Acetic and Acrylic Acid Molecular Imprinted Model Silicone Hydrogel Materials for Ciprofloxacin-HCl Delivery


Abstract
:1. Introduction
2. Results and Discussion
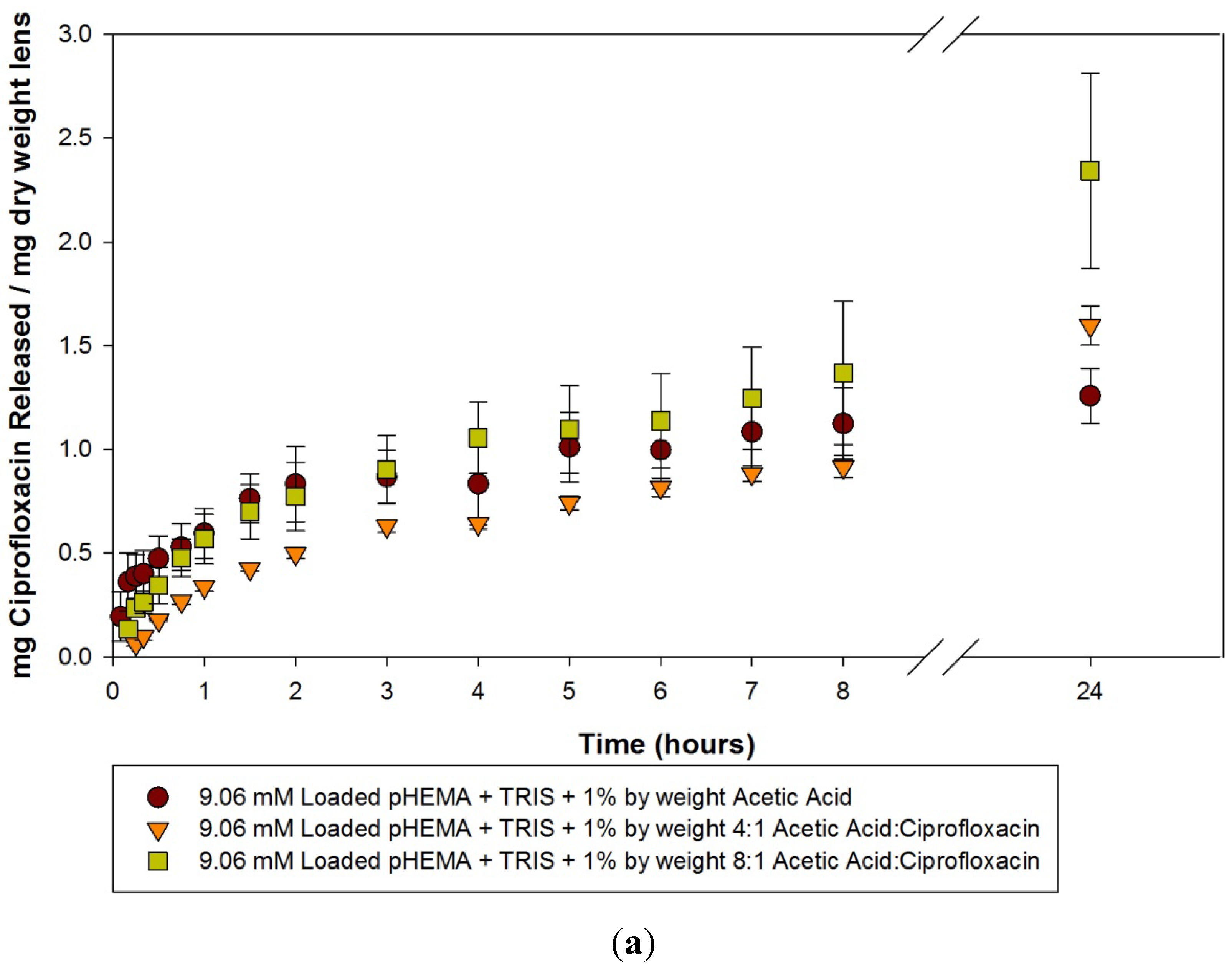
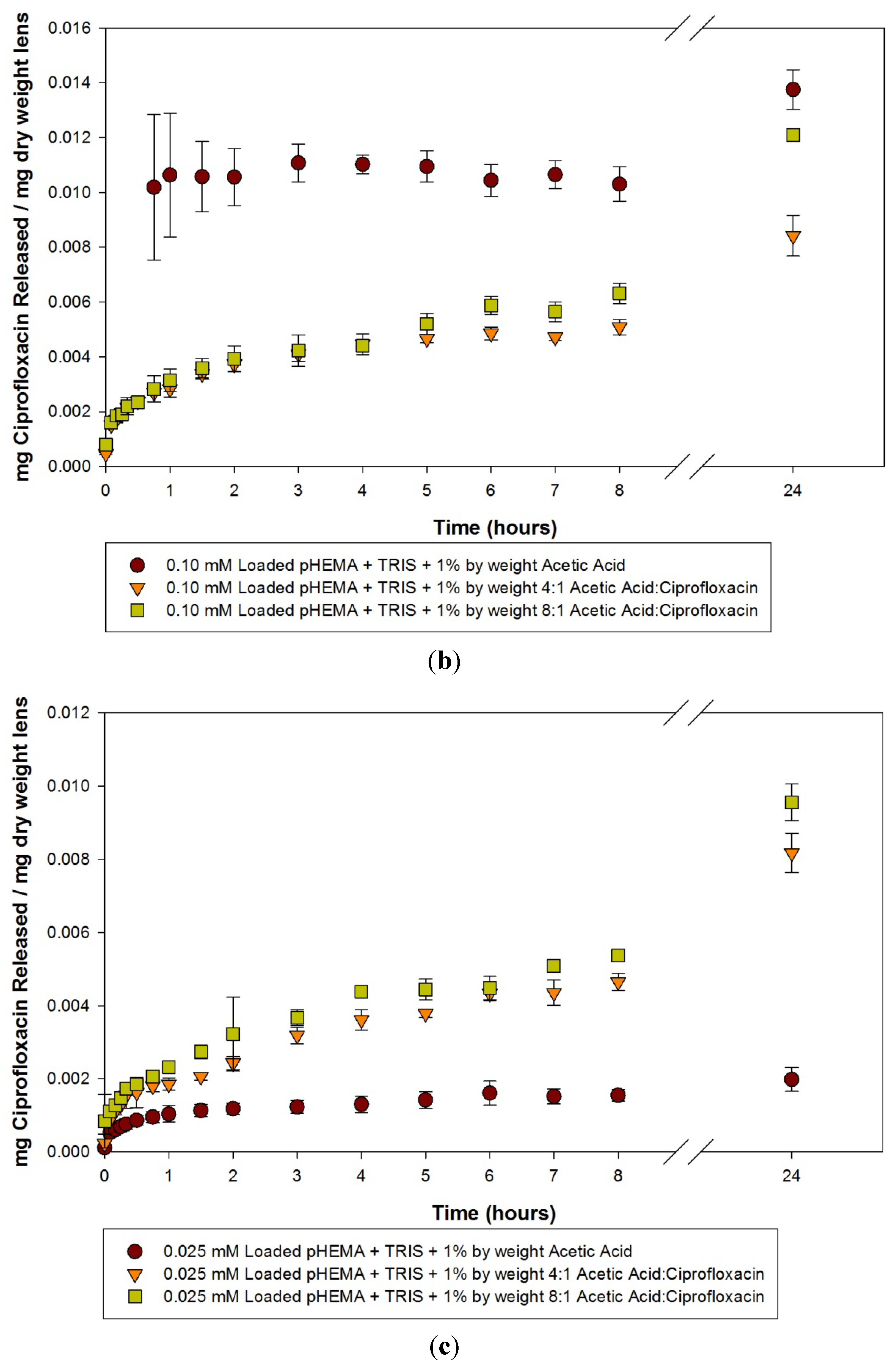
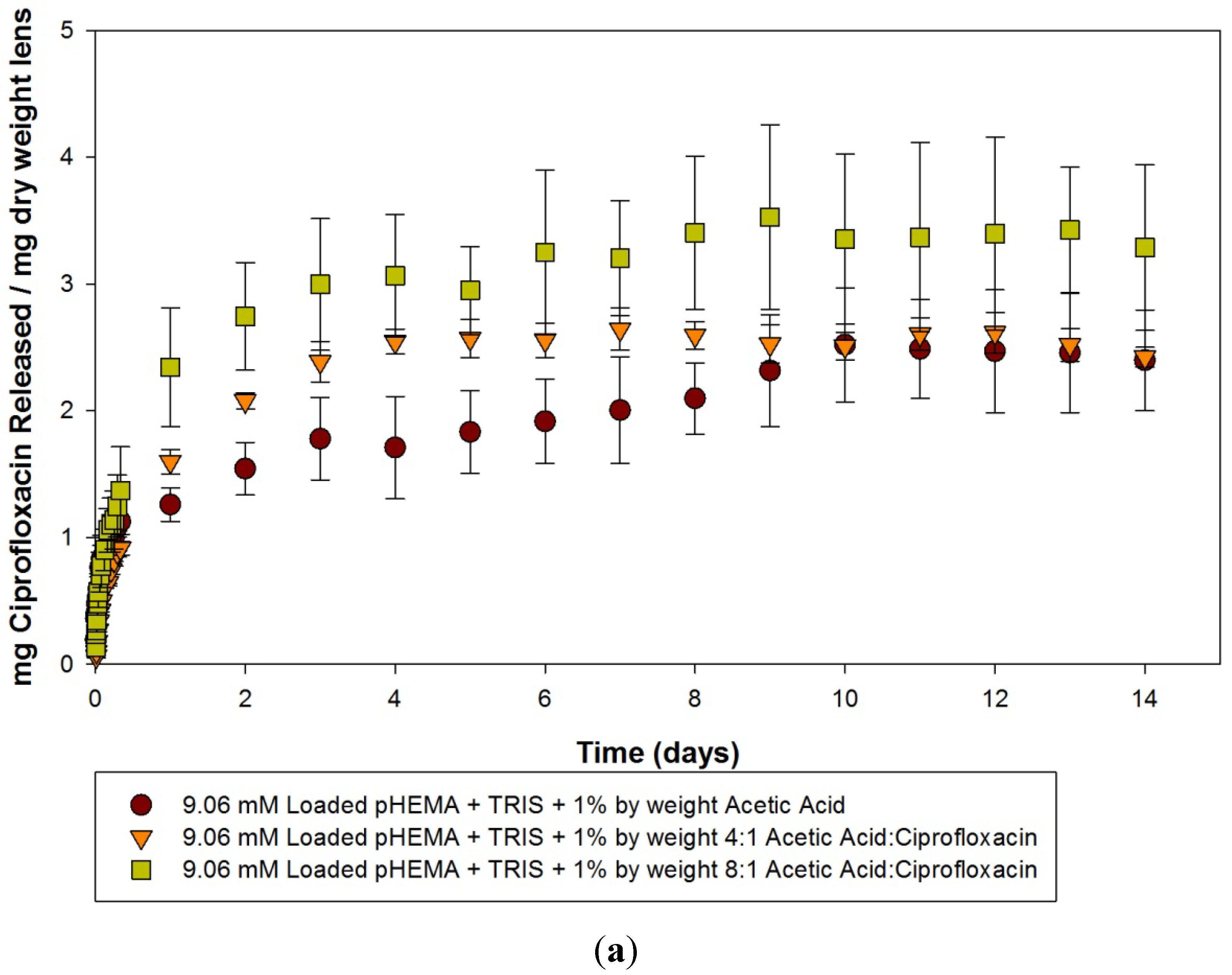
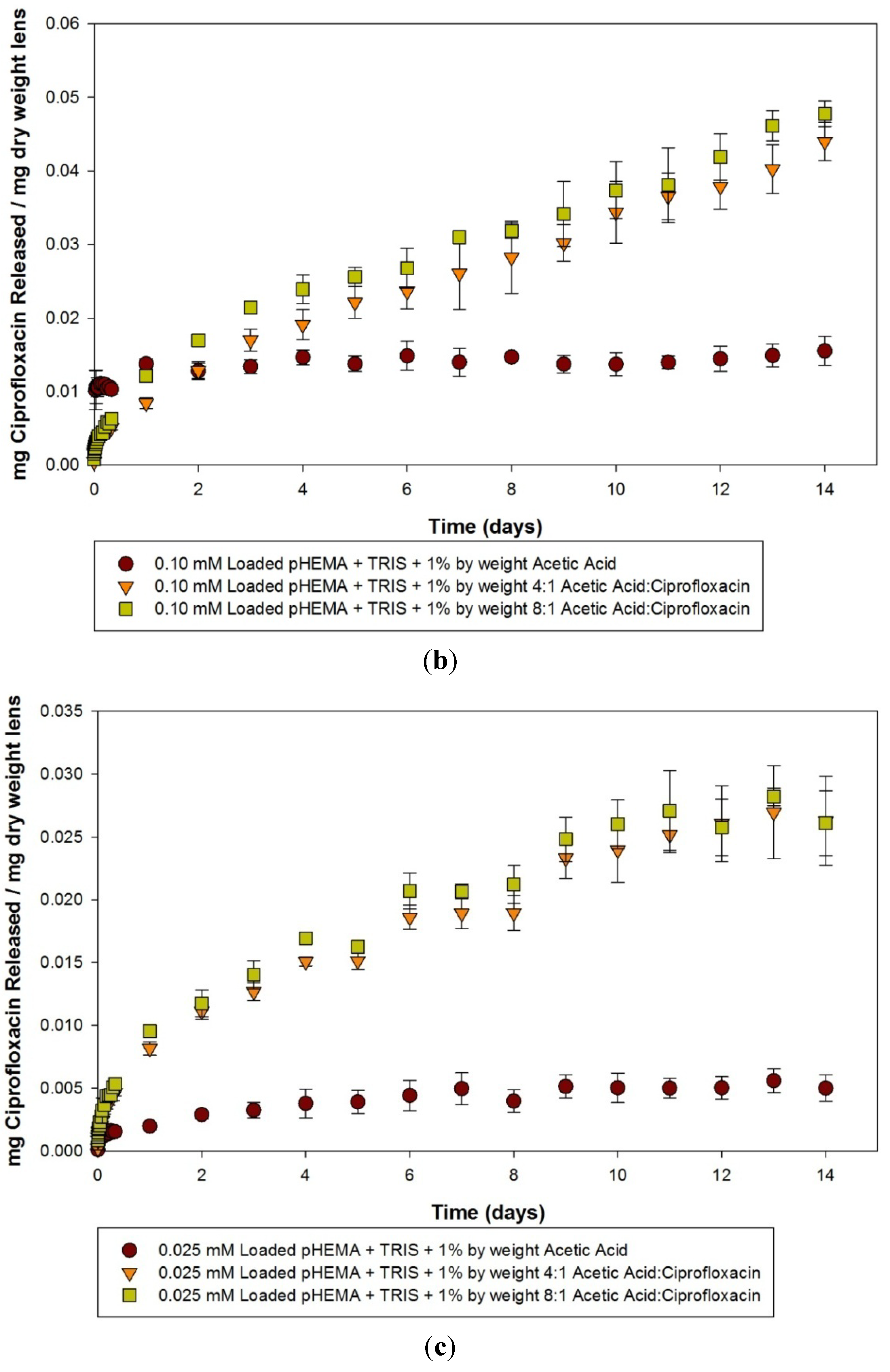
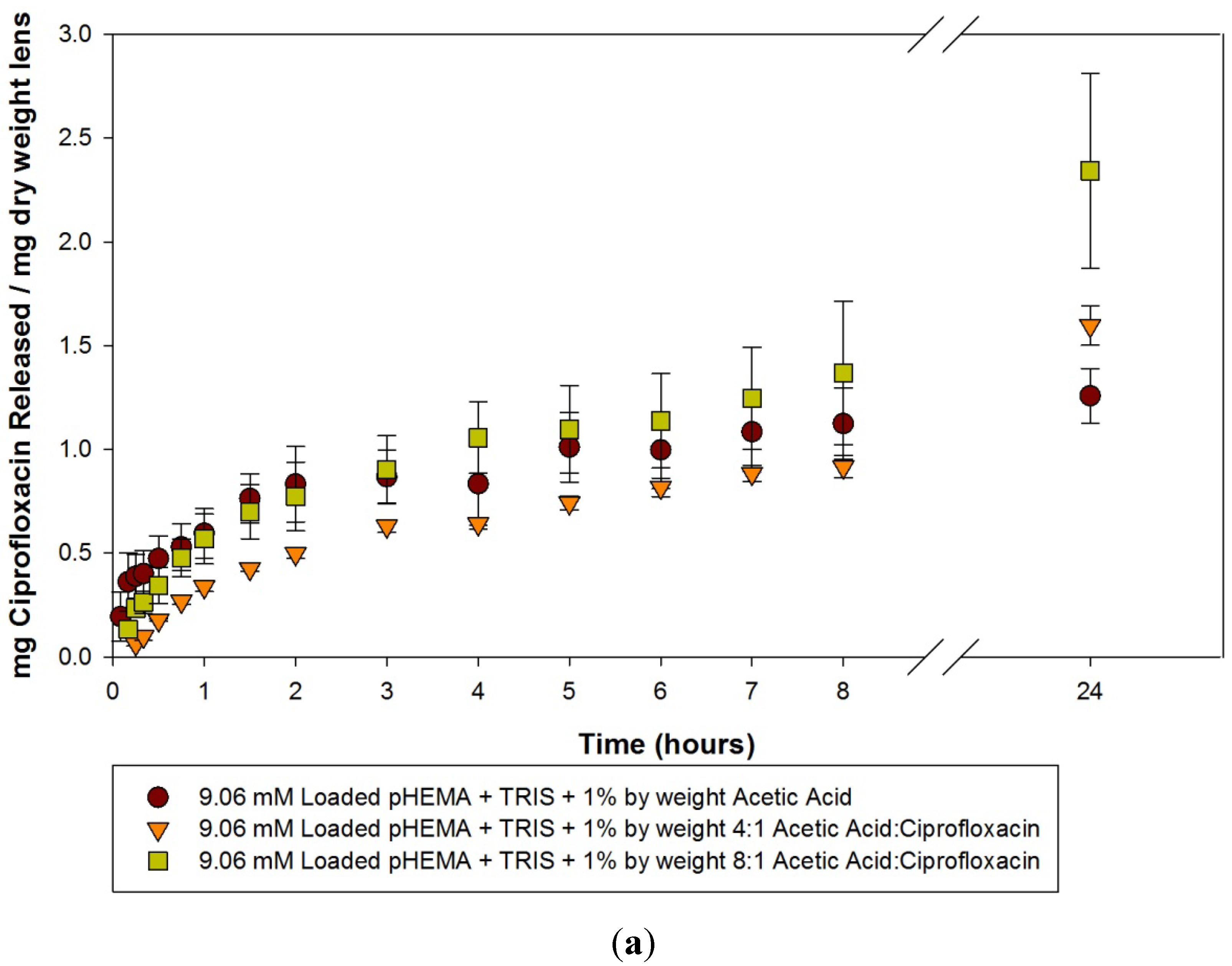
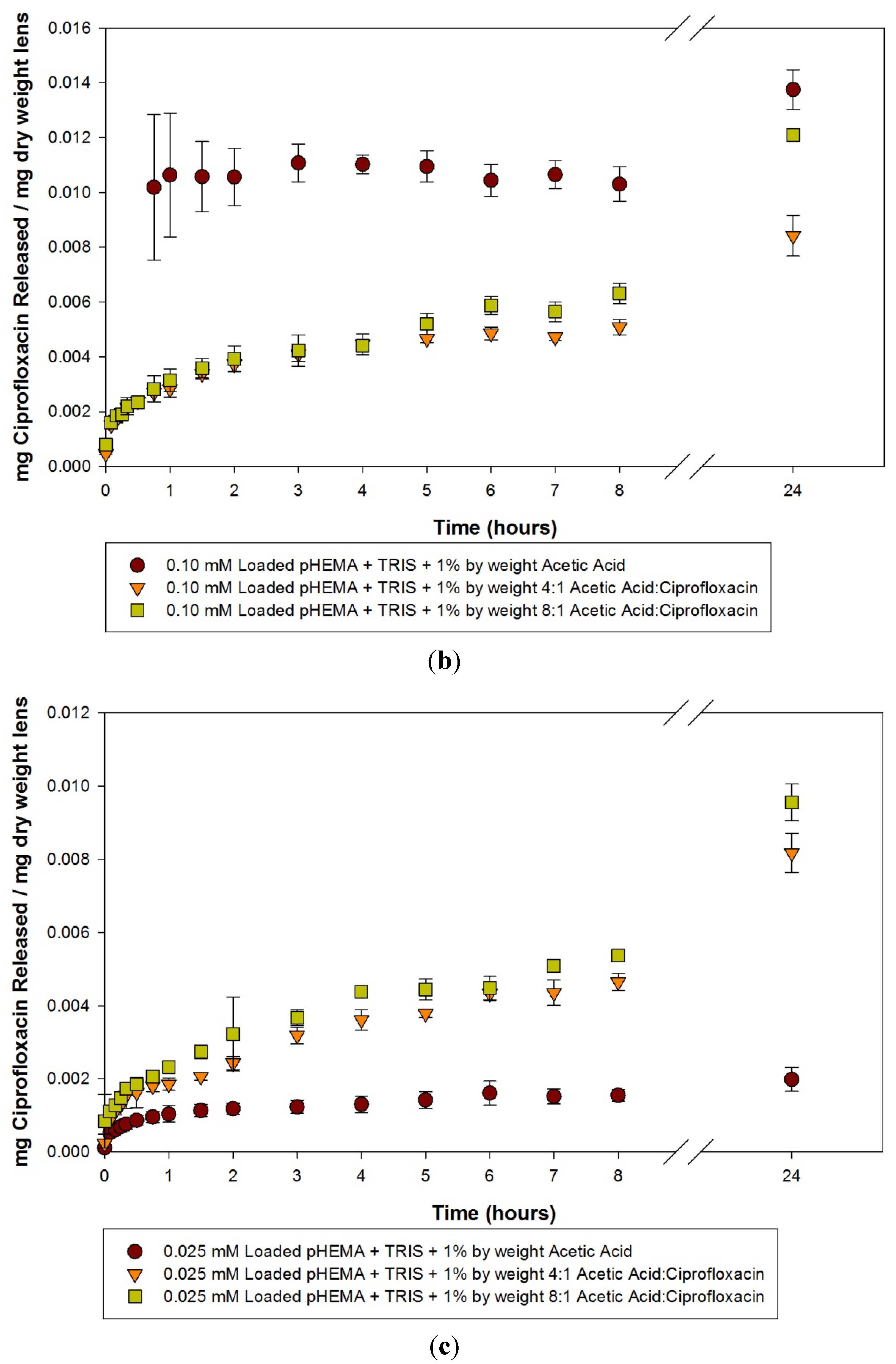
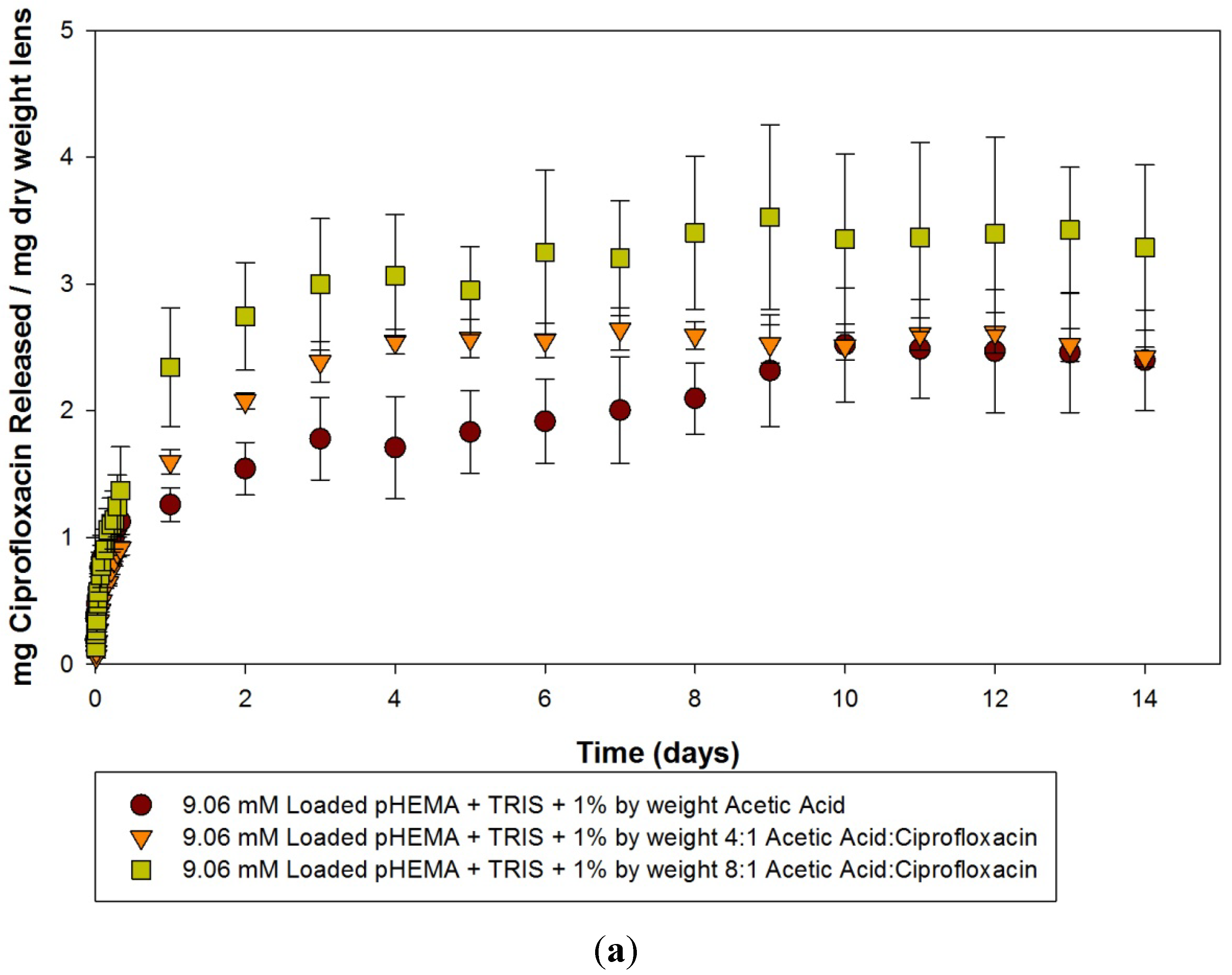
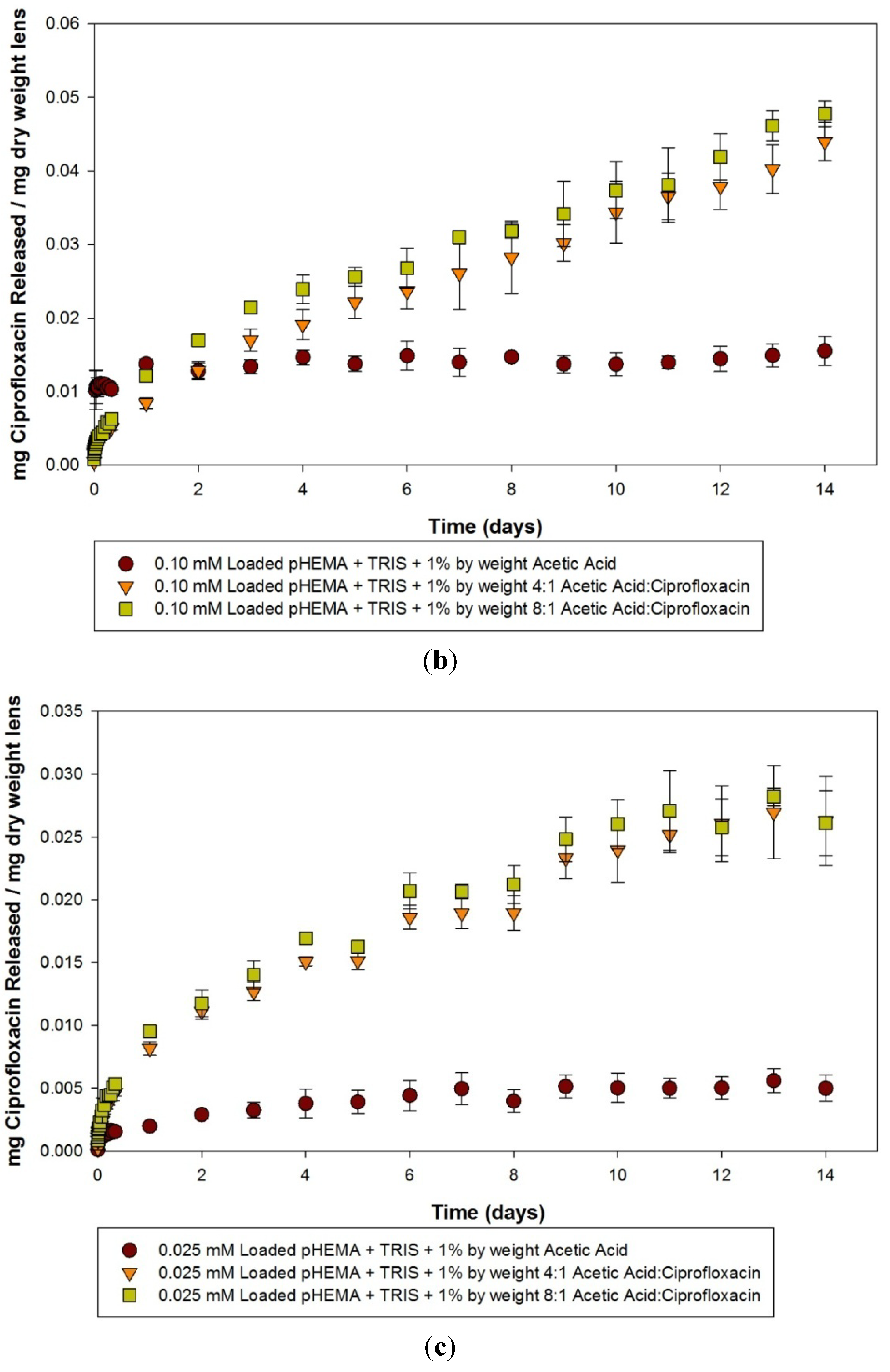
2.1. Pilot Study: Ciprofloxacin pHEMA-Methacryloxypropyltris (Trimethylsiloxy) Silane (TRIS) Materials with Acetic Acid Functional Monomers

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model lens type | Dry weight (g) (Average ± SD) | Water content (%) (Average ± SD) | Centre thickness (mm) (Average ± SD) | Volume (mm3) (Average ± SD) |
|---|---|---|---|---|
| pHEMA + TRIS + 1% by weight Acetic Acid Control | 0.0457 ± 0.0089 | 15.5 ± 2.7 | 0.87 ± 0.12 | 68.1 ± 9.3 |
| pHEMA + TRIS + 1% by weight 4:1 Acetic Acid:Ciprofloxacin | 0.0428 ± 0.0078 | 14.8 ± 2.5 | 0.93 ± 0.16 | 73.2 ± 12.9 |
| pHEMA + TRIS + 1% by weight 8:1 Acetic Acid:Ciprofloxacin | 0.0396 ± 0.0059 | 16.7 ± 2.1 | 0.99 ± 0.14 | 77.3 ± 10.8 |
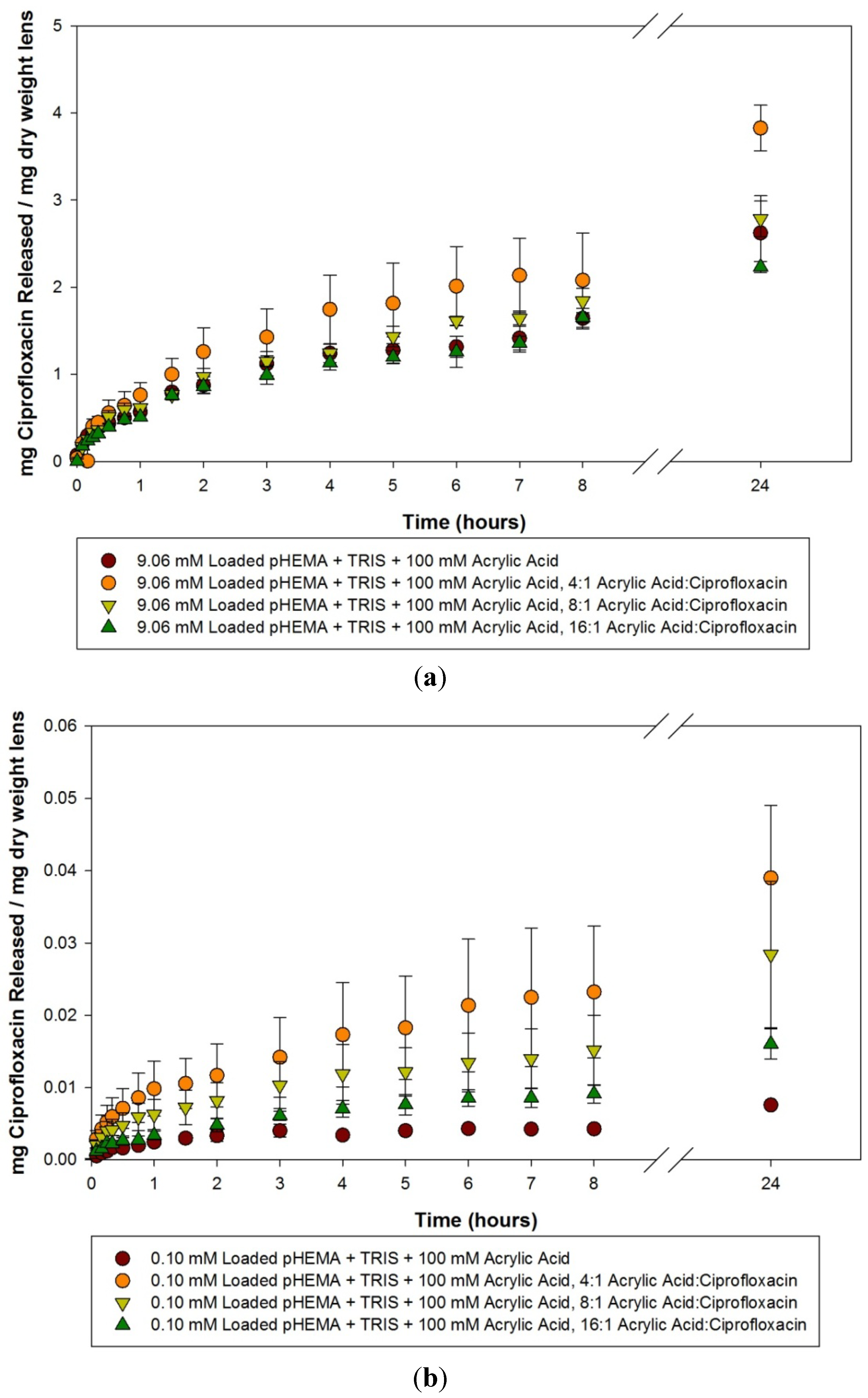
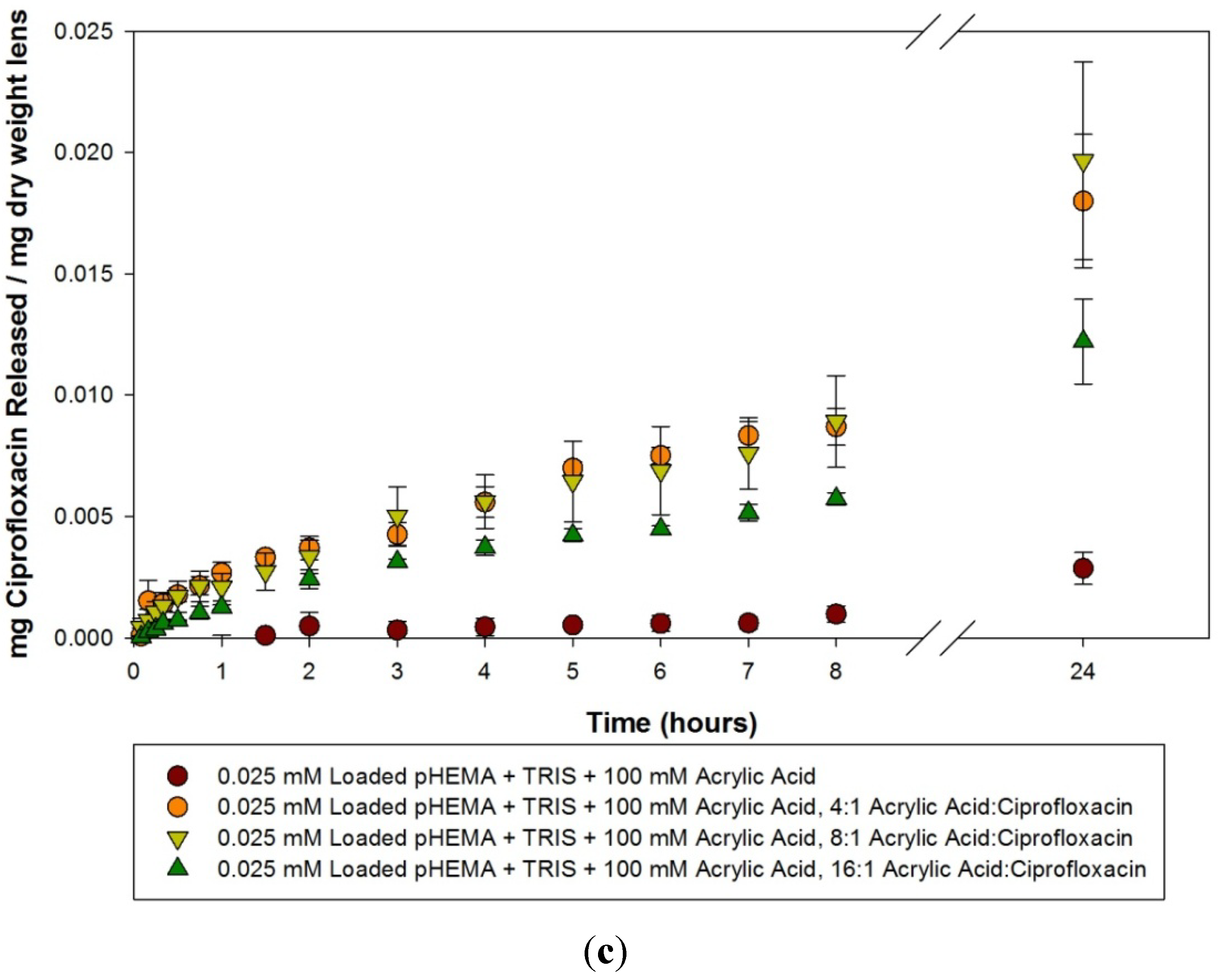
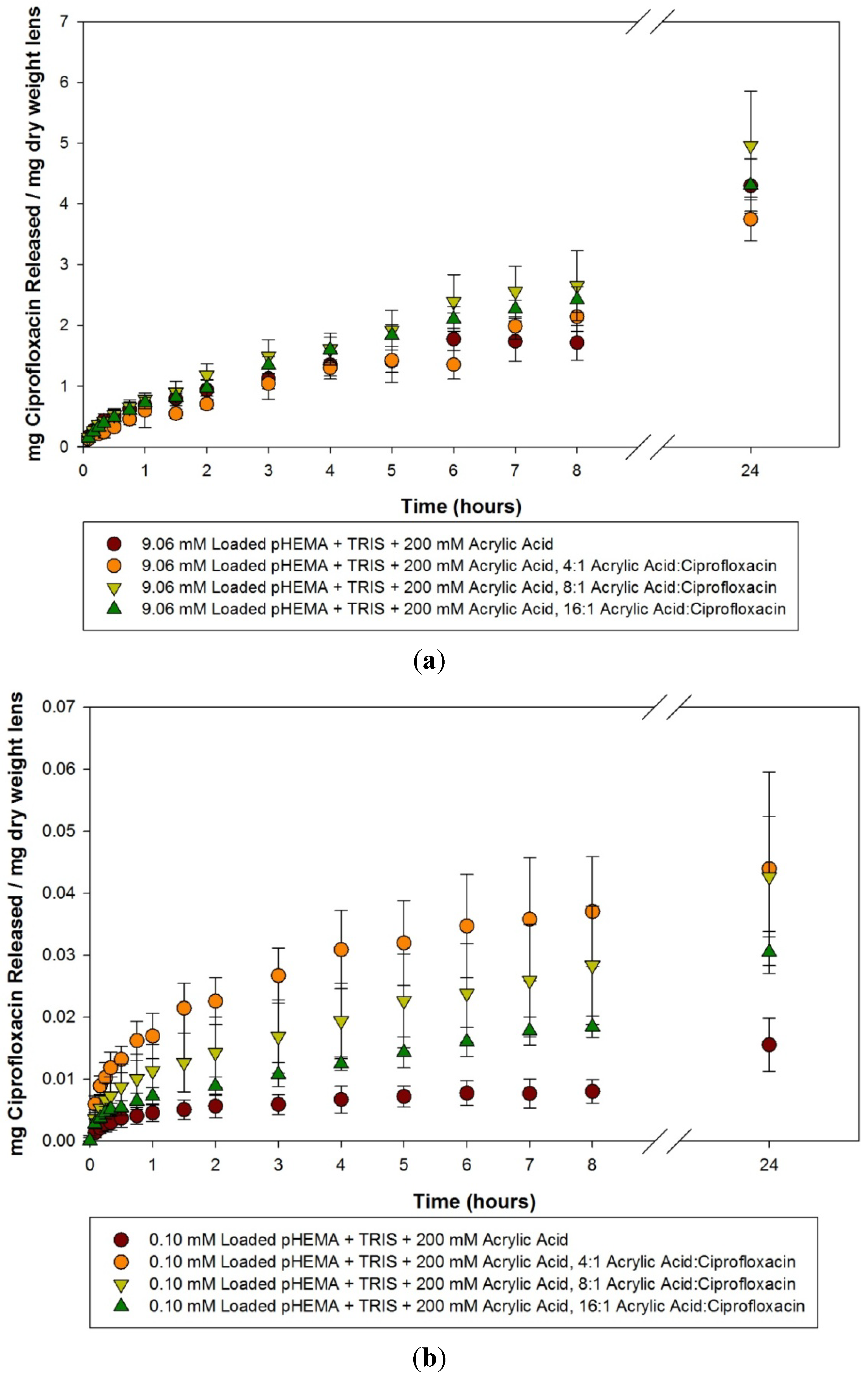
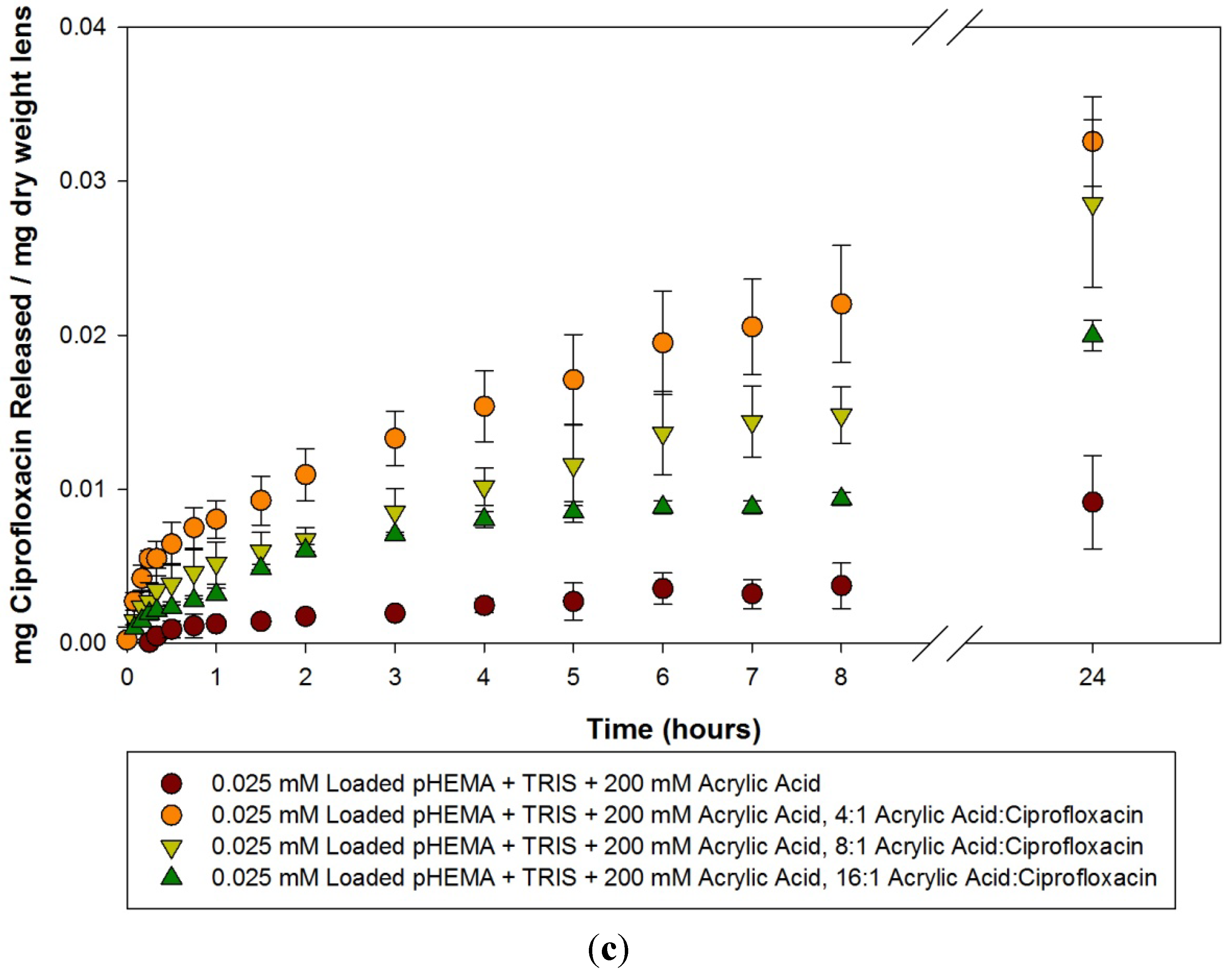
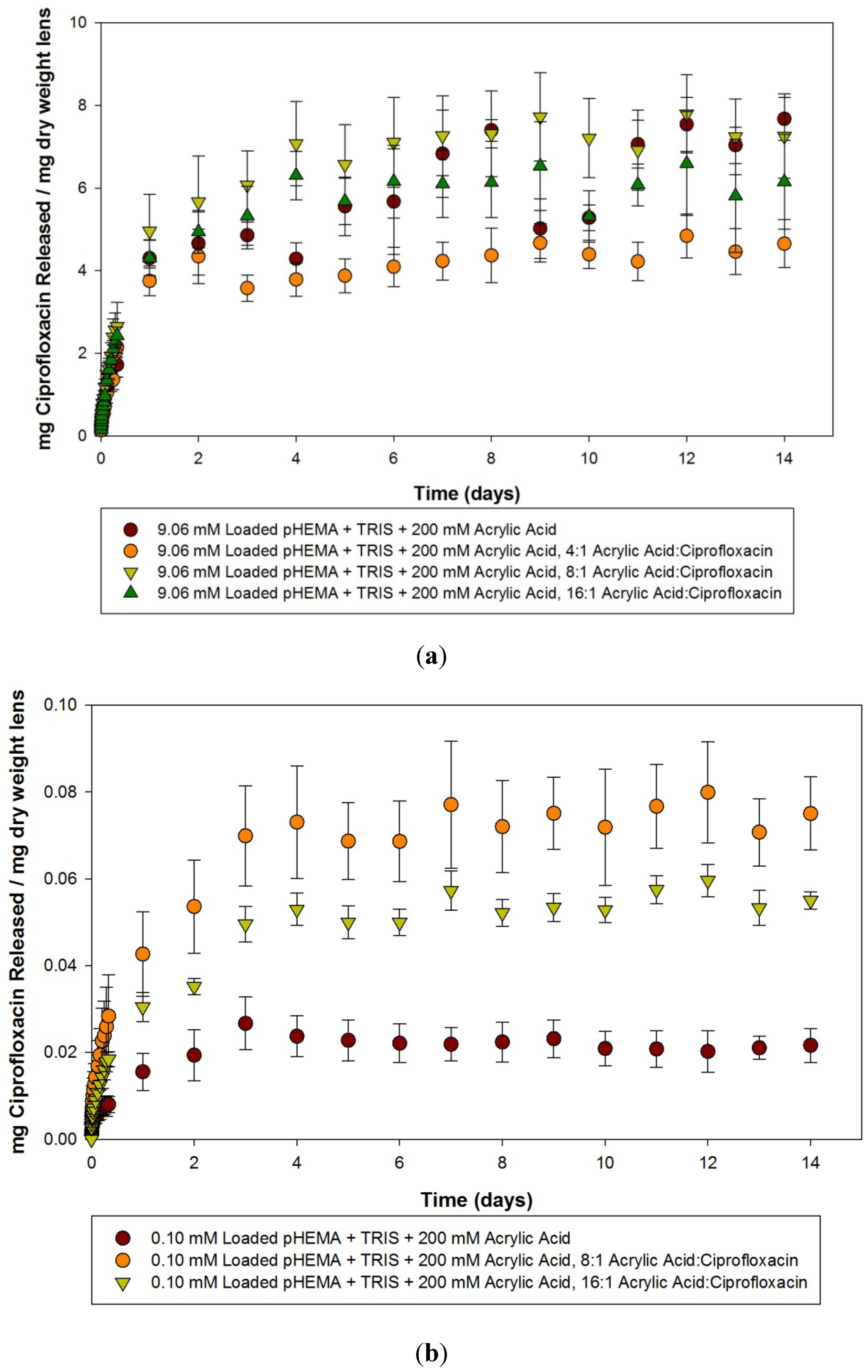
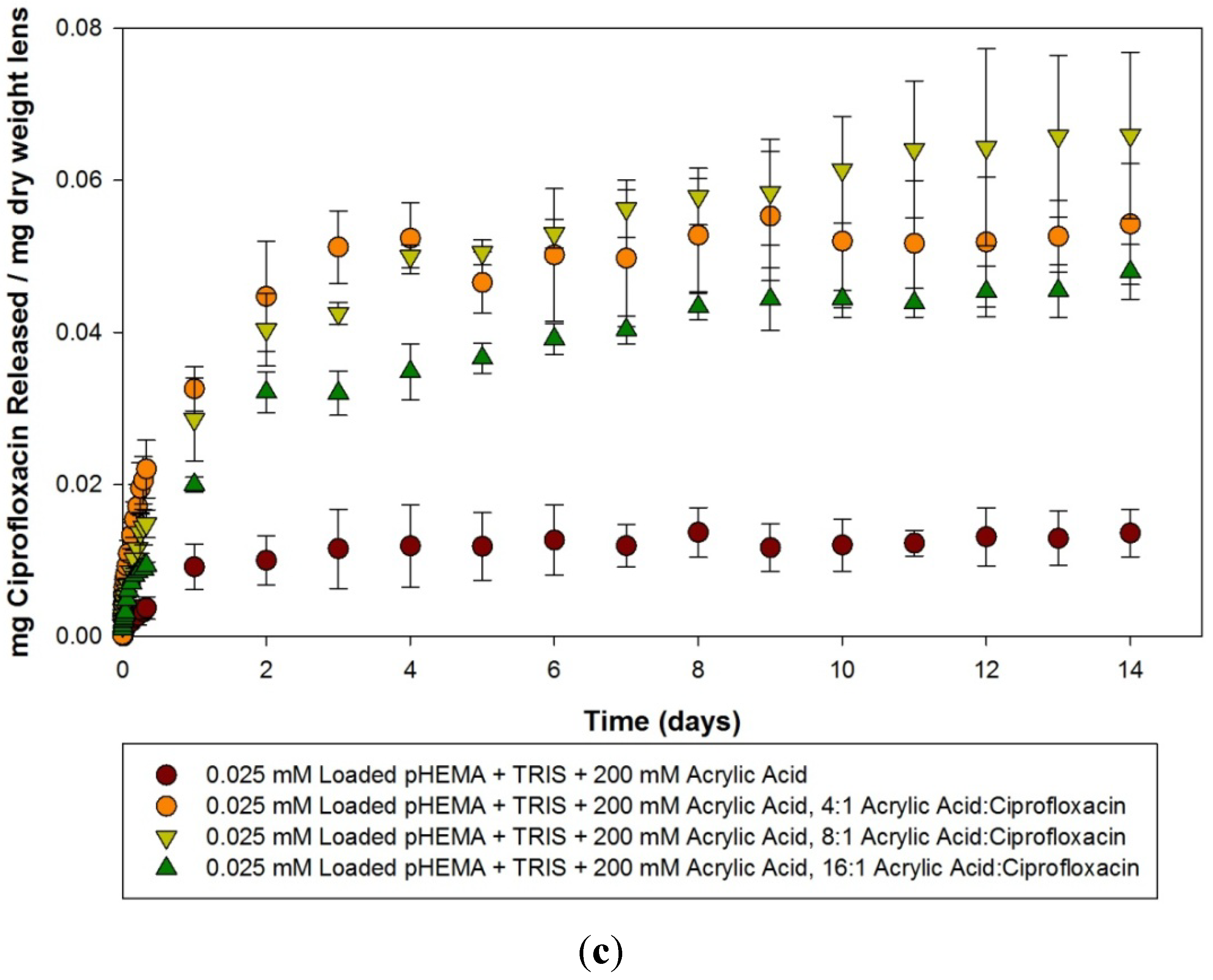
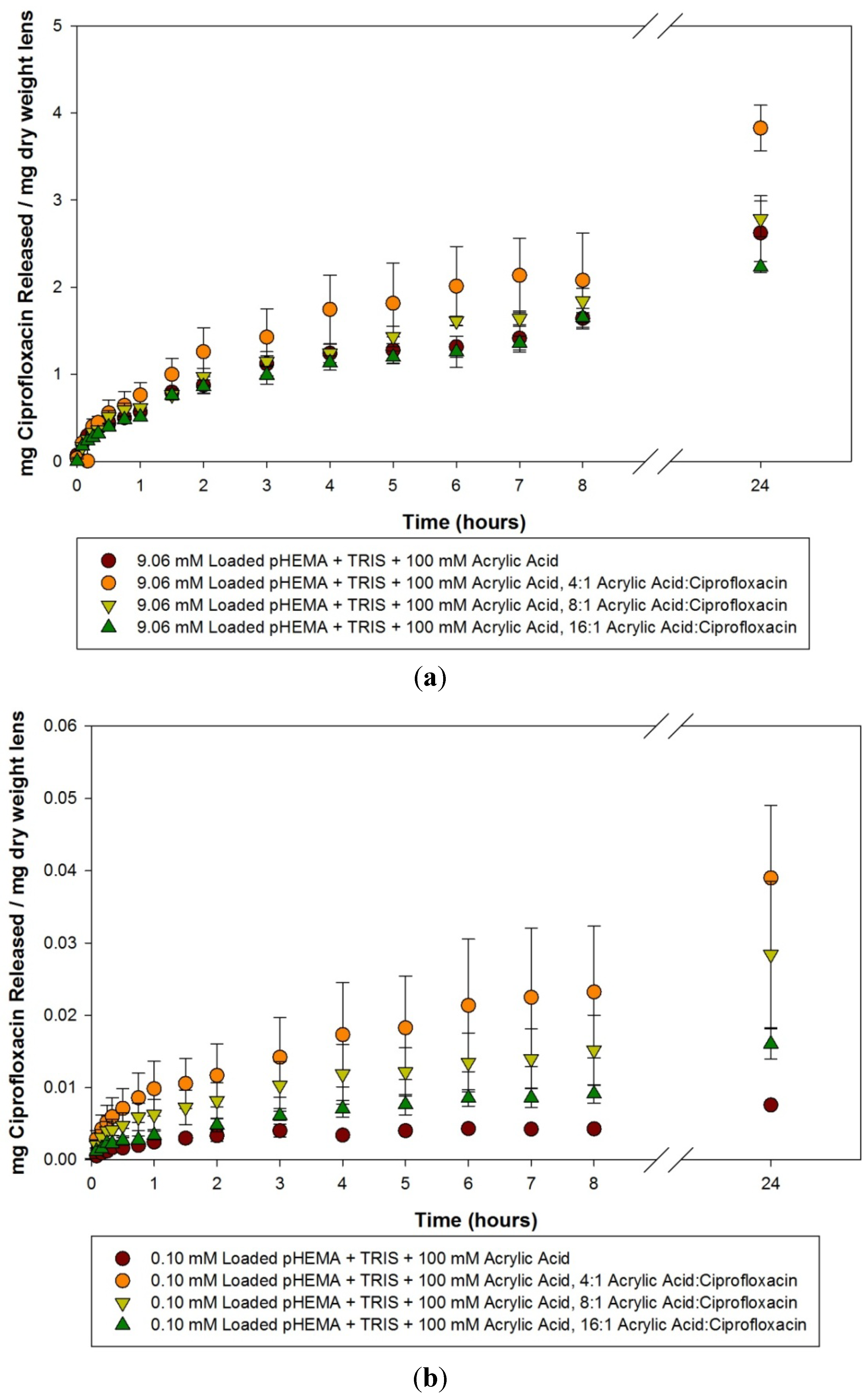
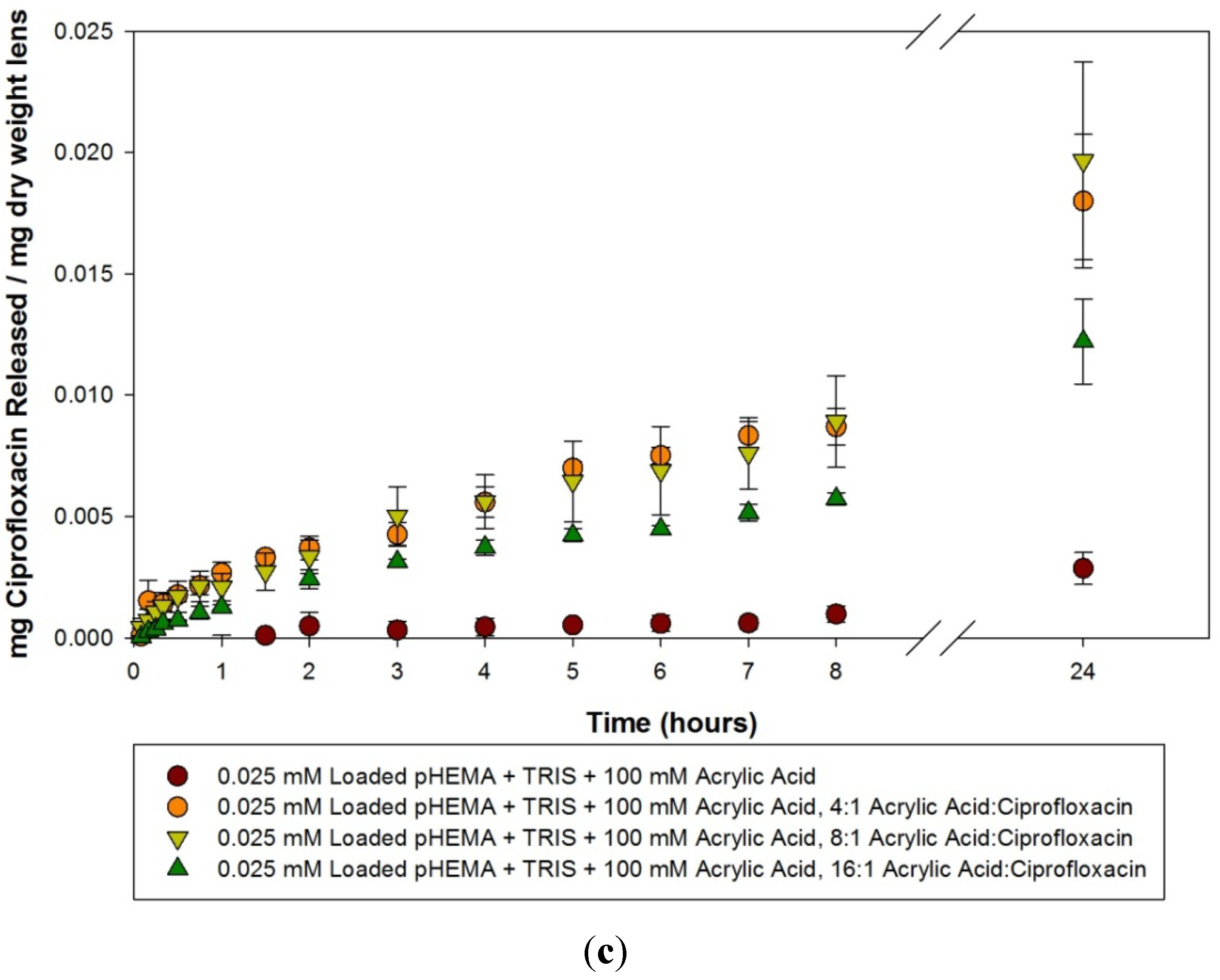
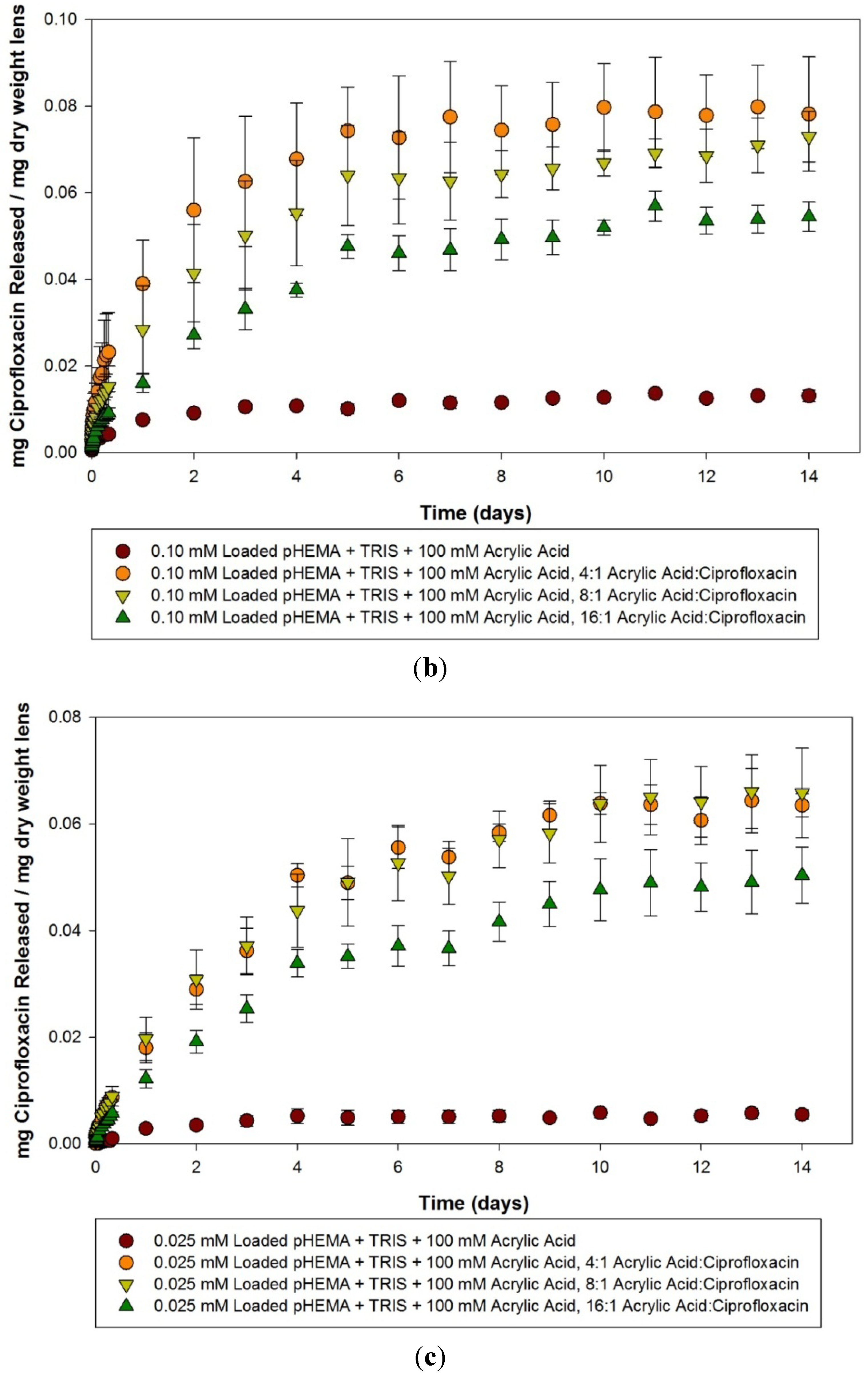
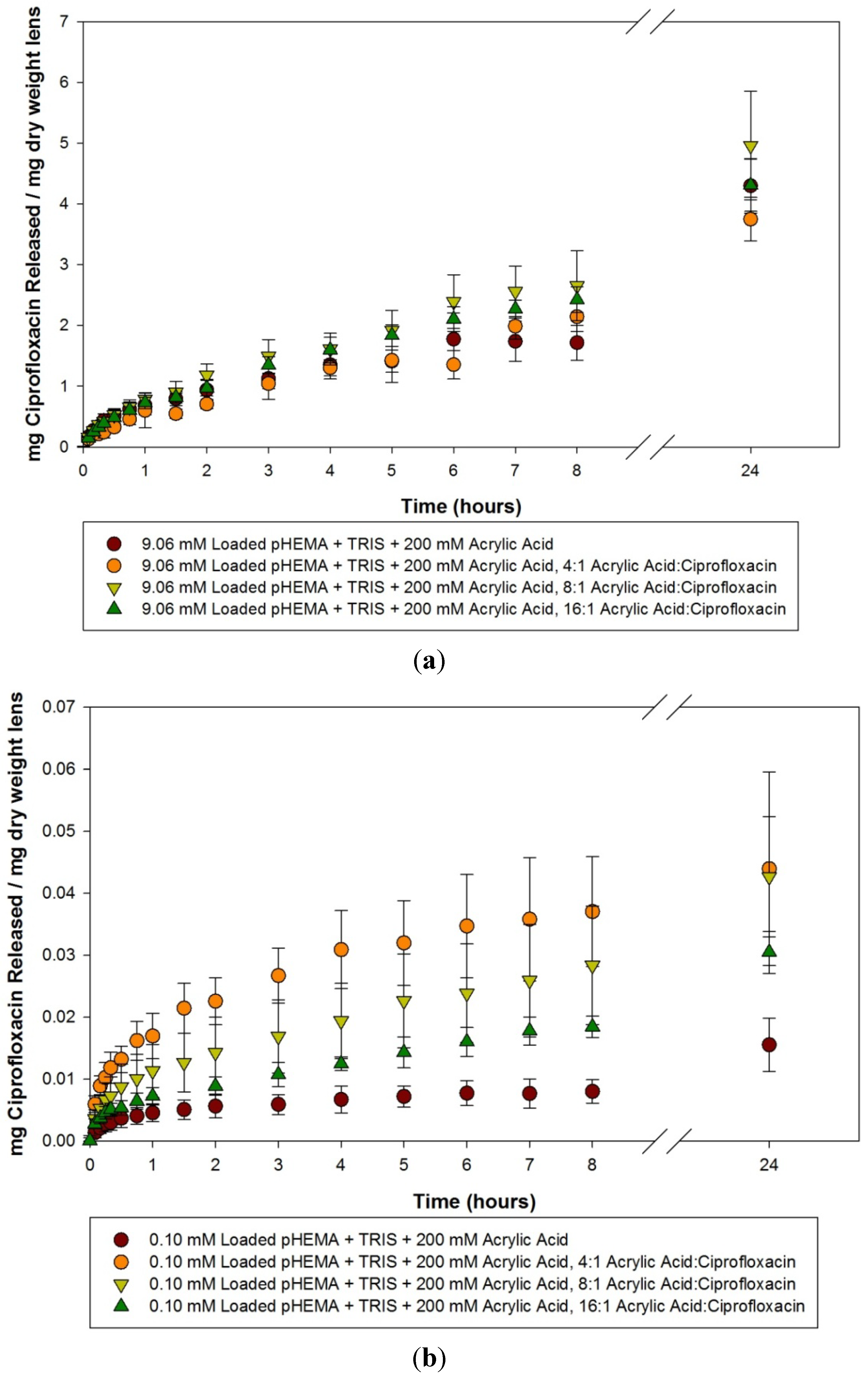
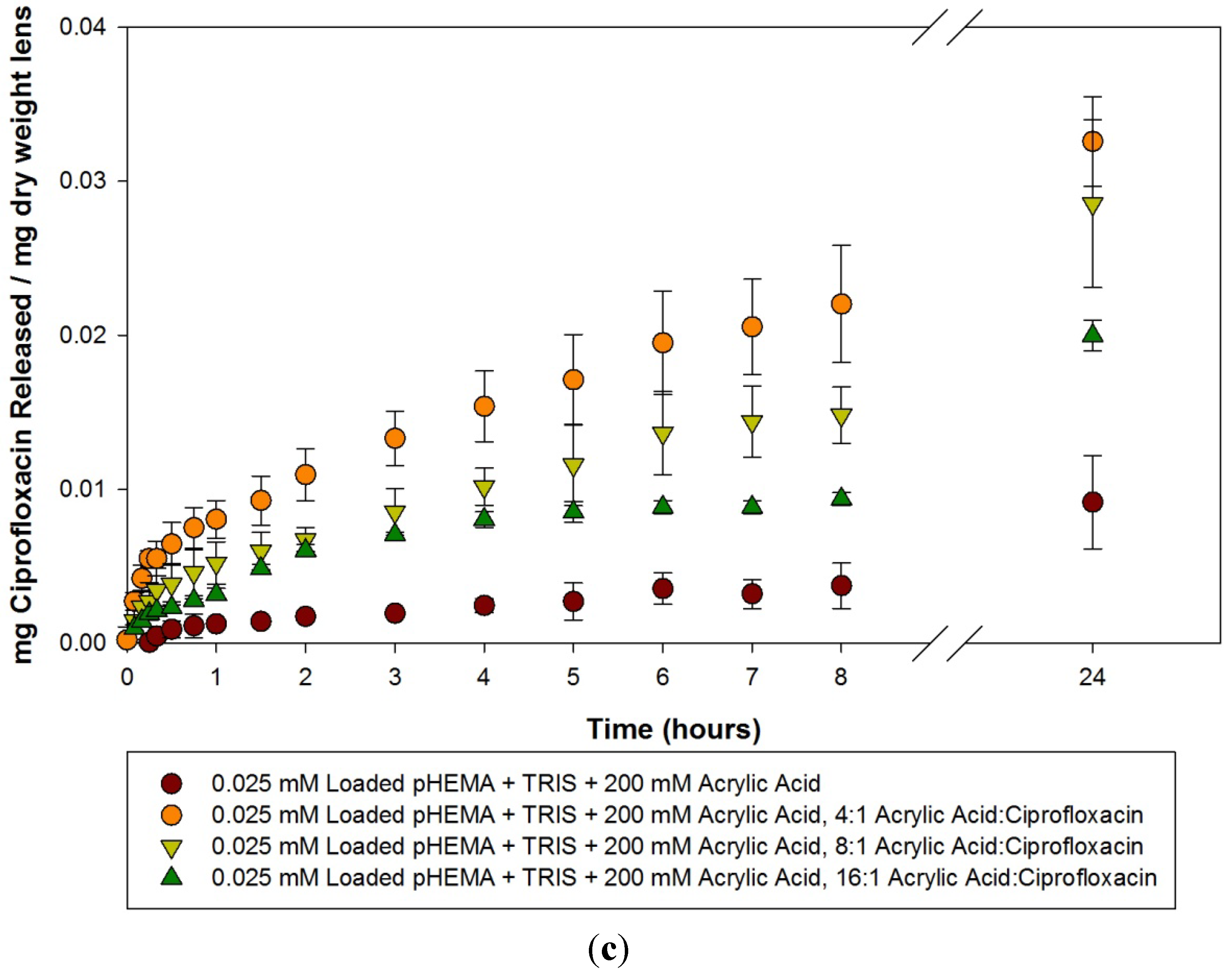
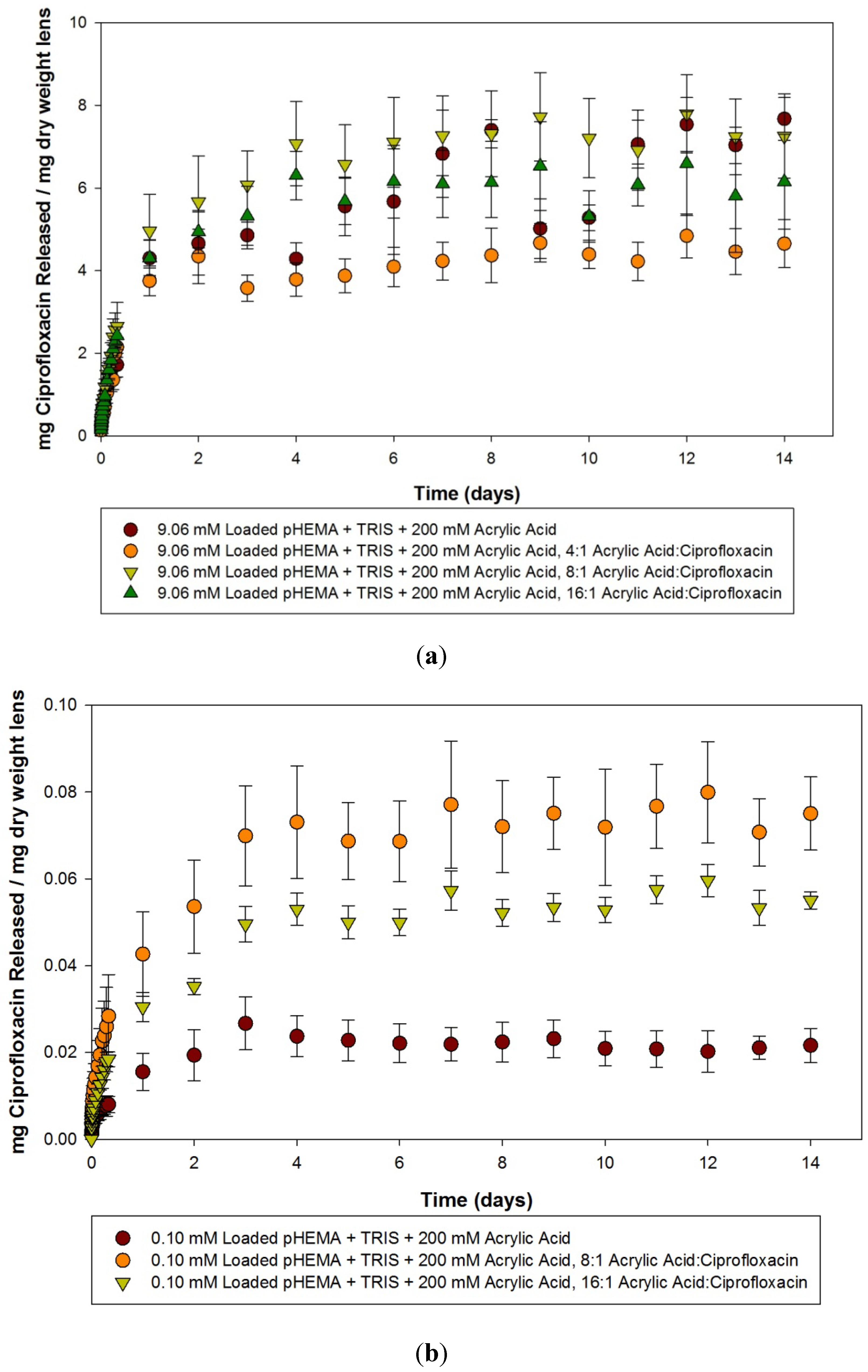
2.2. Ciprofloxacin pHEMA-TRIS Materials with Acrylic Acid Functional Monomers
| Model lens type | Dry weight (g) (Average ± SD) | Water content (%) (Average ± SD) | Centre thickness (mm) (Average ± SD) | Volume (mm3) (Average ± SD) |
|---|---|---|---|---|
| pHEMA + TRIS + 100 mM Acrylic Acid Control | 0.0417 ± 0.0058 | 16.8 ± 4.1 | 0.96 ± 0.07 | 75.5 ± 6.0 |
| pHEMA + TRIS + 200 mM Acrylic Acid Control | 0.0454 ± 0.0064 | 15.1 ± 1.8 | 1.05 ± 0.16 | 82.2 ± 12.6 |
| pHEMA + TRIS + 100 mM Acrylic Acid, 4:1 ratio to ciprofloxacin | 0.035 ± 0.0076 | 16.2 ± 3.6 | 0.78 ± 0.16 | 60.87 ± 12.3 |
| pHEMA + TRIS + 200 mM Acrylic Acid, 4:1 ratio to ciprofloxacin | 0.0576 ± 0.011 | 12.6 ± 2.2 | 1.13 ± 0.3 | 88.3 ± 23.6 |
| pHEMA + TRIS + 100 mM Acrylic Acid, 8:1 ratio to ciprofloxacin | 0.0428 ± 0.0054 | 14.5 ± 2.1 | 1.01 ± 0.12 | 79.6 ± 9.3 |
| pHEMA + TRIS + 200 mM Acrylic Acid, 8:1 ratio to ciprofloxacin | 0.0397 ± 0.010 | 17.7 ± 3.6 | 0.97 ± 0.22 | 75.8 ± 17.4 |
| pHEMA + TRIS + 100 mM Acrylic Acid, 16:1 ratio to ciprofloxacin | 0.0497 ± 0.0053 | 14.3± 2.2 | 1.13 ± 0.13 | 88.6 ± 9.9 |
| pHEMA + TRIS + 200 mM Acrylic Acid, 16:1 ratio to ciprofloxacin | 0.0523 ± 0.0062 | 13.6 ± 1.4 | 1.20 ± 0.14 | 94.6 ± 10.9 |


3. Experimental Section
3.1. Materials
3.2.1. Model Silicone Hydrogels
3.2.2. Molecular Imprinted Materials—Acetic Acid Functional Monomer
3.2.3. Molecular Imprinted Materials—Acrylic Acid Functional Monomer
3.2.4. Molecular Imprinted Materials—Washout
3.3. Drug Solutions
3.4. Water Content, Centre Thickness, Volume and Dry Weight Determination
3.5. Drug Loading into Materials
3.6. Drug Release Kinetics
3.7. Statistical Analysis
4. Conclusions
Acknowledgments
References
- Riley, C.; Young, G.; Chalmers, R. Prevalence of ocular surface symptoms, signs, and uncomfortable hours of wear in contact lens wearers: The effect of refitting with daily-wear silicone hydrogel lenses (senofilcon A). Eye Contact Lens 2006, 32, 281–286. [Google Scholar] [CrossRef] [PubMed]
- White, C.J.; Byrne, M.E. Molecularly imprinted therapeutic contact lenses. Expert Opin. Drug Deliv. 2010, 7. [Google Scholar] [CrossRef]
- Villani, E.; Ceresara, G.; Beretta, S.; Magnani, F.; Viola, F.; Ratiglia, R. In vivo confocal microscopy of meibomian glands in contact lens wearers. Invest. Ophthalmol. Vis. Sci. 2011, 52, 5215–5219. [Google Scholar] [CrossRef] [PubMed]
- Hoare, T.R.; Kohane, D.S. Hydrogels in drug delivery: Progress and challenges. Polymer 2008, 49, 1993–2007. [Google Scholar] [CrossRef]
- Lesher, G.A.; Gunderson, G.G. Continuous drug delivery through the use of disposable contact lenses. Optom. Vis. Sci. 1993, 70, 1012–1018. [Google Scholar] [CrossRef]
- Reynolds, A.; Moore, J.E.; Naroo, S.A.; Moore, C.T.; Shah, S. Excimer laser surface ablation—A review. Clin. Exp. Ophthalmol. 2010, 38, 168–182. [Google Scholar] [CrossRef]
- Boone, A.; Hui, A.; Jones, L. Uptake and release of dexamethasone phosphate from silicone hydrogel and group I, II, and IV hydrogel contact lenses. Eye Contact Lens 2009, 35, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Hui, A.; Boone, A.; Jones, L. Uptake and release of ciprofloxacin-HCl from conventional and silicone hydrogel contact lens materials. Eye Contact Lens 2008, 34, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Karlgard, C.C.S.; Jones, L.W.; Moresoli, C. Ciprofloxacin interaction with silicon-based and conventional hydrogel contact lenses. Eye Contact Lens 2003, 29, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Karlgard, C.C.S.; Wong, N.S.; Jones, L.W.; Moresoli, C. In vitro uptake and release studies of ocular pharmaceutical agents by silicon-containing and p-HEMA hydrogel contact lens materials. Int. J. Pharm. 2003, 257, 141–151. [Google Scholar] [CrossRef]
- Kim, J.; Peng, C.C.; Chauhan, A. Extended release of dexamethasone from silicone-hydrogel contact lenses containing vitamin E. J. Control. Release 2010, 148, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.C.; Kim, J.; Chauhan, A. Extended delivery of hydrophilic drugs from silicone-hydrogel contact lenses containing vitamin E diffusion barriers. Biomaterials 2010, 31, 4032–4047. [Google Scholar] [CrossRef] [PubMed]
- Weiner, A.L.; Gilger, B.C. Advancements in ocular drug delivery. Vet. Ophthalmol. 2010, 13, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, X.; Sun, F. Cyclodextrin-containing hydrogels for contact lenses as a platform for drug incorporation and release. Acta Biomater. 2010, 6, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Danion, A.; Arsenault, I.; Vermette, P. Antibacterial activity of contact lenses bearing surface-immobilized layers of intact liposomes loaded with levofloxacin. J. Pharm. Sci. 2007, 96, 2350–2363. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Lorenzo, C.; Concheiro, A. Molecularly imprinted polymers for drug delivery. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2004, 804, 231–245. [Google Scholar] [CrossRef]
- Hiratani, H.; Alvarez-Lorenzo, C. Timolol uptake and release by imprinted soft contact lenses made of N,N-diethylacrylamide and methacrylic acid. J. Control. Release 2002, 83, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Byrne, M.E. Controlled release of high molecular weight hyaluronic acid from molecularly imprinted hydrogel contact lenses. Pharm. Res. 2009, 26, 714–726. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Lorenzo, C.; Yañez, F.; Barreiro-Iglesias, R.; Concheiro, A. Imprinted soft contact lenses as norfloxacin delivery systems. J. Control. Release 2006, 113, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Andrade-Vivero, P.; Fernandez-Gabriel, E.; Alvarez-Lorenzo, C.; Concheiro, A. Improving the loading and release of NSAIDs from pHEMA hydrogels by copolymerization with functionalized monomers. J. Pharm. Sci. 2007, 96, 802–813. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, S.; Sizemore, S.P.; Byrne, M.E. Biomimetic hydrogels for enhanced loading and extended release of ocular therapeutics. Biomaterials 2007, 28, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Horikawa, S.; Venkatesh, S.; Saha, J.; Hong, J.W.; Byrne, M.E. Zero-order therapeutic release from imprinted hydrogel contact lenses within in vitro physiological ocular tear flow. J. Control. Release 2007, 124, 154–162. [Google Scholar] [CrossRef] [PubMed]
- White, C.J.; McBride, M.K.; Pate, K.M.; Tieppo, A.; Byrne, M.E. Extended release of high molecular weight hydroxypropyl methylcellulose from molecularly imprinted, extended wear silicone hydrogel contact lenses. Biomaterials 2011, 32, 5698–5705. [Google Scholar] [CrossRef] [PubMed]
- Bedard, J.; Bryan, L.E. Interaction of the fluoroquinolone antimicrobial agents ciprofloxacin and enoxacin with liposomes. Antimicrob. Agents Chemother. 1989, 33, 1379–1382. [Google Scholar] [CrossRef] [PubMed]
- Marchese, A.L.; Slana, V.S.; Holmes, E.W.; Jay, W.M. Toxicity and pharmacokinetics of ciprofloxacin. J. Ocul. Pharmacol. 1993, 9, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Pennefather, P.M.; Kaye, S.B.; Hart, C.A. Fluoroquinolones: Place in ocular therapy. Drugs 2001, 61, 747–761. [Google Scholar] [CrossRef] [PubMed]
- Bower, K.S.; Kowalski, R.P.; Gordon, Y.J. Fluoroquinolones in the treatment of bacterial keratitis. Am. J. Ophthalmol. 1996, 121, 712–715. [Google Scholar] [CrossRef] [PubMed]
- PRODUCT MONOGRAPH: CILOXAN® 0.3% Ciprofloxacin Hydrochloride Ophthalmic Solution and Ointment (0.3% as ciprofloxacin) Antibacterial Agent. Available online: http://www.alcon.ca/pdf/Product_pharma/Product_pharma_ciloxan_eng.pdf (accessed on 22 December 2011).
- Ross, D.L.; Riley, C.M. Aqueous solubilities of some variously substituted quinolone antimicrobials. Int. J. Pharm. 1990, 63, 237–250. [Google Scholar] [CrossRef]
- Wilhelmus, K.R.; Abshire, R.L. Corneal ciprofloxacin precipitation during bacterial keratitis. Am. J. Ophthalmol. 2003, 136, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.D.D.; D’Azevedo, P.A.; Francisco, W.; Höfling-Lima, A.L. In vitro activity of fluoroquinolones against ocular bacterial isolates in São Paulo, Brazil. Cornea 2007, 26, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Hiratani, H.; Mizutani, Y.; Alvarez-Lorenzo, C. Controlling drug release from imprinted hydrogels by modifying the characteristics of the imprinted cavities. Macromol. Biosci. 2005, 5, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, R.P.; Dhaliwal, D.K.; Karenchak, L.M.; Romanowski, E.G.; Mah, F.S.; Ritterband, D.C.; Gordon, Y.J. Gatifloxacin and moxifloxacin: An in vitro susceptibility comparison to levofloxacin, ciprofloxacin, and ofloxacin using bacterial keratitis isolates. Am. J. Ophthalmol. 2003, 136, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Schultz, C.; Breaux, J.; Schentag, J.; Morck, D. Drug delivery to the posterior segment of the eye through hydrogel contact lenses. Clin. Exp. Optom. 2011, 94, 212–218. [Google Scholar] [CrossRef] [PubMed]
- van Beek, M.; Weeks, A.; Jones, L.; Sheardown, H. Immobilized hyaluronic acid containing model silicone hydrogels reduce protein adsorption. J. Biomater. Sci. Polym. Ed. 2008, 19, 1425–1436. [Google Scholar]
- Lorentz, H.; Heynen, M.; Kay, L.; Dominici, C.; Khan, W.; Ng, W.; Jones, L. Contact lens physical properties and lipid deposition in a characterized artificial tear solution. Mol. Vis. 2011, 17, 3392–3405. [Google Scholar] [PubMed]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hui, A.; Sheardown, H.; Jones, L. Acetic and Acrylic Acid Molecular Imprinted Model Silicone Hydrogel Materials for Ciprofloxacin-HCl Delivery. Materials 2012, 5, 85-107. https://doi.org/10.3390/ma5010085
Hui A, Sheardown H, Jones L. Acetic and Acrylic Acid Molecular Imprinted Model Silicone Hydrogel Materials for Ciprofloxacin-HCl Delivery. Materials. 2012; 5(1):85-107. https://doi.org/10.3390/ma5010085
Chicago/Turabian StyleHui, Alex, Heather Sheardown, and Lyndon Jones. 2012. "Acetic and Acrylic Acid Molecular Imprinted Model Silicone Hydrogel Materials for Ciprofloxacin-HCl Delivery" Materials 5, no. 1: 85-107. https://doi.org/10.3390/ma5010085