A Systematic Critical Appraisal of the Methodological Quality of Systematic Reviews on the Effect of Autologous Platelet Concentrates in the Treatment of Periodontal Intraosseous Defects

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Literature Search
2.3. Inclusion and Exclusion Criteria
- SRs and meta-analyses of either randomized controlled trials or controlled clinical trials on the effect of APCs on the treatment of periodontal intraosseous defects;
- SRs that evaluated the effect of any type of APC, either alone or in conjunction with other bio-materials or procedures, compared with a non-APC control.
- Narrative reviews;
- SRs including trials on non-intraosseous periodontal defects (or in which such data could not be extracted);
- SRs of in vitro or animal studies.
2.4. Review Selection Process
2.5. Data Extraction
2.6. Methodological Assessment of the Systematic Reviews (SRs)
3. Results
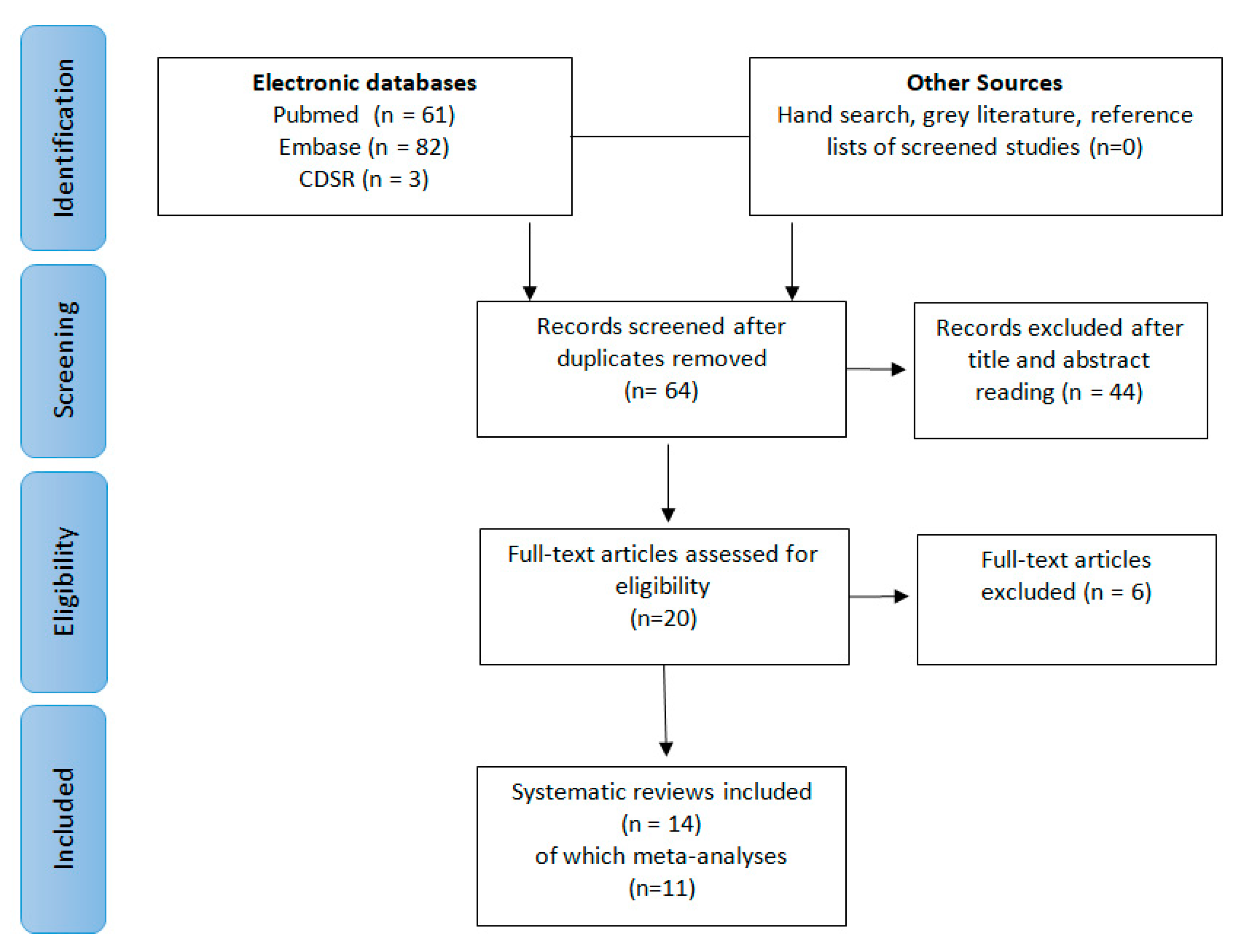
3.1. Study Selection
3.2. Characteristics of the SRs Included
3.3. Methodological Quality
3.4. Summary of Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marx, R.E.; Carlson, E.R.; Eichstaedt, R.M.; Schimmele, S.R.; Strauss, J.E.; Georgeff, K.R. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 638–646. [Google Scholar] [CrossRef]
- Whitman, D.H.; Berry, R.L.; Green, D.M. Platelet gel: An autologous alternative to fibrin glue with applications in oral and maxillofacial surgery. J. Oral Maxillofac. Surg. 1997, 55, 1294–1299. [Google Scholar] [CrossRef]
- Anitua, E. Plasma rich in growth factors: Preliminary results of use in the preparation of future sites for implants. Int. J. Oral Maxillofac. Implant. 1999, 14, 529–535. [Google Scholar]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef] [PubMed]
- Tsay, R.C.; Vo, J.; Burke, A.; Eisig, S.B.; Lu, H.H.; Landesberg, R. Differential growth factor retention by platelet-rich plasma composites. J. Oral Maxillofac. Surg. 2005, 63, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Lau, J.; Ioannidis, J.P.A.; Schmid, C.H. Summing up evidence: One answer is not always enough. Lancet 1998, 351, 123–127. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Haynes, R.B.; Jaeschke, R.Z.; Cook, D.J.; Green, L.; Naylor, C.D.; Wilson, M.C.; Richardson, W.S. Users’ guides to the medical literature: XXV. Evidence-based medicine: Principles for applying the users’ guides to patient care. J. Am. Med. Assoc. 2000, 284, 1290–1296. [Google Scholar] [CrossRef]
- Evans, D. Hierarchy of evidence: A framework for ranking evidence evaluating healthcare interventions. J. Clin. Nurs. 2003, 12, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Jadad, A.R.; Nichol, G.; Penman, M.; Tugwell, P.; Walsh, S. Assessing the quality of randomized controlled trials: An annotated bibliography of scales and checklists. Control. Clin. Trials 1995, 16, 62–73. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Del Fabbro, M. Clinical performance of zirconia implants: A meta-review. J. Prosthet. Dent. 2020, 123, 419–426. [Google Scholar] [CrossRef]
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.M.; Kristjansson, E.; Grimshaw, J.; Henry, D.A.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 2009, 62, 1013–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swartz, M.K. The PRISMA statement: A guideline for systematic reviews and meta-analyses. J. Pediatr. Health Care 2011, 25, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; Hillier-Brown, F.C.; Moore, H.J.; Lake, A.A.; Araujo-Soares, V.; White, M.; Summerbell, C. Searching and synthesising “grey literature” and “grey information” in public health: Critical reflections on three case studies. Syst. Rev. 2016, 5, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rock, L. Potential of platelet rich fibrin in regenerative periodontal therapy: Literature review. Can. J. Dent. Hyg. 2013, 47, 33–37. [Google Scholar]
- Plachokova, A.S.; Nikolidakis, D.; Mulder, J.; Jansen, J.A.; Creugers, N.H.J. Effect of platelet-rich plasma on bone regeneration in dentistry: A systematic review. Clin. Oral Implant. Res. 2008, 19, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Zapata, M.J.; Martí-Carvajal, A.; Solà, I.; Bolibar, I.; Ángel Expósito, J.; Rodriguez, L.; García, J. Efficacy and safety of the use of autologous plasma rich in platelets for tissue regeneration: A systematic review. Transfusion 2009, 49, 44–56. [Google Scholar] [CrossRef]
- Roselló-Camps, À.; Monje, A.; Lin, G.H.; Khoshkam, V.; Chávez-Gatty, M.; Wang, H.L.; Gargallo-Albiol, J.; Hernandez-Alfaro, F. Platelet-rich plasma for periodontal regeneration in the treatment of intrabony defects: A meta-analysis on prospective clinical trials. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 562–574. [Google Scholar] [CrossRef]
- Verma, U.P.; Yadav, R.K.; Dixit, M.; Gupta, A. Platelet-rich fibrin: A paradigm in periodontal therapy-A systematic review. J. Int. Soc. Prev. Community Dent. 2017, 7, 227–233. [Google Scholar]
- Franchini, M.; Cruciani, M.; Mengoli, C.; Masiello, F.; Marano, G.; D’Aloja, E.; Dell’Aringa, C.; Pati, I.; Veropalumbo, E.; Pupella, S.; et al. The use of platelet-rich plasma in oral surgery: A systematic review and meta-analysis. Blood Transfus. 2019, 17, 357–367. [Google Scholar]
- Kotsovilis, S.; Markou, N.; Pepelassi, E.; Nikolidakis, D. The adjunctive use of platelet-rich plasma in the therapy of periodontal intraosseous defects: A systematic review. J. Periodontal Res. 2010, 45, 428–443. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Karanxha, L.; Panda, S.; Bucchi, C.; Nadathur Doraiswamy, J.; Sankari, M.; Ramamoorthi, S.; Varghese, S.; Taschieri, S. Autologous platelet concentrates for treating periodontal infrabony defects. Cochrane Database Syst. Rev. 2018, 2018, CD011423. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Bortolin, M.; Taschieri, S.; Weinstein, R. Is Platelet Concentrate Advantageous for the Surgical Treatment of Periodontal Diseases? A Systematic Review and Meta-Analysis. J. Periodontol. 2011, 82, 1100–1111. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Yuan, J.; Aisaiti, A.; Liu, Y.; Zhao, J. The effect of platelet-rich plasma on clinical outcomes of the surgical treatment of periodontal intrabony defects: A systematic review and meta-analysis. BMC Oral Health 2016, 16, 71. [Google Scholar] [CrossRef] [Green Version]
- Shah, M.; Deshpande, N.; Bharwani, A.; Nadig, P.; Doshi, V.; Dave, D. Effectiveness of autologous platelet-rich fibrin in the treatment of intra-bony defects: A systematic review and meta-analysis. J. Indian Soc. Periodontol. 2014, 18, 698–704. [Google Scholar]
- Najeeb, S.; Khurshid, Z.; Agwan, M.A.S.; Ansari, S.A.; Zafar, M.S.; Matinlinna, J.P. Regenerative Potential of Platelet Rich Fibrin (PRF) for Curing Intrabony Periodontal Defects: A Systematic Review of Clinical Studies. Tissue Eng. Regen. Med. 2017, 14, 735–742. [Google Scholar] [CrossRef]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: Intra-bony defects, furcation defects and periodontal plastic surgery. A systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 67–82. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef]
- Li, A.; Yang, H.; Zhang, J.; Chen, S.; Wang, H.; Gao, Y. Additive effectiveness of autologous platelet-rich fibrin in the treatment of intrabony defects: A PRISMA-compliant meta-analysis. Medicine 2019, 98, e14759. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Ceci, C.; Taschieri, S. Systematic review on the effect of platelet concentrates for the surgical treatment of periodontal defects. Dent. Cadmos 2013, 81, 138–145. [Google Scholar]
- Panda, S.; Doraiswamy, J.; Malaiappan, S.; Varghese, S.S.; Del Fabbro, M. Additive effect of autologous platelet concentrates in treatment of intrabony defects: A systematic review and meta-analysis. J. Investig. Clin. Dent. 2016, 7, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Sun, C.; Huang, S.; Wu, X.; Zhao, Y.; Pan, C.; Wang, H.; Liu, J.; Li, Q.; Kou, Y. Efficacy of Adjunctive Bioactive Materials in the Treatment of Periodontal Intrabony Defects: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2018, 2018, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Baghele, O.K.; Kathole, V.; Tuteja, A.K.; Giri, T. Actual quantitative attachment gain secondary to use of autologous platelet concentrates in the treatment of intrabony defects: A meta-analysis. J. Indian Soc. Periodontol. 2019, 23, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Saleem, M.; Pisani, F.; Zahid, F.M.; Georgakopoulos, I.; Pustina-Krasniqi, T.; Xhajanka, E.; Almasri, M. Adjunctive platelet-rich plasma (PRP) in infrabony regenerative treatment: A systematic review and RCT’s meta-analysis. Stem Cells Int. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ioannidis, J.P.A. The Mass Production of Redundant, Misleading, and Conflicted Systematic Reviews and Meta-analyses. Milbank Q. 2016, 94, 485–514. [Google Scholar] [CrossRef] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Phillips, A.N. Meta-analysis: Principles and procedures. BMJ 1997, 315, 1533–1537. [Google Scholar] [CrossRef] [Green Version]
- Hopewell, S.; McDonald, S.; Clarke, M.; Egger, M. Grey literature in meta-analyses of randomized trials of health care interventions. Cochrane Database Syst. Rev. 2007, 18, MR000010. [Google Scholar] [CrossRef]
- Song, F.; Parekh, S.; Hooper, L.; Loke, Y.K.; Ryder, J.; Sutton, A.J.; Hing, C.; Kwok, C.S.; Pang, C.; Harvey, I. Dissemination and publication of research findings: An updated review of related biases. Health Technol. Assess. (Rockv). 2010, 14, 1–193. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; 2011; Available online: http://handbook.cochrane.org (accessed on 16 September 2020).
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moja, L.P.; Telaro, E.; D’Amico, R.; Moschetti, I.; Coe, L.; Liberati, A. Assessment of methodological quality of primary studies by systematic reviews: Results of the metaquality study cross sectional study. Br. Med. J. 2005, 330, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camargo, P.M.; Lekovic, V.; Weinlaender, M.; Vasilic, N.; Madzarevic, M.; Kenney, E.B. A reentry study on the use of bovine porous bone mineral, GTR, and platelet-rich plasma in the regenerative treatment of intrabony defects in humans. Int. J. Periodontics Restor. Dent. 2005, 25, 49–59. [Google Scholar]
- Addy, M.; Newcombe, R.G. Statistical versus clinical significance in periodontal research and practice. Periodontology 2000 2005, 39, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, A.R.; Rao, N.S.; Agarwal, E.; Bajaj, P.; Kumari, M.; Naik, S.B. Comparative Evaluation of Autologous Platelet-Rich Fibrin and Platelet-Rich Plasma in the Treatment of 3-Wall Intrabony Defects in Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Periodontol. 2012, 83, 1499–1507. [Google Scholar] [CrossRef]
- Gamal, A.Y.; Abdel Ghaffar, K.A.; Alghezwy, O.A. Crevicular Fluid Growth Factors Release Profile Following the Use of Platelet-Rich Fibrin and Plasma Rich Growth Factors in Treating Periodontal Intrabony Defects: A Randomized Clinical Trial. J. Periodontol. 2016, 87, 654–662. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e45–e50. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e51–e55. [Google Scholar] [CrossRef]
- Ghanaati, S.; Booms, P.; Orlowska, A.; Kubesch, A.; Lorenz, J.; Rutkowski, J.; Les, C.; Sader, R.; Kirkpatrick, C.J.; Choukroun, J. Advanced platelet-rich fibrin: A new concept for cell- Based tissue engineering by means of inflammatory cells. J. Oral Implantol. 2014, 40, 679–689. [Google Scholar] [CrossRef]
- Madurantakam, P.; Yoganarasimha, S.; Hasan, F.K. Characterization of Leukocyte-platelet Rich Fibrin, A Novel Biomaterial. J. Vis. Exp. 2015, 103, e53221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choukroun, J.; Ghanaati, S. Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: The first introduction to the low speed centrifugation concept. Eur. J. Trauma Emerg. Surg. 2018, 44, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevins, M.; Kao, R.T.; McGuire, M.K.; McClain, P.K.; Hinrichs, J.E.; McAllister, B.S.; Reddy, M.S.; Nevins, M.L.; Genco, R.J.; Lynch, S.E.; et al. Platelet-Derived Growth Factor Promotes Periodontal Regeneration in Localized Osseous Defects: 36-Month Extension Results From a Randomized, Controlled, Double-Masked Clinical Trial. J. Periodontol. 2013, 84, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Lolato, A.; Panda, S.; Corbella, S.; Satpathy, A.; Das, A.C.; Kumar, M.; Taschieri, S. Methodological Quality Assessment of Systematic Reviews on Autologous Platelet Concentrates for the Treatment of Periodontal Defects. J. Evid. Based Dent. Pract. 2017, 17, 239–255. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Ferrari, D.; Herten, M.; Mihatovic, I.; Wieland, M.; Sager, M.; Becker, J. Effects of surface hydrophilicity and microtopography on early stages of soft and hard tissue integration at non-submerged titanium implants: An immunohistochemical study in dogs. J. Periodontol. 2007, 78, 2171–2184. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search String | No. of Items |
|---|---|---|
| PubMed | (((platelet OR plasma) AND (plasma OR derivative OR gel OR “growth factor” OR fibrin)) AND (periodontal OR periodontitis OR ((intrabony OR intraosseous) AND defect))) AND (“systematic review” OR “meta analysis”) | 61 |
| Embase | (‘platelet’/exp OR platelet OR ‘plasma’/exp OR plasma) AND (‘plasma’/exp OR plasma OR derivative OR ‘gel’/exp OR gel OR ‘growth factor’/exp OR ‘growth factor’ OR ‘fibrin’/exp OR fibrin) AND (periodontal OR ‘periodontitis’/exp OR periodontitis OR ((intrabony OR intraosseous) AND defect)) AND (‘systematic review’/exp OR ‘systematic review’ OR ‘meta analysis’/exp OR ‘meta analysis’) | 82 |
| CDSR | (((platelet OR plasma) AND (plasma OR derivative OR gel OR “growth factor” OR fibrin)) AND (periodontal OR periodontitis OR ((intrabony OR intraosseous) AND defect)) | 3 |
| Study | Reason of Exclusion |
|---|---|
| Franchini et al., 2019 [20] | Pooled together data on intraosseous and non-intraosseous defects |
| Verma et al., 2017 [19] | Pooled together data on intraosseous and non-intraosseous defects |
| Roselló-Camps et al., 2015 [18] | Pooled together data on intraosseous and non-intraosseous defects and data on platelet poor plasma |
| Plachokova et al., 2008 [16] | Pooled together data on intraosseous and non-intraosseous defects |
| Martínez-Zapata et al., 2009 [17] | Pooled together data on intraosseous and non-intraosseous defects |
| Rock et al., 2013 [15] | Not a systematic review |
| Authors and Year | Focused Question/Aim | Search Strategy | Search Period | Key Words | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|---|---|
| Kotsovilis at al. 2010 [21] | What is the efficacy, with respect to clinical, radiographical and patient-centred outcomes, of combinations of platelet-rich plasma (PRP) with other therapeutic bioactive agents/procedures, compared with the efficacy of the same agents/procedures without the adjunctive use of PRP in the therapy of periodontal intraosseous defects in patients with chronic periodontitis and without systemic diseases that could potentially influence the outcome of periodontal therapy? PICO question: no | Electronic search: MEDLINE/PubMed, CENTRAL Manual search and other sources: specialized journals, references of relevant articles, proceedings, position papers, theses, contact with the authors to acquire missing, unclear or unpublished data. Language restrictions: none Publication date restrictions: yes Reference to an established guidelines: no Protocol registration: no | From 11/1997 to 09/2008 | Key words provided: yes Repeatable search string: yes Specific search string for each database: no | Only randomized controlled trials (RCTs), either of a parallel group or of a split-mouth design; all patients included exhibit exclusively chronic periodontitis; all patients included, should have no systemic diseases; Presence of at least one experimental group, in which PRP was clinically applied as an adjunct to other therapeutic bioactive agents/procedures for the therapy of periodontal intraosseous defects; Presence of an appropriate non-PRP control group; Report of change in clinical attachment level between baseline and the end of follow-up period as the primary outcome variable and at least of change in probing pocket depth between baseline and the end of follow-up period as secondary outcome variable. Follow-up period of at least 6 months. | Mixed RCT design, including both parallel group and split-mouth design; use of historical control group; history of periodontal therapy within the preceding 12 month or less; periodontal intraosseous defect(s) extending into furcation area(s) or located around teeth presenting furcation involvement(s); patients receiving any medication reported to interfere with wound healing; patients with abnormal platelet counts; patients receiving antibiotics at the baseline of the RCT and/or during the previous 3 months or less; history of radiotherapy in the head and neck region of the patients; teeth presenting endodontic problems. |
| Del Fabbro et al., 2011 [23] | The aim of the present evidence-based systematic review is to determine whether the use of autologous platelet concentrates may affect the outcome of regenerative procedures for the treatment of periodontal defects and gingival recession. PICO question: no | Electronic search: MEDLINE/PubMed, CENTRAL. Manual search and other sources: specialized journals, references of relevant articles, contact with manufacturing companies for ongoing or unpublished studies. Clinical trials from public registers: no Grey literature: yes Language restrictions: none Publication date restrictions: none Reference to an established guidelines: no Protocol registration: no | Up to 09/2010 | Key words provided: yes Repeatable search string: no Specific search string for each database: no | RCTs assessing the efficacy of platelet concentrates for healing and regeneration of hard and soft tissues in patients undergoing surgical procedures for the treatment of periodontal defects and gingival recession. Studies with a test group using platelet concentrates compared to a control group in which platelet concentrates were not used. | All other types of study designs, like case series, case reports, retrospective studies, technical studies, animal studies, and reviews; studies investigating the effect of platelet concentrates in surgical procedures involving implant therapy, like the maxillary sinus augmentation procedure or articles reporting on any other oral surgical intervention like tooth extraction, inlay and onlay grafts for the treatment of jawbone defects, treatment of odontogenic cysts, and periapical surgery. |
| Del Fabbro et al., 2013 [30] | The aim of this review was to systematically evaluate the effects of autogenous platelet concentrates as an adjunct to the surgical treatment of periodontal defects. PICO question: no | Electronic search: MEDLINE/PubMed, CENTRAL. Manual search and other sources: specialized journals, references of relevant articles, contact with manufacturing companies for ongoing or unpublished studies. Language restrictions: none Publication date restrictions: none Reference to an established guidelines: no Protocol registration: no | Up to 04/2012 | Key words provided: yes Repeatable search string: no Specific search string for each database: no | RCTs and controlled clinical trials (CCTs) assessing the efficacy of platelet concentrates for healing and regeneration of hard and soft tissues in patients undergoing surgical procedures for the treatment of periodontal defects and gingival recession; no limitations regarding the number of patients treated; meta-analysis performed only if platelet concentrate was the only difference between test and control group. | All other types of study designs, like case series, case reports, retrospective studies, technical studies, animal studies, and reviews; Studies investigating the effect of platelet concentrates in surgical procedures involving implant therapy, like the maxillary sinus augmentation procedure or articles reporting on any other oral surgical intervention like tooth extraction, inlay and onlay grafts for the treatment of jawbone defects, treatment of odontogenic cysts, and periapical surgery. |
| Shah et al., 2014 [25] | The aim of the present evidence based systematic review and meta-analysis is to determine the clinical and radiographic outcomes of using platelet-rich fibrin (PRF) for the treatment of periodontal IBDs compared to open flap debridement (OFD). PICO question: no | Electronic search: MEDLINE/PubMed, EBSCO, CENTRAL. Manual search and other sources: none Language restrictions: English Publication date restrictions: yes Reference to established guidelines: no Protocol registration: no | From 01/2005 to 01/2013 | Key words provided: yes Repeatable search string: yes Specific search string for each database: no | Studies (randomized and non-randomized clinical trial ndr) investigating the effect of PRF in the treatment of periodontal intraosseous defects; test group using PRF alone; control group with OFD alone; no limitations regarding the number of patients treated; follow-up of minimum 6 months. | Study designs such as case series, case reports, retrospective studies, technical studies, animal studies and reviews. |
| Hou et al., 2016 [24] | The aim of our study was to evaluate the efficacy of PRP in the surgical treatment of periodontal intrabony defects by comparing clinical outcomes between patients who received PRP as an adjunct to periodontal intrabony defect therapy and those who did not. PICO question: no | Electronic search: MEDLINE/PubMed, EMBASE, ISI Web of Science, CENTRAL. Manual search and other sources: references of relevant articles Language restrictions: none Publication date restrictions: none Reference to established guidelines: PRISMA Protocol registration: no | Up to 06/2015 | Key words provided: yes Repeatable search string: yes Specific search string for each database: no | RCT in which an intervention group receiving PRP was compared with a control group not receiving PRP; patients included having no systemic illness or abnormal platelet counts that could affect the clinical outcome of periodontal therapy; follow-up period of at least 6 months. | Inadequate comparison of the results of PRP for the treatment of periodontal intrabony defects; PRP administered to both the intervention and control groups; use of a biologic material that would hamper meaningful comparisons; other article types, such as reviews, case reports, and animal studies. |
| Panda et al., 2016 [31] | What is the adjunctive effect of autologous platelet concentrates (APCs) over OFD in the treatment of periodontal intraosseous defects? PICO question: yes | Electronic search: MEDLINE/PubMed, EBSCO, CENTRAL. Manual search and other sources: specialized journals. Language restrictions: none Publication date restrictions: none Reference to established guidelines: no Protocol registration: no | Up to 06/2012 | Key words provided: yes Repeatable search string: no Specific search string for each database: no | Clinical trials, either of a parallel group or of a splitmouth design; presence of experimental group in which APCs were clinically applied; presence of an appropriate non-APC control group; patients included in the RCT should present with intrabony defects (clinical attachment level (CAL) ≥4 mm and pocket depth (PD) ≥3 mm); patients included in the RCT should have no systemic diseases; report of clinical attachment level at baseline and at the end of the follow-up period as the primary outcome variable and PD or radiographic defect depth at baseline and at the end of follow-up period as the secondary outcome variable; articles having follow-up period of at least 9 months | RCT design, including both parallel group and splitmouth design; periodontal intrabony defects extending into furcation areas of teeth; intrabony defects extending apically with endodontic involvements. |
| Najeeb et al., 2017 [26] | In patients with intrabony periodontal defects, what is the effect of using PRF-based grafts on the clinical and radiographic outcomes? PICO question: no | Electronic search: MEDLINE/PubMed, Google Scholar, ISI Web of Science Manual search and other sources: references of relevant articles Language restrictions: English Publication date restrictions: yes Reference to established guidelines: no Protocol registration: no | From 1949 to 01/2016 | Key words provided: yes Repeatable search string: no Specific search string for each database: no | Randomized control trials; restoration of bony periodontal defects; PRF as test intervention. | Letters to the editors, commentaries, animal studies, and in vitro studies |
| Castro et al., 2017 [27] | Does L-PRF promote periodontal wound healing in systemically healthy patients (ASA I) during periodontal surgery compared to traditional techniques? PICO question: yes | Electronic search: MEDLINE/PubMed, EMBASE, CENTRAL Manual search and other sources: references of relevant articles citation screening and expert recommendations Language restrictions: English Publication date restrictions: none Reference to established guidelines: PRISMA Protocol registration: no | Up to 07/2015 | Key words provided: yes Repeatable search string: no Specific search string for each database: yes | Randomised controlled clinical trials (RCTs) or controlled clinical trials (CCTs); studies regarding periodontal surgery: intrabony defects, furcation defects and periodontal plastic surgery; L-PRF prepared following the protocol 2700 rpm/12 min or 3000 rpm/10 min; studies conducted in humans; no limitation in follow-up duration; | Case reports, case series, retrospective studies, studies regarding bone augmentation procedures, ridge preservation or implant surgery, other types of platelet concentrates (fibrin glues, PRP, PRGF, A-PRF, I-PRF…), animal studies, in vitro studies other applications of L-PRF in Medicine (Traumatology, Ophthalmology, Dermatology, etc.) or in Dentistry (Endodontics,…) |
| Miron et al., 2017 [28] | What indications has platelet rich fibrin been shown effective for tissue repair/regeneration of either soft or hard tissues in dentistry? PICO question: yes | Electronic search: MEDLINE/PubMed, EMBASE, ISI Web of Science, SciVerse, CENTRAL Manual search and other sources: relevant journals, references of relevant articles Language restrictions: English Publication date restrictions: none Reference to established guidelines: no Protocol registration: no | Up to 05/2016 | Key words provided: yes Repeatable search string: yes Specific search string for each database: no | Human studies evaluating the comparative effects of PRF to an appropriate control or to another regenerative modality in human studies were included. | All human studies evaluating PRF in a case report or case series if controls were not present. All animal and in vitro studies. |
| Saleem et al., 2018 [34] | What are the vertical probing pocket depth reductions, the vertical clinical attachment level gains and the recession reduction at infra-bony defects at least 6 months after Regenerative Surgery with the adjunctive use of PRP as documented in RCTs, compared to the same clinical procedures and biomaterials performed without the use of PRP? PICO question: yes | Electronic search: MEDLINE/PubMed, EMBASE, LILACS, CENTRAL, Current Controlled Trials, ClinicalTrials.gov, World Health Organization International Trials Registry Platform, ISI Web of Knowledge (conference abstracts), Open Grey Manual search and other sources: relevant journals, references of relevant articles, contact with authors Language restrictions: English Publication date restrictions: none Reference to established guidelines: no Protocol registration: no | Up to 12/2016 | Key words provided: yes Repeatable search string: yes Specific search string for each database: no | Study population: Studies were limited to human subjects older than 18 years and in good general health, with a diagnosis of chronic periodontitis and with at least one pair of specular infrabony defects. Type of interventions: guided tissue regeneration (GTR) surgical procedures with and without PRP will be the interventions considered for the comparative evaluation. Type of comparison: Infrabony defects […] by the same regenerative therapy without PRP that were considered the control group. Outcome measures: (i) probing pocket depth reduction (PPDRed mm), (ii) clinical attachment level gain (CAL Gain mm), (iii) recession reduction (RECRed). These were evaluated as the mean difference (mm) from the time of surgery until the end of the evaluation period not before 6 months. Types of Studies: randomized controlled clinical trials (RCTs) only; | Cohort studies or case-control studies. Case series and case reports. Studies considering individuals with a history of aggressive periodontitis or conducted on animal models. |
| Zhou et al., 2018 [32] | The aim of the present systematic review and meta-analysis was to evaluate and compare the clinical outcomes of enamel matrix derivative (EMD), PRP, PRF, and AM in conjunction with demineralized freeze-dried bone allograft (DFDBA) in patients with periodontal intrabony defects, which might have some guiding significance on clinical management strategy for the option of additional bioactive materials. PICO question: no | Electronic search: MEDLINE/PubMed, EMBASE, CENTRAL Manual search and other sources: references of relevant articles Language restrictions: none Publication date restrictions: none Reference to established guidelines: no Protocol registration: no | Up to 12/2017 | Key words provided: yes Repeatable search string: yes Specific search string for each database: no | RCTs that compared the performances of DFDBA with or without one of the four bioactive materials (EMD, PRP, PRF, and AM) in patients with periodontal intrabony defects, with follow-up periods of ≥6 months. | Retrospective cohort studies, animal studies, in vitro studies, case reports, case series, and reviews. |
| Del Fabbro et al., 2018 [22] | To assess the effects of APCs used as an adjunct to periodontal surgical therapies OFD, OFD combined with BG, GTR, OFD combined with EMD) for the treatment of infrabony defects. PICO question: yes | Electronic search: MEDLINE/PubMed, EMBASE, LILACS, CENTRAL, ClinicalTrials.gov, World Health Organization International Trials Registry Platform, Grey Literature Report, Open Grey Manual search and other sources: relevant journals, references of relevant articles Language restrictions: none Publication date restrictions: none Reference to established guidelines: MECIR Protocol registration: Cochrane Database of Systematic Reviews, PROSPERO | Up to 02/2018 | Key words provided: yes Repeatable search string: yes Specific search string for each database: yes | RCTs of both parallel and split-mouth design, involving patients with infrabony defects requiring surgical treatment. Studies had to compare treatment outcomes of a specific surgical technique combined with APC, with the same technique when used alone. | NR |
| Li et al., 2019 [29] | The aim of this updated meta-analysis was to systematically evaluate the additive effectiveness of autologous PRF in the treatment of intrabony defects of chronic periodontitis patients when used along with OFD in terms of clinical and radiological outcomes. PICO question: no | Electronic search: MEDLINE/PubMed, EMBASE, CENTRAL, ISI Web of Knowledge Manual search and other sources: references of relevant articles, contact with authors Language restrictions: English Publication date restrictions: none Reference to established guidelines: PRISMA Protocol registration: no | Up to 11/2017 | Key words provided: yes Repeatable search string: no Specific search string for each database: yes | Trials had to be properly randomized; no additional agents or interventions confounded the comparison; contain patients with histologically proven intrabony defects of chronic periodontitis; patients included in the trials should have no systemic diseases that could potentially influence the outcome of periodontal therapy. | Studies only featuring comparisons of other types of chemotherapy regimens; early studies published as a series of articles from the same institution or author that contained significant overlapping data. |
| Baghele et al., 2019 [33] | The aim of the present meta-analysis is to evaluate actual quantitative mean gains of autologous platelet concentrates (PRF/PRP) in the treatment of intrabony defects in randomized controlled trials over and above that of OFD. The focused question for our meta-analysis is, “Whether there is any clinically significant advantage of using autologous platelet concentrates (PRF/PRP) along with OFD in intrabony defects, as represented by various clinical and radiographic periodontal parameters when compared to use of OFD alone?” PICO question: no | Electronic search: MEDLINE/PubMed, EMBASE, EBSCO, Google Scholar Manual search and other sources: relevant journals, references of relevant articles Language restrictions: English Publication date restrictions: none Reference to established guidelines: PRISMA Protocol registration: submission to PROSPERO (not verified) | Up to 05/2017 | Key words provided: yes Repeatable search string: no Specific search string for each database: no | Human randomized clinical trials, either of a parallel group or of a split-mouth design, reporting adequate and readable data from ≥10 subjects/osseous defects in the PRP or PRF group. A randomized controlled clinical trial where one of the groups received autologous PRF/PRP. The comparator group can be of any treatment modality but only OFD alone was considered for analyses. The patients included in the RCT had no systemic illness or abnormal platelet counts that could affect the clinical outcome of periodontal therapy Periodontal intrabony defects with radiographic IBD ≥3 mm with corresponding CAL ≥5 mm were included. All the defects irrespective of mentioned number of walls (1, 2 or 3 walled defects) were included. Studies determining at least one of these variables were included: the clinical attachment levels (CALs), the depth of intrabony defect, and the probing pocket depths (PPDs) at baseline and final follow-up of at least 6 months | Studies mentioning furcation invasions of teeth. Study designs such as case series, case reports, retrospective studies, in vitro studies, animal studies, reviews, and meta-analyses. |
| Authors and Year | Studies Included (Only Studies on Intrabony Defects Considered) | APCs Evaluated | Groups | Follow-Up Range (Months) | Meta-Analysis | Total Defects Test/Control | Overall SMD (95% CI) | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Kotsovilis et al., 2010 [21] | 10 RCTs | PRP (including PP) | PRP + graft PRP + ABBM vs. ABBM PRP + ABBM + EMD vs. ABBM + EMD PPR + BG vs. BG PRP + β-TCP vs. β-TCP PRP + DFDBA vs. DFDBA PRP + HA vs. HA PRP + GTR PRP + BM + ePTFE-GTR vs. BM + ePTFE-GTR PRP + BM + COL-GTR vs. BM + COL-GTR PRP+ β-TCP + ePTFE-GTR vs. β-TCP + ePTFE-GTR Other comparisons PP + PAM-GTR vs. BG + PAM-GTR | 6–12 | No | 184/183 | NA | General conclusions Most RCTs selected generally demonstrate appropriate methodology with regard to the majority of quality criteria. However, most of studies selected are lacking sample size calculation, and in certain RCTs randomization and allocation concealment methods are not clearly adequate. The selected RCTs differ in their design with regard to therapeutic bioactive agents/procedures combined with PRP for the therapy of periodontal intraosseous defects. The amount of data currently available for each combination of PRP with other therapeutic bioactive agents/procedures could be regarded as limited. Publication bias and its specific types, language bias and time-lag bias, might possibly lead to an overestimation of the efficacy of the adjunctive use of PRP. Specific conclusions The clinical use of PRP is an entirely safe procedure, causing no adverse events or postoperative complications. Diverse outcomes (positive and negative) have been reported for the efficacy of PRP combined with various therapeutic bioactive agents/procedures, reflecting the limited and heterogeneous data available and possibly suggesting that the specific selection of agents/procedures combined with PRP could be important. Implications for research and clinical practice Randomized controlled clinical trials should include an appropriate (concurrent with the experimental group) non-PRP control group and longer follow-up periods. Consensus on an appropriate methodology for PRP preparation seems to be required. A specific protocol for the clinical use of PRP cannot be recommended at present. |
| Del Fabbro et al., 2011 [23] | 10 RCTs | PRP | PRP + graft PRP + ABBM vs. ABBM (2) PRP + HA vs. HA PRP + BG vs. BG PRP +DFDBA vs. DFDBA PRP + ABBM + EMD vs. ABBM + EMD PRP + GTR PRP + ABBM + GTR vs. ABBM + GTR (2) PRP + β-TCP + GTR vs. β-TCP + GTR (2) Other comparisons (not meta-analysed): PRP+ABBM+GTR vs. GTR PRP + ABBM + GTR vs. none PRP + β-TCP + GTR vs. β-TCP PRP+GTR vs. GTR + BG and PRP + β-TCP vs. β-TCP PRP + ABBM + GTR vs. ABBM + GTR PRP + β-TCP vs. β-TCP | 6–12 | Yes | 307/295 | PRP + graft or GTR vs. graft or GTR CAL Gain (10): 0.50 mm (95% CI: 0.12–0.88 mm, p = 0.01) Sub-groups: GTR (4): 0.04 mm (95% CI: −0.33, 0.41 mm, p = 0.75) no-GTR (6): 0.84 mm (95% CI: 0.27, 1.42 mm, p = 0.004) P (7):0.39 mm (95% CI: −0.01, 0.79 mm) SM (3): 0.80 mm (95% CI: 0.10, 1.50 mm) | Platelet-rich plasma may be advantageously used as an adjunct to grafting procedures, but not in combination with GTR, for the treatment of intrabony defects |
| Del Fabbro et al., 2013 [30] | 18 RCTs | PRP PRF | APC alone PRF vs. OFD (3) PRP vs. OFD PRP + graft PRP + graft PRP + ABBM vs. ABBM (3) PRP + HA vs. HA PRP + BG vs. BG PRP + DFDBA vs. DFDBA PRP + ABBM + EMD vs. ABBM + EMD PRP + HA + β-TCP vs. HA + β-TCP PRP + β-TCP vs. β-TCP (2) PRP + GTR PRP + β-TCP + GTR vs. β-TCP + GTR (2) PRP + ABBM + GTR vs. ABBM + GTR (2) PRP + MTB + GTR vs. MTB + GTR Other comparisons (not meta-analysed): PRF + HA vs. OFD PRP + ABBM + GTR vs. GTR PRP + ABBM + GTR vs. none PRP + GTR vs. GTR + BG PRP + β-TCP + GTR vs. β-TCP PRP + β-TCP vs. β-TCP PRP + ABB + GTR vs. ABB + GTR PRP + β-TCP vs. β-TCP | 6–12 | Yes | 327/305 | PRP + graft or GTR vs. graft or GTR CAL gain (18): 0.67 mm (95%: 0.55, 0.78 mm), p < 0.001 Subgroups: P (11): 4.70% (95% CI: 0.97, 8.43%, p = 0.01) SM (7): 12.22% (95% CI:7.54, 16.90%, p < 0.001) GTR (5): 2.77% (95% CI: −2.23, 7.77%, p = 0.28) non-GTR (13): 9.17% (95% CI:5.39, 12.94%, p < 0.001) APC vs. OFD CAL gain (4): 4.96% (95% CI: −1.65, 11.58%, p = 0.14) | The use of APCs may exert a positive adjunctive effect for the treatment of intrabony defects when used in combination with graft materials, but not with GTR. No significant adjunctive benefit of APCs could be demonstrated for the treatment of gingival recession and furcation defects. A standardization of study design and clinical protocols is needed in future studies in order to gain more insight into the true effect of APCs in periodontal regeneration. |
| Shah et al., 2014 [25] | 5 RCTs | PRF | PRF alone PRF vs. OFD (5) Other comparisons not meta-analysed: PRP vs. OFD PRF vs. PRP PRF vs. PRF + HA PRF + HA vs. OFD | 9–12 | Yes | 103/102 | PRF vs. OFD CAL gain (5): 0.95 (95%: IC: 0.20–1.71, p < 0.001 *) PDred (5): 1.10 (95% CI: 0.56–1.64, p < 0.001 *) IBDred (5): 2.33 (95% CI: 1.43–3.23, p < 0.001 *) RECinc (5): −0.47 (−1.52–0.58, p > 0.05) * | This meta-analysis showed clinically significant improvements in the periodontal parameters like CAL gain, IBDred, PDred when intrabony defects were treated with PRF alone compared to OFD. As PRF is easy to obtain autologous material, effective and user friendly, can be more widely used in periodontal regeneration. |
| Hou et al., 2016 [24] | 12 RCTs | PRP | PRP + graft PRP + HA vs. HA PRP + ABBM vs. ABBM (3) PRP + BG vs. BG PRP + DFDBA DFDBA (2) PRP + β-TCP + HA vs. β-TCP + HA PRP + GTR PRP + β-TCP + GTR vs. β-TCP + GTR (2) PRP + ABBM + GTR vs. ABBM + GTR (2) Other comparisons (not meta-analyzed): PRP + HA vs. HA PRP + β-TCP vs. β-TCP (2) | 6–13 | Yes | 217/215 | PRP + graft or GTR vs. graft or GTR CAL gain (12): 0.76 mm (95% CI: 0.34, 1.18 mm, p = 0.0004) PDred (12): 0.53 mm (95% CI: 0.21, 0.85 mm, p = 0.001) Subgroups: GTR (4): 0.08 mm (95% CI: −0.30, 0.46 mm, p = 0.67) no-GTR (8): 1.22 mm, 95% CI: 0.88, 1.57 mm, p<0.00001) P (7): 0.45 mm (95% CI: −0.05, 0.94 mm, p = 0.08) SM(5): 1.20 mm (95% CI: 0.72, 1.69 mm, p < 0.00001) | The adjunctive use of PRP together with conventional grafting procedures may be a beneficial treatment approach. However, when combined with the use of a regenerative technique, such as GTR, the beneficial effect of PRP on the treatment of intrabony defects is negligible. |
| Panda et al., 2016 [31] | 15 RCTs | PC (PRP and PRF) | APC alone PRF vs. OFD (4) PRP vs. OFD (1) PRP + graft PRP + TMB vs. TMB PRP + β-TCP vs. β-TCP PRP + ABBM vs. ABBM (2) PRP +DFDBA vs. DFDBA PRP + BG vs. BG PRP + HA vs. HA PRP + GTR PRP + β-TCP + GTR vs. β-TCP + GTR (2) PRP + ABBM + GTR vs. ABBM + GTR (2) Other comparisons (not meta-analyzed): PRF + HA + OFD vs. OFD | 9–12 | Yes | NA | PRFvsOFD (4) CAL gain: 1.48 (95% CI: 1.16, 1.79), p = 0.003 * PRP + graft vs. graft (7) CAL gain: 2.00 (95% CI: 1.68, 2.32), p < 0.001 * PRP + GTR vs. GTR (4) CAL gain: 0.03 (95% CI: −0.32, 0.37), p = 0.74 * PRP vs. OFD (1) CAL gain: 0.10 (95% CI: −0.09; 0.29), p = 0.30 * | Based on the results obtained from the present systematic review it can be concluded that the evidence on the beneficial additive effect of APCs in surgical treatment of intrabony defects has been increasing in recent years. Platelet concentrates may be advantageously used as a cost-effective adjunct to surgical regenerative therapy, even in combination with bone grafts, although they did not show any advantage when used together with GTR. Moreover, platelet-rich fibrin proved to be effective as a sole regenerative material for treatment of intrabony defects, in combination with OFD. Further long-term, multicentre clinical trials are to be carried out to validate these treatment strategies in evidence-based clinical practice. |
| Najeeb et al., 2017 [26] | 13 RCTs | PRF | APC alone PRF vs. OFD (6) PRP vs. OFD APC + graft PRF + DFDBA vs. DFDBA (2) PRF + HA vs. HA PRF + ABBM vs. ABBM PRGF + ABBM vs. ABBM Other comparisons: PRF + ABBM vs. PRF PRF + DFDBA vs. PRF PRF vs. EMD PRF + MF vs. OFD MF vs. OFD ABG vs. OFD | 1–12 | No | NA | NA | The PRF when combined with OFD, produces better outcomes compared to the OFD alone. The regenerative potential of PRF results in better augmentation and regeneration of periodontal bone defects. In addition, PRF may augment the regenerative potential of bone grafts. However, more long-term and well-designed clinical trials are needed to ascertain the clinical efficacy of PRF and PRF containing bone grafts. |
| Castro et al., 2017 [27] | 13 RCTs | L-PRF | PRF alone PRF vs. OFD (6) Other comparisons (not meta-analyzed): PRP vs. OFD PRF vs. ABBM PRF vs. DFDBA (3) PRF vs. EMD PRF vs. HA Other comparisons: PRF vs. ABG | 6–12 | Yes | 129/129 | PRF vs. OFD CAL gain (6): 1.2 mm (95% CI: 0.5, 1.9, p < 0.001) PDred (6): 1.1 mm (95% CI: 0.6, 1.6, p < 0.001) BF (6): 1.7 mm (95% CI: 1.0, 2.3, p < 0.001) | Favourable effects on hard and soft tissue healing and postoperative discomfort reduction were often reported when PRF was used. Nevertheless, standardization of the protocol is needed to obtain an optimal effect of PRF in regenerative procedures. Correct handling of PRF as well as the use of enough clots/membranes per surgical site might be crucial to obtain benefits from this technique. This biomaterial can be taken into consideration due to its reported good biological effects, low costs and ease of preparation. |
| Miron et al., 2017 [28] | 10 RCTs | PRF | PRF alone PRF vs. OFD (6) PRF + graft PRF + HA vs. HA PRF + DFDBA vs. DFDBA PRF + MF vs. MF PRF + GTR PRF + GTR vs. GTR Other comparison: PRF vs. DFDBA | 6–12 | No | NA | NA | This systematic review demonstrates the widespread use of PRF in dentistry in various clinical settings. Although this regenerative modality remains unfamiliar to many clinicians, the evidence supporting its use has accumulated over the years, demonstrating its ability to improve tissue regeneration. The combination of PRF with regenerative therapy has been shown to be most promising for periodontal repair of intrabony […] defects […]. […] Nevertheless, its ease of use, combined with its low cost and autologous source, makes it an ideal biomaterial worth further investigation across a variety of surgical procedures in dentistry. |
| Saleem et al., 2018 [34] | 15 RCTs | PRP | PRP + graft PRP + ABG vs. ABG PRP + HA vs. HA PRP + HA + β-TCP vs. HA + β-TCP PRP + ABBM vs. ABBM (2) PRP + DFDBA vs. DFDBA PRP + GTR PRP + ABBM + GTR vs. ABBM + GTR (2) PRP + β-TCP + GTR vs. β-TCP + GTR PRP + ABBM + GTR vs. GTR PRP + EMD PRP + EMD + ABBM vs. EMD + ABBM (2) Other comparisons: PRP + ABBM + GTR vs. OFD Other comparisons (not meta-analyzed): PRP vs. OFD PRP + EMD + ABBM vs. EMD + ABBM PRP + β-TCP vs. β-TCP PRP + TMB vs. TMB | 6–60 | Yes | NA | NA | The adjunctive use of PRP in the regenerative treatment of infrabony defects can be considered as an affordable technique to get a better CAL gain and PDred in the surgical treatment of periodontal infrabony defects. Anyway, the limitations of the provided studies are the lack of baseline data regarding the defect size and their morphology, the absence of reports of other relevant clinical outcomes, as the bone fill, and the heterogeneity between studies. On the basis of this systematic review, the regeneration/ repair of infrabony defects would favour the use of adding PRP to a simple surgical repositioned flap technique, like in the OFD, with the use of bone grafts (xenografts, HA, or TCP). No better results would be achievable using combinations with biomodulators (Emdogain) or membranes, the PRP just would act as a biomodulator itself. In a biological sense, this observation would state for the biomolecular signalling action between PRP and the surrounding cellular environment that any membrane could interrupt or modify. The use of bone grafts would state as a blood clot stabilizer enhancing the osteoinductive properties of the PRP itself. Future Research/Observations According to the main reported pitfalls, future studies should be aimed first, designed according to RCT schemes in order to provide clinical evidences. A comparison between a surgical flap approach alone and the adjunctive use of PRP would be needful in order to explore the role of growth factors alone in periodontal regeneration and the healing process, as well as the radiographic bone level assessment before and after treatment, as they represent a critical parameter in success assessment. In order to explore which growth factor would be better suited in periodontal procedures, a multiple-arm RCT would be needful comparing PRP with other blood-derived agents available as well as with the different techniques adopted to deliver it. |
| Zhou et al., 2018 [32] | 9 RCTs | PRP, PRF | APC + graft PRP + DFDBA vs. DFDBA (4) PRF + DFDBA vs. DFDBA (2) Other comparisons: EMD + DFDBA vs. DFDBA AM + DFDBA vs. DFDBA | 6–12 | Yes | PRP+DFDBA vs. DFDBA (76/76) PRF+DFDBA vs. DFDBA (40/40) | Subgroups: PRP+DFDBA vs. DFDBA PDred (4): 0.47 95% CI: 0.14, 0.80, SS (p-value NA) CAL gain (4): 0.80 95% CI: 0.27, 1.32, SS (p-value NA) RECred (4): 0.45 95% CI: −0.18, 1.09, NSS (p-value NA) BF (4): 0.71 95% CI: 0.13, 1.29, SS (p-value NA) BR (3): −0.13 95% CI: −0.48, 0.21, NSS (p-value NA) PRF+DFDBA vs. DFDBA PDred (2): 0.88 95% CI: 0.41, 1.34, SS (p-value NA) CAL gain (2): 1.61 95% CI: 1.10, 2.12, SS (p-value NA) RECred (2): 0.77 95% CI: 0.31, 1.22, SS (p-value NA) BF: (2): 0.89 95% CI: −0.46, 2.24, NSS (p-value NA) BR (2): −0.18 95% CI: −0.62, 0.26, NS (p-value NA) | Within the limitation of this analysis, it is indicated that PRF exerts the most significant adjunctive effect on soft tissue healing, while PRP exhibits a unique impact on hard tissue reconstruction in the treatment of periodontal intrabony defect. […] Therefore, it seems reasonable to suggest that the autologous PRF/PRP could be taken as a preferred adjunct to promote periodontal regeneration due to its proven good biological effects, low costs, and ease of preparation. Nevertheless, standardization of the protocol for the preparation and application of PRF/PRP is needed to obtain an optimal effect in regenerative procedures. |
| Del Fabbro et al., 2018 [22] | 38 RCTs | PRP PRGF PRF | APC alone APC vs. OFD (12) APC + graft APC + graft vs. graft (17) APC + GTR APC+GTR vs. GTR (7) APC + EMD APC + EMD vs. EMD (2) | 3–12 | Yes | APC + OFD vs. OFD (255/255) APC + OFD + graft vs. OFD + graft (284/284) APC + GTR vs. GTR (124/124) APC + EMD vs. EMD (38/37) | APC vs. OFD (F-U 9–12 m): Pdred(12): 1.29 mm (95% CI: 1.00 1.58 mm; p < 0.00001 P(7): 0.99, 95%CI0.90 to 1.07; p < 0.00001 SM(5): 1.86, 95% CI 1.07 to 2.66; p < 0.00001 CAL gain (12): 1.47 mm, 95% CI 1.11 to 1.82 mm; p < 0.00001 P(7): 0.99, 95%CI0.84 to 1.14; p < 0.00001 SM (5): 2.36,95% CI 1.19 to 3.54; p = 0.00008 BF (9): 34.26%, 95% CI 30.07% to 38.46%; p < 0.00001 P (7): 35.77%, 95% CI 31.20% to 40.35%; p < 0.00001 SM (2): 27.32%, 95% CI 20.92% to 33.72%; p < 0.00001 APC + graft vs. graft APC + graft vs. graft (all F-U): PDred (17): 0.54 mm,95% CI 0.33 to 0.75 mm; p < 0.00001; P (5): 0.81, 95% CI 0.58 to 1.03; p < 0.00001 SM (12): 0.47, 95% CI 0.24 to 0.71; p = 0.000099 CAL gain (17): 0.72 mm, 95% CI 0.43 to 1.00 mm; p < 0.00001 P (5): 0.89, 95% CI 0.49 to 1.29; p = 0.000012 SM (12): 0.67, 95% CI 0.35 to 0.99; p = 0.000047 BF (11): 8.10% 95% CI 5.26 to 10.97; p < 0.00001 P (3): 9.66%,95% CI 5.39% to 13.94%; p < 0.00001 SM (8): 7.73%, 95% CI 4.50% to 10.97%; p < 0.00001 APC + graft vs. graft (F-U 3–6 m): PDred (11): 0.62, 95% CI 0.30 to 0.94; p = 0.00015 P (1): 0.84, 95% CI 0.60 to 1.07; p < 0.00001 SM (10): 0.58, 95% CI 0.25 to 0.92; p = 0.00067; CAL gain (11): 0.47, 95% CI 0.11 to 0.84; p = 0.012 P (1): 1.00, 95% CI 0.93 to 1.07; p < 0.00001 SM (10): 0.40, 95% CI 0.02 to 0.77; p = 0.039; BF (6): 4.76%, 95% CI 1.27% to 8.25%; p = 0.0076 P (1): 10.00%, 95% CI4.90% to15.10%; p = 0.00012 SM (5): 3.59%, 95% CI 0.13% to 7.05%; p = 0.042 APC + graft vs. graft (F-U 9–12 m): PDred (10): 0.50, 95% CI 0.31 to 0.69; p < 0.00001 P (4): 0.58, 95% CI 0.09 to 1.06; p = 0.020 SM (6): 0.49, 95% CI 0.26 to 0.72; p = 0.000039 CAL gain (6): SM 0.84, 95% CI 0.62 to 1.06; p < 0.00001 BF (6): 9.99%, 95% CI 6.44% to 13.55%; p < 0.00001 P (2): 8.87%, 95% CI 1.03% to 16.71%; p = 0.027 SM (4): 10.16%, 95% CI 6.18% to 14.14%; p < 0.00001 APC + GTR vs. GTR APC + GTR vs. GTR (all F-U): PDred (7): 0.92, 95% CI −0.02 to 1.86; p = 0.054 P (3): 0.25, 95% CI −0.15 to 0.64; p = 0.22 SM (4): 1.52, 95% CI 0.54 to 2.51; p = 0.0024 CAL gain (7): 0.42, 95% CI −0.02 to 0.86; p = 0.060 P (3): 0.09, 95% CI −0.32 to 0.50; p = 0.66 SM (4): 0.67, 95% CI 0.20 to 1.14; p = 0.0048 APC + GTR vs. GTR (F-U 3–6 m): PDred (3): SM: 1.07 (95% CI −0.71 to 2.86) p = 0.24 CAL gain (3): SM: 0.54, 95% CI 0.18 to 0.89; p = 0.0031 APC + GTR vs. GTR (F-U 9–12 m): PDred (5): 0.68, 95% CI −0.66 to 2.02; p = 0.32 P (3): 0.25, 95% CI −0.15 to 0.64; p = 0.22 SM (2): 1.53, 95% CI −0.85 to 3.91; p = 0.21 CAL gain (5): 0.27, 95% CI −0.39 to 0.93; p = 0.42 P (3): 0.09, 95% CI −0.32 to 0.50; p = 0.66 SM (2): 0.51, 95% CI −0.72 to 1.73; p = 0.42 APC + EMD vs. EMD: PDred (2): 1.13, 95% CI −0.05 to 0.30; p = 0.16 P (1): −0.10, 95% CI −1.32 to 1.12; p = 0.87 SM (1): 0.13, 95% CI −0.05 to 0.31; p = 0.15 CAL gain (2): 0.10,95% CI −0.13 to 0.32; p = 0.40 P (1): −0.20, 95% CI −1.06 to 0.66; p = 0.65 SM (1): 0.12, 95% CI −0.12 to 0.36; p = 0.32 BF (1): −0.60%, 95% CI −6.21% to 5.01%; p = 0.83 | There is very low-quality evidence that the adjunct of APC to OFD or OFD + graft when treating infrabony defects may improve probing pocket depth, clinical attachment level, and radiographic bone defect filling. For GTR or EMD, insufficient evidence of an advantage in using APC was observed. |
| Li et al., 2019 [29] | 12 RCTs | PRF | PRF alone PRF vs. OFD (12) Other comparisons (not meta-analyzed): PRP vs. OFD T-PRF vs. OFD Other comparisons: MF vs. OFD PRF + MF vs. OFD PRF + ATV vs. OFD PRF + RSV vs. OFD | 9–12 | Yes | 287/287 | PRF vs. OFD CAL gain (12): 1.29; 95% CI 0.–1.61; p< 0.00001 PDred (12): 1.01; 95% CI 0.95– 1.08; p< 0.00001 RECinc (8): 0.45; 95% CI 0.31–0.58; p< 0.00001 IBDred (8): 1.73; 95% CI 1.38–2.08; p < 0.00001 BF (8): 36.47; 95% CI 31.85–41.08; p< 0.00001 | Adjunctive use of PRF with OFD significantly improves fill defects when compared to OFD alone. However, additional powered studies with much larger sample sizes are needed to obtain a more concrete conclusion. Although the interpretation of the study results was limited, we believe that to a certain extent, our analyses may provide valuable information for physicians who need to decide the best treatment strategy among all possible regimens for patients with intrabony defects. |
| Baghele et al., 2019 [33] | 25 RCTs | PRP PRF | APC alone PRF vs. OFD (13) PRP vs. OFD (3) Other comparisons (not meta-analyzed): T-PRF vs. OFD PRF + HA vs. OFD PRF + MF vs. OFD PRF + ABBM vs. OFD PRF + RSV vs. OFD PRF + ATV vs. OFD PRP + DFDBA vs. OFD PRP + DFDBA vs. PRP (2) PRP + ABBM/P-15 vs. PRP PRF + ABBM vs. PRF PRF + EMD vs. PRF PRF vs. ABG (2) PRF vs. PRP PRF vs. DFDBA MF vs. OFD | 6–18 | Yes | 504/501 | APC vs. OFD CAL gain (16): 0.39 (95% CI, 0.35, 0.43, p < 0.00001) Pdred (16): 0.68 (95% CI, 0.63, 0.73, p < 0.00001) IBDred (13): 1.65 (95% CI, 1.57, 1.73, p < 0.00001) RECinc (13): 0.24 (95% CI, 0.22, 0.26, p < 0.00001) | Considering all the limitations, we conclude that, use of platelet concentrates (PRF/PRP) as sole grafting agents in periodontal intrabony defects does have an identifiable superiority over not using them during access flap surgeries in terms of only intrabony defect fill. The superiority in terms of clinical parameters (CAL gain, PDred, and RECinc) is negligible. Therefore, use of PRP/PRF can be recommended, with some reservations, as sole grafting material considering its potential for bone fill irrespective of negligible CAL gain and PDred. Considering overall moderate effect sizes in favor of PRP/PRF even for BF, the recommendation should be taken with caution. We did not find any outcome to recommend positively use of PRF/ PRP technologies for treating periodontal intrabony defects if your aim is CAL gain and PDred. There is a need to identify biological cascades and other related factors which are responsible for a wide range of almost negative to highly superior results among analyzed studies. A dedicated large sample size RCT should be carried out to substantiate the findings of this meta-analysis. |
| Comparison | Systematic Reviews | Studies Included | Defects (Test/Control) | Effect Size: SMD (95% CI) | Statistical Significance | p-Value |
|---|---|---|---|---|---|---|
| PRP vs. OFD | Panda et al., 2016 [31] | 1 | 18/18 * | 0.10 (95% CI: −0.09; 0.29) * | No | 0.30 * |
| PRF vs. OFD | Shah et al., 2014 [25] | 5 | 103/102 | 0.95 (95% CI: 0.20, 1.71) | Yes | <0.001 * |
| Panda et al., 2016 [31] | 4 | 81/80 * | 1.48 (95% CI: 1.16, 1.79) | Yes | 0.003 * | |
| Castro et al., 2017 [27] | 6 | 129/129 | 1.20 (95% CI: 0.5, 1.9) | Yes | <0.001 | |
| Li et al., 2019 [29] | 12 | 287/287 | 1.29 (95% CI: 0.96–1.61) | Yes | 0.00001 | |
| PRP + graft vs. graft | Del Fabbro et al., 2011 [23] | 6 | 113/115 | 0.84 (95% CI: 0.27, 1.42) | Yes | 0.004 |
| Panda et al., 2016 [31] | 7 | 141/140 * | 2.00 (95% CI: 1.68, 2.32) | Yes | <0.001 * | |
| Zhou et al., 2018 [32] | 4 ** | 76/76 | 0.80 (95% CI: 0.27, 1.32 | Yes | NA | |
| Hou et al., 2016 [24] | 8 | 151/149 | 1.22 (95% CI: 0.88, 1.57) | Yes | <0.00001 | |
| PRP + GTR vs. GTR | Del Fabbro et al., 2011 [23] | 4 | 66/66 | 0.04 (95% CI: −0.33, 0.41) | No | 0.75 |
| Panda et al., 2016 [31] | 4 | 66/66 * | 0.03 (95% CI: −0.32, 0.37) | No | 0.74 * | |
| Hou et al., 2016 [24] | 4 | 66/66 | 0.08 (95% CI: −0.30, 0.46) | No | 0.67 | |
| PRF + graft vs. graft | Zhou et al., 2018 * [32] | 2 | 40/40 | 1.61 (95% CI: 1.10, 2.12) | Yes | NA |
| APC vs. OFD | Del Fabbro et al., 2018 [22] | 12 | 255/255 | 1.47 (95% CI 1.11 to 1.82) | Yes | <0.00001 |
| Baghele et al., 2019 [33] | 16 | 504/501 | 0.39 (95% CI, 0.35, 0.43) | Yes | <0.00001 | |
| APC + graft vs. graft | Del Fabbro et al., 2018 [22] | 12 | 284/284 | 0.72 (95% CI 0.43 to 1.00) | Yes | <0.00001 |
| APC + GTR vs. GTR | Del Fabbro et al., 2018 [22] | 7 | 124/124 | 0.42 (95% CI −0.02, 0.86) | No | 0.060 |
| APC + EMD vs. EMD | Del Fabbro et al., 2018 [22] | 2 | 38/37 | 0.10 (95% CI−0.13, 0.32) | No | 0.40 |
| Authors and Year | ‘A Priori’ Design Provided? | Duplicate Study Selection and Data Extraction? | Comprehensive Literature Search? | Status of Publication (i.e., Grey Literature) as an Inclusion Criterion? | List of Studies (Included and Excluded)? | Characteristics of the Included Studies? | Quality of Included Studies Assessed and Documented? | Scientific Quality Used Appropriately in Formulating Conclusions? | Appropriate Methods Used to Combine the Findings of Studies? | Likelihood of Publication Bias Assessed? | Conflict of Interest Stated? | AMSTAR Score Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kotsovilis et al., 2010 [21] | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | NA | NA | 2 | 17 |
| Del Fabbro et al., 2011 [23] | N | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 2 | N | 14 |
| Del Fabbro et al., 2013 [30] | N | 2 | 2 | 2 | 2 | 1 | 1 | 2 | N | 1 | N | 13 |
| Shah et al., 2014 [25] | N | 2 | 1 | 1 | N | 2 | 2 | 1 | 1 | N | N | 10 |
| Hou et al., 2016 [24] | N | 2 | N | 1 | 2 | 1 | 1 | 1 | 2 | 2 | N | 12 |
| Panda et al., 2016 [31] | 1 | 2 | 2 | N | 2 | 1 | 2 | 2 | 1 | 2 | N | 15 |
| Castro et al., 2017 [27] | 1 | 2 | 2 | N | 2 | 2 | 2 | 1 | 2 | N | N | 14 |
| Miron et al., 2017 [28] | 1 | 2 | 2 | N | N | 1 | N | N | NA | NA | N | 6 |
| Najeeb et al., 2017 [26] | 1 | 1 | N | N | N | 1 | 2 | 2 | NA | NA | N | 7 |
| Del Fabbro et al., 2018 [22] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 |
| Saleem et al., 2018 [34] | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | N | 16 |
| Zhou et al., 2018 [32] | N | 2 | N | N | N | 1 | 2 | 1 | 2 | 2 | N | 10 |
| Baghele et al., 2019 [33] | 1 | N | 2 | 1 | N | 1 | 2 | 1 | 1 | 2 | N | 11 |
| Li et al., 2019 [29] | N | 2 | N | 1 | N | 2 | 2 | 1 | 2 | N | N | 10 |
| AMSTAR score | 9 | 25 | 19 | 14 | 16 | 19 | 22 | 19 | 16 | 14 | 4 | 12.6 (4.2) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guida, A.; Cecoro, G.; Rullo, R.; Laino, L.; Del Fabbro, M.; Annunziata, M. A Systematic Critical Appraisal of the Methodological Quality of Systematic Reviews on the Effect of Autologous Platelet Concentrates in the Treatment of Periodontal Intraosseous Defects. Materials 2020, 13, 4180. https://doi.org/10.3390/ma13184180
Guida A, Cecoro G, Rullo R, Laino L, Del Fabbro M, Annunziata M. A Systematic Critical Appraisal of the Methodological Quality of Systematic Reviews on the Effect of Autologous Platelet Concentrates in the Treatment of Periodontal Intraosseous Defects. Materials. 2020; 13(18):4180. https://doi.org/10.3390/ma13184180
Chicago/Turabian StyleGuida, Agostino, Gennaro Cecoro, Rosario Rullo, Luigi Laino, Massimo Del Fabbro, and Marco Annunziata. 2020. "A Systematic Critical Appraisal of the Methodological Quality of Systematic Reviews on the Effect of Autologous Platelet Concentrates in the Treatment of Periodontal Intraosseous Defects" Materials 13, no. 18: 4180. https://doi.org/10.3390/ma13184180