular approach to easily processable supramolecular bilayered scaffolds with tailorable properties. J. Mater. Chem. B 2014, 2, 2483–2493. [Google Scholar]
- Hympanova, L.; Mori da Cunha, M.G.M.C.; Rynkevic, R.; Zündel, M.; Gallego, M.R.; Vange, J.; Callewaert, G.; Urbankova, I.; van der Aa, F.; Mazza, E.; et al. Physiologic musculofascial compliance following reinforcement with electrospun polycaprolactone-ureidopyrimidinone mesh in a rat model. J. Mech. Behav. Biomed. Mater. 2017, 74, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Guan, J.; Fujimoto, K.L.; Hashizume, R.; Anca, L.; Wagner, W.R. Tailoring the degradation kinetics of poly(ester-carbonate urethane)urea thermoplastic elastomers for tissue engineering scaffolds. Biomaterials 2011, 31, 4249–4258. [Google Scholar]
- Ma, Z.; Hong, Y.; Nelson, D.M.; Pichamuthu, J.E.; Leeson, C.E.; Wagner, W.R. Biodegradable polyurethane ureas with variable polyester or polycarbonate soft segments: Effects of crystallinity, molecular weight, and composition on mechanical properties. Biomacromolecules 2011, 12, 3265–3274. [Google Scholar]
- Fukushima, K. Poly(trimethylene carbonate)-based polymers engineered for biodegradable functional biomaterials. Biomater. Sci. 2016, 4, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Bennink, G.; Torii, S.; Brugmans, M.; Cox, M.; Svanidze, O.; Ladich, E.; Carrel, T.; Virmani, R. A novel restorative pulmonary valved conduit in a chronic sheep model: Mid-term hemodynamic function and histologic assessment. J. Thorac. Cardiovasc. Surg. 2018, 155, 2591–2601. [Google Scholar] [CrossRef]
- Konerding, M.A.; Bohn, M.; Wolloscheck, T.; Batke, B.; Holste, J.L.; Wohlert, S.; Trzewik, J.; Förstemann, T.; Hartung, C. Maximum forces acting on the abdominal wall: Experimental validation of a theoretical modeling in a human cadaver study. Med. Eng. Phys. 2011, 33, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Konerding, M.A.; Chantereau, P.; Delventhal, V.; Holste, J.L.; Ackermann, M. Biomechanical and histological evaluation of abdominal wall compliance with intraperitoneal onlay mesh implants in rabbits: A comparison of six different state-of-the-art meshes. Med. Eng. Phys. 2012, 34, 806–816. [Google Scholar] [CrossRef]
- Boontheekul, T.; Hill, E.E.; Kong, H.-J.; Mooney, D.J. Regulating Myoblast Phenotype Through Controlled Gel Stiffness and Degradation. Tissue Eng. 2007, 13, 1431–1442. [Google Scholar] [CrossRef]
- Klinge, U.; Müller, M.; Brücker, C.; Schumpelick, V. Application of three-dimensional stereography to assess abdominal wall mobility. Hernia 2005, 2, 11–14. [Google Scholar] [CrossRef]
- Arbos, M.A.; Ferrando, J.M.; Quiles, M.T.; Vidal, J.; López-Cano, M.; Gil, J.; Manero, J.M.; Peña, J.; Huguet, P.; Schwartz-Riera, S.; et al. Improved surgical mesh integration into the rat abdominal wall with arginine administration. Biomaterials 2006, 27, 758–768. [Google Scholar] [CrossRef]
- Li, Y.; Chu, Z.; Li, X.; Ding, X.; Guo, M.; Zhao, H.; Yao, J.; Wang, L.; Cai, Q.; Fan, Y. The effect of mechanical loads on the degradation of aliphatic biodegradable polyesters. Regen. Biomater. 2017, 4, 179–190. [Google Scholar] [CrossRef]
- Zaccaria, S.; van Gaal, R.C.; Riool, M.; Zaat, S.A.J.; Dankers, P.Y.W. Antimicrobial peptide modification of biomaterials using supramolecular additives. J. Polym. Sci. Part A Polym. Chem. 2018, 56, 1926–1934. [Google Scholar] [CrossRef]
- De Feijter, I.; Goor, O.J.; Hendrikse, S.I.; Comellas-Aragonès, M.; Söntjens, S.H.; Zaccaria, S.; Fransen, P.P.; Peeters, J.W.; Milroy, L.G.; Dankers, P.Y. Solid-Phase-Based Synthesis of Ureidopyrimidinone-Peptide Conjugates for Supramolecular Biomaterials. Synlett 2015, 26, 2707–2713. [Google Scholar]
- Dankers, P.Y.W. Supramolecular Biomaterials: Introducing a Modular Approach. Ph.D. Thesis, Eindhoven University of Technology, Eindhoven, The Netherlands, May 2006. [Google Scholar]
- Sheikh, Z.; Brooks, P.J.; Barzilay, O.; Fine, N.; Glogauer, M. Macrophages, foreign body giant cells and their response to implantable biomaterials. Materials 2015, 8, 5671–5701. [Google Scholar] [CrossRef]
- Brown, B.N.; Mani, D.; Nolfi, A.L.; Liang, R.; Abramowitch, S.D.; Moalli, P.A. Characterization of the host inflammatory response following implantation of prolapse mesh in rhesus macaque. Am. J. Obstet. Gynecol. 2015, 213, 668.e1–668.e10. [Google Scholar] [CrossRef]
- Gao, Y.; Arfat, Y.; Wang, H.; Goswami, N. Muscle atrophy induced by mechanical unloading: Mechanisms and potential countermeasures. Front. Physiol. 2018, 9, 235. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, E.; Duarte, J.A. Skeletal Muscle Loading Changes its Regenerative Capacity. Sports Med. 2016, 46, 783–792. [Google Scholar] [PubMed]
- Uezumi, A.; Ito, T.; Morikawa, D.; Shimizu, N.; Yoneda, T.; Segawa, M.; Yamaguchi, M.; Ogawa, R.; Matev, M.M.; Miyagoe-Suzuki, Y.; et al. Fibrosis and adipogenesis originate from a common mesenchymal progenitor in skeletal muscle. J. Cell Sci. 2011, 124, 3654–3664. [Google Scholar] [CrossRef]
- Uezumi, A.; Fukada, S.I.; Yamamoto, N.; Takeda, S.; Tsuchida, K. Mesenchymal progenitors distinct from satellite cells contribute to ectopic fat cell formation in skeletal muscle. Nat. Cell Biol. 2010, 12, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Pagano, A.F.; Demangel, R.; Brioche, T.; Jublanc, E.; Bertrand-Gaday, C.; Candau, R.; Dechesne, C.A.; Dani, C.; Bonnieu, A.; Py, G.; et al. Muscle Regeneration with Intermuscular Adipose Tissue (IMAT) Accumulation Is Modulated by Mechanical Constraints. PLoS ONE 2015, 10, e0144230. [Google Scholar] [CrossRef] [PubMed]
- Maeda, E.; Asanuma, H.; Noguchi, H.; Tohyama, H.; Yasuda, K.; Hayashi, K. Effects of stress shielding and subsequent restressing on mechanical properties of regenerated and residual tissues in rabbit patellar tendon after resection of its central one-third. J. Biomech. 2009, 42, 1592–1597. [Google Scholar] [CrossRef]
- Hamrick, M.W.; McGee-Lawrence, M.E.; Frechette, D.M. Fatty Infiltration of Skeletal Muscle: Mechanisms and Comparisons with Bone Marrow Adiposity. Front. Endocrinol. 2016, 7, 69. [Google Scholar] [CrossRef]
- Gladstone, J.N.; Bishop, J.Y.; Lo, I.K.Y.; Flatow, E.L. Fatty infiltration and atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with poor functional outcome. Am. J. Sports Med. 2007, 35, 719–728. [Google Scholar] [CrossRef]
- Bruce, C.R.; Dyck, D.J. Cytokine regulation of skeletal muscle fatty acid metabolism: Effect of interleukin-6 and tumor necrosis factor-alpha. Am. J. Physiol. Endocrinol. Metab. 2004, 287, E616–E621. [Google Scholar] [CrossRef]
- Petersen, E.W. Acute IL-6 treatment increases fatty acid turnover in elderly humans in vivo and in tissue culture in vitro. Am. J. Phys. Endocrinol. Metab. 2004, 288, E155–E162. [Google Scholar] [CrossRef] [PubMed]
- Mutwali, I. Incisional hernia: Risk factors, incidence, pathogenesis, prevention and complications. Sudan Med. Monit. 2014, 9, 81. [Google Scholar] [CrossRef]
- Amato, G.; Agrusa, A.; Romano, G.; Salamone, G.; Gulotta, G.; Silvestri, F.; Bussani, R. Muscle degeneration in inguinal hernia specimens. Hernia 2012, 16, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Köckerling, F.; Koch, A.; Lorenz, R.; Schug-Pass, C.; Stechemesser, B.; Reinpold, W. How Long Do We Need to Follow-Up Our Hernia Patients to Find the Real Recurrence Rate? Front. Surg. 2015, 2, 24. [Google Scholar] [CrossRef] [PubMed]
- Ozog, Y.; Konstantinovic, M.L.; Werbrouck, E. Persistence of polypropylene mesh anisotropy after implantation: An experimental study. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 1180–1185. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Native Muscle | Macroporous Polypropylene (Restorelle®) | Electrospun Polycarbonate Ureidopyrimidinone (UPy-PC) |
|---|---|---|---|
| Mesh thickness (µm) | - | 300 | 250–300 |
| Fiber size (µm) | - | 80.0 | 1.86–3.2 |
| Density (g/m2) | - | 19.0 | 41 |
| Comfort zone stiffness (N/mm) | 0.20 ± 0.14 # | 0.57 ± 0.06 # *** | 0.07 ± 0.06 *** |
| Comfort zone young’s modulus (N/mm2) | 0.17 ± 0.09 # | 3.94 ± 0.3 # **** | 0.38 ± 0.015 **** |
| Time Point | 30 days | 90 days | 180 days | ||||
|---|---|---|---|---|---|---|---|
| Group | PP | UPy-PC | PP | UPy-PC | PP | UPy-PC | |
| Gap bridging | Signs of degradation | 0% (0/6) | 0% (0/6) | 0% (0/6) | 50% (3/6) | 0% (0/6) | 100% (6/6) |
| Recurrence of hernia | 0% (0/6) | 0% (0/6) | 0% (0/6) | 0% (0/6) | 0% (0/6) | 33% (2/6) | |
| Contraction (-) | −20.8 ± 6.43% | −5.4 ± 4.7% | −15 ± 5.2% | +4 ± 10.4% | −15 ± 7.6% | +1.7 ± 13.5% | |
| Reinforcement | Signs of degradation | 0% (0/6) | 0% (0/6) | 0% (0/6) | 18.6% (1/6) | 0% (0/6) | 100% (6/6) |
| Recurrence of hernia | 0% (0/6) | 0% (0/6) | 0% (0/6) | 0% (0/6) | 0% (0/6) | 0% (0/6) | |
| Contraction (-) | +12.7 ± 5.9% | +12.7 ± 6.2% | +7.6 ± 5.3% | +21.3 ± 10.1% | +1.52 ± 7.8% | +22.1 ± 9.8% | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori da Cunha, M.G.M.C.; Hympanova, L.; Rynkevic, R.; Mes, T.; Bosman, A.W.; Deprest, J. Biomechanical Behaviour and Biocompatibility of Ureidopyrimidinone-Polycarbonate Electrospun and Polypropylene Meshes in a Hernia Repair in Rabbits. Materials 2019, 12, 1174. https://doi.org/10.3390/ma12071174
Mori da Cunha MGMC, Hympanova L, Rynkevic R, Mes T, Bosman AW, Deprest J. Biomechanical Behaviour and Biocompatibility of Ureidopyrimidinone-Polycarbonate Electrospun and Polypropylene Meshes in a Hernia Repair in Rabbits. Materials. 2019; 12(7):1174. https://doi.org/10.3390/ma12071174
Chicago/Turabian StyleMori da Cunha, Marina Gabriela M. C., Lucie Hympanova, Rita Rynkevic, Tristan Mes, Anton W. Bosman, and Jan Deprest. 2019. "Biomechanical Behaviour and Biocompatibility of Ureidopyrimidinone-Polycarbonate Electrospun and Polypropylene Meshes in a Hernia Repair in Rabbits" Materials 12, no. 7: 1174. https://doi.org/10.3390/ma12071174