Rapid Prototyping of Personalized Articular Orthoses by Lamination of Composite Fibers upon 3D-Printed Molds

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design Methods, and Open-Source and Proprietary Software
2.1.1. Three-Dimensional and Personalized Ankle Digitalization
2.1.2. Computer-Aided Design of Personalized Splints and Related Molds
2.2. Manufacturing Procedures and Materials
2.2.1. Proof-of-Concept Personalized Ankle Immobilizing, Supporting or Protecting Splints
2.2.2. Rapid 3D-Printed Molds for Lamination and Autoclave Curing of Composite Fibers
2.2.3. Lamination and Curing of FRPs toward Final Articular Splints
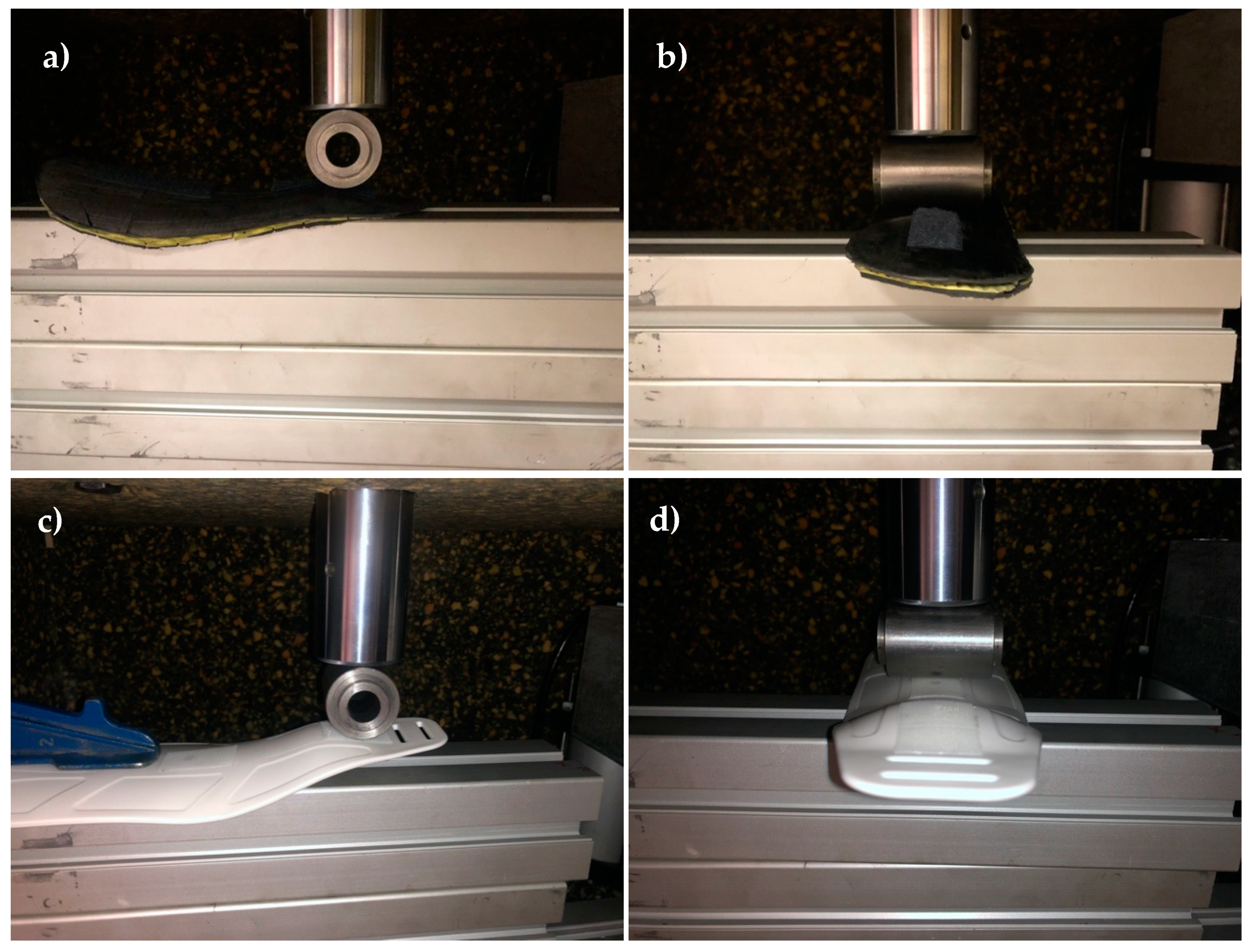
2.3. Mechanical Testing and Comparative Study
3. Results
3.1. Main Results
3.2. Discussion
4. Current Challenges and Future Proposals
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ahluwalia, A.; De Maria, C.; Díaz Lantada, A. The Kahawa Declaration: A manifesto for the democratization of medical technology. Glob. Health Innov. 2018, 1, 1–4. [Google Scholar] [CrossRef]
- Pauli, G. The Blue Economy: 10 Years, 100 Innovations, 100 Million Jobs; Paradigm Publications: New Mexico, NM, USA, 2010. [Google Scholar]
- Scholz, M.-S.; Blanchfield, J.P.; Bloom, L.D.; Coburn, B.; Elkington, M.; Fuller, J.; Gilbert, M.E.; Muflahi, S.; Pernice, M.F.; Rae, S.; et al. The use of composite materials in modern orthopaedic medicine and prosthetic devices: A review. Compos. Sci. Technol. 2011, 71, 1791–1803. [Google Scholar] [CrossRef]
- Rajak, D.K.; Pagar, D.D.; Menezes, P.L.; Linul, E. Fiber-Reinforced Polymer Composites: Manufacturing, Properties, and Applications. Polymers 2019, 11, 1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blok, L.G.; Longana, M.L.; Yu, H.; Woods, B.K.S. An investigation into 3D printing of fibre reinforced thermoplastic composites. Addit. Manuf. 2018, 22, 176–186. [Google Scholar] [CrossRef]
- Xiao, H.; Han, W.; Ming, Y.; Ding, Z.; Duan, Y. A sensitivity analysis-based parameter optimization framework for 3D printing of continuous carbon fiber/epoxy composites. Materials 2019, 12, 3961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhou, Z.; Zhang, F.; Tan, Y.; Tu, Y.; Yang, B. Performance of 3D-printed continuous-carbon-fiber-reinforced plastics with pressure. Materials 2020, 13, 471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, H.; Tan, Y.; Zhang, F.; Zhang, J.; Tu, Y.; Cui, K. Selectively enhanced 3D printing process and performance analysis of continuous carbon fiber composite material. Materials 2019, 12, 3529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Liu, W.; Qiu, Y.; Wei, Y. A one-component, fast-cure, and economical epoxy resin system suitable for liquid molding of automotive composite parts. Materials 2018, 11, 685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Z.; Xiao, J.; Tao, L.; Wei, Y.; Wang, S.; Zhang, H.; Zhu, S.; Yu, M. Preparation of high-performance carbon fiber-reinforced epoxy composites by compression resin transfer molding. Materials 2019, 12, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández Zapico, G.; Ohtake, N.; Akasaka, H.; Munoz-Guijosa, J.M. Epoxy toughening through high pressure and shear rate preprocessing. Sci. Rep. 2019, 9, 17343. [Google Scholar] [CrossRef] [PubMed]
- Wikipedia. Kinect. Available online: https://en.wikipedia.org/wiki/Kinect (accessed on 1 February 2020).
- Skanect. 3D Scaning: Fast, Easy and Low Cost. Available online: https://skanect.occipital.com/ (accessed on 1 February 2020).
- González-Ortega, D.; Díaz-Pernas, F.J.; Martínez-Zarzuela, M.; Antón-Rodríguez, M. A Kinect-based system for cognitive rehabilitation exercises monitoring. Comput. Methods Programs Biomed. 2014, 113, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Rogati, G.; Leardini, A.; Ortolani, M.; Caravaggi, P. Validation of a novel Kinect-based device for 3D scanning of the foot plantar surface in weight-bearing. J. Foot Ankle Res. 2019, 12, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahluwalia, A.; De Maria, C.; Madete, J.; Díaz Lantada, A.; Makobore, P.N.; Ravizza, A.; Di Pietro, L.; Mridha, M.; Munoz-Guijosa, J.M.; Chacón Tanarro, E.; et al. Biomedical Engineering Project Based Learning: Euro-African Design School Focused on Medical Devices. Int. J. Eng. Educ. 2018, 34, 1709–1722. [Google Scholar]
- Folgado, R.; Peças, P.; Henriques, E. Life cycle cost for technology selection: A case study in the manufacturing of injection moulds. Int. J. Prod. Econ. 2010, 128, 368–378. [Google Scholar] [CrossRef]
- Stratasys. FDM for composite tooling. In Design Guide; Direct industry: Marseille, France, 2016; pp. 1–65. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mold Type | Manufacturing Time (h) | Cost (€) | Roughness (μm) | Molding Cycles |
|---|---|---|---|---|
| Machined aluminum | ~20–30 | ~1500 | 0.4 | >30,000 * |
| 3D-printed ABS coated with epoxy | 45.5 | 47.36 | 0.5 | >5 |
| Polished ABS after 3D printing | 41 | 40.58 | 3.6 | 1–2 |
| Splint | Material | Joint | Number of Layers | Thickness (mm) | Weight (g) |
|---|---|---|---|---|---|
| Customized 1 | T700 epoxy prepreg, 300 g/m2 | Ankle | 7 | 2.1 | 53.5 |
| Customized 2 | T700 epoxy prepreg, 300 g/m2 | Ankle | 4 | 1.2 | 24.0 |
| Commercial | Thermoplastic polymer | Ankle | – | 2.5 | 54.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munoz-Guijosa, J.M.; Zapata Martínez, R.; Martínez Cendrero, A.; Díaz Lantada, A. Rapid Prototyping of Personalized Articular Orthoses by Lamination of Composite Fibers upon 3D-Printed Molds. Materials 2020, 13, 939. https://doi.org/10.3390/ma13040939
Munoz-Guijosa JM, Zapata Martínez R, Martínez Cendrero A, Díaz Lantada A. Rapid Prototyping of Personalized Articular Orthoses by Lamination of Composite Fibers upon 3D-Printed Molds. Materials. 2020; 13(4):939. https://doi.org/10.3390/ma13040939
Chicago/Turabian StyleMunoz-Guijosa, Juan Manuel, Rodrigo Zapata Martínez, Adrián Martínez Cendrero, and Andrés Díaz Lantada. 2020. "Rapid Prototyping of Personalized Articular Orthoses by Lamination of Composite Fibers upon 3D-Printed Molds" Materials 13, no. 4: 939. https://doi.org/10.3390/ma13040939